NURSING - Oncology Nursing at UC San Diego Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

J O U R N A L O F
SPRING 2018
NURSING
u n i v e r s i t y o f c a l i f o r n i a , s a n d i e g o
Oncology Nursing at UC San Diego Health
TRANSFORMING CARE AND IMPROVING
OUTCOMES ACROSS THE CONTINUUM
INNOVATE, INVOLVE, INSPIRE
SPRING 2018
JOURNAL OF
NURSING
Inside Message from the
The Chief Clinical Officer
W
2 Message from the Chief Clinical Officer elcome to the 15th issue of the UC San
Margarita Baggett, MSN, RN Diego Health Nursing Journal. This
issue will focus on Oncology Nursing:
AN INTRODUCTION TO ONCOLOGY Transforming Care and Improving Outcomes across
NURSING AT UC SAN DIEGO HEALTH the Continuum. Did you know that there are over 600
nurses working in Oncology services? RN’s, LVN’s, and
4 An Overview of Oncology Nursing at UC San Diego Health
Advanced Practice Providers practice in various settings
Paige Burtson MSN, RN, NEA-BC and Vicki Bradford, BSN, RN, MBA
including the Moores Cancer Center, the Ambulatory
Publisher
6 Oncology Nursing Profiles
Compiled By: Ellen Carr, MSN, RN, AOCN® and Matt Redila,
Five Magnet Clinics, the Jacobs Medical Center, the Hillcrest Medical
Center, and the Outpatient Pavillion. And, over 50%
UCSD Image of Nursing Council
Editors-in-Chief
MSN, RN, CCRN, CNL Componets of the APP’s and RN’s have earned their advanced
certifications! These nurses are providing exceptional
Paige Burtson MSN, RN, NEA-BC STAFF AND PATIENT EXPERIENCE care to our patients in both the inpatient and outpatient
Vicki Bradford, BSN, RN, MBA Transformational settings.
10 Strategies to Promote Staff Wellbeing and Prevent Burnout
Editorial Board
in Inpatient Oncology Units Leadership Structural With the addition of the recently opened Koman Outpatient Pavilion (KOP), UC San Diego
Jill Deetz BSN, RN, NE-BC Health can now offer a “one stop shop” for patients diagnosed with Breast Cancer in our new
Karen Armenion, MSN, RN and Andrea Bogardus, BSN, RN, CHPN
Celine Palmiter, BSN, RN OCN® Empowerment Comprehensive Breast Health Center (CBHC). This truly enables our nurses to embrace the
12 An Extraordinary Outcome Due to Family Presence in an essence of our Nursing Professional Practice Model, where “our focus on developing caring
Advisors Exemplary
Stacie Macaluso, BS Intensive Care Unit relationships with patients, families, each other and ourselves allows us to create an environment
Steffanie Strathdee and Matt Redila, MSN, RN, CCRN, CNL Professional Practice where feeling cared for is an everyday experience”.
Design
I was so pleased to see the themes of patient and family centered care along with having an
Burritt Design 14 Nurses and Radiation Therapists as Superheroes: New Knowledge
interprofessional approach being reflected and valued by our teams. In the article “An Extraordinary
Photography A Unique Approach to Caring for Kids in Radiation Oncology
and Innovation Outcome due to Family Presence in an ICU,” we learn about a gentlemen in Thornton ICU that
Shelby Samonte, RN Sofia Olivares, RN
rapidly decline due to a superbug. It was a family member who suggested trying a type of therapy
Empirical Outcomes which the nurses, doctors, and therapists from the Pulmonary, Critical Care and Infectious Disease
CONTINUOUS QUALITY IMPROVEMENT
departments agreed would be worth pursuing. It was the first application in the United States of
16 The Implementation of an ICU Diary Program to Prevent this type of therapy (bacteriophage) and was credited to saving his life along with the staff from
Post-Intensive Care Syndrome Shared Governance Thornton ICU. What a wonderful outcome showing a truly collaborative environment! You can
Truong-Giang Huynh, BSN, RN, CCRN committee membership is a read even more articles about teamwork in both, “Changing the Care Delivery Model using
great way to become
Clinical Nurse Leaders and Licensed Vocational Nurses in the Oncology Setting” and “Nurses and
20 Implementing Proactive Code Nurse Rounds to Decrease Radiation Therapists as Superheroes”.
personally involved in the
Delay in Rapid Response Activation
Magnet journey and to help Innovation is another theme that is prevalent in many articles. “Implementing Proactive Code
Mary Hellyar, MSN, RN, CNS
shape the future of nursing at RN Unit Rounds to Decrease Mortality and Provide Peer support for Nursing Staff ”, “the
UCSD. For more information Implementation of an ICU Dairy Program to Prevent Post-Intensive Care Syndrome”, and
INNOVATIONS IN ONCOLOGY CARE
go to our nursing website at “CAR-T Therapy: A Novel Treatment for Patients with Relapsed Lymphoma or Leukemia” are
22 The Comprehensive Breast Health Center at the Koman Family http:// medinfo.ucsd.edu/ great examples of our nurses creating new processes and using cutting-edge therapies to help our
Outpatient Pavilion nursing/ committees/ to learn patients achieve better outcomes. I applaud all of you for being so creative in finding new and
Cecilia Kasperick, MSN, RN, CNL about committee membership improved ways to care for our patients.
24 CAR-T Therapy: A Novel Treatment for Patients with Relapsed
opportunities. Nurses Week is a wonderful time to celebrate the dedication and commitment of our entire nursing
team and to recognize how hard these team members work each day. Reading “Strategies Promote
Lymphoma or Leukemia
Staff Wellbeing and Prevent Burnout in Inpatient Oncology Units” I am reminded how important
Aran Tavakoli, MSN, RN, CNS
it is to take the time to care for ourselves as well as our patients. I encourage all of you to take
26 The Development of an Inpatient Palliative Care Unit some time and enjoy the activities we have planned during the week of May 7-10 to celebrate
Karen Armenion, MSN, RN Nurses Week! Activities include Gourmet Food Truck events with free chair massages and a photo
booth, Gratitude Table, Nursing Podcast, Bannister House Fiesta, and the MAGNET focused 2018
28 Changing the Care Delivery Model using Clinical Nurse Leaders Nursing Excellence Awards
(CNL) and Licensed Vocation Nurses (LVN) in the Oncology Setting
Wishing you a wonderful Nurses Week.
Melissa Callahan, BSN, RN OCN, Jessica Hanson MSN, RN, CNL, CCRN
& Laura Vento, MSN, RN, CNL In Gratitude,
Margarita Baggett, MSN, RN
Chief Clinical Officer
A N I N T R O D U C T I O N TO O N C O LO GY N U R S I N G AT U C S A N D I E G O H E A LT H
An Overview of Oncology Nursing at
UC San Diego Health
By: Paige Burtson MSN, RN, NEA-BC and Vicki Bradford, BSN, RN, MBA
N
urses with interest in
specializing in oncology
nursing have an amazing array
of opportunities at UC San Diego
Health. Established in 1978, Moore’s
Cancer Center is ranked among the
top 50 oncology programs in the
nation and is the San Diego region’s
only National Cancer Institute-
designated Comprehensive Cancer
Center. This designation is reserved
for centers with the highest
achievements in cancer research, and genetic counseling. There are then, we have performed over 1800 Surgery, Gynecology Oncology,
clinical care, education and approximately 600 nurses working in autologous and 980 allogeneic Urology, Head and Neck Surgery,
community contributions. The Oncology services at MCC and (related, unrelated and cord blood) and Solid Organ Transplant.
Moore’s Cancer Center’s (MCC) JMC. Over 250 RNs, LVNs and transplants. Our multidisciplinary JMC 5FG Medical Oncology/
unique blend of cancer research and Advanced Practice Providers (NPs team consists of attending physicians, Palliative Care Unit: a 24- bed
patient care is transforming cancer Paige Burtson MSN, RN, NEA-BC is the Vicki Bradford, BSN, RN, MBA is the and PAs) work at MCC and satellite advanced practice providers, transplant progressive care unit focused on
prevention, detection and treatment. Director of Nursing for Inpatient Oncology MCC Asst. Director of Nursing. In locations located in Hillcrest, coordinators, clinic nurse case medical oncology, and palliative care.
In November 2017, the Jacobs Services at UC San Diego Health, Jacob’s collaboration with MCC nurse leaders, Encinitas and Vista. Over 350 RNs managers, social workers, quality The unit features a 12-bed pod that
Medical Center (JMC) opened at the Medical Center. In this role, Paige is Vicki is responsible for clinical and and LVNs work in the Oncology nurse, data management and financial is co-managed by the Hospital
responsible for operational, clinical and regulatory oversight for clinic, procedure service line in the inpatient setting. teams. We also work closely with
La Jolla campus featuring the Foster regulatory oversight over a blood and and infusion services. Medicine and Palliative Care Teams.
Pavilion, 108 all-private, beds focused Oncology nurses ensure appropriate Apheresis, Stem Cell Processing
marrow transplant unit, a surgical JMC 6th floor Blood and Marrow
on surgical oncology, medical care coordination, provide education Laboratory, Infusion Center, Radiation
oncology unit, a medical/surgical ICU, Transplant (BMT) Unit: a 36-bed
oncology, blood and marrow and a medical oncology/palliative care
and resources to facilitate informed Oncology, Procedure Suite,
decision making, and timely access to Operating Room, inpatient nursing, progressive care unit that is all
transplant, neuro-oncology and unit.
quality health and psychosocial care pharmacy and infectious disease. positive pressure allowing patients
palliative care. All beds outside of the
throughout all phases of their care. who are immunocompromised to
ICU are progressive care beds where Radiation Oncology: Utilizing their move throughout the unit. This unit
staff bring the necessary equipment Moore’s Cancer Center includes: knowledge of radiobiology in the also features a patient gym to
and training to the patient versus Infusion Center: Open 363 days a treatment of various forms of cancer, optimize wellness among the BMT
moving the patient from floor to year, Infusion Center RNs and APPs nurses provide care coordination, patients who frequently have long
floor. In addition, there are 36 oversee cancer and non-cancer- recognize the risk factors and inpatient stays.
intensive care beds in Jacobs Medical related infusions and other implement nursing interventions for In addition to providing
Center that serve critically ill patients treatments. Each Infusion Center the common side effects of extraordinary care, several MCC and
with both Oncology and non- RN must have Oncology Nursing treatment. JMC RNs and APPs have been
Oncology medical, surgical and Society (ONS) Chemotherapy/ Jacobs Medical Center includes: selected for poster and panel
neurological diagnoses. Biotherapy certification JMC 3GH Medical Surgical Intensive presentations at ONS Congress and
Both outpatient and inpatient care
Multi-Specialty Clinic: As essential Care Unit: a 24-bed ICU caring for other national oncology associations.
settings provide oncology nurses the
members of more than 14 Specialty medical/surgical, oncology, obstetrics, Over 50% of APPs and RNs have
opportunity to collaborate across
Care Teams, nurses ensure care and abdominal transplant patients. earned advanced certification (OCN,
disciplines. Because every cancer
coordination, management of patient They also service as the code team AOCNP, AOCNS and so forth).
– and every patient – is different,
toxicities, and ongoing patient and and rapid response team for all JMC Shared governance councils are
nurses are an integral part of each
family education. units. robust and engaged in the Oncology
multi-disciplinary team, involving
service line, providing opportunities
specialists in medical, surgical and Blood and Marrow Transplant: The JMC 4th floor Surgical Oncology for professional, clinical and
radiation oncology, pathology, Blood and Marrow Transplant Unit: a 36-bed progressive care unit leadership growth in amplifying
diagnostic radiology, nuclear Program performed its first serving a variety of surgical services: Magnet principles. We are proud to
medicine, social work, palliative care, autologous transplant in 1989. Since Surgical Oncology, Colorectal be oncology nurses!
4 U C S D J O U R N AL O F NU RS ING | S P RING 2018 5
A N I N T R O D U C T I O N TO O N C O LO GY N U R S I N G AT U C S A N D I E G O H E A LT H Compiled By: Ellen Carr, MSN, RN, AOCN® and Matt Redila, MSN, RN, CCRN, CNL
UCSD Ellen Carr, MSN, RN,
AOCN®
currently is the
NURSING JOURNAL PICTORIAL 2018 Clinical Educator for
the UC San Diego Matt Redila, MSN, RN,
Moores Cancer Center
CCRN, CNL
Multispecialty Clinic.
is the Nurse Manager
Before becoming the
for the 3GH ICU,
Clinic’s Educator, she
formerly Thornton ICU.
was a Nurse Case
What motivates you to provide excellent oncology care? Manager for 14 years
He started his nursing
career with Thornton
for the Cancer Center’s
ICU as a new-graduate
surgical head/neck
nurse. Although 3GH
oncology practices. In
ICU is a medical-
addition, Ellen is the
surgical oncology ICU,
Editor of the Clinical
the 3GH ICU nurses are
Journal of Oncology
Victoria Vu, BSN, RN, OCN® also trained to care for
Nursing (CJON), a peer-reviewed journal of the Oncology
Interim Assistant Nurse Manager the obstetric, abdominal transplant, cardiac, and neurology
Nursing Society (ONS). CJON advances excellence in clinical
Moores Cancer Center: Infusion Services patient populations.
practice for nurses specializing in the care of patients with an
actual or potential diagnosis of cancer.
Having cancer is not something a person signs up for, so providing them excellent
compassionate care is something I feel blessed to have the opportunity to do. I chose
oncology for many reasons; foremost is that we develop a long lasting relationship
with patient and family members. I feel like I’m giving them hope by providing
them with education to help with side effects, listening to them, offering a word of
encouragement, and a friendly smile in this difficult journey.
April Morgan, RN, Reiki Master
Infusion Nurse
UC San Diego Health Cancer Services – Vista & Encinitas
The great medicine we provide is only a portion of the healing we provide. A smile
or a hug breaks down barriers and lets the patients know they matter. We are on this
Susan Stalter, BSN, RN, OCN® journey together. I want them to know I will care for them the same way I would a
Nurse Case Manager family member.
Moores Cancer Center: Blood & Marrow Transplant (BMT)
Knowing that I make a difference! I strive to provide the best nursing care possible
for our patients & they always know our dedicated BMT team can be reached
for questions, concerns or reassurance 24/7. We guide our patients through a
long & complicated journey. Sometimes just a warm smile or hug gives support &
encouragement.
Celine Palmiter, BSN, RN, OCN®
Nurse Case Manager
Moores Cancer Center: Multispecialty Clinic
My care and compassion for my patients is my motivation. My toughest days can
never compare to anything that my patients are going through. To be able to help
Polly D. Nobiensky, BSN, RN, OCN® and be there for them during the extent of their cancer journey can be demanding
Nurse Case Manager and challenging, but is so rewarding.
Moores Cancer Center: Radiology Oncology
As a nurse in Radiation Oncology, I am motivated by my nursing colleagues. They all
respect and seek my years of experience to build their own practices. Dr. Sandhu and
our physician team allow me to have autonomy with our patients and practice. Most
of all, I am motivated by our patients. Everyone has their own cancer story and I hope
to help guide them through the toughest time of their lives.
My care and compassion for my patients
is my motivation.
6 U C S D J O U R N AL O F NU RS ING | S P RING 2018 7
UCSD
NURSING JOURNAL PICTORIAL 2018 Knowing that I make a difference!
CONTINUED
I want to provide the best care for my patients
What motivates you to provide excellent oncology care? Chelsea Dean-Robles, BSN, RN
5FG Medical/Oncology/Palliative Care, Jacobs Medical Center
It’s an honor to be an oncology RN. Here at UCSD, we partner with our patients
to create a plan that is tailored to each patient’s individual needs. Through this
collaboration, our patients find a strength in themselves that is truly awe-inspiring.
Tania Miller, BSN, RN, CMSRN® I’m honored to be their healthcare advocate, their educator, and their teammate in
Clinical Nurse their life’s journey.
6 East Hillcrest
UC San Diego Health
What motivates me to provide excellent patient care is the inspiration that I draw
from the 6 East Nursing Team. These nurses have shown me the true meaning of
teamwork, camaraderie and patience. Working with a caring team motivates me to
take care of people who come to us at a low point in their lives and work towards
making them whole again.
April Parker, BSN, RN, OCN
6 Bone Marrow Transplant (BMT), Jacobs Medical Center
I believe it is a calling to be an oncology nurse. Yes, it’s a profession of ups and
downs but what a gift to be able to provide a little slice of normalcy for a patient and
their family. We can often overlook the little things in life, like feeling the sunshine on
Shirley Cruz, BSN, RN, OCN
our skin, but perspective is always brought to life with the gift of oncology nursing.
3GH Intensive Care Unit, Jacobs Medical Center
Working in an Oncology ICU opens your eyes to how a disease like cancer can turn
a fully-functioning, independent individual, into someone fighting for their life. As a
nurse, it is our responsibility to make sure our patients and their loved ones are cared
for both physically and emotionally. We truly have an amazing opportunity to make
a difference in someone’s life while they are going through what could be the most
vulnerable they have ever been. Few things are more rewarding than when a patient
comes back to visit us after they leave the hospital, and to see how they are back to
doing the things that they love!
Marisa Del Rio, BSN, RN
4FGH Surgical Oncology, Jacobs Medical Center
I want to provide the best care for my patients because that person could be my
family. They are going through a very difficult time with unfortunate circumstances
and I want to make sure they receive the best care possible.
I believe it is a calling to be an oncology nurse.
8 U C S D J O U R N AL O F NU RS ING | S P RING 2018 9
S TA F F A N D PAT I E N T E X P E R I E N C E
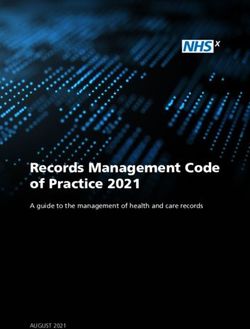
Patient Satisfaction Nursing Scores CAHPS
Strategies for Promoting Staff Wellbeing and
Year Communication Courtesy Listen Explain
Preventing Burnout in Inpatient Oncology Units 2013 86 92.6 82.6 82.6
2014 84 89.9 80.4 81.8
By: Karen Armenion, MSN, RN and Andrea Bogardus, BSN, RN, CHPN
2015 86.3 90.8 84.2 83.9
W
2016 86.4 90.4 83.3 85.4
orking with patients
with cancer is rewarding,
2017 88.7 95.5 87.5 83
but can also lead to staff
burnout. Staff members frequently Be The Match Drive (September 20, 2017)
help patients and families cope 7 staff members volunteered for the day. Pictured
Care Team and/or the nursing staff
with death and dying. Cancer here: April Parker, Andrea Bogardus, Sandy Morin,
gathers together to remember the
treatment can be lengthy and has Alyson McDonough
patient. A small rock is passed on
negative side effects that challenge
from one staff person to another as
the coping skills of most patients
each speaks about his or her memory
and families. Nursing staff members
of the patient. The rocks are placed
are a caring presence through it
all, assisting patients and families as
inside a glass vase on the unit to Nursing Retention for BMT Unit and UCSD
serve as a reminders of the lives that 2013 - 2017
they confront what is frequently the
we have cared for.
biggest challenge of their lives. The
Remembrance Rock Rounds
members of the staff, in turn, need a
allow the staff members to speak
support structure to help them care
about the patient as they remember
for themselves and to enable them
him or her. It provides them an
to be a loving presence for their Andrea Bogardus, BSN, RN, CHPN Karen Lubanga Armenion, MSN, RN
opportunity to value the patient as
patients. Following are two examples is a Registered Nurse on the Blood graduated with a Bachelor of Science in
and Marrow Transplant unit at Jacobs Nursing from Cebu Normal University in a person that they cared for. It is a
of support structures in place at UC
Medical Center. Andrea has been a the Philippines. She ranked 16th overall way for the staff to create closure
San Diego Health that promote
Registered Nurse for 6 years. She in the Philippine National Licensure in caring for the patient and their
staff well-being: 1) Remembrance
started her career on an Acute Leukemia Examination for Registered Nurses in families. The process has emerged
Rock Rounds – an inter-professional Telemetry unit at the University of 1999. Since then, she has worked in organically from the staff as a way to
effort to help staff cope with the Michigan, Ann Arbor. She has worked several organizations as a registered come together after a patient’s death.
death of a patient, 2) The Workplace at UCSD on the BMT unit for the last nurse in the acute care setting. She The unit is now in the process of
Bliss Committee – a staff-led effort 4 years. She earned her bachelor’s joined UC San Diego Health in 2003 as investigating ways to measure the
focused on members helping each degree from Eastern Michigan University. a clinical nurse II in the HIV/Infectious
effectiveness of remembrance rock
other through recognition and social Andrea is the Shared Governance Chair Disease Unit. She pursued her Master’s
rounds in assisting the staff to cope
support. for the BMT unit and is the Co-Chair Degree in Nursing and graduated in
of the Workplace Bliss Committee. 2009 from the University of Phoenix.
with death and dying.
Remembrance Rock Rounds
Andrea is an active preceptor on her Karen has 12 years of administrative The Workplace Bliss Committee
Jacobs Medical Center 5FG is a unit for nursing students, new grads, nursing leadership experience; 7 years Jacobs Medical Center 6FGH and acknowledgement of work activities. Survey results demonstrated
palliative care and medical oncology and experienced nurses. Andrea is also a as an acute care nurse manager. She has
is a blood and marrow transplant performed. Social support from co- an increase in staff morale and
unit on which the nursing staff often Certified Hospice and Palliative Nurse. been successful in improving operations,
(BMT) unit where a Workplace Bliss workers enhances the effects of work in feelings of recognition in all
witnesses the dying process. Nurses work processes, nurse-sensitive
Committee (WBC) was created engagement and nurses’ satisfaction. categories of the Press Ganey. Nurse
are challenged to address the physical, outcomes and patient experience at
by the staff. The WBC focuses on Promoting a fun work environment retention scores steadily increased
emotional, psychological and spiritual the unit, divisional and organizational
levels. Karen has been a mentor for improving staff morale, encouraging is important for employee morale after the initiation of the WBC
aspects of care every day. Nurses in
nursing staff in their leadership and staff recognition, increasing and productivity. Outside work exceeding the retention rates for
the medical oncology and palliative
clinical advancement. She promotes workplace satisfaction, and creating activities and celebrations involving UCSD Health. Patient satisfaction,
care unit go back and forth between
transformational leadership in her daily an atmosphere of fun in which all food are most favored by employees measured through the HCAHPS, also
actively treating one patient while interactions with staff and patients. staff members, including members for providing a sense of fun. To increased.
helping another patient cope with She provided leadership in the opening of the interdisciplinary team, work determine the effectiveness of the Remembrance Rock Rounds and
death. This process takes a toll on the of Jacobs Medical Center 5FG, the together and help each other. WBC, pre and post surveys were the Workplace Bliss Committee are
nursing staff. Medical Oncology and Palliative Care
Supporting the well-being analyzed as well as Press Ganey evidence that frontline staff members
5FG staff members recognize the Unit. Karen is the recipient of the 2014
of the staff is vital to improving Patient and Employee Satisfaction can be successful in initiating
need to help each other replenish Nurse Manager of the Year for Empirical
patients’ quality of care. Two areas scores (Table 4) and retention structures and processes that promote
compassion at the bedside. A few Outcomes.
that influence work satisfaction data (Figure 1). Over 60% of the caring both for themselves and others.
days after a patient dies, the Palliative
are relationships with co-workers staff participated in outside work
10 U C S D J O U R N AL O F NU RS ING | S P RING 2018 11
S TA F F A N D PAT I E N T E X P E R I E N C E
An Extraordinary Outcome Due to
Family Presence in an Intensive Care Unit
By: Steffanie Strathdee and Matt Redila, MSN, RN, CCRN, CNL
N
urse-led inter-
professional bedside
rounds that include
the patient and family was
adopted as a daily practice
for Oncology and non-
Oncology diagnoses in the
intensive care unit (ICU) at
UC San Diego Health in the
Thornton ICU and now in the
Jacobs Medical Center ICU.
Since patients in the ICU are Steffanie Strathdee Dr. Strathdee is Matt Redila, MSN, RN, CCRN, CNL
an infectious disease epidemiologist. is the Nurse Manager for the 3GH ICU,
frequently seriously ill and She is Associate Dean of Global Health
Patient and his wife.
formerly Thornton ICU. He started his
oftentimes intubated, family Sciences and Harold Simon Professor of nursing career with Thornton ICU as a
Medicine at the University of California new-graduate nurse. Although 3GH ICU excreted once the bacteria are gone. began to get better and yet hadn’t READ MORE AT:
members become key San Diego where she directs the is a medical-surgical oncology ICU, the However, each bacteria has to be had a shower in 5 months, another https://health.ucsd.edu/news/topics/
campus-wide Global Health Institute.
members of the inter- 3GH ICU nurses are also trained to care matched to a specific phage; not just nurse coordinated the approvals from phage-therapy/Pages/default.aspx
She is married to Thomas L. Patterson, for the obstetric, abdominal transplant, any phage will do. his hospitalist and Infection Control
professional team. This case Professor of Psychiatry at UC San Diego. cardiac, and neurology patient An international ‘phage hunt’ to make this happen. When Tom WATCH THEIR TEDX:
populations.
study involves a non- ensued. Multiple departments at suffered ICU psychosis and couldn’t youtube.
Thornton and UC San Diego Health sleep because of being turned every comwatch?v=AbAZU8FqzX4&feature=
Oncology patient, but
Sciences cut through the red tape to 2 hours, the charge nurse noted that youtu.be
demonstrates the impact that CASE STUDY experimental treatment, allow Tom to receive IV phage since he had no pressure wounds, she
bacteriophage therapy. This therapy therapy under an Emergency put a sign over his bed saying
family presence can have in In 2015, Tom Patterson and his consists of naturally-evolved viruses Investigational New Drug (EIND) “GOAL: A GOOD NIGHT SLEEP!
wife Steffanie Strathdee, vacationed that attack bacteria. In the TICU, the
achieving extraordinary from the US Food and Drug TURN EVERY 4 HRS.” He and
in Egypt. After falling ill, Tom was inter-professional team, the patient, Administration (FDA), the first Steffanie contend that it made all the
patient outcomes. medevacked to UC San Diego and the family participate daily in application in the US. After just a few difference.
Health, Thornton Intensive Care nurse-led rounds. It was during days of phage therapy, Tom woke up Under the outstanding care of the
Unit (TICU) where he was rounds that Steffanie presented the from his coma and began his long TICU team, Tom beat all odds,
diagnosed with a multi-drug resistant possibility of bacteriophage therapy, recovery. fought off this superbug, and was
bacterial infection, Acinetobacter and the Infection Disease, Pulmonary, He and Steffanie credit discharged home in August 2016. He,
baumanii, which the World Health and Critical Care teams embraced bacteriophage therapy and the TICU Chip and Steffanie and the Infectious
Organization (WHO) considers to the idea. Dr. Chip Schooley agreed care team with saving his life. Beyond Disease, Pulmonary & Critical Care
be one of the deadliest superbugs. to manage the treatment protocol. the applications of medicine, nursing, teams have helped several other
After several months of care in the Bacteriophages exist anywhere physical therapy, occupational therapy patients receive bacteriophage
TICU and multiple rounds of bacteria exist. The virus takes over and speech pathology, the humanity therapy since his illness. Tom’s case
ineffective antibiotic therapy, Tom’s the bacteria and turns it into a phage of the care team made the difference has been covered extensively in the
clinical status declined; he became manufacturing plant, each bacterial in Tom’s recovery. When it looked press.
comatose and was on life support. cell death yielding hundreds of like Tom was going to die, his nurse
Steffanie continued to pursue progeny phages. Human cells are not offered Steffanie a hug. When he
treatment options, which included an harmed by phages; the phages are
12 U C S D J O U R N AL O F NU RS ING | S P RING 2018 13
S TA F F A N D PAT I E N T E X P E R I E N C E
Nurses and Radiation Therapists as Superheroes:
A UNIQUE APPROACH TO CARING FOR KIDS IN
RADIATION ONCOLOGY
By: Sofia Olivares, RN
“Hi! My name is Robert, I’m five and
I have cancer in my brain!”
This was my first encounter and support. The pediatric radiation
with a pediatric patient in radiation nurse utilizes critical thinking skills Sofia sharing a special moment
oncology. I had just shifted from along with knowledge of princesses, with her patient
pediatrics to pediatric radiation super heroes, popular cartoons, music,
oncology and had some reservations movies and fashion.
about whether or not I could UCSD pediatric radiation them as they fall asleep. addition, I keep in communication serves as the advocate for the child as
weather the change. Could I handle oncology embraces family-centered Being a pediatric radiation with the referring team and provide well as their parents.
it emotionally? Would I be a strong care. In family-centered care the oncology clinician requires that one continuous updates on the patient’s I am honored to work with
enough nurse for my patients and patient, family and clinicians work understand where the patient is in treatment plan and response to the UCSD radiation oncology
families? Seeing Robert’s contagious together to plan, educate and provide the course of the disease process. Is treatment. team as a pediatric nurse. Our
smile and sweet demeanor assured patient care. Clinicians involve the patient newly diagnosed? Has Unfortunately, like in the adult pediatric radiation oncologist,
me I was in the right place. parents, grandparents, siblings and the child been undergoing chemo setting, we encounter many pediatric radiation therapist, anesthesiologists,
Radiation oncology nursing friends in the patient’s experience. therapy or other treatment prior to patients who are at the end-of-life administrative staff and social
Sofia Olivares, RN is a Pediatric
requires collaboration with the We encourage the family members radiation? Or perhaps, the patient and require radiation for palliation. worker are invested in providing the
Radiation Oncology Nurse at the UCSD
oncology teams from outside to be involved in the child’s care. is under treatment for end-of-life Many times, these are patients who best care possible to the pediatric
Moore’s Cancer Center and has been
facilities (Radys Children’s’ Hospital, We ask the families to come along a pediatric nurse for over 12 years.
care? Each of these stages requires have undergone radiation in the past population and families. The thought
Kaiser Permanente, and Balboa with the patient to the treatment She began her nursing career at UCLA
a different approach to patient care. and return for additional treatment of becoming a pediatric radiation
Medical Center just to name a few), room, to observe what is involved Mattel Children’s Hospital and went Tailoring care to the time cycle of because of disease progression and oncology nurse never crossed my
the UCSD radiation oncology team in the treatment setup, and most on to become a circulating and scrub the disease provides individualized the need for pain relief. The care mind in nursing school. Gratefully,
and UCSD pediatric anesthesia team. importantly to provide support nurse at Children’s Hospital Los Angeles. meaningful and compassionate care. team allows extra time for these my five-year-old patient Robert
The nurse coordinates central line to their child. In certain cases, we After a year of working in the OR, she We meet many children that appointments. Extra time is used to sparked a fire in my heart that will
placement, chemotherapy schedules, have the parents speak to their child became a pediatric radiation nurse are newly diagnosed with cancer. assist with positioning, for addressing never fade and now I cannot imagine
assist with transportation, manage over the microphone as the child at CHLA and was awarded the Daisy Typically, these patients and families medication needs, and sometimes, to being anything other than a pediatric
side-effects, and provides guidance undergoes treatment. We strive Award. She moved to San Diego in 2010 have had minimal exposure to the be a shoulder to cry on. The nurse oncology nurse.
to create a safe, calm and trusting
and returned to UCSD as the pediatric hospital setting and staff. Many of
environment for both the patient
nurse in radiation oncology. Sofia them have endured multiple MRIs, Pictured left to right:
is a Certified Pediatric Hematology CTs, surgeries, blood transfusions, Mario Moreno, Radiation Therapy Technologist (RTT), Asim
and their parents. The staff also Oncology Nurse and is a member of the
understand if the patients do not chemotherapy within a short amount Billoo, RTT, Sarah Galbraith, RTT, Katie Newton, RTT
Association of Pediatric Hematology
want to have family present, this is of time prior to arriving at radiation
Oncology Nurses.
especially true for teenage and young oncology. What they thought was a
adult patients who want to maintain routine examination for a stomach
a sense of control and independence. ‘bug’ or sinus infection resulted in
In addition, we allow parents to a devastating diagnosis of cancer.
accompany their child to the They are in shock and we must
treatment room if the child requires be prepared to handle and address
anesthesia for treatment. This allows their needs. The staff understand
for an extra layer of comfort and that the family and child may be
reassurance for the child. We advise overwhelmed and frightened. As the
the parents, grandparents and siblings nurse, I coordinate with our social
that it is ok to hold their child’s/ worker to meet with the family to
sibling’s hand and tell them you love assess their social, emotional and
spiritual needs. I collaborate with
the radiation therapists to coordinate
Maycie Whelan, RTT (left) appointment times that work best
Chelsea Klika, RTT (right) with the patients and families. In
14 U C S D J O U R N AL O F NU RS ING | S P RING 2018 15
C O N T I N U O U S Q UA L I T Y I M P R OV E M E N T
The Implementation of an ICU Diary Program
to Prevent Post-Intensive Care Syndrome
By: Truong-Giang Huynh, BSN, RN, CCRN
H
ospitals throughout the US are after surviving an ICU stay.1
often pressured to focus their The term post-intensive care
time and energy on measures syndrome (PICS) and post-intensive
that provide immediate outcomes care syndrome-family (PICS-F) were
such as discharge timeliness or coined to describe the symptoms
infection control practices. Although patients and families experience after
they are very important, strategies are their ICU stay. Many European
rarely aimed at improving long-term countries have been writing ICU
outcomes for patients admitted to an diaries for over 20 years to thwart ICU staff practicing writing diary entries.
intensive care unit (ICU), including some of the symptoms associated
oncology patients. Nurses in the with PICS/PICS-F. Symptoms of
Jacobs ICU at UC San Diego Health PICS/PICS-F include but are not
are on the cutting edge in addressing limited to post-traumatic stress the ICU can reconstruct their illness implementation. The first was
this problem through the disorder, anxiety, ICU-acquired narrative with day-to-day accounts understanding how hospitals often
implementation of the ICU diary weakness, and cognitive from both the nurses as well as their cite having a difficult time
program. dysfunction.2,3 family and friends’ accounts. implementing change unless they can
Numerous studies have explored Compared to European countries, After being introduced to PICS/ identify something that sticks with
the long-term lasting effects an ICU ICU diaries are relatively new in the PICS-F, and learning how ICU the audience.5 The second was that
stay has on patient survivors. Similar United States. Their use with Truong-Giang Huynh, BSN, RN, CCRN diaries could mitigate PICS/PICS-F, nurses as a group tend to be more
studies have also been conducted on oncology patients is rare. The impetus is the Assistant Nurse Manager for the Jacobs ICU team members conservative and avoid change
the lasting effects ICU patient family to implement diaries for patients and the Jacobs Medical Center 3GH-
(previously Thornton ICU) decided compared to teachers, information
ICU. He loves learning, innovation,
members’ experience. Both patients their family members was to fill in that caring for the patient in the specialists, and scientists.6 Armed
and motivating nurses. Giang holds
and families have shown to be at great potential gaps in their memory with Bachelor’s degrees in both Biology and
immediate ICU environment was with this knowledge, the team
risk for developing new or worsened clinician and family input4. Nursing. He will be graduating with his not enough. A team of four nurses developed an all-inclusive 4-hour
physical, cognitive, or mental illness Ultimately the patient after leaving Master’s in Nursing from Point Loma (Giang, Alice, Sam, and Miranda) in-person class on ICU diaries.
Nazarene University in the Spring of decided implementation of an ICU The team established a mandatory
2018. In his spare time, you’ll find him diary program in their ICU was ICU nurse Allison Riley writing an ICU
taking his wife on dates, woodworking, imperative to help offset the long- diary journal entry for her patient.
or learning how to garden. lasting effects of an ICU stay. The
team applied and was accepted into
the American Association of Critical
Care Nurses Clinical Scene
Investigation Program, where
evidence-based practice tools and
strategies were taught and applied.
The development of the ICU
Diary Program required a multi-stage
process. The cover and theme of the
ICU diary was “your stay, your story.”
This captivating slogan was branded
all over notebooks, pens, mousepads,
Far left: ICU nurses in the ICU diary
t-shirts throughout the unit to
class practice writing diary entries.
stimulate interest and ultimately
create buy-in.
Left: The ICU diary and pen provided to Several variables had to be
patients and family members, created addressed within the ICU diary
by the Jacobs/Thornton ICU diary team. group prior to project education and
16 U C S D J O U R N AL O F NU RS ING | S P RING 2018 17
class. The class included these the diary as often as they wished. post-intensive care syndrome for REFERENCES:
components: PICS/PICS-F While staff wrote messages of caring, both patients and families. UC San 1. Needham DM, Davidson J, Cohen H,
introduction, the history of ICU families were encouraged to write Diego was so supportive of the pilot Hopkins RO, Weinert C, Wunsch H, et al.
diaries, what to include and exclude similar messages that would help program in the Jacobs/Thornton Improving long-term outcomes after
from the ICU diary, how patients are reconstruct the timeline of events ICU that all other ICUs within the discharge from intensive care unit: report
screened and debriefed for PICS in meaningful to the patient. These organization are adopting the practice from a stakeholders’ conference. Critical
the post-ICU recovery clinic, events could have included entries in the summer of 2018. The ICU Care Medicine. 2012;40(2):502-9
measurement of the project’s such as a political elections, football Diary Program also falls in line with 2. Jones C, Backman C, Capuzzo M,
outcomes data. game outcomes, or missed birthdays. the latest recommendation from the Egerod I, Flaatten H, Granja C, Rylander
The team established a mandatory Entries describing their agitation and 2017 Family-Centered Care C, Griffiths R. Intensive care diaries
class. The class included these required restraint usage could help Guidelines published by the Society reduce new onset post traumatic stress
components: PICS/PICS-F clarify any false memories or of Critical Care Medicine as a means disorder following critical illness: A
introduction, the history of ICU thoughts patients might have to improve patient and family randomised, controlled trial. Critical
diaries, what to include and exclude experienced. outcomes. Care. 2010;14(5).
from the ICU diary, how patients are In addition to providing families
3. Hermans G, Van den Berghe G. Clinical
screened and debriefed for PICS in with a diary and pen, an instant
review: Intensive care unit acquired
the post-ICU recovery clinic, camera was made available in case
weakness. Critical Care. 2015;19(274).
measurement of the project’s family members wanted to capture
outcomes data. As part of the class, their environment or care team with 4. Huynh TG, Covalesky M, Sinclair S,
the team empaneled four previous their permission. When patients were Gunter H, Norton T, Chen A, Yi C.
ICU patients admitted to the ICU transferred or discharged out of the Measuring outcomes of an intensive care
ICU nurses in the ICU diary class practicing a diary entry. and their family members, who ICU, the ICU diary was given to unit family diary program. Advanced
shared recollections from their ICU them for their keeping. The ICU Critical Care. 2017;28(2).
stay. These stories included having Diary Program Team kept track of 5. Gladwell M. (2000). The tipping point:
many false memories, anxiety over each ICU diary patient and referred How little things can make a big
memory losses and gaps, them all to the post-ICU recovery difference. New York:Little, Brown and
posttraumatic stress, and lengthy clinic. A physician from the clinic Company.
physical recoveries still existent years would call to set an appointment to
ICU nurse managers practicing writing a diary entry. later. Each panel member endorsed follow up with the patient, typically 6. Kalisch B, Curley M. (2008).
implementation of the ICU Diary 30 days after their hospital discharge Transforming a nursing organization.
Project since they confirmed they to debrief their stay. This included a JONA, 38(2): 76-83.
wished they had some type of physical, mental, and cognitive
support during their ICU stay. follow-up as well as reviewing the
The interactions between the ICU diary with the patient.
patient and family member panel The team measured two
with nurses was very emotional. outcomes with the project, rates of
There were very few dry eyes, which post-ICU recovery clinic referrals as
directly corresponded with responses well as family satisfaction with care
from many course evaluations. Many and decision-making scores in their ICU Nurse Aaron Poindexter writing a diary entry for his patient
nurses responded that the class ICU. Referrals more than doubled
renewed their sense of caring and with the implementation of the ICU
empathy. After all ICU frontline staff diary program and family satisfaction
completed the ICU Diary Program scores marginally increased. Though
class, the first ICU diary was there was not a significant increase in
implemented in June, 2016. family satisfaction scores, this could
The expectation was that the staff be attributed to either a high baseline
nurses would initiate an ICU diary benchmarking score in the high 90th
on any patient expected to stay in percentile compared to similar units
the ICU for more than 2 days and in the world, or simply choosing the
had the potential for a memory gap. wrong measured outcome. 4
Memory gaps included scoring The ICU Diary Program had
positive on delirium assessments, many successful secondary outcomes.
being intubated and/or sedated, or The ICU Diary Project was well
having procedures requiring received by patients and families.
moderate sedation. Front-line staff were instructed how
Staff members were instructed to to connect to patients on a more
write at least one handwritten entry human level rather than a standard
per day. Family members were also provider-to-patient connection,
encouraged to write to the patient in helping to mitigate the effects of
18 U C S D J O U R N AL O F NU RS ING | S P RING 2018 19CO N T I N U O U S Q UA L I T Y I M P R OV E M E N T
Post Survey Confidence Results
Implementing Proactive Code Nurse Rounds to
Decrease Delay in Rapid Response Activation
The data clearly shows
that nurses on the units
find proactive rounds
By: Mary Hellyar, MSN, RN, CNS helpful and that it has
helped them escalate
care when indicated.
ORIGIN to identify patients at a high risk for
Late in 2015, three events deterioration. Once identified, the
occurred, signifying the Thornton code nurse and the charge nurse or
ICU (TICU) code team’s need to bedside nurse would evaluate the
initiate proactive rounding. First, patient together. This proactive
there was a joint reflective practice rounding fostered collaboration and Finally, proactive rounding has been correlated with a reduction in
meeting between the nurses on 2East real time peer review and education. Code nurse in action. delayed rapid response activation and an increase in the percent
and Thornton ICU, in which nurses If the patient met criteria for a rapid of patients that survive a Rapid Response Team (RRT) or code
from both units expressed a desire for response, it was called. This was done rounding by the initial TICU code through discharge.
the code nurses to consult with the to ensure the formal rapid response nurse, it has been established as an
unit charge nurses to identify patients process remained intact and to allow expectation for the Sulpizio
that would benefit from early tracking through the I-report system. Cardiovascular Center and Hillcrest
intervention by the code nurses. Any process issues were resolved Medical Center code teams.
Second, there was a mock Code Blue through collaborative reflective
called while the TICU code team practice. OUTCOMES
was engaged in another rapid Proactive rounding continued
when the code team unit expanded Early identification of sepsis
response. Due to competing Mary Hellyar MSN, RN, ACNS-BC, CCRN symptoms is critical with oncology
priorities, the back-up team’s to the new Jacobs Medical Center
(JMC) and now includes the women
has been a Critical Care Clinical Nurse and blood marrow transplants (BMT)
response time was delayed. Third, the Specialist within the oncology service patients due to their
code blue team noted an increase and infants units. Additionally, line since 2016. She started her career
proactive rounding is completed immunocompromised state. These
with “delay in rapid response with UCSD Health in 2002 and prior
patients can decompensate rapidly,
activations” throughout the hospital. twice per shift with more focused to her current role, she was the Nurse
rounding on patients who have been Manager for Thornton Intensive Care
thus prompt identification and
In response to the three factors utilization of Code Sepsis is crucial.
listed above, the code nurse was recently transferred from the Unit. Mary has been a nurse for over
Intensive Care Unit (ICU), high-risk 29 years. She earned her ADN in 1989 BMT nurses are trained to identify
relieved of all other responsibilities in and initiate Code Sepsis when the
order to focus on offering assistance, obstetrical patients, and a new from San Bernardino Valley College,
population of oncology patients a Bachelor’s Degree in Business and patient meets Severe Sepsis Criteria.
education and providing peer review Management from the University of BMT is the biggest utilizer of
to other units. They began rounding receiving Chimeric Antigen
Receptor T-Cell (CAR-T) therapy.
Redlands in 2002, and MSN/CNS from Code Sepsis. Between October 2016
once per shift and had informal Point Loma Nazarene University in 2013. until July 2017, the unit called 75
discussions with unit charge nurses With the success of proactive
Code Sepsis and of those, only 2
patients did not survive until Delay in Activation Data
discharge. Due to the collaboration
between Code Nurse and BMT
La Jolla Code Sepsis iReports by Unit
nurse through proactive rounding,
October 2016- July 2017 the sepsis mortality rate has
continually decreased since
implementation in early 2017.
BMT is the biggest utilizer of Code
Sepsis. Between October 2016 until
July 2017, the unit called 75 Code
Sepsis and of those, only 2 patients did
not survive until discharge. Due to the
collaboration
20 U C S D J O U R N AL O F NU RS ING | S P RING 2018 21I N N OVAT I O N S I N O N C O LO GY C A R E
The Comprehensive Breast Health Center
at the Koman Family Outpatient Pavilion
By: Cecilia Kasperick MSN, RN, CNL
F
or many years oncology for natural light and the “open
nurses have collaborated concept” floor plan allows patients to
on patient care at Moores easily transition between treatment
Cancer Center, but for the first areas. The overall feel of the space
time, nurses who specialize in is inviting, and reflects the care,
Breast Health will be housed under integrity and professionalism
one roof. The third floor of the characteristic of oncology nursing. UCSD CBHC ACS Walk Team
Koman Family Outpatient Pavilion Most of the nurses working in
(KFOP) has casually been referred the Comprehensive Breast Health
to as “a one stop shop” for patients Center are Oncology Certified mental and emotional needs of our Survivorship care and community “The OP is an ideal environment to
diagnosed with breast cancer, or and complete annual continuing patients. Patient testimonies, and outreach are also long standing collaborate and provide exceptional
experiencing breast health issues. education. For many years, breast letters submitted to “We Listen,” traditions for the breast team. patient care.” “We are excited to
The new Comprehensive Breast team medical/surgical RN’s have assure us we are on the right track. Annually our interdisciplinary be a part of something bigger
Health Center (CBHC) will provide excelled in patient education. They As a matter of fact, every department team, along with patient “survivors” than ourselves.” “I look forward to
services for all dimensions of breast continually create resources to ensure affiliated with breast care has received & their families, fundraise and collaborating more closely with other
health, including: breast radiology new knowledge and innovations compliments, and we strongly believe participate in the “American Cancer breast oncology nurses;” and “This is
(mammograms, ultrasounds, MRIs, are incorporated, and they teach Cecilia Kasperick MSN, RN, CNL our move to the OP will enhance Society walk: Making Strides Against a great opportunity to enhance our
nuclear medicine & breast biopsies), complex subject matter in a way that is the Breast Cancer Nurse Navigator at
patient experience and satisfaction. Breast Cancer” and “Padres Pedal the patient’s experience.”
medical and surgical oncology clinics,is easy for patients to understand. UC San Diego Moores Cancer Center.
Recent patient feedback has Cause.” Both of these organizations In summary, opening the
a dedicated infusion center, same-day Our Infusion Center nurses have a She received her master’s degree in
included statements such as: fund breast cancer research and Koman Family Outpatient
surgery operating suites, an in-house long history of conducting research,
nursing from the University of San Diego,
“I just cannot say enough good patient services. In 2018, as we “rub Pavilion- Comprehensive Breast
pharmacy, and ancillary services, suchcreating process improvement
and has worked at UCSD since 2007.
things about the breast cancer team. elbows” in our new space, we look Health Center, enables nurses to
Cecilia has spent the majority of her forward to growing these teams and embrace the essence of our Nursing
as social work, genetic counseling, projects, and presenting their results career working with oncology patients, The professionalism, thoroughness,
pain management and physical/ at national conferences. As our work kindness, warmth, and friendliness, increasing our CBHC presence in Professional Practice Model, where
and is passionate about preventive care,
occupational therapy. Truly, this is aspaces merge, and we interact on a not to mention the “make things the community. “our focus on developing caring
early detection and balanced living
COMPREHENSIVE Breast Health daily basis, we hope to collaborate throughout treatment. happen” attitude of (this team), has Nurses who work in the OP relationships with patients, families,
Center. more, sharing our strengths and been absolutely remarkable. I can breast center where given the each other and ourselves allows us to
initiating joint only imagine what good things are opportunity to share thoughts about create an environment where feeling
projects. Infusion ahead!” our move. This is what they said: cared for is an everyday experience.”
“(They) are truly amazing - so professional, center and clinic “I always expect to feel scared
knowledgeable, terrific bedside manner staff will share or sad when I come here, but the 2017 UCSD Padres Pedal the Cause CBHC Team
a break room, edge” treatments are discussed, and opposite always happens. I feel
and topnotch in every way. Could there so undoubtedly individual treatment plans emerge. hopeful and really lucky that I get to
ever be a better team? Not on my new friendships Collaborative care and “personalized receive my care at UCSD.”
book and I’m glad they’re leading the and professional medicine” are deeply embedded in “(They) are truly amazing - so
collaborations will the culture of the CBHC. Sharing professional, knowledgeable, terrific
way on this new journey in my life!” emerge. space on the third floor will enhance bedside manner and topnotch in
Nurses in the this practice and support cohesive every way. Could there ever be a
Outpatient Pavilion patient care. better team? Not on my book and
For the past 3 years, (OP) also have the opportunity to Each department affiliated with I’m glad they’re leading the way on
representatives from the cancer participate in interdisciplinary breast breast healthcare hold national this new journey in my life!”
center Department of Nursing conferences. Once a week, physicians, accreditations. We are recognized “Kudos and hats off to all who
have been involved with planning advanced practice providers, nurses, as a “center of excellence” by the have already touched the hearts of
this facility; and nurses are excited clinical trial coordinators, genetic National Cancer Institute (NCI) and both my husband and I - certainly
to play a significant role in this counselors and social workers the National Accreditation Program all of which reflects the compassion,
expansion. “Warm,” “beautiful” and meet to discuss each new patient. for Breast Centers (NAPBC). We care, and skills of this incredible
“cutting edge” are words they have National Comprehensive Cancer treat not only patient’s physical UCSD group. Thank you for
used to describe the environment. Network (NCCN) guidelines are bodies, but strive to provide holistic partnering with me on this next
Floor to ceiling windows allow reviewed, best practices and “cutting care, encompassing the physical, chapter of my life’s journey!”
22 U C S D J O U R N AL O F NU RS ING | S P RING 2018 23I N N OVAT I O N S I N O N C O LO GY C A R E
assistance with ventilation they are
transferred to the Intensive Care
CAR-T Therapy: A Novel Treatment for Patients Unit.
Neuro-toxicities can present as
mild to life threatening. Mild
with Relapsed Lymphoma or Leukemia toxicities can include somnolence,
confusion, encephalopathy that can
progress from mild, where it is not
limiting activities of daily living, to
By: Aran Tavakoli, MSN, RN, CNS severe disorientation, obtundation or
stupor, combative delirium, seizures,
and/or fatal brain swelling. Neuro-
toxicities may mimic signs and
symptoms of a stroke including
P
atients with relapsed or Neelapu SS, Bartlett NL, et al, 2017). dysphagia and acute change in level
refractory-to-treatment In adult and pediatric heavily of consciousness. (Brudno
Leukemia or Lymphoma face pretreated relapsed refractory ALL, Kochendefer, 2016). All patients have
dire mortality rates and rarely achieve high remission rates of 67-93% have a neurology consult and examination
BMT Team
disease free outcomes. The majority been reported (Frey, 2017). These are so that a baseline is established,
of adults with acute lymphoblastic outcomes that have not been seen for before needing neurology’s services
leukemia (ALL) will relapse at some these diseases, ever. for an acute change. indicated for certain pediatric and In summary, CAR-T therapy has
point and up to 25% have resistance CAR-T uses advanced cell Because of the severity of the side young adult patients (up to age 25) significant life threatening side-
to treatment and will die of their transfer, where the patient’s own effects and unique patient with a specific form of acute effects, but once these side effects
disease (Up to Date, ALL 2017). Less immune system cells are collected via management, a close relationship lymphoblastic leukemia (ALL). On resolve, patients recover and have a
than 10% of patients with relapsed apheresis and shipped to a drug between the BMT unit and the ICU October 18, 2017,Yescarta higher chance at long term disease-
diffuse large B cell lymphoma company. The drug company then has developed. Prior to admission, (axicabtagene ciloleucel) by Kite free survival than in the past. These
(DLBCL) will experience prolonged isolates the T-Cells and exposes them the ICU is notified of these patients Pharma Inc., the CAR-T therapy new immunotherapy treatments are
disease-free survival with second-line to a virus that has been reprogramed and the patient management guide is being trialed at UCSD, was approved improving the odds and the
treatments. Though, over time, with different content that is no sent to nursing and the intensivist. to treat adult patients with certain longevity of responses to these
advancements have been made in the longer infectious. The viral vector RRT nurses proactively round on types of large B-cell lymphoma who treatments will continue to be
treatment of this disease, the majority delivers a message to the T-cells to the patient while they are on the have not responded to or who have monitored as more patients are
of patients are not cured (Up to attack leukemia and lymphoma cells. Aran Tavakoli, MSN, RN, AOCNS BMT unit. Then, when a patient is relapsed after at least two other treated.
Date, Lymphoma 2017). These reprogramed T-cells are grown is an Oncology Clinical Nurse Specialist. transferred to the ICU, BMT nursing courses of treatment.
A new therapy called Chimeric in culture, frozen and shipped back
She has worked at UCSD Health since staff does reverse proactive rounds.
Antigen Receptor T-Cells (CAR T) to UCSD (Frey, 2017).
2010. She earned her Bachelor’s in The BMT resource nurse will check
Nursing from Loma Linda University and on the ICU nurse each shift, see the
could improve the survival of patients After receiving conditioning her Master’s in Oncology Nursing from
with these diseases as well as other chemotherapy, the patient’s cells are patient, and answer questions about
UCLA. She has been actively involved in
hematologic malignancies (e.g.: defrosted at the bedside and infused oncology-specific care or treatments.
the Oncology Nursing Society, holding
multiple myeloma). CAR-T belongs through a central line. This is all very local and national leadership positions
When patients have life threating
REFERENCES: in adults. Lowenberg, B. ed. UpToDate.
to a group of therapies called anti-climactic. What is climactic, are and contributing to national think tanks
complications it is critical that the
Brudno, J.N., & Kochenderfer, J.N (2016). Waltham, MA: UpToDate Inc. http://www.
Immunotherapy that uses the help of the acute side effects patients can get on leadership. Aran is published and has medical teams are communicating
Toxicities of chimeric antigen receptor T uptodate.com (Accessed on October, 20,
a patient’s own immune system to from this treatment. Patients can have given presentations at local and national with each other. Patients may need
cells: Recognition and management. 2017.)
destroy cancer cells. The responses so severe cytokine release syndrome and conferences. Her current interests to be started on high doses of
Blood, 127, 3321-3330. Doi:10.1182/
far to this therapy, used after all other neurotoxicity that require care in the include care of the patient receiving methylprednisolone, but only at the
blood-2016-04-703751 Locke FL, Neelapu SS, Bartlett NL, et al.
treatments have stopped working, Intensive Care Unit (ICU) including
immune effector cells, oncology nursing correct stage of toxicity. Because
Primary results from ZUMA-1: a pivotal
have been remarkable for both adults vasopressors and mechanical
education and improving quality nursing patients can progress quickly to
care. Freesman, A.S., & Friedberg, J.W. trial of axicabtagene ciloleucel (Axi-cel;
and children. (NCI, 2017). ventilation. system failure, the BMT team needs
Treatment of relapsed or refractory KTE-C19) in patients with refractory
Initial CAR-T outcomes are Cytokine release syndrome can to be continuously updated on the
diffuse large B cell lymphoma. Negrin, aggressive non-Hodgkin lymphoma
promising. It has been reported in include the following symptoms: patient’s condition if it worsens to
R.S. ed. UpToDate. Waltham, MA: (NHL) Proceedings of the 107th Annual
the literature that there is 40-50% Elevated temperatures, chills and provide treatment recommendations.
UpToDate Inc. http://www.uptodate.com Meeting American Association Cancer
complete response (CR). In the rigors, tachycardia, hypotension, Though these agents have been
(Accessed on October 20, 2017.) Research; Washington (DC): AACR; 2017.
study that was open here at UCSD, hypoxia, generalized body edema used at UCSD on clinical trials,
p. CT019.
phase 2 ZUMA-1 for patients that from capillary leak syndrome, recently 2 drug companies have
Frey, N. (2017). The what, when and how
have DLBCL , the primary analysis headache, rash, nausea, weakness and received approval for their product
of CAR T cell therapy for ALL. Best National Cancer Institute (NCI). CAR T
of 101 patients showed an overall increased C-reactive protein (Brudno through the Federal Drug
Practice & Research Clinical Hematology, Cells: Engineering Patients’ Immune Cells
response rate of 82%, including a Kochendefer, 2016). The patient’s Administration (FDA). The first
30: 275-281. to Treat Their Cancers. https://www.
complete response (no evidence of temperatures can also rise to greater CAR-T therapy approved by the
cancer.gov/about-cancer/treatment/
disease) of 54% at greater than 6 than 103.0o F. If the patient requires FDA on August 30, 2017 was
Larson, R.A. Treatment of relapsed or research/car-t-cells Accessed on
months of follow-up (Locke FL, vasopressors to maintain perfusion, or Kymriah (tisagenlecleucel) that is
refractory actue lymphoblastic leukemia October, 20, 2017
24 U C S D J O U R N AL O F NU RS ING | S P RING 2018 25You can also read