ARTIFICIAL AIRWAYS BVE, RRT, RCP - Kevin T. Martin V7115 HC 05
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ARTIFICIAL AIRWAYS
by
Kevin T. Martin
BVE, RRT, RCP
V7115 HC 05
RC Educational Consulting Services, Inc.
P.O. Box 1930, Brockton, MA 02303-1930
(800) 441-LUNG / (877) 367-NURS
www.RCECS.com

ARTIFICIAL AIRWAYS
BEHAVIORAL OBJECTIVES
UPON COMPLETION OF THE READING MATERIAL, THE PRACTITIONER WILL BE
ABLE TO:
1. Identify the characteristics of the following artificial airways:
• Oropharyngeal
• Nasopharyngeal
• Endotracheal tubes
• Tracheostomy tubes
• Laryngeal Mask Airway (LMA)
• Esophageal-Tracheal Combitube™
• Double Lumen Endotracheal Tubes (DLET)
2. Identify the medical indications specific to each of the above listed airways.
3. Identify the clinical contraindications for each of the above listed airways.
4. Identify the quantifiable advantages and disadvantages of the above listed airways.
5. Identify clinical cautions required in the use of the above listed airways.
6. Describe an endotracheal tube changer and describe its’ use.
7. Describe the clinical general steps in tracheal tube weaning.
8. Identify and describe three stoma maintenance devices.
9. Define and explain the effects of an artificial airway on a patient’s work of breathing.
10. List the specific quantifiable conditions that require airway management.
11. List the clinical conditions that may require emergency tracheal intubation.
12. Explain the proven care necessary to prevent complications associated with artificial
airways.
13. Describe two scientific different methods of securing an endotracheal tube.
14. Describe two techniques to prevent excessive intra-cuff pressures.
15. Identify the three primary clinical emergencies the clinician may encounter when dealing
with artificial airways.
16. List the medical criteria that are factors in a patient being at greater risk for re-intubation.
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 1
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
17. Identify five general recommendations for care of the artificial airway.
18. Using critical thinking skills and the information learned in this activity, complete a
clinical practice exercise.
COPYRIGHT © OCTOBER 1985 BY RC EDUCATIONAL CONSULTING SERVICES, INC.
COPYRIGHT © April 2000 BY RC Educational Consulting Services, Inc.
(# TX 1 762 726)
AUTHORED 1985 BY KEVIN T. MARTIN, BVE, RRT, RCP
REVISED 1988, 1991, 1993, 1996 BY KEVIN T. MARTIN, BVE, RRT, RCP
REVISED 2001 BY MICHAEL R. CARR, BA, RRT, RCP
REVISED 2003 BY SUSAN JETT LAWSON, RCP, RRT-NPS AND MICHAEL R. CARR,
BA, RRT, RCP
REVISED 2006 BY MICHAEL R. CARR, BA, RRT, RCP
REVISED 2010 BY AIMEE STAGGENRORG, MA, BA, RRT
ALL RIGHTS RESERVED
This course is for reference and education only. Every effort is made to ensure that the clinical
principles, procedures and practices are based on current knowledge and state of the art
information from acknowledged authorities, texts and journals. This information is not intended
as a substitution for a diagnosis or treatment given in consultation with a qualified health care
professional.
2 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
TABLE OF CONTENTS
INTRODUCTION ...........................................................................................................................7
TYPES OF AIRWAYS....................................................................................................................7
Oropharyngeal Airways...........................................................................................................7
Nasopharyngeal Airways.........................................................................................................8
Endotracheal tubes (ETT)......................................................................................................10
Problems associated with orotracheal tubes .....................................................................14
Advantages of nasotracheal tubes over orotracheal tubes for long-term intubation .......14
Problems associated with nasotracheal tubes ...................................................................15
Tracheostomy tubes...............................................................................................................15
Purpose of design..............................................................................................................16
Inner Cannula ..............................................................................................................16
Obturator......................................................................................................................16
15mm connector ..........................................................................................................16
Neck plate or flange.....................................................................................................17
Cuffs ............................................................................................................................17
Pilot balloon.................................................................................................................17
Dimensions .......................................................................................................................17
Tracheostomy tube sizing and conversion........................................................................18
Metal tracheostomy tubes.................................................................................................20
Rusch tracheostomy tubes ................................................................................................20
Pediatric tracheostomy tubes ............................................................................................21
Speaking tracheostomy tubes ...........................................................................................21
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 3
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
Percutaneous dilational tracheostomy tubes (PDT)..........................................................22
Tracheal tube wedge.........................................................................................................23
ALTERNATIVE INVASIVE AIRWAYS ....................................................................................23
Laryngeal mask airway (LMA) .............................................................................................23
Advantages .......................................................................................................................25
Disadvantages...................................................................................................................25
Combitude{..........................................................................................................................26
Advantages .......................................................................................................................27
Disadvantages...................................................................................................................27
Contraindications..............................................................................................................27
Cuffed oropharyngeal mask airway (COPA) ........................................................................28
Placing and using the COPA ............................................................................................28
Lingual nerve injury after use of a cuffed oropharyngeal airway ....................................30
Pharyngeal-tracheal lumen airway (PtL)...............................................................................30
AIRWAY ADJUNCTS..................................................................................................................30
Tracheal tube changers ..........................................................................................................31
Stoma maintenance devices (trach “buttons”).......................................................................31
Olympic button, Kistner valve and Montgomery valve ...................................................32
Tracheostomy tube weaning........................................................................................32
GENERAL INFORMATION........................................................................................................32
INDICATIONS..............................................................................................................................33
Specific conditions that require airway management ...........................................................34
Conditions which may require emergency tracheal intubation ............................................34
4 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
CONTRAINDICATIONS .............................................................................................................35
COMPLICATIONS .......................................................................................................................35
Predisposing Factors..............................................................................................................35
Tracheal Damage...................................................................................................................35
Decrease in the effectiveness of the cough............................................................................36
Decrease in mucociliary activity ...........................................................................................36
Tracheal ulceration ................................................................................................................36
Stenosis..................................................................................................................................36
Glottis or subglottic edema....................................................................................................37
Infection.................................................................................................................................37
Swallowing dysfunction ........................................................................................................37
PREVENTION OF COMPLICATIONS.......................................................................................38
Intra-cuff pressure..................................................................................................................40
Minimal leak technique (MLT) .............................................................................................40
Minimum occluding volume (MOV) ....................................................................................41
PRECAUTIONS, HAZARDS, AND/OR COMPLICATION.......................................................42
EMERGENCIES............................................................................................................................42
Cuff leaks....................................................................................................................................42
Accidental extubation .................................................................................................................43
Obstructions................................................................................................................................44
Additional hazards or complications related to emergency airway management .....................45
Algorithm for a difficult airway .................................................................................................45
CARE OF THE ARTIFICIAL AIRWAY .....................................................................................47
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 5
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
SUMMARY...................................................................................................................................49
CLINICAL PRACTICE EXERCISE ............................................................................................49
PRACTICE EXERCISE DISCUSSION .......................................................................................52
SUGGESTED READING AND REFERENCES .........................................................................55
6 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
INTRODUCTION
T
he following material discusses types, indications, complications, emergencies and care of
adult artificial airways. The majority of the paper is devoted to endotracheal and
tracheostomy tubes as used in the acute care environment. Unless otherwise noted,
airways for the adult patient population are discussed. Unique airways used in skilled nursing
facilities, rehabilitation, and home care not discussed in this course.
TYPES OF AIRWAYS
OROPHARYNGEAL AIRWAYS
A
n oropharyngeal airway is used in an unconscious patient to reduce risk of obstructing
the airway with the tongue, or to prevent potential laceration of the tongue if the
incoherent patient has a seizure. These airways are commonly called “oral” airways.
Oral airways are used to keep the tongue from occluding the airway and as a bite block. When
properly inserted and positioned, the tongue is held up and out of the hypopharynx. The airway
is reinforced so biting cannot crush it. Oral airways have a channel through the middle or along
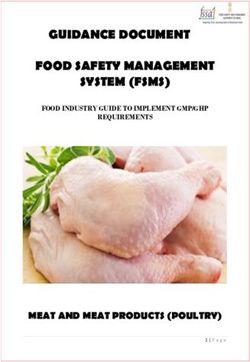
the sides to allow for suctioning of oral secretions. Guedel oral airways have a channel down the
middle. Berman oral airways have an I-beam design with side channels. Oral airways come in
sizes from 000 for neonates to 6 for adults.
Example of the Berman oral airways
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 7
duplication is prohibited by law.
ARTIFICIAL AIRWAYS
ORAL AIRWAY
Oral airways are inserted upside down from the side or top of the mouth then twisted 180
degrees around so the distal tip is positioned in the inferior oropharynx. Care should be taken
during insertion that the tongue is not inadvertently pushed down into the throat. A tongue
depressor can aid insertion. To determine proper airway size, place the airway along the cheek
and measure the distance from the corner of the mouth to the tragus of the ear (the cartilaginous
point near the opening). Tubes too long can put pressure on the epiglottis and may obstruct the
airway. A tube too short can push the tongue back and decrease ventilation. If the flange sticks
out more than a few millimeters, select a smaller airway. Oropharyngeal airways are to be used
only with the unconscious patient as they may cause vomiting and laryngospasm in the alert or
semiconscious patient.
NASOPHARYNGEAL AIRWAYS
A nasopharyngeal airway is used to relieve upper airway obstruction caused by the tongue or soft
palate falling against the posterior wall of the pharynx. These airways are commonly referred to
as nasal airways or “trumpets”. They are inserted for repeated suctioning, bronchoscopies and as
an airway for an intoxicated or semiconscious patient. They help guide catheters toward the
trachea and prevent unnecessary irritation of the nasal mucosa. It may be possible to avoid
intubation with frequent suctioning through a nasal airway in some patients. Nasal airways are
made of red rubber or silicone. They have fixed or adjustable flanges on the proximal end,
depending upon the manufacturer. One brand has an inflatable balloon at the end to ease passage
through the nose. The balloon is deflated after insertion.
8 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
NASAL AIRWAY
Nasal airways are lubricated with a sterile water-soluble lubricant and inserted through the nare.
Use a sterile 4 by 4 -inch gauze pad to smear the lubricant over the length of the airway. The
bevel should face the midline during insertion. Once in place, the distal tip is located behind the
base of the tongue like an oral airway. The length of the airway can be estimated by measuring
the distance from the tip of the nose to the tragus of the ear plus one inch. The airway must be
rotated periodically between the nares to prevent mucosal crusting. Nasopharyngeal airways
should also be removed and cleaned at least once every 24 hours. Keep the nares clean and dry
while in place.
If a nasal airway is not available an un-cuffed ET tube can be used. The length of the tube can
be cut to fit the patient’s nasopharynx. The tube connector will prevent the tube from slipping
deeper into the nasal passage. This method does present a problem. The connector’s internal
diameter is smaller than the tube and may prevent suction catheter passage and limit gas flow
rates during ventilation.
Complications of using nasal airways are bleeding, sinusitis, otitis media, and nasal necrosis.
You can avoid or decrease opportunity of these complications by using generous lubrication, and
vasoconstrictive agents.
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 9
duplication is prohibited by law.ARTIFICIAL AIRWAYS
ENDOTRACHEAL TUBES (ETT)
An endotracheal tube is indicated when a patient’s airway requires airway protection, tracheal
suctioning or when ventilation is necessary. Endotracheal tubes can be inserted nasally or orally.
Oral endotracheal (figure 1) tubes have a preformed curve at a 450 angle. Nasal endotracheal
(figure 2) tubes have a preformed curve curved at a 600 angle. Once the selected tube is in place,
the distal tip rests in the trachea just above the carina. Most have an opening (Murphy’s eye) in
the wall near the distal tip. Should the tip be occluded, ventilation may still be possible through
this opening. There also is an inflatable cuff attached near the distal end of adult tubes. Cuff
inflation seals the airway so all ventilation must occur through the endotracheal tube. The cuff is
inflated via a pilot balloon valve and line attached to the endotracheal tube. Infant tubes have no
cuff. Endotracheal tubes less than sizes 5.0 are generally uncuffed. Some 5.0 tubes are
manufactured with and without cuffs however.
Figure 1
Figure 2
There are many types of endotracheal tubes used for specific purposes. Double Lumen
Endotracheal Tubes (DLET) are special tubes that provide selective endobronchial intubation,
and independent lung ventilation. One lumen is advanced into a main stem bronchus, the other
lumen remains in the trachea for selective endobronchial intubation. Carlens tubes are used for
the left main stem bronchus and White tubes are used for the right main stem. The distal tip is
curved to enter the bronchus and there is a carinal “hook” to hold it in place. The Robertshaw
tube is used for either main stem bronchus and has no carinal hook.
10 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Carlen double-lumen endotracheal tube, with carinal hook in position.
White double-lumen endotracheal tube, with carinal hook in position.
Indications for the use of DLET:
• Isolation of one lung from another due to infection and/or hemorrhage
• Control of distribution of ventilation as in bronchopleural fistula
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 11
duplication is prohibited by law.ARTIFICIAL AIRWAYS
• Surgical opening of a major conducting airway in the cases of a large unilateral bulla or cyst
or a tracheobronchial tree disruption
• Unilateral bronchopleural lavage as a treatment for pulmonary alveolar proteinosis
• Surgical exposure to perform a pneumonectomy or upper lobe resection
• Independent lung ventilation
Contraindications of a DLET include:
• Full stomach (risk of aspiration)
• Difficult placement due to abnormal airways or lesions
• Patients who would not tolerate being off mechanical ventilation or PEEP
Points to remember 28:
• These tubes are more rigid and bulkier than standard tubes
• Must be rotated during insertion to gain proper alignment with the proper bronchus
• Fiberoptic bronchoscopy should be performed to ensure the proper placement
• The resistance to flow through each tube will be increased since each lumen is
smaller than the same size single lumen tubes
• A longer suction catheter will be needed to access the bronchial tube
Armored tubes (Figure 4) have steel wire wound through the walls. An advantage of the
armored tubes over regular ones is that they will not collapse if the patient should bite down.
They are used for surgery so the tube can be bent without kinking, also. The armored tube is the
most appropriate airway for head trauma victims and patients with frequent seizure activity.
RAE (Ring-Adair-Elwin) tubes are used for the same purpose, but they are preformed and have
no steel wire. Stainless steel tubes are used for laser surgery so the light will bounce harmlessly
off its walls.
12 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Figure 4
Preformed tubes have been preshaped for better patient comfort or security. One style has a
forward bend so that the tube can be taped to the chin. There is also a pediatric tube with a bend
for taping it to the forehead.
Guidable trigger tubes make it easier to intubate a patient with anterior larynx or to perform a
blind nasal intubation.
Figure 5
Mallinckrodt Critical Care makes several specialized tubes. The Endotrol (Figure 5) has a loop
on the proximal end. The user can pull on the loop to control the direction of the distal tip to aid
intubation. The Hi-Lo Jet tube is used for high-frequency jet ventilation. It has an extra lumen
for monitoring and irrigation. Other manufacturers make additional tubes for specialized
functions.
Experimental ultra thin-walled ETT’s have been produced for use with infants. These specially
manufactured tubes have a wall thickness of only 0.2 mm. This gives a much larger inner
diameter (ID) for the lumen. The result is a tremendous decrease in airway resistance to
breathing. Conventional 2.5 mm I.D. tubes have a wall thickness of 0.6 mm and 4.5 mm I.D.
tubes a 0.85 mm thickness. Ultra thin-walled tubes can lower resistance by as much as three
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 13
duplication is prohibited by law.ARTIFICIAL AIRWAYS
times. These tubes are not commercially available at this time; they have been “bench-tested”
only.
Problems Associated With Orotracheal Tubes 28
• They are poorly tolerated in conscious and semiconscious patients
• They are difficulty to stabilize and may be easily dislodged
• Inadvertent extubation is common
• A bite block may be necessary to prevent biting of tube
• Vagal stimulation may cause bradycardia and hypotension.
• Oral hygiene is difficult
• They require a laryngoscopy during insertion
• Patients are unable to mouth words
• Lips may be lacerated
• There is a potential for laryngeal pathology
• The tip of the tube moves when the patient’s head position changes
(1) Extension of the head moves the tip toward the oropharynx (possible
extubation)
(2) Flexion of the head moves the tip toward the carina (possible right
endobronchial intubation)
• Oral feeding is difficult
Advantages of Nasotracheal Tubes over Orotracheal Tubes for Long-Term Intubation 28
• Easier to stabilize
• May be better tolerated by some patients
• May be inserted blindly (laryngoscopy is unnecessary in most cases)
• Oral hygiene is easily accomplished
14 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
• The patient is able to mouth words
• Attachment of equipment is easier and safer; there is less torque on the trachea
Problems Associated With Nasotracheal Tubes 28
• The tip of the tube moves when the patient’s head position changes
• Pressure necrosis in area of the alae nasi may occur
• Sinus drainage may be obstructed, and acute sinusitis may result
• Eustachian tube drainage may be obstructed, and otitis media may result
• The incidence of vocal cord damage after 3 to 7 days (also seen with oral ETT’s)
increases
• Vagal stimulation is possible, but it occurs less frequently than with the oral ETT
• Skilled personnel are necessary for placement
• The nasal passage limits the tube size; a tube at least 0.5 mm ID smaller than the oral
route is required
(1) Men: 7.5 to 8.5 mm ID
(2) Women: 6.5 to 7.5 mm ID
• The angle of curvature is acute; the resistance to gas flow is increased; there is
difficulty in suctioning; and the work of breathing is increased when compared with an
orotracheal tube in the same patient
• There is a potential for laryngeal pathology
A tracheostomy tube is indicated for long-term airway management or when facial trauma or
surgery prevents the use of an oral or nasal endotracheal tube.
TRACHEOSTOMY TUBES
Tracheostomy tubes also are inserted in the trachea, but insertion is through a tracheal stoma.
They are similar to an endotracheal tube but much shorter and more rigid. Most tracheostomy
tubes have an inner and outer cannula, obturator, and inflatable cuff. Some have no inner cannula
or cuff. The obturator provides a smooth surface to ease insertion and prevent tissue and blood
debre from entering the tube during insertion. The obturator is removed when the airway is in
place. Inner cannulas can be removed and cleaned periodically. Some inner cannulas are
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 15
duplication is prohibited by law.ARTIFICIAL AIRWAYS
disposable. Most tubes also come with a decannulation plug.
The variation in tracheostomy tubes is endless. Sizes, materials, style and specific applications
differ. The practitioner must learn the basic theory of operation of tracheostomy tubes and the
wide array that exists. Basically, each tracheotomy tube consists of a neck flange, tube body and
cuff.
Low Pressure Cuffed Tracheostomy Tubes
Courtesy of Shiley - Nellcor
PURPOSE OF DESIGN
Inner Cannula
This device can be removed to clean secretions and blood from the interior surface without
removing the entire tube. Shiley manufactures tracheostomy tubes with disposable inner
cannulas.
Obturator
The obturator prevents blood or mucus from entering the tube as it is being inserted and provides
a smoothly tapered surface to facilitate introduction of the tube into the airway and is removed
when the tube is in the proper position.
15mm Connector
This is the standard connector, which allows connection to resuscitation bags and other
respiratory equipment.
16 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Neck Plate or Flange
This enables the tube to be secured around the patients’ neck with ties or collar. Some surgeons
initially suture the flange to the patients’ neck. These sutures are removed in approximately 3-5
days by the surgeon or respiratory therapist. They are replaced with the standard tracheostomy
ties or alternative commercially available ties.
Cuffs
Cuffs seal the airway to allow positive pressure ventilation and minimize the risk of aspiration of
stomach contents into the lungs. They do not eliminate aspiration; even the best cuffs have
microscopic air leakage. Aspiration of pharyngeal secretions commonly occurs with cuffed
artificial airways. Tubes that remain connected to continuous suction can suction above the cuff
and lower the risk of aspirated secretions, but these systems have not gained wide use since their
introduction and cost may be a factor. Knowing these facts, we cannot emphasize enough the
importance of oral care, oral suction and proper procedures prior to and during deflation of cuffs.
Pilot Balloon
The cuff is inflated (not foam cuffs) using a syringe. A spring-loaded one-way valve on the pilot
balloon maintains cuff inflation when the syringe is removed. The pilot balloon functions to
show an inflated, or not inflated, condition of the cuff. It is impossible to judge the pressure
within the cuff by squeezing the pilot balloon. The best practice is to use MLT (Minimal leak
technique) or MOT (minimal occlusion technique) to determine the lowest amount of air aspirated
in to seal the cuff.
DIMENSIONS
Anatomic variations of neck length, location and diameter of the tracheostomy incision
are factors that affect tube sizing for patients. Surgeons hope to limit the damaged area by
avoiding large stoma sites and excessively large tubes. Generally, a 10 mm OD (7 mm ID) tube
is optimal for women and 11 mm OD (8 mm ID) tube for men. French sizing is based on the
circumference of the outer surface of the tube. Conversion to French formula: Maximum
diameter (Fr) = ID (mm) x 3. Roughly the size of the trach or ETT should be 2/3 the internal
diameter of the trachea. Tube length has been standardized, but extra long and adjustable tubes
are available which are helpful in the morbidly obese patient. The intratracheal part of the tube
should be straight and somewhat flexible. A desirable tube has a smooth curvature with a small
radius between intratracheal and extratracheal limbs. This permits an entrance of close to 90
degrees, lessening pressure on the longitudinal aspect of the tracheal stoma. Once in the trachea,
the tube sides or tip should not produce pressure points on the tracheal wall. In addition to the
tracheal wall, the esophagus and major blood vessels are at risk for erosion. The flange should
emit gentle yet firm fixation of the tube. Excessive movement of the tube increases the potential
for lesions especially at the stoma level. This is the rationale for securing the ventilator circuits
with a Velcro wrap during mechanical ventilation and using tracheostomy collars instead of T
adapters when a precise FIO2 is not required with aerosol therapy. Some tubes have adjustable
flanges to change the extratracheal dimension.
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 17
duplication is prohibited by law.ARTIFICIAL AIRWAYS TRACHEOSTOMY TUBE SIZING AND CONVERSION French Jackson Trach Size Size Tube Size ETT Size mm OD mm ID Patient age 13 00 00 2.5 4.3 2.5
ARTIFICIAL AIRWAYS
Fenestrated Tracheostomy Tube
Courtesy of Mallinckrodt - Nellcor
Schematic Fenestrated
cuffless Model 304
Neck plate, moving around 2 axis
15mm connector of inner cannula Fenestration of outer cannula
Outer cannula
Decannulation plug blue
Fenestration of inner cannula
Outer diameter of inner cannula
Inner diameter of inner cannula
Courtesy of Kapitex Healthcare
Lanz tubes have pressure controlling pilot balloons, which are easily recognized by the presence
of a large floppy PVC cover over the pilot balloon. The compliance of the pilot balloon limits the
pressure in the cuff to 20-25 mmHg.
Kamen-Wilkinson or Bivona Fome Cuff tubes (following picture) have cuffs that contain
polyurethane foam that expands when the pilot tube is open to the atmosphere. It operates
opposite to other cuffs. For insertion, the cuff is actively deflated by use of a syringe to remove
the air. After insertion, the pilot tube, is opened, and the cuff expands until it contacts the tracheal
wall. As the cuff expands, the pressure it exerts on the trachea decreases. This means that the
smaller the tube with respect to the airway, the less pressure is exerted on the airway wall. There
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 19
duplication is prohibited by law.ARTIFICIAL AIRWAYS
is no pilot balloon and the pilot tube should never be plugged.
Obturator
Inflation Line Connector
Flange
Tube Ties
Fome-Cuff
Side-Port Connector
Courtesy of: Portex Limited, Hythe, Kent CT216JL.uk
Metal Tracheostomy Tubes
Bausch and Lomb continue to carry stainless steel and sterling silver tracheostomy, speaking and
laryngectomy tubes. The advantages of these tubes is that the tissue growth into the cannula is
reduced, thin wall construction minimizes bulk, which makes concealment easier and is more
comfortable to the patient, and precise mating of tube and cannula eliminates the space where
secretions can build up. The disadvantages include granuloma formation, tracheal wall erosion
and tube occlusion against the tracheal wall. Steel or Silver tubes can not be used if mechanical
ventilation is required.
Rusch Tracheostomy Tubes
Tracheoflex® tracheostomy tubes are PVC siliconized and stainless steel spiral reinforced. The
flange and neckband are adjustable. It is X-ray opaque and has a low volume cuff. Rusch also
offers Laryngoflex® reinforced tubes for laryngectomy. The significance of knowing the
composition of these tubes is that you cannot take these patients for a MRI without changing
their tracheostomy tube!
Tracheoflex
Courtesy of Rusch, Inc.
20 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Pediatric Tracheotomy Tubes
Tracheostomy tubes began their most prevalent use with pediatric patients during the diphtheria
epidemic in the early 1800’s for upper airway obstruction. In 1932, a tracheotomy was performed
for those with poliomyelitis for prophylactic and therapeutic indications, not just obstruction of
the upper airway. After years of evolution and now increased need due to improved neonatal
outcomes, pediatric tracheostomy tubes are available in many sizes, lengths, materials and
configurations. These smaller tracheostomy tubes are usually a single-cannula tube without an
inner cannula or a cuff. There are tight to shaft (TTS) cuffed tubes made by Bivona which are
instilled with sterile water used for children who can be off their ventilator periodically. Older
children who require ventilation probably need cuffed tracheostomy tubes to achieve an adequate
seal. Children who do not require mechanical ventilation should have tracheostomy tubes that
allow airflow around the tube in order to reduce the chances of tracheal wall damage. Fenestrated
tubes are not recommended for pediatric use as the opening may be obstructed with granulated
tissue.
Pediatric And Neonatal Tracheostomy Tubes
Courtesy of Shiley - Nellcor
Speaking Tracheostomy Tubes
These tubes, such as the Pitt Speaking Tube, have a separate pilot tube that directs compressed
gas to an exit point just above the cuff that passes through the vocal cords. This allows the
patient, with practice, to coordinate speech.
Laryngectomy tubes are shorter than standard tracheostomy tubes from the outer neck skin to the
trachea. Removal of the larynx obviates the need for a cuff on these tubes. They are generally
rigid in design and have three pieces. It is important to keep in mind that those having had a
laryngectomy have had the connection between the upper and lower air severed, and emergency
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 21
duplication is prohibited by law.ARTIFICIAL AIRWAYS
responses must be directly to the stoma and not the nose and mouth.
Several manufacturers produce “talking” tracheostomy tubes or devices to allow vocalization.
Talking trach tubes have an additional line similar to the pilot balloon line. When the line is
attached to a gas source, flow is released above the cuff. This produces flow through the vocal
cords even when the cuff is inflated. The patient can therefore communicate even though the
airway is sealed. The Passy-Muir Trach Speaking Valve and Olympic Trach-Talk are one-way
valves attached to a tracheostomy tube. They allow flow on inspiration through the tube but force
expiratory flow through the vocal cords. The cuff must be deflated for these devices and should
not be used if the patient is asleep.
PMV 007 (Aqua)
PMV 005 (White) PMV 2020 (Clear) with
the PMA 2020-S Adapter
PMV 2000 (Clear) with
the PMV Secure-It{
PMV 2001 (Purple) with the
PMA 2000 Oxygen Adapter
Passy-Muir Tracheostomy and Ventilator Speaking Valves
Courtesy of Passy-Muir
Percutaneous Dilational Tracheostomy Tubes (PDT) 28
Advantages when performed properly as compared with surgical tracheostomy are:
• No operating room required
• No need to move high-risk patients
• General anesthesia not required
• Decreased incidence of pneumothorax, bleeding, and stenosis
• Stoma closes quickly after decannulation with less scar tissue formed
Disadvantages are:
• If inadvertent decannulation occurs before maturation of tracheostomy tract (2 weeks),
reinsertion may lead to complications such as bleeding and tracheal trauma. Oral
intubation is recommended in this case.
22 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
• Should not be performed on patients who are morbidly obese, have burns to the neck,
have bleeding disorders, have anatomic abnormalities of the trachea or cervical region,
or had a previous tracheostomy.
Product Features
• Tapered distal tip and inverted cuff shoulder provide easy insertion
• Cylindrical cuff provides low-pressure seal to help protect sensitive tracheal tissue
• Integral snap-lock connector facilitates changing the inner cannula
• Swivel neck flange affords greater comfort and easier cleaning while buffering
movement
Tracheal Tube Wedge
Used to detach respiratory equipment and prevent needless tugging and pulling to disconnect
trachs and other respiratory equipment.
ALTERNATIVE INVASIVE AIRWAYS
T
he Laryngeal Mask Airway (LMA) is sometimes called “mask on a tube”. An inflated cuff
forms a low-pressure seal in the laryngeal inlet. ACLS 2003 guidelines have deemed the
LMA as an additional technique for invasive airway control and ventilation.
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 23
duplication is prohibited by law.ARTIFICIAL AIRWAYS
There are several LMA products including the LMA-Classic™, LAM-Flexible™, LMA-
Unique™, a single-use LMA, the LMA-Fastrach™, and an LMA designed to facilitate
endotracheal intubation. These devices are latex-fee.
LMA Size Patient Size
1 Neonates and infants up to 5 kg.
1½ Infants between 5-10 kg.
2 Infants and children between 10-20 kg.
2½ Children between 20-30 kg.
3 Children over 30 kg. and small adults
4 Normal and large adults
5 Large adults
The standard insertion technique is to hold the LMA like a pen with the mask aperture facing
forward and the black line on the airway tube oriented anteriorly toward the upper lip of the
patient. The tip of the cuff is then pressed upward against the hard palate, flattening the cuff
against it. The position of the mask is then verified and your index finger inserts the tube further
into the mouth. The jaw may be pushed downwards with your middle finger. The LMA is
advanced without force into the hypopharynx until a definite resistance is felt. Before removing
the hand that inserted the LMA, the other hand is brought from behind the patient’s head to press
24 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
down on the LMA to prevent displacement of the tube. The cuff is inflated with the volume
specific to the LMA size used.
Laryngeal
Advantages
• Provides a clear airway leaving hands free
• Designed for blind insertion
• Alternative for difficult or impossible intubations
• Eliminates need for use of neuromuscular blocking agents for laryngoscopy
• Can be left in place in recovery room until protective reflexes have returned
• Can be heat sterilized for repeated use
• No need for proper positioning of the airway for alignment or landmarks
• Better choice than an ETT for patient with possible unstable neck injuries or access to the
airway/patient is difficult
• The possibility of fatal errors with the LMA is much lower than with ETT
Disadvantages
• The laryngeal mask does not prevent regurgitation or aspiration
• Laryngeal spasm may occur if the patient is too lightly anesthetized during surgical
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 25
duplication is prohibited by law.ARTIFICIAL AIRWAYS
stimulation
• Bronchial secretions may irritate the vocal cords and provoke laryngeal spasm during
recovery from anesthesia
• Cost for reusable LMAs are in excess of $200.00
Obstruction may occur if:
• The Laryngeal mask is inserted incorrectly
• The Laryngeal mask is dislodged
• The epiglottis is pushed down during insertion
• The cuff is deflated before protective reflexes return
• Laryngeal spasm occurs as a result of too light anesthesia or from
Mucosal irritation from secretions
Combitube™ (Figure 6) As the name of this airway implies, it is a combination tube: a
combination of an endotracheal tube and an esophageal tube. Remember the esophageal obturator
airway (EOA)? The Combitube is a modification and advancement of that device. The
Combitube has two separate, clear, polyvinyl chloride (PVC) tubes, fused together longitudinally.
One tube is patent while the other is blind. The blind tube is longer than the patent tube and is
color-coded blue on its’ more proximal end as its’ pilot balloon. Two inflatable balloons are
located on the tube; one proximal latex 100 ml balloon that functions as the oropharyngeal balloon,
and a more distal conventional 15 ml PVC balloon. Between the balloons, on the blind-ended
tube, are eight small perforations. Each tube has a standard 15 mm connector on its’ proximal end
for connection to a breathing circuit. Like the laryngeal-mask airway, the Combitube is placed
blindly. It can be lubricated prior to insertion with avoidance of occluding the perforations,
however, this is not mandatory. The use of this airway has both a low reported rate of
complications and few published evaluations.
The Esophageal-Tracheal Combitube™ is another device that was recommended as a Class IIb
advanced airway device in the 2003 ACLS Provider Manual.
There are two sizes available: 37 Fr for patients between 4-5.5 feet tall (SA-small adult) and 41 Fr
for patients over 5 feet tall (A-adult). Either may be used for 5-5.5 feet tall individuals.
26 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Combitube – Figure 6
Advantages
• Blind placement without laryngoscope
• Unique design provides patent airway esophageal or tracheal placement
• Reduces risk of aspiration of gastric contents. Requires no restraining devices.
Disadvantages
• It’s not considered a secure airway
• Does not guard against pulmonary aspiration
• ACLS medications cannot be administered unless the trachea itself is intubated
Contraindications
Do not use in patients with:
• An intact gag reflex
• Known esophageal disease
• History of ingestion of caustic material
• Presence of upper airway obstruction
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 27
duplication is prohibited by law.ARTIFICIAL AIRWAYS
Cuffed Oropharyngeal Mask Airway (COPA)
Figure 7: Cuffed
Figure Oropharyngeal
7: Cuffed OropharyngealMask
MaskAirway
Airway (COPA)
(COPA)
Both the LMA and Combitube suffer from limitations regarding cost and training. The use of
more simple, recognizable airway adjuncts may overcome some of these problems. The recently
introduced cuffed oropharyngeal airway (COPA) (Figure 7) is a simple modification of a Guedel
airway and goes a long way to fulfilling these goals. The device is inserted like a standard oral
airway with the addition of an inflatable pharyngeal cuff and universal connector. While it was
originally developed for use during spontaneously breathing subjects under general anaesthesia,
the COPA does allow positive pressure ventilation to occur provided lung compliance is good and
airway pressures are not high. Initial work has suggested practitioners can easily insert the device
and ventilation is possible in nearly every case. There appears to be a leak in a number of patients
but this rarely impairs the ability to effectively ventilate the lungs. A larger size COPA, than
standard Guedel airway, also appears to be more effective. Further work has suggested that the
COPA, while conferring no advantage to patients if bag and mask ventilation is being done well,
does allow good ventilation if the bag and mask system is proving ineffective. Thus, while the
device confers no protection of the airway against regurgitation and aspiration, it does appear to
have some advantages over simple bag and mask ventilation if this is not being performed well.
If we accept that training all healthcare staff in the use of the LMA and Combitube is a practical
impossibility, then the COPA may represent an important intermediary between bag and mask
and more sophisticated airway devices.
Placing and Using the COPA
The COPA currently comes in four sizes (8 - green, 9 - yellow, 10 - red, 11 - light green).
Selecting the right size is one of the most important steps of using the COPA. As a guide to
choosing the right size, a COPA held next to the patient’s head should result in the bite block just
above the teeth with the tip of airway at angle of mandible. This is usually one size larger than
the corresponding oral airway that would be used in that patient. Choosing the right size is
important, as the airway is designed to “lock into place” behind the base of the tongue. Once the
right size is chosen, the device should be prepared for use by lubricating it, placing the included
strap behind the patients head, testing the cuff, completely deflating the cuff and pre-oxygenating
28 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
the patient. Insertion is facilitated with a dose of Propofol. This dose approximates the usual
induction dose. The technique for insertion is the same as insertion of oral airway - either the
reverse Guedel technique or the direct Guedel technique may be used. Since most people are
already familiar with these techniques, which are already easy to learn, the learning curve for use
of this device is not steep. Once inserted, the device should be strapped into place before any
manipulation. This ensures that the COPA will not “pop out” of position with subsequent
airway maneuvers. When strapping the COPA in place, make sure that the device is in the
midline. If the proper size has been chosen, the colored bite block should “transition” at the teeth.
After strapping the device in place, do a jaw thrust/chin lift. Then inflate the cuff with the
proper amount of air:
• Size 8 - 25 cc
• Size 9 - 30 cc
• Size 10 - 35 cc
• Size 11 - 40 cc
Once in place, the following steps should be taken:
• Connect the circuit
• Gentle positive pressure
• Allow return of spontaneous ventilation
• Use “airway maintenance techniques” if needed
Some of the “Airway Maintenance Techniques” suggested by the company to ensure that the
COPA works easily are:
• Increased or decreased head tilt
• Turn head to one side
• Support the shoulders
• Gentle chin lift may be needed early in case
• Positive airway pressure up to 10 cm H2O
When the anesthetic is complete, removal of the airway is easy as well. First, allow emergence
from anesthesia while leaving the patient relatively undisturbed. Watch for return of airway
reflexes - signs of this includes, swallowing, phonation, etc. Do not deflate the cuff; rather
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 29
duplication is prohibited by law.ARTIFICIAL AIRWAYS
remove the device intact. Any secretions and such will be carried with the inflated cuff upon
removal. Once removed, verify good spontaneous ventilation and airway patency of the patient.
Lingual Nerve Injury after Use of a Cuffed Oropharyngeal Airway
Gentle airway manipulation with the use of the cuffed oropharyngeal airway is recommend, this
will help with the avoidance of excessive cuff inflation and early recognition of such a
complication if it occurs.
Pharyngeal-Tracheal Lumen Airway (PtL)
Courtesy Of: Alliance Medical Inc.
The PtL (Pharyngeal-tracheal Lumen) Airway is a double lumen adjunct that can deliver effective
ventilation to a patient whether the device is placed in the trachea or esophagus. Unique design
requires no syringes to inflate the airway balloons and has an integrated bite block design to aid in
keeping an airway patent.
AIRWAY ADJUNCTS
N ote that the following airways have been determined as “class indeterminate
recommendation” in the 2000 ACLS guidelines which means that there is evidence
lacking for the inclusion of these devices in the guidelines:
• Esophageal obturator airway (EOA)
• Esophageal pharyngeal airway
• Pharyngotracheal lumen airway
• Berman intubating-pharyngeal airway (BIPA)
30 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.ARTIFICIAL AIRWAYS
• Tracheal-esophageal airway
Tracheal tube changers are slender, flexible tubes inserted in existing ETT’s to aid re-intubation.
They are similar to the guide-wires used for changing intravascular catheters. The changer is
placed in the existing ETT and the ETT removed, leaving the changer in place. The new ETT is
then slid over the changer and advanced into the trachea. They can be used for changing ETT’s
due to cuff leaks or other problems. They also can be used on a patient where there is doubt as to
whether they will tolerate extubation. The changer can be left in place for several hours following
extubation and then removed if re-intubation is not necessary.
Stoma maintenance devices (trach “buttons”) are used for weaning patients from trach tubes and
for those in whom periodic suctioning or ventilation is needed. Trach buttons are short, straight
tubes that maintain the stoma without impinging on the airway lumen. They can be plugged so
the patient must breathe through the upper airway.
spacer
plug
cannula
Tracheal Button
Courtesy of Aaron’s Home Page
Features Of The Tracheostomy Button:
1. The hollow outer cannula has a slightly flared proximal end, which keeps it from slipping
all the way into the patient. The distal end is flanged and split into several flexible
“grippers”.
2. A closure plug fits into the outer cannula and snaps into the flexible grippers on the end of
the outer cannula. This seals the button so that the patient breathes through the upper
airway.
3. A hollow inner cannula can be inserted into the outer cannula instead of the plug. This
inner cannula has a standard 15-mm OD so that a Briggs adapter or other respiratory care
equipment can be attached if needed. The patient can also be suctioned.
4. Spacers of various widths are used to make sure that the inner cannula is placed in the
This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized 31
duplication is prohibited by law.ARTIFICIAL AIRWAYS
patient to the right depth. The end of the tube should enter the trachea but not obstruct it.
The Olympic button, Kistner Valve and Montgomery valve are examples of these related devices.
They extend through the anterior neck to the tracheal wall. The purpose is to prevent stoma
closure and allow access to the trachea for suctioning and emergency resuscitation. Unites are
generally composed of rigid Teflon or flexible silicone rubber. The valve type has a one-way
valve to allow inspiration through the tube, permitting vocalization and exhalation. Sizing
requires measurement of distances from the neck to the posterior stoma. Note that not all these
devices can be attached to a standard 15mm adapter used for resuscitation. Of course, prior to
insertion of any of these less commonly used devices, the manufacturer instructions should be
reviewed carefully.
Tracheostomy Tube Weaning: Prior to weaning the patient from a tracheostomy tube, pre-
weaning criteria such as laboratory values within acceptable limits, must be met. In addition, a
thorough assessment of the patient and their ability to breathe, expel secretions and prevent
aspiration needs to be made. There are various weaning procedures. In the past, using a
fenestrated tracheostomy tube to wean has been popular, but the recommendation now is to
progress to a smaller tracheostomy tube (not less than 4 O.D.), then to plugging, then extubation
or a tracheostomy button.
To acquire more information on this specific topic, we refer you to our courses “Passy-Muir
Tracheal and Ventilator Speaking Valves” and “Tracheostomy”.
The remaining material in this course applies strictly to endotracheal and tracheostomy tubes.
GENERAL INFORMATION
I nsertion of an endotracheal tube (ETT) or tracheostomy tube alters the geometry of the upper
airway and changes airway resistance, work of breathing (WOB), dead space (VD) volume,
and the potential for airway obstruction. The changes in resistance, WOB, and VD are related
to the type of airway used, its internal diameter, and fluid mechanics.
All artificial airways increase resistance to breathing. Airway resistance increases about three
times with the insertion of an artificial airway. Obviously, WOB increases proportionally. The
patient must generate a higher-pressure gradient on each breath to achieve the same minute
volume. The increase in resistance through tracheostomy tubes and ETT’s is similar. (The
expected decrease in resistance due to the short length of a tracheostomy tube is offset by its
greater curvature).
Bypassing the normal airway, even with a large artificial airway, significantly decreases airway
diameter and increases resistance. The cross-sectional area of an 8 mm internal diameter ETT is
50 mm2. (Cross-sectional area of the trachea is 150-300 mm2 and the oropharynx is 600 mm2).
This decrease in total cross-sectional area significantly increases resistance and WOB, the smaller
the artificial airway, the greater the impact on airway resistance. The newest generations of
ventilators often have a tube compensation feature which does decrease some of the resistance
32 This material is copyrighted by RC Educational Consulting Services, Inc., (800) 441-LUNG. Unauthorized
duplication is prohibited by law.You can also read