Sometimes we need to think of zebras: The identification of bone tumors in children - BC Medical Journal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

May 2020: 62:4
Pages 121–152
Sometimes we need
to think of zebras:
The identification of
bone tumors in children
IN THIS ISSUE
Concrete vs COVID-19: How
the built environment can
limit the spread of disease
Measuring multimorbidity
to support chronic disease
management and prevention
Pandemic fears
COVID reflections
Social distancing:
Origins and effects
bcmj.org
BC Medical Journal vol. 62 no. 4 | MAY 2020 121
You can now use Dr. Bill
absolutely free.
Use our powerful billing software to submit
as many claims as you want at no charge.
dr bill ad
Focus on patient care.
Let us handle your billing for you.
Register today for FREE at dr-bill.ca
122 BC Medical Journal vol. 62 no. 4 | MAY 2020
0 7 10 21 27 35
First Visit to Physio- Visit to Visit to Visit to
recollected walk-in therapy walk-in walk-in family
symptoms clinic starts clinic clinic doctor
Visit to
(9 weeks)
45
family
doctor
May 2020
Volume 62 | No. 4
Pages 121–152 Visit to sports medicine,
positive imaging,
65
First
appointment
93 referral to BCCH Visit to
sports
at BCCH,
CT, PET 95 eGFR
medicine
Echocardio- 102
gram, biopsy
97 Initiation of
103 chemotherapy
101
Central line
placed
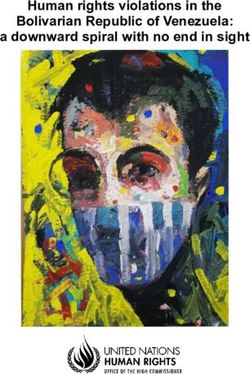
Patient journey maps are a powerful tool to illustrate relevant interactions with the health care system from the time of first symptoms to the initiation of definitive therapy.
This map created using BC Children’s Hospital data for our cover article on bone tumors in children shows that the patient saw primary health care physicians seven times
before being referred to tertiary care.
125 Editorials CLINICAL 137 Premise
Farewell, Kash, Social distancing: Origins and effects,
David Richardson, MD 130 Sometimes we need to think of George Szasz, CM, MD
My pandemic fears, zebras: An observational study
David B. Chapman, MBChB on delays in the identification 138 News
of bone tumors in children, n Doctors of BC COVID-19 resource
127 President’s Comment T. Justin Dhinsa BSc, Paula Mahon, page
COVID-19 reflections, RN, Caron Strahlendorf, MB
n Follow-up of living kidney donors:
Kathleen Ross, MD A call for collaboration
134 COHP n News from the Doctors Technology
128 Letters Concrete versus COVID-19: How Office
Is our health system ready for digital the built environment can limit the n Digestive symptoms present in mild
health today? Exploring the way spread of disease, Lloyd Oppel, MD COVID-19 disease, sometimes
forward, Kendall Ho, MD, Helen without fever
Novak Lauscher, MD, Chad Kim 135 BCCDC n Psychological PPE: Peer support
Sing, MD, Maryam Matean, MPH Measuring multimorbidity to support beyond COVID-19
chronic disease management and n Heart disease, stroke, and diabetes all
prevention, Drona Rasali, PhD, at once: A triple threat
Crystal Li, MSc, Caren Rose, PhD News items continued on page 124
Environmental impact Postage paid at Vancouver, BC. Canadian Publications Mail, Product Sales Agreement #40841036. Return undeliverable copies
The BCMJ seeks to minimize its negative impact on the to BC Medical Journal, 115–1665 West Broadway, Vancouver, BC V6J 5A4; tel: 604 638-2815; email: journal@doctorsofbc.ca.
environment by:
Advertisements and enclosures carry no endorsement of Doctors of BC or BCMJ.
• Supporting members who wish to read online with an
e-subscription to bcmj.org © British Columbia Medical Journal, 2020. All rights reserved. No part of this journal may be reproduced, stored in a retrieval system, or trans-
• Avoiding bag use, and using certified-compostable plant-based mitted in any form or by any other means—electronic, mechanical, photocopying, recording, or otherwise—without prior permission in
bags when needed writing from the British Columbia Medical Journal. To seek permission to use BCMJ material in any form for any purpose, send an email to
• Working with Mitchell Press, ranked third in North America for journal@doctorsofbc.ca or call 604 638-2815.
sustainability by canopy.org Statements and opinions expressed in the BCMJ reflect the opinions of the authors and not necessarily those of Doctors of BC or the
• Printing with vegetable-based inks institutions they may be associated with. Doctors of BC does not assume responsibility or liability for damages arising from errors or omis-
• Using FSC-certified paper sions, or from the use of information or advice contained in the BCMJ.
• Printing locally in British Columbia The BCMJ reserves the right to refuse advertising.
BC Medical Journal vol. 62 no. 4 | MAY 2020 123
On the cover
Sometimes we need to think of zebras:
The identification of bone tumors in children
Clinicians are often encouraged to follow the diagnostic
path most likely—to look for horses, not zebras when
they hear hoofbeats. Pediatric bone sarcomas are
rare and difficult to diagnose, with common sites for
osteosarcoma including the distal femur and proximal
tibia. Patients typically present with chronic localized
pain that is intermittent, often with no fever, weight
loss, or malaise. Because the presentation can be similar
to what a clinician would expect for tendonitis and
other benign pathologies, patients frequently receive
physiotherapy rather than referral to a tertiary care
centre for further workup. Article begins on page 130..
This evocative sketch by the late Dr Max Schultz, an anesthesiologist, accompanies a brief poem and his obituary
The BCMJ is published by Doctors of BC. The journal provides
on page 142.
peer-reviewed clinical and review articles written primarily by BC
physicians, for BC physicians, along with debate on medicine and
medical politics in editorials, letters, and essays; BC medical news;
career and CME listings; physician profiles; and regular columns.
Print: The BCMJ is distributed monthly, Contents continued from page 123
other than in January and August.
Web: Each issue is available at www.bcmj.org. News (continued) 143 CME Calendar
Subscribe to print: Email journal@doctorsofbc.ca. n Possible role for voice analysis in
Single issue: $8.00
Canada per year: $60.00
telemed and patient care 144 Guidelines for Authors
Foreign (surface mail): $75.00 n Arthritis research education series
Subscribe to notifications: launches with knee osteoarthritis and 146 Classifieds
To receive the table of contents by email, visit
running
www.bcmj.org and click on “Free e-subscription.”
Prospective authors: Consult the “Guidelines for Authors”
150 Back Page
at www.bcmj.org for submission requirements. 141 WORKSAFEBC Thursday mornings:
New WorkSafeBC early concussion My experience as a practising patient,
an assessment program, Ed Martin, BA
Luisa Johns, BSc
Editor Proofreader
David R. Richardson, MD Ruth Wilson
142 Obituaries
Editorial Board Web and social media
Dr James ( Jim) Harvey Sherstan
Jeevyn Chahal, MD coordinator Dr Maxwell (Max) Schultz
David B. Chapman, MBChB Amy Haagsma
Brian Day, MB
Cover concept and
Caitlin Dunne, MD
art direction, Jerry Wong,
David J. Esler, MD
Peaceful Warrior Arts
Yvonne Sin, MD
Cynthia Verchere, MD Design and production
Laura Redmond, Scout
Managing editor
Creative
Jay Draper
Printing
Associate editor
Mitchell Press
Joanne Jablkowski
Advertising
Senior editorial and
Kashmira Suraliwalla
production coordinator
604 638-2815
Kashmira Suraliwalla
or journal@doctorsofbc.ca
Copy editor
ISSN: 0007-0556
Barbara Tomlin
Established 1959
124 BC Medical Journal vol. 62 no. 4 | MAY 2020
editorials
Farewell, Kash
A
s I write this editorial, COVID-19 is to many changes in journal publishing and our
rapidly spreading across the globe and organization over the years, not to mention be-
drastically changing the daily lives of ing a line of continuity for four editors and six
its inhabitants. It is a time of anxiety and fear, managing editors.
leading to many a grim thought. During this In addition to her excellent work at the
period of negativity and darkness, I would like BCMJ, she is also the production coordinator
to celebrate a positive source of the Report to Members (for-
of light. After 36 years of merly the White Report). She is
dedicated service, Kashmira The physicians well known around Doctors of
Suraliwalla, senior editorial BC because of her help with
of BC owe her a
and production coordinator many social and charitable
at the BCMJ, has announced debt of gratitude. projects, such as the annual
her retirement. staff summer picnic and the
Kash, as she is affection- Canadian Cancer Society’s
ately known, grew up in Bombay, India, and Daffodil Campaign. Kash is always ready to
immigrated to Vancouver as a young adult. An contribute to other people’s efforts, and is of-
avid traveler and global citizen she’s an active ten the instigating force behind a fundraiser
member of the Zoroastrian community here or charitable endeavor, whether for earthquake
on the West Coast. She started as an editorial relief, hurricane relief, a humanitarian crisis, or Ms Kashmira Suraliwalla, 2018
assistant at the BCMA, as Doctors of BC was other worthwhile cause.
formerly known, in 1983. As the journal grew, To my mind, the BCMJ and Kash are forever
she became the production coordinator, and linked as she has been serving our journal with I will miss her insightful suggestions and ob-
then started her current position, which sees patience and humor since long before I arrived servations on both our organization and the
her working in such diverse areas as Editorial on the scene. The physicians of BC owe her a provincial medical system. We wish Kash the
Board wrangling, finance, ad sales, and article debt of gratitude, and I would personally like very best in the next chapter of her life. n
submissions (to name a few). She has adjusted to thank her for her years of dedicated service. —Dave Richardson, MD
Expand your practice to
#virtualCARE by seeing patients
via phone and video.
For resources, FAQs and tips visit
doctorsofbc.ca/covid-19
@doctorsofbc
@bcsdoctors
@doctorsofbc
BC Medical Journal vol. 62 no. 4 | MAY 2020 125
Editorials
My pandemic fears
31 March 2020
B
y the time this editorial, written at international colleagues is that even though During the early stages of the pandemic
the end of March, makes it to print, it they took all the necessary protective measures, in BC, the physicians with whom I work were
will be hopelessly out of date. I hope they too are getting sick with COVID-19. It aware of community spread of the disease sev-
that my fears today do not become our reality doesn’t help that we feel as though we may run eral days before it was announced officially.
when this is read in the May issue of the BCMJ. out of personal protective During the early stages of
Thanks to the COVID-19 pandemic, today’s equipment. It doesn’t help the pandemic in BC, some
reality for many front-line physicians consists when the published sta- The keys to containing staff were wearing masks
of virtual office visits, virtual meetings, virtual tistics of confirmed cases at all times in the hospital
contact with friends and loved ones, and virtu- of COVID-19 do not
this disease are rigorous (not only during patient
ally being on the edge of panic every day. take into account that we testing and contact contact), but they were
We physicians in this province have been stopped testing the gen- tracing, strict controls reprimanded by hospital
told to keep our heads down, to keep calm, eral population 2 weeks on people’s movement administration for doing
and to not publicly disagree with the official ago. Of course, the num- so. A couple of weeks later,
(border controls and
statements coming from the various levels of ber of confirmed cases we were told by the same
government and the medical profession’s rep- will appear to be fewer if social distancing), and people that it was advis-
resentative and regulatory bodies with regard you change your testing enforced quarantine of able to wear a mask at
to the COVID-19 pandemic. I understand the criteria. high-risk individuals. all times in the hospital.
logic behind this message; they don’t want the In my opinion— Last week, I had hospital
public to panic. The unintended consequence is shared by epidemiologists rounds for my group. My
that many health care providers are currently in and infectious disease specialists throughout the daily ritual after hospital rounds was to shower
a state of panic. Those of us who are exposing world, and annunciated by the World Health and change clothes and shoes before going to
ourselves daily to people who could potentially Organization—the keys to containing this dis- my office. I now wear a mask and eye protection
make us very sick or even kill us are feeling very ease are rigorous testing and contact tracing, all the time when I am in public or at work.
stressed. It doesn’t help when we know that strict controls on people’s movement (border Many physicians in our hospital had to buy eye
things are worse than they are being made out controls and social distancing), and enforced protection for themselves, as I did. I clean my
to be. It doesn’t help when the news from Italy quarantine of high-risk individuals. Unfortu- hands multiple times a day. Yet, I fear that is
is of civil unrest and the news from New York is nately, we stopped testing widely, and the con- not enough to avoid getting the virus. Today,
that refrigeration trucks are being used to store trols on people’s movement were perhaps 1 or without any obvious stimulus, my fear ramped
bodies. It doesn’t help when the news from our 2 weeks too late, and they are too weak. up to such a high level that I imagined this
editorial to also be my obituary.
If this pandemic can be likened to a war, and
health care workers are the army, then it feels as
if we are being sent into battle without bullets
and without adequate body armor.
I apologize to readers for the gloomy na-
ture of this editorial, and I apologize to those
trying to keep everyone calm. The only miti-
gating factor, perhaps, is that by the time you
read this my words will either seem hopelessly
pessimistic and overdramatic, or the situation
will be much worse and these words will seem
calm compared with how everyone is actually
feeling. I hope it’s the former. n
—David B. Chapman, MBChB
126 BC Medical Journal vol. 62 no. 4 | MAY 2020
president’s comment
COVID-19 reflections
I
t is 2 April 2020 as I write this President’s to the pandemic has been supported by public Facebook, Slack, and WhatsApp groups to sup-
Comment. Across Canada the first wave health, government, health authorities, health port each other, plan next steps, and debrief
of the coronavirus crisis is beginning to care leaders, health care workers, and the public. about critical situations and the ongoing stress
take off. Using frameworks fine-tuned through Canadians have weathered an unprecedented of being in a hazardous environment.
other pandemics, we have been implementing disruption to our lives and to the health care Untold numbers of physicians and other
stronger and stronger public health measures system, which has mobilized to meet the nec- health care providers have shown up to work
to slow the spread. And yet the numbers are essary changes in a way that many would not every day facing the threat that they would
slowly rising. I feel like I am standing on the have thought possible over such a short time. fall ill. Many may still fall ill, and some may
beach watching the water drain away ahead of Virtual care ramped up seemingly overnight not survive. Tough decisions lie ahead about
the tsunami. in support of COVID-19 screening and longi- the rationing of critical care if our resources
Last month I messaged all of you to mobi- tudinal care. Our front-line primary care and are outpaced. Knowing this, you all continue
lize our profession in amplifying the orders of specialist providers have been working with to come to work anyway. All of you are heroes.
one of our own, Dr Bonnie Henry, our provin- all partners to ensure that patients can still ac- I hope by the time this is published we will
cial health officer. I cannot imagine a calmer cess care for their usual medical conditions and see the light at the end of the darkness, and
and more organized physician to lead our health ensure that our most vulnerable patients stay we will have conquered the first wave of the
care system and the public through this time— connected to necessary services. coronavirus. We know the virus will come back
providing information that is timely, relevant, Physicians and health care leaders inside our for a second wave, and I’m confident you will
factual, and free from alarmist tone. Many of facilities have put aside differences and pulled rise to face this challenge with the same coura-
you joined the communication stream to add together to nimbly solve critical issues involv- geous and innovative spirit you’ve all embodied
your professional knowledge, personal experi- ing physical space, beds, ventilators, oxygen thus far.
ence, and credibility to ensure the public got supplies, testing processes, staff shortages, and I will be standing there with you, provid-
the message to self isolate and practise physical shortages of personal protective equipment. No ing hands-on care, all the while doing my best
distancing. one has been idle. to keep those I work with and care for, safe
This is a time unlike any we have seen before, Physicians have rallied together to share from harm.
and one I hope we will not see again in our knowledge about processes that were successful, —Kathleen Ross, MD
lifetime. Physicians’ tireless work in responding and those that were less so. You have created President, Doctors of BC
2019–20 Doctors of BC
Board of Directors
President Director-at-Large General Practice Director-at-Large Specialist
Dr Kathleen Ross Dr Adam Thompson Dr Barb Blumenauer
President-Elect Director-at-Large General Practice Director-at-Large Specialist 1 year
Dr Matthew Chow Dr Lawrence Welsh Dr Andrew Yu
Board Chair Director-at-Large Specialist Director-at-Large Specialist
Dr Jeff Dresselhuis Dr Lloyd Oppel Dr Sophia Wong
BC Medical Journal vol. 62 no. 4 | MAY 2020 127
Letters to the editor We welcome
original letters of less than 300 words; we may edit them for clarity
delivery today. We must prepare to integrate
digital health into mainstream health care.
On 1 November 2019, a panel at the Tech-
and length. Letters may be emailed to journal@doctorsofbc.ca, submitted
nologies in Emergency Care Vancouver Con-
online at bcmj.org/submit-letter, or sent through the post and must include
ference (TEC Vancouver) discussed how to
your mailing address, telephone number, and email address. Please disclose
prepare our health workforce for digital in-
any competing interests. novations. Fifty leaders representing health,
government, private sector, patients, and aca-
demia tackled the problem. We highlight some
Is our health system ready for digital health today? take-home messages from the discussion here.
We need to stop making things hoping they
Exploring the way forward
get used. Without guidance from health leaders
Asking “Is our society ready to go digital?” may lives. Yet, asking “Is our health system ready and front-line clinicians, private sector solutions
seem absurd considering that digital technolo- for digital health?” is not farfetched, reflecting can miss the mark. Research, education, and
gies are core to almost every aspect of our daily the relative lack of digital uptake in health care Continued on page 140
EMPATHY
LISTENING
PATIENCE
TIME-MANAGEMENT
TRUST
CLARITY
ORGANIZATION
RESPONSIVENESS
RESPECT
GET BETTER SOON.
We’re talking to you, doc. MCC 360. Get better.
Strengthen your communication, collaboration, and
professional skills with MCC 360, the multi-source
feedback tool that can help you become an even
better doctor, while earning up to 15 CPD credits.
mcc.ca/360physicians
128 BC Medical Journal vol. 62 no. 4 | MAY 2020
Doctors of BC
Links and resources for COVID-19
Doctors of BC is actively supporting members during the coronavirus (COVID-19)
pandemic in a variety of ways. Work includes advocacy on behalf of physicians
with government, the provincial health officer, and health authorities, as well as
ensuring members have access to appropriate tools, benefits, and insurance.
An information resource from Doctors of BC, updated regularly:
www.doctorsofbc.ca/covid-19
This page has information on:
• COVID-19 changes to billing
• Virtual care support
• An online forum for collaboration on COVID-19
• Insurance and benefits updates during COVID-19
• Important external resources
• Support for physicians feeling stress during COVID-19
For questions or concerns about COVID-19, contact us directly at
covid19@doctorsofbc.ca
BC Medical Journal vol. 62 no. 4 | MAY 2020 129
Clinical
T. Justin Dhinsa, BSc, Paula Mahon, RN, DHealth, CNCCP(C), Caron Strahlendorf, MB, FRCPC, FCP
Sometimes we need
to think of zebras:
An observational study on
delays in the identification of
bone tumors in children
Patients eventually diagnosed with osteosarcoma or Ewing sarcoma
often spend many weeks receiving physiotherapy and visiting other
health care professionals in the primary care setting before they are
referred to a tertiary care centre.
ABSTRACT of research on delays in appropriate management suspicious if there is a history of night pain, an
Background: Pediatric bone sarcomas are rare of pediatric bone tumor and to increase awareness atypical pain pattern following minor trauma, or
and difficult to diagnose. Osteosarcoma is the of osteosarcoma and Ewing sarcoma. a soft tissue mass on examination.
most common and Ewing sarcoma is the second
most common of these. Most cases are identi- Methods: Six pediatric patients at BC Children’s Background
fied in individuals age 13 to 16 years. Common Hospital who were diagnosed with either osteo- Bone sarcomas make up 6% of all pediatric
sites for osteosarcoma include the distal femur sarcoma or Ewing sarcoma in 2018 were identified cancers, with the most common being osteo-
and proximal tibia. Patients typically present with from the oncology database. The dates of their sarcoma and the second most common being
chronic localized pain that is intermittent. There interactions with the health care system were used Ewing sarcoma.1,2 Osteosarcoma is a malig-
is often no fever, no weight loss, and no malaise. to create patient journey maps. nant mesenchymal neoplasia characterized by
Because the presentation can be similar to what the production of osteoid or bone by the ma-
a clinician would expect for tendonitis and other Results: Each patient saw an average of four health lignant cells.3 Ewing sarcoma is part of the
benign pathologies, patients frequently receive care professionals before referral to BC Children’s Ewing sarcoma family of tumors, which share
physiotherapy rather than referral to a tertiary care Hospital, and three patients spent 4 to 9 weeks histological characteristics and chromosomal
centre for further workup. A quality improvement receiving physiotherapy. On average, 114 days translocations. Ewing sarcomas are small round
observational study was proposed to address a lack elapsed from the time patients had their first symp- blue cell tumors that can develop in bone or
toms to when they received chemotherapy, and soft tissue.3 The peak incidence for both os-
81% of this time was spent within the primary teosarcoma and Ewing sarcoma coincides with
care system. the adolescent growth spurt. Most cases are
Mr Dhinsa is an undergraduate student
identified in individuals age 13 to 16 years, and
in the Faculty of Medicine at the Conclusions: The study reveals an overall delay in
females tend to present at a younger age than
University of British Columbia. Dr Mahon diagnosis and treatment of pediatric bone tumors
males.1 Both diseases most commonly occur
is a clinical assistant professor in the and highlights the need for general practitioners to
in the metaphyses of long bones.4,5 One large
School of Nursing at UBC. Dr Strahlendorf further consider sarcomas in the differential diag-
population-based series suggested that as many
is a clinical associate professor in the nosis when patients present with chronic localized
as 75% of osteosarcomas originate in the distal
Division of Hematology and Oncology in pain, especially when patients are in the at-risk
femur.6 Other common sites for osteosarcoma
the Department of Pediatrics at UBC. age group and the pain is localized to one of the
include the proximal tibia, proximal humerus,
common sites. Practitioners should be even more
middle femur, and proximal femur.4
This article has been peer reviewed.
130 BC Medical Journal vol. 62 no. 4 | MAY 2020Dhinsa
TJ, Mahon P, Strahlendorf C Clinical
Patients often present with chronic localized chemotherapy.10 Ewing sarcoma is more sen- were then reviewed to determine the dates of
pain that is intermittent. Clinical diagnosis is sitive to chemotherapy and radiotherapy than appointments, imaging, and interventions. Pa-
difficult because there is often no family his- osteosarcoma, so radiation can be considered in tient journey maps were created to illustrate all
tory to consider, no fever, no weight loss, and place of or in addition to surgery.11 As a result of relevant interactions with the health care system
no malaise. The pain is often first noticed after modern multimodal therapies for osteosarcoma, from the time of first symptoms to the initia-
trauma to the site.7 A bone sarcoma patient’s 66% of patients without metastases, 50% with tion of chemotherapy. The visual representations
presentation will frequently be similar to what limited pulmonary metastases, and 25% with of important events for all patients were then
a clinician would expect for tendonitis, muscle more advanced metastases are expected to be compared to determine if there were patterns
injury, Osgood-Schlatter disease, meniscal le- long-term survivors.12 that might help physicians considering these
sions, and other benign pathologies.7 The ob- System-wide awareness of osteosarcoma diagnoses. Information that could be used to
scure nature of bone sarcomas can result in and Ewing sarcoma is needed along with timely identify patients or the health care professionals
patients receiving inadequate pain management referral. Only seven articles about delays in ap- involved in their care was not included in the
and attending physiotherapy sessions rather propriate management of pediatric bone tumors research records. The study was approved by the
than being referred to a tertiary care centre for have been published to date, and none of them UBC Children’s and Women’s Health Centre
further workup. are based on research in Canada or the United of British Columbia Research Ethics Board.
Early identification of patients is important States.7,13-18 A quality improvement observa-
because bone tumors frequently metastasize. tional study of patients treated at BC Children’s Results
Before treatment protocols changed to include Hospital (BCCH) was proposed to address this One of the patient journey maps created using
both neoadjuvant and adjuvant chemotherapy, lack of research and to expedite the identifica- BCCH data reveals that the patient saw pri-
80% to 90% of patients with osteosarcoma died tion and referral of affected individuals. mary health care physicians seven times before
as a result of their disease metastasizing. It has being referred to tertiary care [Figure 1]. Before
been hypothesized that the majority of these Methods referral, the patient saw walk-in clinic physi-
patients had subclinical metastases that went To prevent biased selection of study subjects, the cians, family physicians, and a sports medicine
undetected.8,9 last six pediatric patients diagnosed in 2018 at physician. In addition, this patient received
The current treatment protocol for osteo- BCCH with osteosarcoma or Ewing sarcoma 9 weeks of physiotherapy. Another patient saw
sarcoma is surgery combined with 12 weeks were identified in the hospital’s oncology da- all the professionals named above as well as
of neoadjuvant and 29 weeks of adjuvant tabase. The medical records of these patients an emergency room physician before referral.
0 7 10 21 27 35
First Visit to Physio- Visit to Visit to Visit to
recollected walk-in therapy walk-in walk-in family
symptoms clinic starts clinic clinic doctor
Visit to
(9 weeks)
45
family
doctor
Visit to sports medicine,
positive imaging,
65
First
appointment
93 referral to BCCH Visit to
sports
at BCCH,
CT, PET 95 eGFR
medicine
Echocardio- 102
gram, biopsy
97 Initiation of
103 chemotherapy
101
Central line
placed
Figure 1. Patient journey map of all relevant health care encounters for one study subject with Ewing sarcoma.
BC Medical Journal vol. 62 no. 4 | MAY 2020 131Clinical An observational study on delays in the identification of bone tumors in children
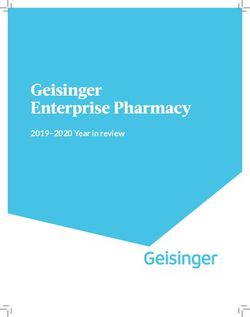
On average, 114 days elapsed from the time
patients had their first symptoms to when they
were treated for their bone tumors, and patients
spent 81% of this time in the primary care sys-
tem visiting multiple health care professionals
[Figure 2]. The six patients whose records were
reviewed had an average of four interactions 9 First symptoms
with health care professionals, not including 93 days
regular physiotherapy. Physiotherapists were 12 Chemotherapy
seen by three of the six patients for 4 to 9 weeks.
On average, patients were seen 1.5 days after
referral to BCCH and began chemotherapy
10.5 days after their first appointment.
A symptom common among all patients was
chronic localized pain that progressed to be- Days from first recollected symptoms to first primary care visit
come very severe. Three of the patients recalled Days from first primary care visit to BCCH oncology referral
night pain and two noted that they began to Days from BCCH oncology referral to initiation of chemotherapy
notice the pain after minor trauma.
Figure 2. Average time in days that six study subjects with osteosarcoma or Ewing sarcoma waited at three
Conclusions
points during their patient journeys: from first symptoms to first primary care visit, from first primary care visit
Bone sarcoma is often overlooked as a possible to BCCH referral, and from referral to chemotherapy.
diagnosis. The patient journey maps created
from BCCH data reveal an overall delay in
diagnosis and treatment of pediatric bone tu- tolls that delays have on patients and their fami- of decreasing prevalence are the distal femur,
mors, with most of the delay in the primary care lies, which can be inferred but not quantified proximal tibia, proximal humerus, middle femur,
setting. This accords with findings from Widhe from the time depicted between health care and proximal femur.4,6
and Widhe, and Goedhart and colleagues, who encounters. Despite these limitations, the study Obtaining a plain radiograph is the recom-
conclude that timely care of bone sarcoma pa- findings still point to the importance of iden- mended first step in the workup when bone tu-
tients is needed between the first primary care tifying bone tumor cases sooner. mors are a possibilty.19 Goedhart and colleagues
visit and referral to a tertiary care centre.7,13 In suggest that delays in care could be reduced if
fact, Widhe and Widhe found that when bone Recommendations general practitioners lower the threshold at
sarcomas were identified on radiographs, the ra- While the early diagnosis of a bone sarcoma which they order plain radiographs.13 If the
diographs had usually been ordered to assess for is difficult, we believe that increased aware- radiograph findings are negative but suspicion
more common pathologies such as fractures.7 ness could reduce delays. General practitioners remains high, a CT or MRI scan is warranted.
Existing studies have found it difficult to should be aware that bone sarcoma patients The definitive diagnosis is made after biopsy,
correlate the delays in diagnosis and manage- typically present with localized chronic inter- but it can be accurately predicted by considering
ment with worse prognoses, as more aggres- mittent pain at the age of 13 to 16 years. The clinical features with imaging results.12
sive tumors are usually diagnosed before less onset of the pain may follow a minor traumatic
aggressive ones.13,14 However, when metastases injury to the region with the sarcoma. Moreover, Summary
are due to a delayed diagnosis, earlier detec- as Widhe and Widhe note, the post-trauma General practitioners should further consider
tion would increase survival and the possibility pain history of bone sarcoma patients is atypical bone sarcomas in the differential diagnosis for
of limb-saving procedures.7,16 Also, as treat- because the pain from trauma seems to resolve chronic localized pain, especially when patients
ment modalities improve, the speed of diagno- over several days only to return in a more pro- are in the at-risk age group and the pain is
sis may play a more important role in patient gressive and severe form. Nocturnal pain should localized to one of the common sites. Practi-
prognoses.17 increase suspicion.15 tioners should be even more suspicious if there
General practitioners conducting physi- is a history of nocturnal pain, an atypical pain
Study limitations cal examinations should look for a tender soft pattern following minor trauma, or a soft tissue
The size of our study population was limited tissue mass that is firmly fixed to the underly- mass on examination. In accord with Goedhart
by the rarity of the diseases studied. As well, ing bone, even though in the majority of cases and colleagues, we recommend that general
the patient journey maps created from BCCH these masses are not palpable on a patient’s first practitioners consider lowering the threshold at
records do not reveal the emotional and physical visit.7 Common sites for osteosarcoma in order which they order plain radiographs. We believe
132 BC Medical Journal vol. 62 no. 4 | MAY 2020Dhinsa TJ, Mahon P, Strahlendorf C Clinical
that heightened awareness of bone sarcoma 7. Widhe B, Widhe T. Initial symptoms and clinical features 11. Haeusler J, Ranft A, Boelling T, et al. The value of lo-
symptoms can reduce the delay in diagnosis in osteosarcoma and Ewing sarcoma. J Bone Joint Surg cal treatment in patients with primary, disseminated,
Am 2000;82:667-674. multifocal Ewing sarcoma (PDMES). Cancer 2010;116:
and treatment. Although osteosarcoma and 8. Cade S. Osteogenic sarcoma: A study based on 133 443-450.
Ewing sarcoma are rare causes of chronic local- patients. J R Coll Surg Edinb 1955;1:79-111. 12. Wang LL, Gebhardt MC, Rainusso N. Osteosar-
ized pain, it is critical to consider them since 9. Dahlin DC, Unni KK. Osteosarcoma of bone and its coma: Epidemiology, pathogenesis, clinical pre-
outcomes are heavily dependent on the stage important recognizable varieties. Am J Surg Pathol sentation, diagnosis, histology. UpToDate. Topic
1977;1:61-72. last updated 16 July 2019. Accessed 20 February
when a tumor is first identified. n 20202. www.uptodate.com/contents/osteosarcoma
-epidemiology-pathogenesis-clinical-presentation
Competing interests -diagnosis-and-histology?search=Osteosarcoma:%20
The obscure nature Epidemiology,%20pathogenesis,%20clinical%20
None declared.
of bone sarcomas presentation,%20diagnosis,%20histology&source
=search_result&selectedTitle=1~109&usage_type
References can result in patients =default&display_rank=1#H12.
1. Bleyer A, O’Leary M, Barr R, Ries LA, editors. Cancer
receiving inadequate 13. Goedhart LM, Gerbers JG, Ploegmakers JJ, Jutte PC.
epidemiology in older adolescents and young adults Delay in diagnosis and its effect on clinical outcome
15 to 29 years of age, including SEER incidence and pain management and in high-grade sarcoma of bone: A referral oncological
survival: 1975-2000. Bethesda, MD: National Cancer
Institute; 2006. NIH Pub. No. 06-5767.
attending physiotherapy centre study. Orthop Surg 2016;8:122-128.
14. Sneppen O, Hansen LM. Presenting symptoms and
2. Stiller CA, Bielack SS, Jundt G, Steliarova-Foucher sessions rather than treatment delay in osteosarcoma and Ewing’s sarco-
E. Bone tumours in European children and adoles-
cents, 1978-1997. Report from the Automated Child-
being referred to a ma. Acta Radiol Oncol 1984;23:159-162.
15. Pan KL, Chan WH, Chia, YY. Initial symptoms and de-
hood Cancer Information System project. Eur J Cancer tertiary care centre layed diagnosis of osteosarcoma around the knee joint.
2006;42:2124-2135.
3. Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens
for further workup. J Orthop Surg (Hong Kong) 2010;18:55-57.
16. Bacci B, Ferrari S, Longhi A, et al. Delay in diagno-
F, editors. WHO classification of tumours of soft tissue sis of high-grade osteosarcoma of the extremities.
and bone. 4th ed. Lyon: IARC Press; 2013. Has it any effect on the stage of the disease? Tumori
4. Meyers PA, Gorlick R. Osteosarcoma. Pediatr Clin North 10. Janeway KA, Maki R. Chemotherapy and radiation 2000;86:204-206.
Am 1997;44:973-989. therapy in the management of osteosarcoma. Up- 17. Goyal S, Roscoe J, Ryder WD, et al. Symptom inter-
5. Cotterill SJ, Ahrens S, Paulussen M, et al. Prognostic fac- ToDate. Topic last updated 9 May 2019. Accessed val in young people with bone cancer. Eur J Cancer
tors in Ewing’s tumor of bone: Analysis of 975 patients 20 February 2020. www.uptodate.com/contents/ 2004;40:2280-2286.
from the European Intergroup Cooperative Ewing’s chemotherapy-and-radiation-therapy-in-the-man 18. Yang JY, Cheng FW, Wong KC, et al. Initial presentation
Sarcoma Study Group. J Clin Oncol 2000;18:3108-3114. agement-of-osteosarcoma?search=chemotherapy and management of osteosarcoma, and its impact on
6. Mirabello L, Troisi RJ, Savage SA. Osteosarcoma inci- -and-radiation-therapy-in-the-management-of%20 disease outcome. Hong Kong Med J 2009;15:434-439.
dence and survival rates from 1973 to 2004: Data from osteosarcoma&source=search_result&selectedTitle 19. Papagelopoulos PJ, Galanis EC, Vlastou C, et al. Current
the Surveillance, Epidemiology, and End Results Pro- =1~150&usage_type=default&display_rank=1. concepts in the evaluation and treatment of osteosar-
gram. Cancer 2009;115:1531-1543. coma. Orthopedics 2000;23:858-867.
BC Medical Journal vol. 62 no. 4 | MAY 2020 133coHp
Concrete versus COVID-19:
How the built environment
can limit the spread of disease
O
n a recent road trip I had occasion proper urban design can reduce contagion. Sim- It is fair to ask whether we have done
to use a rest-stop washroom. As I ilarly, an important tool in the fight against enough in our buildings to limit the risks posed
washed my hands I noted the in- tuberculosis was the provision of adequate in- by everyday objects. Doorknobs, light switches,
structions above the sink encouraging hand door ventilation.1 toilet handles, faucet knobs are all unbiquitous,
washing to prevent influenza and other infec- Reduction of infectious diseases is not the but are they necessary?
tious diseases, and then I turned to leave. To only health benefit that can be achieved with Researchers in Singapore studied
exit the washroom I had to pull on the handle proper design of living spaces and communities. COVID-19 patients’ living spaces and found
of a heavy metal door. Being familiar with the Urban design can be used that the virus was present
saying that the doorknob is the second-dirtiest to promote active trans- Doorknobs, light on toilets, sinks, door han-
part of the washroom, I pondered my options portation, access to shade, dles, and light switches.5
for a germ-free exit. opportunities for social
switches, toilet handles, Current events will
I quickly discounted the window; it was too interaction, clean air, and faucet knobs are all place more focus on
high. Instead, I resolved to use local materials many other benefits. unbiquitous, but are opportunities to design
to escape. As there were no paper towels, I used While much of the they necessary? washrooms and other
toilet paper to make a glove with which to grab progress in preventing living spaces in ways that
the door handle. I pulled the door open—wide infections has come from reduce surface contacts.
enough to allow me to exit with a graceful pir- providing clean air and water, the role of fomites Motion-sensing light switches, doors that swing
ouette—and carried on my way. As I drove away (objects that are touched by multiple people) outward on exit, self-flushing toilets, pedal-
I wondered about the slow adoption of new is another factor. In some instances, the role of operated sinks, and sensor-triggered hand dry-
building standards that eliminate the touching fomites is clear: we don’t reuse needles or tongue ers are all options that offer ways to make the
of shared surfaces. depressors because of the obvious risk of trans- built environment a bigger ally in the reduction
Awareness of the role that urban design mitting disease. There are a host of pathogens of disease. n
plays in disease prevention is hardly new. Fa- that can be deposited on surfaces, then trans- —Lloyd Oppel, MD
mously, in 1854 English physician John Snow mitted to whoever else touches that surface.
demonstrated that an outbreak of cholera in E. Coli, Streptococcus, MRSA, yeast, norovirus, References
London was attributable to water drawn from and influenza are all examples. When it comes 1. Duhl LJ, Sanchez AK. Healthy cities and the city plan-
a single well. At the time, sewage was carried to colds and flu, however, the role of fomites is ning process: A background document on links be-
tween health and urban planning. World Health
in street gutters or pits scattered around resi- somewhat less clear.2 Organization. 1999. Accessed 31 March 2020. https://
dential areas, leading to fecal contamination of Although studies have demonstrated the apps.who.int/iris/handle/10665/108252.
drinking water. ability to recover viruses from surfaces (espe- 2. Stephens B, Azimi P, Thoemmes MS, et al. Microbial ex-
The subsequent adoption of piping systems cially nonporous surfaces) days after initial de- change via fomites and implications for human health.
Curr Pollution Rep 2019;5:198-213.
that brought clean water directly into houses position,3 the recovery of viral nucleic acid does 3. van Doremalen N, Bushmaker T, Morris DH, et al. Aero-
is recognized as a landmark example of how not necessarily mean that those surfaces are a sol and surface stability of SARS-CoV-2 as compared
significant source of transmission, and good with SARS-CoV-1. N Engl J Med 2020. doi: 10.1056/
ventilation, personal spacing, and hand washing NEJMc2004973.
This article is the opinion of the 4. Bin SY, Heo JY, Song MS, et al. Environmental con-
may be the mainstay of preventive measures.
tamination and viral shedding in MERS patients dur-
Environmental Health Committee, Nevertheless, given the evolving state of un- ing MERS-CoV outbreak in South Korea. Clin Infect Dis
a subcommittee of Doctors of BC’s derstanding of the role that touched surfaces 2016;62:755-760.
Council on Health Promotion, and is not play in the spread of COVID-19 (let alone the 5. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmen-
necessarily the opinion of Doctors of BC. other pathogens that are present), policies that tal, and personal protective equipment contamination
This article has not been peer reviewed by by severe acute respiratory syndrome coronavirus 2
promote environmental hygiene are thought to (SARS-CoV-2) From a symptomatic patient. JAMA 2020.
the BCMJ Editorial Board. be justified.4 doi: 10.1001/jama.2020.3227.
134 BC Medical Journal vol. 62 no. 4 | MAY 2020BCCDC
Measuring multimorbidity The age-standardized prevalence rate of
multimorbidity among individuals having two
or more chronic diseases is calculated for the
to support chronic disease indicator. The measurement is expected to en-
hance our understanding of the epidemiology
management and prevention of multimorbidity to inform prevention efforts,
reduce disease burden, and align health care
services with holistic patient needs.4 This also
M
underscores the importance of monitoring mul-
ultimorbidity, the co-occurrence nationally validated case definitions revealed timorbidity to provide insights to broaden our
of two or more disease conditions multimorbidity prevalence rates of 26.5% mindset of single disease–centric approaches to
(2+), manifests itself in manifold and 24.8% in Canada and BC, respectively, management of chronic disease in the primary
challenges in the present-day health manage- in 2011/12.5 While these Canadian and BC care setting and prevention as part of public
ment of patients. Multimorbidity has been one prevalence rates are substantial, a fixed set of health. Furthermore, the risk and protective fac-
of the most complex phe- well-defined chronic con- tors and socioeconomic determinants of health
nomena in health care sys- ditions is needed, along associated with most chronic conditions indi-
tems around the world in Multimorbidity has with use of a standardized vidually are common but can be tackled con-
recent times. It affects all surveillance methodology sidering multimorbidity as a composite disease
been one of the most
age groups, but a geriatric to improve measurement entity for planning upstream prevention. n
focus in health research is complex phenomena of multimorbidity that —Drona Rasali, PhD, FACE
prominent owing to high- in health care systems would consistently in- BCCDC, Provincial Health Services Authority
er prevalence among old- around the world form practice, program, (PHSA)
er adults.1 Moreover, the in recent times. and policy planning.4 —Crystal Li, MSc
co-occurrence of multiple Recently we intro- BCCDC, PHSA
diseases leads to greater duced an indicator mea- —Caren Rose, PhD
chances of complications and greater severity suring multimorbidity prevalence2 in individuals BCCDC, PHSA, UBC School of Population and
compared to single diseases, and the combined living with two or more chronic conditions from Public Health
burden of multimorbidity and the health care a list of 16 chronic diseases listed in chronic
resources required to manage it may be much disease registries. The indicator is intended for References
greater than the sum of single diseases.2,3 use in health surveillance on a periodic ba- 1. Aydede SK, Rasali D, Osei W, Hunt T. Multimorbidity
Due to Canada’s aging population, multi- sis to support management and prevention of and health-related quality of life among older adults.
J Gerontol Geriatr Res 2017;6:388.
morbidity is increasingly becoming a key public chronic diseases in BC. The chronic diseases
2. Li C, Rasali D, Rose C, et al. Introducing a new health
health and primary care issue in the prevention with identified case definitions5,6 selected for indicator for British Columbia – chronic disease mul-
and management of chronic diseases.4 Cana- the multimorbidity indicator are: timorbidity. Poster presentation at the PHABC Annu-
dian adults 20 years and older who were sur- • Asthma al Conference. 2019. Accessed 25 March 2020. https://
phabc.org/wp-content/uploads/2019/11/PHABC_Mul-
veyed with a list of nine self-reported chronic • Chronic kidney disease
timorbidities_Indicator_poster-Final.pdf.
conditions had a multimorbidity prevalence of • Chronic obstructive pulmonary disease 3. US Department of Health and Human Services. Multiple
12.9% in 2011/12.3 BCCDC’s recent analy- • Dementia chronic conditions: A strategic framework. Optimum
sis of 16 chronic diseases, as defined in BC’s • Diabetes health and quality of life for individuals with multiple
chronic conditions. December 2010. Accessed 25 March
chronic disease registries, showed nearly one • Epilepsy
2020. www.hhs.gov/sites/default/files/ash/initiatives/
third (28.6%) of BC residents 20 years or older • Heart failure mcc/mcc_framework.pdf.
had multimorbidity (2+) in 2014/15.2 Another • Hospitalized stroke 4. Roberts KC, Rao DP, Bennett TL, et al. Prevalence and
Canadian study using data for five conditions • Hypertension patterns of chronic disease multimorbidity and associ-
(cardiovascular disease, respiratory disease, • Ischemic heart disease ated determinants in Canada. Health Promot Chronic
Dis Prev Can 2015;35:87-94.
mental illness, hypertension, and diabetes) with • Mood and anxiety disorders 5. Feely A, Lix LM, Reimer K. Estimating multimorbidity
• Multiple sclerosis prevalence with the Canadian Chronic Disease Sur-
• Osteoarthritis veillance System. Health Promot Chronic Dis Prev Can
This article is the opinion of the BC Centre • Osteoporosis 2017;37:215-222.
for Disease Control and has not been 6. Tonelli M, Wiebe N, Fortin M, et al. Methods for iden-
• Parkinsonism tifying 30 chronic conditions: Application to adminis-
peer reviewed by the BCMJ Editorial • Rheumatoid arthritis trative data. BMC Med Inform Decis Mak 2016;15:31.
Board.
BC Medical Journal vol. 62 no. 4 | MAY 2020 135Expand your practice to
#virtualCARE by seeing patients
via phone and video.
For resources, FAQs and tips visit
doctorsofbc.ca/covid-19
@doctorsofbc
@bcsdoctors
@doctorsofbc
136 BC Medical Journal vol. 62 no. 4 | MAY 2020premise
Social distancing:
in being a good citizen by following the advice
of professionals may help.
A 2015 study suggested that long-term so-
Origins and effects cial isolation (in the absence of a threat like
the current viral infection) increased the risk
of mortality by 29% for people with chronic
Under normal circumstances the interpersonal distances chosen by conditions such as heart disease, depression,
and dementia.
people depend on many things. But what are the impacts of required
There are no studies about the unintended
changes in behavior during unprecedented times? side effects of enforced long-term social dis-
George Szasz, CM, MD tancing. Confinement of families with chil-
dren may result in unexpected interpersonal
tensions. The physical closeness may exacer-
S
taying away from each other has become Hall proposed four main zones of space bate domestic violence. Missing the coping
crucial to slow the spread of the coronavi- between individuals: mechanisms provided by the emotional expe-
rus. Public health officials have instructed • Intimate distance (less than half a metre), riences of sporting or artistic events, or reli-
us to practise social distancing, stay home, avoid such as in giving or receiving a hug. gious ceremonies, may be a problem for many
crowds, and refrain from touching one another. • Personal distance (about 1 metre), usually people. Anxiety about finances secondary to job
In 1963, when Edward Hall, a cultural an- reserved for family or losses and the interrup-
thropologist, coined the term proxemics to define good friends. tion of schooling are only
studies about social distancing in everyday life, • Social distance (2 to 3 In ordinary times the part of a predictable rise
nobody thought that a virus, 100 times smaller metres), when meeting in mental health prob-
than even a bacterium, would make human strangers.
amygdala is suspected lems. And this is only a
closeness a big problem. Hall’s concern was • Public distance (more of processing strong short list of what a submi-
that closer distances between two persons may than 5 metres), such as reactions to violations croscopic lifeless protein
increase visual, tactile, auditory, or olfactory in public presentations. of social spaces. Now we can do when it burrows
stimulation to the point that some people may Under ordinary cir- itself into the cells of our
are facing compulsory
feel intruded upon and react negatively. Today cumstances, the interper- body to copy and copy
we are worried about becoming exposed to a sonal distance chosen by social distancing and copy itself, multiply-
viral attack. people depends on atti- beyond the amygdala ing to wreak havoc in our
tudes toward each other, and proxemics. lives, and even kill us. n
as well as gender, age, and
even climate. In addition, Suggested reading
“contact cultures” use closer interpersonal dis- Kennedy DP, Gläscher J, Tyszka JM, Adolphs R.
Dr George Szasz is a member of tances and engage in more touching; “noncon- Personal space regulation by the human amyg-
the Order of Canada and professor tact cultures” exhibit opposite preferences. In dala. Nat Neurosci 2009;12:1226-1227.
emeritus at the UBC Faculty of ordinary times the amygdala is suspected of Miller G. Social distancing prevents infections, but
Medicine. Throughout his career processing strong reactions to violations of so- it can have unintended consequences. Science.
he practised on the North Shore cial spaces. Now we are facing compulsory social Accessed 8 April 2020. www.sciencemag.org/
and worked for the UBC Faculty of distancing beyond the amygdala and proxemics. news/2020/03/we-are-social-species-how-will
Medicine in numerous positions. We are ordered by public health authorities to -social-distancing-affect-us
After retiring from UBC, he was a create distances between households, neighbor- Wikipedia. Proxemics. Accessed 8 April 2020.
member and chair of the Medical hoods, cities, and even countries. https://en.wikipedia.org/wiki/Proxemics
Advisory Committee of the BC College Overall, people are resilient to short-term
of Physicians and Surgeons. Now in social distancing, although individuals who al-
his 91st year, married for 65 years, ready have problems with loneliness, anxiety,
and caring for his wife with terminal depression, substance abuse, or other health
dementia at home, he continues issues are likely to be vulnerable to even more
rowing at the Vancouver Rowing Club problems. In the short run, understanding the
and writing for the BCMJ blog. purpose of prolonged isolation and having pride
137 BC Medical Journal vol. 62 no. 4 | MAY 2020 137News We welcome news items of less than 300 words; we
• Implementation planning for practices tran-
sitioning from a manual system.
may edit them for clarity and length. News items should be emailed to • Questions to ask dictation software vendors
journal@doctorsofbc.ca and must include your mailing address, telephone when deciding which dictation offering best
number, and email address. Writers should disclose any competing interests. suits your practice.
Many practices have found the initial setup
and ongoing subscription expenses outweighed
by both improved patient care stemming from
more accurate documentation and a more
Doctors of BC COVID-19 improve and standardize the care and follow-up
of people who donate a kidney. Our strategy to efficient documentation process leading to
resource page have the best possible medical care for kidney long-term savings. Those who would like assis-
Doctors of BC has developed a physician donors in the months and years after donation tance with planning dictation software imple-
resource web page to keep members updat- will be achieved through education and col- mentation, improving usage of their current
ed on the COVID-19 work happening at laboration. Our collaborative efforts include system, or engaging with vendors are invited
Doctors of BC, the Ministry of Health, the stakeholder engagement with family physicians, to contact the Doctors Technology Office at
BCCDC, and other organizations. The latest kidney donors, and the care teams involved in dtoinfo@doctorsofbc.ca. The guide is available
information relating to virtual care, member living kidney donation. online at www.doctorsofbc.ca/sites/default/files/
insurance and benefits during the outbreak, We are seeking input from and partner- dto-guide-using_dictation_software_in_
CMPA protections, data from the BCCDC, ship with physicians who either have kidney medical_practices.pdf. https://divisionsoffamily
and more are provided: www.doctorsofbc donors under their care, or have an interest in practice.cmail20.com/t/i-l-xjljutd-jldujuxt-u/.
.ca/working-change/advocating-physicians/ the care of kidney donors. Your involvement in
coronavirus-covid-19-updates. the initiative can range from singular input to New forms guidelines and best practices
Additionally, members are encouraged to continuous participation. If interested, please Creating new forms and updating forms has
send any COVID-19 related questions and email us at shawna.mann3@vch.ca. been a longstanding pain point for physicians,
feedback to covid19@doctorsofbc.ca. clinic staff, EMR vendors, and form creators.
—Shawna Mann, MD, FRCPC
Transplant Nephrology Locum, Vancouver While a provincial e-forms project is under-
Follow-up of living General Hospital way to help address frustrations, the Doctors
kidney donors: A call for Technology Office has developed an interim
Reference guide, Forms Guidelines and Best Practices, to
collaboration 1. BC Transplant. 2019 organ donation and transplanta- assist with creating, editing, and distributing
Kidney donation in British Columbia is on the tion. Accessed 23 March 2020. www.transplant.bc.ca/ forms. The guide offers recommendations for
rise,1 and that means the number of kidney Documents/Statistics/BCT-2019-Stats-FINAL.pdf.
creating and updating forms, how to deter-
donors in the province who require routine or mine whether a form is needed, and how to
specialized follow-up is becoming increasingly News from the Doctors support the updating process. The Doctors of
prevalent. While donors are chosen because of Technology Office Technology Office is available to provide on-
their excellent health status, after kidney dona- going support for forms development and can
tion, these individuals require medical vigilance Guide to using dictation software
help connect form producers with the e-forms
to keep them in optimal health. in medical practices
project team and EMR vendors as needed. For
According to a recent environmental scan, A new resource from the Doctors Technology
questions, guidance, or help on engagement,
the majority of kidney transplant programs Office provides support for physicians who are
contact the Doctors Technology Office at dto
in Canada do not have standardized donor in the process of adopting dictation software
info@doctorsofbc.ca. View the guide online
follow-up. In BC, the current informal model or are considering making the transition. The
at www.doctorsofbc.ca/sites/default/files/
relies heavily on family physicians to follow guide, Using Dictation Software in Medical Prac-
dto-guide-forms_guidelines_best_practices.pdf.
kidney donors on an annual basis to ensure tices, is a collaboration of the Doctors Technol-
that their basic kidney health parameters are ogy Office and the College of Physicians and
Virtual care support
satisfactory. If health concerns arise, the fam- Surgeons of BC’s Physician Practice Enhance-
To assist physicians in employing virtual care
ily physician will either manage the condition ment Program. It outlines:
within their practice, the Doctors Technology
or, if necessary, refer the donor to a specialist. • Benefits of dictation software (with journal
Office has developed a variety of virtual care
The Vancouver Transplant Nephrologists references).
resources. To accommodate increasing requests
and Canadian Blood Services have teamed up to • Types of dictation software.
for immediate support, the office will also be
138 BC Medical Journal vol. 62 no. 4 | MAY 2020You can also read