Smartphones let surgeons know WhatsApp: an analysis of communication in emergency surgical teams
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The American Journal of Surgery (2015) 209, 45-51
Association for Surgical Education
Smartphones let surgeons know WhatsApp: an
analysis of communication in emergency surgical
teams
Maximilian J. Johnston, M.B., B.Ch., M.R.C.S.a,*,
Dominic King, M.B., Ch.B., M.R.C.S.b, Sonal Arora, M.R.C.S., Ph.D.a,
Nebil Behar, M.Sc., F.R.C.S.c, Thanos Athanasiou, Ph.D., F.E.T.C.S.d,
Nick Sevdalis, Ph.D.a, Ara Darzi, M.D., F.R.C.S., F.A.C.S.d
a
Centre for Patient Safety and Service Quality; bCentre for Health Policy, Department of Surgery and
Cancer, St Mary’s Hospital, Imperial College London, London, UK; cDepartment of Surgery, Chelsea
and Westminster Hospital NHS Foundation Trust, London, UK; dDepartment of Surgery and Cancer,
Imperial College London, London, UK
KEYWORDS: Abstract
Communication; BACKGROUND: Outdated communication technologies in healthcare can place patient safety at risk.
Information This study aimed to evaluate implementation of the WhatsApp messaging service within emergency
technology; surgical teams.
Patient safety; METHODS: A prospective mixed-methods study was conducted in a London hospital. All emergency
mHealth; surgery team members (n 5 40) used WhatsApp for communication for 19 weeks. The initiator and
Surgery receiver of communication were compared for response times and communication types. Safety events
were reported using direct quotations.
RESULTS: More than 1,100 hours of communication pertaining to 636 patients were recorded,
generating 1,495 communication events. The attending initiated the most instruction-giving communi-
cation, whereas interns asked the most clinical questions (P , .001). The resident was the speediest
responder to communication compared to the intern and attending (P , .001). The participants felt that
WhatsApp helped flatten the hierarchy within the team.
CONCLUSIONS: WhatsApp represents a safe, efficient communication technology. This study lays
the foundations for quality improvement innovations delivered over smartphones.
Ó 2015 Elsevier Inc. All rights reserved.
Maximilian J. Johnston, Sonal Arora, Dominic King, Nick Sevdalis, and Ara Darzi are affiliated with the Imperial Patient Safety Translational Research
Centre (www.cpssq.org), which is funded by the National Institute for Health Research (40490), UK. The funders had no role in the study. The other authors
declare no conflicts of interest.
This paper was presented at the Association for Surgical Education meeting in Chicago in April 2014 and won a Paper of Distinction Award.
* Corresponding author. Tel.: 144-207-594-7925; fax: 144-207-594-3137.
E-mail address: m.johnston@imperial.ac.uk
Manuscript received April 24, 2014; revised manuscript July 31, 2014
0002-9610/$ - see front matter Ó 2015 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.amjsurg.2014.08.030
46 The American Journal of Surgery, Vol 209, No 1, January 2015
Patient care has been revolutionized by the information 3. Evaluate the response times to communication for
age; the last 2 decades have seen diagnostics and different communication types, domains, and clinician
treatments transformed by widespread technological prog- grades.
ress.1 However, the method by which physicians commu- 4. Explore participant’s perception of WhatsApp for team
nicate with each other remains reminiscent of a period communication.
before smartphones and social media. Apart from certain
hipster parts of New York and London, pager systems
are no longer seen as an effective communication tool Methods
given the obvious advantages of cell phones. Many hospi-
tals still use outdated pager systems as the foundation for Recruitment
clinical communication between physicians, nurses, and
other health care professionals. This is despite problems An acute general surgery team responsible for all
including long waiting-times for the return of a page, emergency admissions in a London (United Kingdom)
high costs, frequent interruptions, and the inability to teaching hospital participated in this study. The nature of
identify the location or identity of the caller.2–4 From a pa- the team’s emergency workload involves rapid assessment,
tient safety perspective, this is of significant concern given management, and discharge of all acute surgical patients.
the fact that poor communication often lies at the heart of All team members were included so no sampling was
an adverse event.5 Although previous studies have evalu- required. An attending, a resident, and 2 interns rotating on
ated communication in acute settings,6,7 the focus has a weekly basis made up the team, meaning 40 team
been on direct or face-to-face communication. The Situa- members participated in the study. Medical students and
tion, Background, Assessment and Recommendation junior residents also joined the team at occasional times for
(SBAR) communication tool has been produced, and education or training.
some interventions evaluating its use have been trialed
but it has not been widely adopted. It remains difficult Details of app
to measure the effect of SBAR implementation as it is a
verbal communication tool.8 WhatsApp is an app, used by more than 500 million
No study available to date has evaluated the use of mobile people worldwide that allows smartphone users to send text
electronic communication in surgical teamsddespite the messages and other types of media (such as videos, voice
fact that many physicians are now jettisoning their hospital messages, and photographs) to their contacts. It also
pagers and using their personal cell phones to facilitate facilitates the creation of groups; this allows multiple users
professional communication.9 Approximately 80% of US phy- to participate in and monitor the conversation. WhatsApp
sicians have smartphone access at work.10 Smartphones are avoids charging for each message by using cellular data plans
built on mobile operating systems and have more advanced and wireless Internet networks; an annual subscription is
connectivity and computing power compared with traditional currently $0.99. For the purposes of this study, participants
mobile phones. WhatsApp (WhatsApp Inc., Mountain View, used the secure wireless network rather than their mobile
CA) is an increasingly popular mobile messaging application data plan when using WhatsApp to ensure security.
(app) available on all smartphone platforms. With its wide-
spread uptake, we believe that WhatsApp represents a disrup-
Project approval
tive innovation in health care communication offering
numerous benefits to clinicians and especially emergency sur-
This project was confirmed as a service evaluation; formal
geons. The unpredictable nature of working as an emergency
ethical approval was not required. Participants used their
surgeon who must be available at all times to manage unstable
own smartphones over the hospital’s secure wireless network
patients alongside performing surgeries and running clinics
and gave informed consent before participation. Approval
places a premium on safe and efficient communication. If
was secured from the hospital’s information governance
the team is to function well and avoid clinical incidents, they
department on the basis of 3 conditions being met:
must be able to communicate swiftly and clearly at all times.5
This study aims to evaluate, for the first time, the use of What- 1. No storage of WhatsApp data on participant devices
sApp for facilitating communication in an emergency surgery beyond the end of the working week was allowed.
setting and discuss its wider application to healthcare. The team attending downloaded and kept a hard
copy in a secure location for record keeping purposes.
2. Patient-identifiable data were omitted from team
Objectives communication on WhatsApp; the patient’s initials
and a brief clinical description allowed team members
1. Identify the common initiators and receivers of to identify the subject of communication without
communication within a team. breaking confidentiality.
2. Establish the types and clinical domains of communi- 3. Professional behavior had to be exercised in all
cation used through WhatsApp. communication on WhatsApp. To facilitate this, all
M.J. Johnston et al. Smartphone communication in surgery 47
participants were offered a weekly induction briefing were analyzed using the chi-square test; data regarding
from the attending detailing the aforementioned condi- response times were analyzed using Kruskal-Wallis and
tions along with practice guidelines. These guidelines Mann-Whitney tests. These analyses evaluate whether
reminded participants of the importance of contempo- certain communication types and clinical domains occurred
raneous documentation of clinical decisions communi- more commonly than others. In addition, standardized qual-
cated via WhatsApp in the clinical notes. itative methodology was used to identify emergent themes
regarding the nature of these communication events. Two
coders used a coding framework to categorize these commu-
Innovation nications, noting in particular where potential patient safety
events had occurred. Such episodes are reported with
WhatsApp was used as the official platform for commu- supporting quotes. Participant’s reflections of using What-
nication after a 2-week pilot period. All communication sApp were captured using semistructured interviews
between team members was captured over a consecutive 19- lasting approximately 10 minutes, conducted at the study
week period (October 2012 to March 2013). Clinicians center, which were analyzed using standard qualitative
continued to be notified of cardiorespiratory arrest and techniques.
periarrest scenarios via the pager device; all other matters
were communicated on WhatsApp. Communication was
stored on the WhatsApp platform itself between 8 AM and 8 Results
PM Monday to Friday. From the stored information, scripts
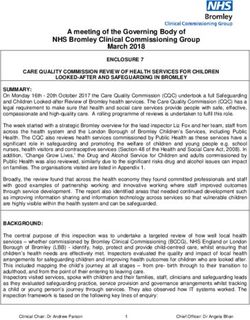
were produced to represent 1 week of communication each. A total of 1,140 hours of clinical communication
pertaining to 636 patients over 95 days was recorded. This
Analysis and statistics yielded 1,495 communication events (a median of 65.5
communication events per week). Of these, 359 came from
After removal of patient-identifiable details by the team’s the attending, 318 from the resident, 784 from the interns,
attending, data were extracted from the scripts regarding the and 34 from other team members. The pattern of commu-
identity of the initiator and receiver of each communication nication from each participant over the course of the study is
event, the response time, communication type, and clinical displayed in Fig. 1. Communication events were grouped
domain of each episode. These communications were then into episodes (n 5 658) and coded according to their type
analyzed to uncover the inner workings of the team. (administrative question, clinical question, information-
Communication events were analyzed using SPSS (version giving, or instruction-giving) and the clinical domain to
20; IBM); statistical significance was taken when P was which they pertained (administration, discharge, education,
less than .05. Data regarding communication frequency investigations, prescribing, theater, or ward care).
Figure 1 A line chart showing the frequency of communications per week by each grade and the total number.48 The American Journal of Surgery, Vol 209, No 1, January 2015 Figure 2 A diagram showing the frequency and direction of communication events. (For interpretation of the references to color in this Figure, the reader is referred to the Web version of this article.) Initiators and recipients of communication Interns initiated the most communication episodes (413; 64.9%) followed by the attending (151; 23.7%) and resident (72; 11.3%). Other team members initiated the remaining episodes. For episodes where the intended receiver was not specified or multiple receivers were specified, the receiver was classified as ‘‘team’’; hence, the greater number of received episodes than initiated. The team received the most communication episodes (269; 38.7%) followed by the attending (196; 28.2%), the resident (132; 19.0%), and the interns (98; 14%; Fig. 2). Types of communication events In terms of frequency, clinical questions formed the most common type of communication event (417; 39.3%) followed by information-giving comments (378; 35.6%), instruction-giving comments (207; 19.5%), and adminis- trative questions (60; 5%). Clinical questions (n 5 417; chi-square 5 248; P , .001), administrative questions (n 5 60; chi-square 5 7.75; P 5 .02), and information- giving comments (n 5 378; chi-square 5 192; P , .001) were most likely to be initiated by interns. The ‘‘team’’ received more information-giving comments than any other communication type (n 5 269; chi-square 5 93; P , .001). An example of an instruction-giving comment can be Figure 3 A WhatsApp screenshot showing instruction-giving seen in Fig. 3. Often, several different types of communica- communication. (For interpretation of the references to color in tion were combined in a single communication episode this Figure, the reader is referred to the Web version of this (Fig. 4). article.)
M.J. Johnston et al. Smartphone communication in surgery 49
differences between the attending vs resident (P , .001),
attending vs intern (P , .001), and resident vs intern
(P 5 .007).
There was also a significant difference between response
times according to the type of communication [H(3) 5
13.05; P 5 .005). In particular, this response time differed
with regard to administrative questions (median 1 minute)
vs clinical questions (5 minutes; P 5 .006), instruction-
giving comments (2.5 minutes) vs clinical questions
(5 minutes; P 5 .003), and information-giving comments
(3 minutes) vs instruction-giving comments (2.5 minutes;
P 5 .019).
There was a significant interaction between grade and
response time for clinical questions in that the attending
responded slower than residents and interns [H(2) 5 28.9;
P 5 ,.001]. Testing the response times according to the
clinical domain of communication episodes revealed no
significant differences between the various types [H(6) 5
3.5; P 5 .739].
Qualitative analysis of reflective comments
Participants were asked to reflect on the use of Whats-
App. Interns felt that the ability to send a quick message
rather than make a phone call was helpful: ‘‘I like being
Figure 4 A WhatsApp screenshot from the intern’s handset able to send a message about basic questions that require a
showing different types of communication and a potential patient simple answer, it is reassuring’’. The attending was grateful
safety event. (For interpretation of the references to color in this for the increased level of supervision WhatsApp gave him:
Figure, the reader is referred to the Web version of this article.) ‘‘The fact that I can constantly monitor what my team is
doing for my patients allows me to step in when needed but
leave them to it at other times.’’ The resident felt that
Clinical domain of communication events WhatsApp helped to remove communication barriers be-
tween junior and senior colleagues ‘‘I feel that this system
Most communication episodes concerned ward care and has encouraged the juniors to keep us updated, even about
investigations. Requests for clinical assistance or advice things they think are minor. They may not take the trouble
were often the focus of ward care communication: ‘‘Patient to page us with informative updates to avoid disturbing us
EH in High Dependency - I’m worried she’s got pulmonary in theater but are very happy to send a WhatsApp
edema. I’ve stopped fluids, started Oxygen, ordered a chest message.’’ The team has decided to continue using Whats-
x-ray and giving 20mg IV Furosemide [Lasix]’’ (intern). App in the future.
‘‘Good. Please get urgent Medical review’’ (attending).
Although prescribing questions were not very common,
some were vital for patient safety: ‘‘Shall I restart Aspirin Comment
and Clopidogrel [Plavix] for sub-arachnoid hemorrhage
patient who is going home?’’ (intern). ‘‘No, don’t restart. Principal results
Please check with Cardiology’’ (attending).
This study explored the use of WhatsApp by an
emergency general surgery team in London using both
Response times quantitative and qualitative methodology. This is the first
study of its kind that investigates how such a communi-
The attending responded to 193 communication epi- cation system operates within a clinical team and quan-
sodes in a median time of 7 minutes, the resident to 174 tifies both the direction and type of communication
communication episodes (median 2 minutes), and interns between doctors. Most communication initiated by interns
to 177 communication episodes (median 3 minutes). The was information giving or a clinical question, whereas
difference in these response times among the professional more senior team members provided instruction-giving
grades was statistically significant [H(2) 5 41.3; P , comments. Clinical questions were responded to more
.001], with subgroup analyses revealing significant slowly than other types of communication and this may be50 The American Journal of Surgery, Vol 209, No 1, January 2015
because of their relative complexity compared with other This study involved an entire population rather than a
communication types. A simple administrative question or sample, eliminating the potential for participant bias.
instructive comment may only require a short, quick Consecutive weeks of data collection mean that selection
response, but a clinical question often requires a doctor bias was also not an issue. There was no observer bias or
to review a patient or at least check a test result; therefore, measurement bias on the ability to record; date and time
the reply takes longer. In general, the attending took stamp clinical communications removed any interpretation
longer than the other team members to reply to commu- error. Detailed qualitative analysis of team perceptions
nication, which may be a reflection of higher workload. allowed in-depth exploration of the participant’s receptive-
This is important from the patient perspective as the ness to WhatsApp. The statistical analysis presented in this
attending is responsible for the team and must be study allows the crucial role of hierarchy within the team to
contacted when definitive decisions about patient care be explored in detail, something that has not previously been
need to be made.11 researched in surgical teams outside of the operating room.
The greatest potential benefit from using systems such as
Comparison with prior work WhatsApp is the increased involvement and supervision
from the attending surgeon. However, as this work is taken
There is a paucity of literature that examines health care forward, care must be taken to ensure that the autonomy of
worker’s response times to communication; this is an other decision makers in the team (such as the resident) is
important subject and deserves greater focus. Research on preserved to avoid prolonging their learning experience.
medical emergency teams has revealed that ineffective The use of a single center and exploration of communi-
communication methods can lead to treatment delays and cation in emergency surgery only may limit the application
failed escalation of care.12,13 Worse still, studies have of the findings to other hospitals and specialties. There was
highlighted that patients are subject to significant harm an absence of out-of-hours communication in this study,
because of poor communication.14,15 Human factors such and further work is required to evaluate the use of WhatsApp
as hierarchical barriers and inadequate information transfer and other communication tools between different health
techniques contribute to these failures.16 In this study, the care staff (eg, nurses). There was no comparison of any
threat to patient safety presented by these factors was suc- communication outside the WhatsApp platform or an
cessfully overcome through the use of WhatsApp. assessment of the quality of communication; these areas
The fact that almost all health professionals in the were outside the scope of this study. Furthermore, the
United States of America and the United Kingdom now communication pathways may be different in private health
carry cell phones (and increasingly smartphone devices) care institutions, limiting the generalizability of the findings
has disrupted the way many clinical teams are communi- to academic centers. Consideration of wireless network
cating. WhatsApp represents a successful technological coverage and hospital dead zones (areas without wireless
innovation that effectively replaced the pager over a short service) will be needed as this system is expanded into other
time period and continues to be used well after the period clinical areas and institutions.
this trial ended. The findings of this study are in
agreement with research showing that handheld computers Conclusions
improve efficiency, clinical decision making, and docu-
mentation practice.17 These positive aspects may have an The findings of this study provide a novel and detailed
effect on the quality and safety of health care delivery. examination of the communication between members of a
Future research could seek to determine how well commu- clinical team. It meets the current need for evaluation of
nication tools such as SBAR and innovations such as communication methods in healthcare.21 The WhatsApp
WhatsApp work together. Successful interventions in platform was deemed to be user friendly and was exten-
this area should aim to include strategies for improve- sively used to facilitate communication within a team
ments in both the content (eg, SBAR) and mode (Whats- where junior physicians rotate on a weekly basis. In addi-
App) of communication. tion, significant benefits were realized through a system
Change efforts in healthcare are often ambitious and use in which senior physicians had a constant overview of ac-
a whole-system goal18; the use of a more modest initial tivities undertaken within their team without active interfer-
target in this study may have contributed to its success. ence, allowing their juniors to develop a degree of clinical
Computer-based innovations supporting decision making independence at minimal risk to patient safety. WhatsApp
have been successful in improving the safety of medication also provides an added benefit of providing a record of
prescribing. The barriers overcome by these systems, of communication for audit and training purposes. Although
which WhatsApp is an example, may be a platform for there is some concern around the use of mobile messaging
further successful innovation in the health care communica- services in transferring sensitive data,22 strict information
tion sector.19 Further development of health care communi- governance policies and a cautious approach to confidenti-
cation technology will need to include the integration of ality and safety will enable the beneficial aspects of such
direct access to patient information.20 communication platforms to be made widely available.23M.J. Johnston et al. Smartphone communication in surgery 51
WhatsApp was universally accepted as a simple and 9. Franko OI, Tirrell TF. Smartphone app use among medical providers
efficient frugal innovation for communicating within a in ACGME training programs. J Med Syst 2012;36:3135–9.
10. Payne KB, Wharrad H, Watts K. Smartphone and medical related app
surgical team. It helped flatten the traditional hierarchy use among medical students and junior doctors in the United
between team members, thereby overcoming the human Kingdom (UK): a regional survey. BMC Med Inform Decis Mak
factor barriers to effective communication. Increased 2012;12:121.
connectedness between team members allowed junior 11. Silverman AT, Goldfarb MA, Baker T. When should a surgical resident
trainees to have easy access to a more experienced call an attending surgeon? J Surg Educ 2008;65:206–12.
12. Cioffi J, Salter C, Wilkes L, et al. Clinicians’ responses to abnormal vital
clinician, which provided them with greater support and signs in an emergency department. Aust Crit Care 2006;19:66–72.
supervision. This study illustrates the potential for simple 13. Peebles E, Subbe CP, Hughes P, et al. Timing and teamwork
technological innovation to improve patient safety. In dan observational pilot study of patients referred to a rapid
doing so, it lays the groundwork for both technology response team with the aim of identifying factors amenable to
development and subsequent testing in the clinical re-design of a rapid response system. Resuscitation 2012;83:
782–7.
environment. 14. Lingard L, Espin S, Whyte S, et al. Communication failures in the
operating room: an observational classification of recurrent types
and effects. Qual Saf Health Care 2004;13:330–4.
15. Nagpal K, Arora S, Abboudi M, et al. Postoperative handover:
References problems, pitfalls, and prevention of error. Ann Surg 2010;252:
171–6.
1. Powell-Cope G, Nelson AL, Patterson ES. Patient care technology and 16. Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures:
safety. In: Hughes RG, ed. Patient Safety and Quality: An Evidence- an insidious contributor to medical mishaps. Acad Med 2004;79:
based Handbook for Nurses. Rockville, MD: Agency for Healthcare 186–94.
Research & Quality (AHRQ); 2008. 17. Mickan S, Tilson JK, Atherton H, et al. Evidence of effectiveness of
2. Coiera E, Tombs V. Communication behaviours in a hospital setting: health care professionals using handheld computers: a scoping review
an observational study. BMJ 1998;316:673–6. of systematic reviews. J Med Internet Res 2013;15:e212.
3. Wu R, Rossos P, Quan S, et al. An evaluation of the use of smart- 18. Macfarlane F, Barton-Sweeney C, Woodard F, et al. Achieving and
phones to communicate between clinicians: a mixed-methods study. sustaining profound institutional change in healthcare: case study us-
J Med Internet Res 2011;13:e59. ing neo-institutional theory. Soc Sci Med 2013;80:10–8.
4. Nguyen TC, Battat A, Longhurst C, et al. Alphanumeric paging in an 19. Brigic A, Bloor J, Clark A, et al. How will health-care organizations
academic hospital setting. Am J Surg 2006;191:561–5. meet venous thromboembolism targets? Br J Hosp Med 2011;72:
5. Nagpal K, Arora S, Vats A, et al. Failures in communication and infor- 35–8.
mation transfer across the surgical care pathway: interview study. BMJ 20. Whittaker R. Issues in mHealth: findings from key informant inter-
Qual Saf 2012;21:843–9. views. J Med Internet Res 2012;14:e129.
6. Lingard L, Regehr G, Espin S, et al. A theory-based instrument to eval- 21. McElroy LM, Ladner DP, Holl JL. The role of technology in clinician-
uate team communication in the operating room: balancing measurement to-clinician communication. BMJ Qual Saf 2013;22:981–3.
authenticity and reliability. Qual Saf Health Care 2006;15:422–6. 22. Schrittweiser SF, Kieseberg P, Leithner P, et al. Guess who’s texting
7. Sevdalis N, Wong HW, Arora S, et al. Quantitative analysis of intrao- you? Evaluating the security of smartphone messaging applications.
perative communication in open and laparoscopic surgery. Surg En- Annual Network & Distributed Security System Symposium; 2012;
dosc 2012;26:2931–8. San Diego, USA.
8. Marshall S, Harrison J, Flanagan B. The teaching of a structured tool 23. Rodrigues JJ, de la Torre I, Fernandez G, et al. Analysis of the security
improves the clarity and content of interprofessional clinical commu- and privacy requirements of cloud-based electronic health records sys-
nication. Qual Saf Health Care 2009;18:137–40. tems. J Med Internet Res 2013;15:e186.You can also read