Sexually Transmitted Infections: What is new in 2022 for OBGYNs? - The webinar will begin shortly.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Sexually Transmitted Infections:
What is new in 2022 for OBGYNs?
The webinar will begin shortly.
This webinar is sponsored by the NYC STD Prevention Training Center (PTC)
NYC STD Prevention Training Center
NYC STD Prevention Training Center
The CDC-funded NYC STD Prevention Training Center at Columbia University
provides a continuum of education, resources, consultation and technical
assistance to health care providers, and clinical sites. www.nycptc.org
Didactic Presentations Clinical Consultation Warmline
Webinars, conferences, trainings Clinical guidance regarding STD cases; no
and grand rounds presentations to identifying patient data is submitted
enhance and build knowledge www.stdccn.org
Technical Assistance Resources
Virtual and on-site technical assistance regarding Clinical guidance tools regarding the STD
quality improvement, clinic implementation and treatment guidelines, screening
best practices around sexual health provision algorithms and knowledge books, such
For more information please contact:
as the Syphilis Monograph.
Gowri Nagendra Soman MPH To download a copy please visit:
gn103@cumc.columbia.edu http://bit.ly/SyphilisMonograph2019PTC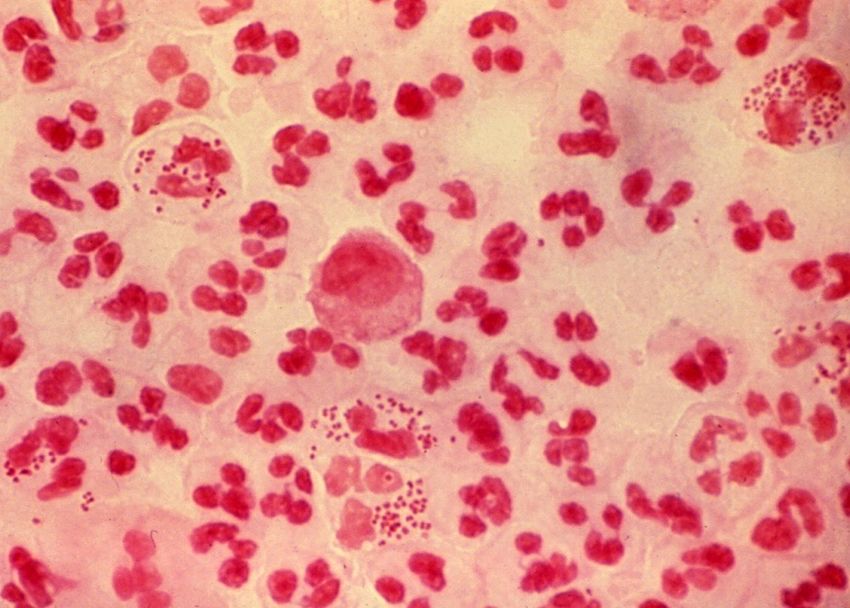
Housekeeping
• Please be sure to remain on mute during the webinar
• Please send your question(s) Q&A chatbox and not the chat. We will do
our best to address questions.
Continuing Education
• Continuing Education is available through the CDC Training and Education Online
System for the live webinar. This is a separate system from your registration.
• Instructions for completing evaluation and obtaining CE will be emailed to
attendees after the webinar.
• Deadline for obtaining CE is May 28th 2022.
WEBINAR RECORDING
• Today’s webinar is being recorded and you will receive a link to the presentation at
a later date.
NYS and NYC STI Epidemiology Gale Burstein, MD, MPH, FAAP Commissioner of Health, Erie County, NY Clinical Professor of Pediatrics, Jacobs School of Medicine Buffalo, NY NYC STD Prevention and Training Center

2020 STI Diagnoses Highlighted for New York State 6
(excluding New York City)
CHLAMYDIA GONORRHEA EARLY CONGENITAL
SYPHILIS SYPHILIS
- 14.8% + 45% - 6.7% + 20%
2019: 48,183 | 2020: 41,032 2019: 11,923 | 2020: 17,291 2019: 1,582 | 2020: 1,478 2019: 10 | 2020:12
First decrease after 5 6 consecutive years of First decrease after 9 4 consecutive years of
consecutive years of increases increases consecutive years of increase increase
60% 55% 20% 82%
18%
decrease in 66%
increase
among
of diagnoses
among
increase in
females
of diagnoses
among males 77.8%
males females males of potential
of diagnoses
among 11% congenital syphilis
cases were averted in
13% females
69%
decrease in males
2020
decrease in
females increase in 38%
cases in the decrease in cases
* Regional data displays region with the largest Rochester Region* in the Central Region* Office of Sexual Health and Epidemiology
percent change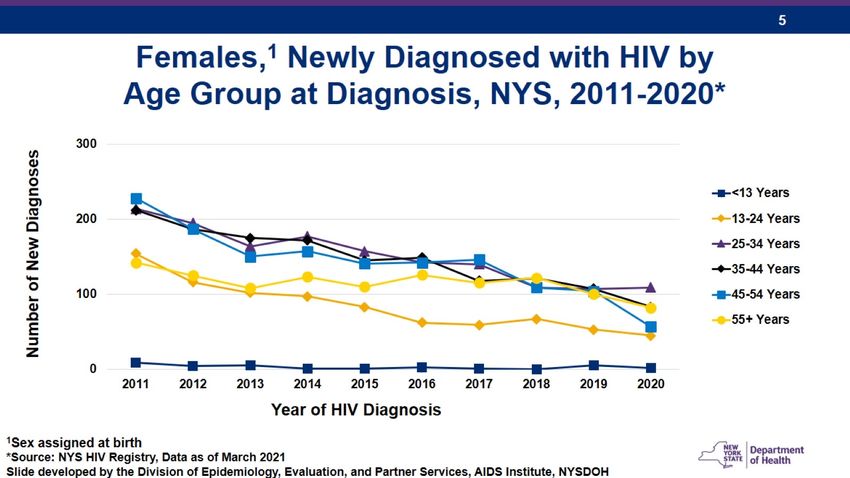
Congenital syphilis cases and primary & secondary syphilis diagnoses among persons
7
of reproductive capacity, NYS (excluding NYC), 2020
Number of Primary & Secondary Syphilis diagnoses
among persons of reproductive capacity (n = 424)
0 cases 4 - 14 cases
1 - 3 cases > 14 cases
Congenital Syphilis Cases
(n = 53)
* Colors among non-zero case counties were determined using quartiles Office of Sexual Health and Epidemiology
NYC STI Overview
8
• After several years of STI increases in NYC Health Department, large
decreases observed in chlamydia and gonorrhea rates in 2020 vs 2019
• Decreases in selected STI rates likely related to COVID-19 public health
emergency
o Reduced STI detection due to combination of reduced screening and testing and
decreased transmission
• Among reported STI cases, notable inequities persist
https://www1.nyc.gov/assets/doh/downloads/pdf/std/sti-2020-report.pdf Office of Sexual Health and Epidemiology
Number and percentage of congenital syphilis-related pregnancies related9 to
syphilis acquired during pregnancy, NYC, 2010-2020
Other missed opportunities:
• Lack of prenatal care
25 • Inadequate syphilis treatment during pregnancy 100%
Number of pregnancies linked to congenital
% related to syphilis acquired in pregnancy
• Missed syphilis screening
• Errors in public health response to syphilis laboratory results
20
75%
15
syphilis
50%
10
25%
5
0 0%
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Year
Office of Sexual Health and Epidemiology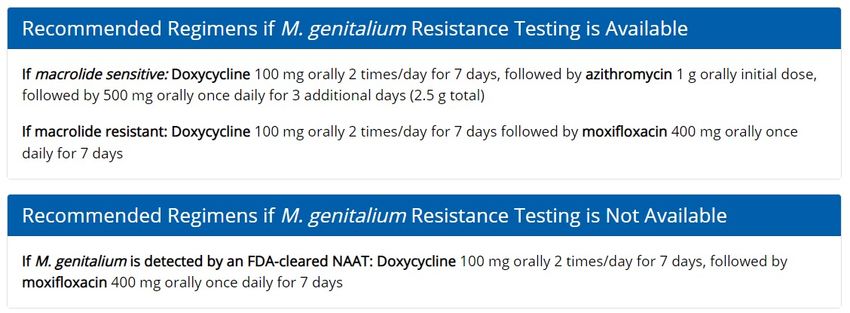
Characteristics of pregnant people linked to congenital syphilis cases
(n = 129), NYC, 2010-2020
Characteristic Number Percentage
Age group (years)
15 – 19 9 (7.0)
20 –29 77 (59.7)
30 – 39 37 (28.7)
40 – 49 6 (4.7)
Race/ethnicity
Black, non-Hispanic/Latino 63 (49.2)
Hispanic/Latina 34 (26.6)
White, non-Hispanic/Latino 9 (7.0)
Asian, non-Hispanic/Latino 5 (3.9)
Other 17 (13.3)
Country of birth
Born outside of the US 52 (46.4)
Born in the US 60 (53.6)
Area-based poverty level
Low (Syphilis
11
• Syphilis is increasing among NYC women, especially young women of
color
• Congenital syphilis is a sentinel event because it represents system
failures, usually at multiple levels: patient, provider, hospital, public health
system
• Pregnant New Yorkers must be screened for syphilis 3 times
o At first prenatal examination (NYS law)
o During 3rd trimester between 28-32 weeks (NYC regulation) (NYS bill)
o At delivery (NYS law)
Office of Sexual Health and Epidemiology12
STI Clinical Updates
Elana Tal, MD, MS
Clinical Assistant Professor of Obstetrics and Gynecology
Complex Family Planning
Jacobs School of Medicine and Biomedical Sciences
Buffalo, NY
I have no relevant financial relationships with the manufacturer(s) of any commercial
product(s) and/or provider(s) of commercial services discussed in this CME activity.
I do not intend to discuss an unapproved/investigative use of a commercial
product/device in my presentation.X
Outline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancySyphilis
Syphilis: diagnosis
• Diagnosis requires non-treponemal (eg RPR) + treponemal
• Traditional algorithm = non-treponemal à treponemal
• Reverse algorithm = treponemal à non-treponemal
• Non-treponemal titers used to follow response to treatment
• Treponemal tests often positive for life
• Make friends with ID, lab, and/or health departmentSyphilis: diagnosis
• Atypical presentations are more common than previously thought
• 50% have multiple lesions
• 37% have painful lesions
• Consider syphilis if HSV is negative
• RPR takes 14-21 days to turn positive
• Bring back patients with ulcers to review results and possibly retest
• Consider treponemal testSyphilis: treatment
Penicillin Allergy
Non-pregnant: doxycycline 100 mg PO BID x 14 day
Pregnant: desensitization and penicillinSyphilis in pregnancy: diagnosis
• Maternal testing @ NOB, ~28 weeks, delivery
• UNIVERSAL 3rd trimester screen
• Get detailed ultrasound if patient diagnosed >20 weeks
• Evidence of fetal or placental syphilis increases risk of treatment failure
• Signs include fetal hepatosplenomegaly, ascites, hydrops, anemia, thickened
placenta
• Repeat testing at delivery for any stillbirth >20 weeks
• Neonates should not be discharged from hospital without maternal
RPR resultSyphilis in pregnancy: treatment
• Adequate maternal treatment = PCN initiated at least 30 DAYS before
delivery
• Give 2nd dose of PCN to reduce risk of congenital syphilis
• Need to restart series if >9 days since last doseSyphilis in pregnancy: Jarisch-Herxheimer reaction
• Acute febrile reaction with headache, myalgia, rash, hypotension
• Due to endotoxin release
• Onset usually within 1-2 hours of treatment, peak at 8 hours, resolve
24-48 hours
• Associated with contractions, preterm labor, NRFHT (stillbirth is rare)
• CFM is recommended for treatment after viabilitySyphilis Key Points • What’s new: increase in congenital syphilis • What to do: be diligent about diagnosis and treatment during pregnancy to prevent congenital syphilis
Gonorrhea
Gonorrhea: diagnosis
• NAAT preferred
• Clinician-collected and patient-collected vaginal swabs equivalent in
sensitivity and specificity
• First-void urine or liquid based cytology for Pap smears acceptable
• With test for chlamydia
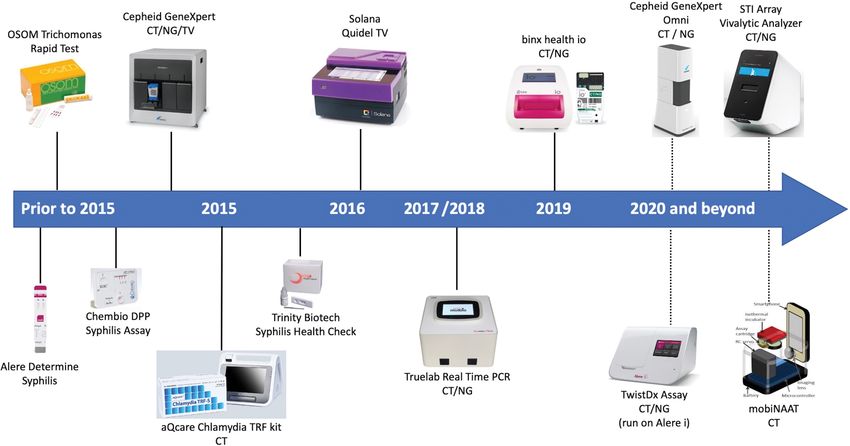
• If cephalosporin resistance suspected, do culture with sensitivitiesPoint of care tests
Visby Medical
Sexual Health
Click TestGonorrhea: treatment New
Penicillin Allergy
Gentamicin 240 mg IM + Azithromycin 2 g PO
[Cross reactivity with 2nd and 3rd generation
cephalosporin isGonorrhea: resistance
Gonorrhea: resistance
https://www.cdc.gov/drugresistance/pdf/threats-report/gonorrhea-508.pdfGonorrhea: new potential treatments • Solithromycin (macrolide) • Zoliflodacin (topoisomerase inhibitor) • Gepotidacin (triazaacenaphthylene) • Chlosthioamide (DNA gyrase inhibitor)
Gonorrhea: follow-up
• TOC only if pharyngeal infection or symptoms do not resolve
• CDC recommends pharyngeal swab for patients with urogenital gonorrhea
who report oral sex
• Retest in 3 months for reinfection
• Retest in 3rd trimester if pregnant
• Notify health department of treatment failuresGonorrhea Key Points • What’s new: increased drug resistance • What to do: treat with ceftriaxone 500 mg IM (1000 mg if >150 kg)
Chlamydia
Chlamydia: treatment New
Chlamydia: treatment
• 567 male and female participants with urogenital
chlamydia
• Directly observed therapy
• Cure rate 100% in doxycycline group vs 97% in
azithromycin groupChlamydia: treatment
• 625 men who have sex with men with rectal chlamydia
• Cure rate 97% in doxycycline group vs 77% in azithromycin groupChlamydia: treatment
• 416 female patients self-collected vaginal and rectal swabs
• High rates of coinfection (77%) despite low report of recent anal
intercourse (3%)
• Cure rate for urogenital chlamydia 95% in doxycycline group vs
94% in azithromycin group
• Cure rate for rectal chlamydia 96% in doxycycline group vs 79% in
azithromycin groupChlamydia: treatment
• Azithromycin is effective at genitourinary sites
• BUT high rates of rectal chlamydia in patient with genital infections
• AND doxycyline is superior in anorectal chlamydia cure
• Link between persistent rectal chlamydia and urogenital chlamydia
unclear, but complete eradication is the goalChlamydia: treatment
Azithromycin Doxycycline
Benefits of azithromycin Benefits of doxycycline
- Directly observed therapy - Higher cure rates for rectal chlamydia
Benefits
- On site administration with no need for
pharmacy
- More privacy from partners and parents
Drawbacks of azithromycin Drawbacks of doxycycline
- Lower cure rates for rectal chlamydia - Lack of adherence (14 pills, risk of
Drawbacks
esophagitis)Chlamydia Key Points • What’s new: recognition of rectal chlamydia and superiority of doxycycline for this site • What to do: treat with doxycycline 100 mg BID x 7 days in non-pregnant patients
Trichomoniasis
Trichomoniasis: diagnosis
• No universal screening recommendation
• Liberal testing with NAAT advisable for
patients at risk
• If concern for resistance:
• Obtain InPouch TV culture medium from
CDC to send for testing
• In the meantime keep escalating treatmentTrichomoniasis: treatment New
Trichomoniasis: treatment
• 623 female participants
• Retest at 4 weeks more likely to be negative in 7-day-dose group
(11%) than the single-dose group (19%)Trich Key Points • What’s new: data showing superiority of 1 week of metronidazole over single dose • What to do: treat female patients with metronidazole 500 mg BID x 7 days
Pelvic Inflammatory Disease
PID: treatment New
PID: treatment
• 233 female participants
• No difference at 3 days
• At 30 days, metronidazole group were less likely to have endometrial
anaerobes, pelvic tenderness, or M. genitaliumPID: follow-up
• IUDs should not be routinely removed
• Outpatients should be re-evaluated 3 days
• Sex partners from last 60 days should be evaluated and/or
presumptively treated for gonorrhea and chlamydia regardless of
patient results
• Retest in 3 monthsPID Key Points • What’s new: data showing benefits of metronidazole • What to do: add metronidazole to regimens
Expedited Partner Therapy
Expedited partner therapy
• For gonorrhea, chlamydia, or trichomoniasis
• Cefixime 800 mg PO once ± doxycycline 100 mg BID x 7 days
appropriate for gonorrhea if partner cannot access ceftriaxone
IM
• Can call in or write script if have partner’s name and DOB
• Can write for “Expedited Partner” with DOB 1/1/1901 if
unknown
• Write “EPT” in notes field
• Okay to prescribe to minors
https://www.health.ny.gov/publications/21282.pdfMycoplasma genitalium
Mycoplasma genitalium
• Common cause of non-gonococcal urethritis in men
• Weak data show associations with cervicitis, PID, infertility,
spontaneous abortion, preterm birthMycoplasma genitalium: diagnosis
• NAAT
• Wide macrolide resistance
• Culture takes months, only available in
research settings
• Molecular markers of resistance under
evaluation
• Screening of asymptomatic people is
not recommended
• Beware STI panels
• Test in cases of recurrent cervicitis,
consider for PIDMycoplasma genitalium: treatment
If no resistance testing and no access to moxifloxacin, use
doxycycline then azithromycin regimen and do TOC in 3 weeksMycoplasma genitalium Key Points • What’s new: mycoplasma genitalium • What to do: look out for more guidance in coming years
Hepatitis C
Hepatitis C: screening in pregnancy New
Metronidazole and alcohol
Metronidazole and alcohol
• Not necessary to advise patients to abstain from alcohol
Fjeld H, Raknes G. Er det virkelig farlig å kombinere metronidazol og alkohol? [Is combining metronidazole and
alcohol really hazardous?]. Tidsskr Nor Laegeforen. 2014 Sep 16;134(17):1661-3. Norwegian.Fluconazole in pregnancy
Fluconazole in pregnancy
• Increased risk of heart defects
after 1st trimester exposure
(OR 1.79, 95% CI 1.18-2.71)
• Use topical insteadOutline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
Diligently screen all
• Syphilis
pregnant people
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea Ceftriaxone 500-1000 mg IM
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia Doxycycline 100 mg BID x 7 days
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia
Metronidazole 500 mg BID x 7 days
• Trichomoniasis
for women
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
Add metronidazole
• PID
to regimens
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium Be aware of it
• Hepatitis C
• Metronidazole and alcohol
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol No need to abstain
• Fluconazole in pregnancyOutline
• Syphilis
• Gonorrhea
• Chlamydia
• Trichomoniasis
• PID
• Mycoplasma genitalium
• Hepatitis C
• Metronidazole and alcohol
Avoid PO especially
• Fluconazole in pregnancy
in 1st trimesterHSV
HSV
• No updates in 2021
• Chronic, lifelong viral infection
• Symptoms are self-limited, recurrent, painful, vesicular or
ulcerative lesions
• Many infections are asymptomatic
• Increasing proportion of anogenital HSV infections
attributable to HSV-1
• HSV-1 less likely to cause recurrences or subclinical viral sheddingHSV
…
• Significant emotional
component to diagnosis
…
• Can be challenging to
counsel patients
• CDC has very helpful
…
guidance re counseling
points
• Support groups existHSV
• Screening among the general population is NOT recommended
• Viral detection tests:
• NAAT from lesions are most sensitive
• Culture sensitivity is low especially as lesions are healing
• Important to know if HSV-1 vs HSV-2 to counsel about what to expect
with recurrences or need for suppressive therapy
• Antibody detection tests:
• HSV-2+ means +genital infection
• HSV-1+ harder to interpret because identified from oral or anogenital
infectionsHSV
• Treatment depends on indication
• Valacyclovir has least frequent dosing
Indication Valacyclovir dosing
Primary (non-pregnant or 1 g BID x 7-10 days
pregnant)
Episodic 500 mg BID x 3 days
1 g QD x 5 days
Suppressive (non-pregnant) 1 g QD
Suppressive (pregnant) 500 mg BIDYou can also read