Scotland's Out-of-Hospital Cardiac Arrest Strategy 2021-2026 - March 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Scotland’s Out-of-Hospital
Cardiac Arrest Strategy 2021-2026
March 2021
Scotland’s Out of Hospital Cardiac Arrest Strategy
1. Foreword
2. Introduction
a. Progress to date
b. Partners to the strategy
c. Covid-19
3. Summary of the Strategy aims
Pathway for survival:
4. Getting Scotland Ready - We will ensure people in Scotland can identify the signs of a cardiac arrest.
5. Bystander Action - We will encourage an increased willingness to call 999, deliver bystander CPR and defibrillation among
people who witness an out-of-hospital cardiac arrest.
6. Hospital Care - We will ensure patients receive high-quality, person-centred care.
7. Aftercare - We will ensure that people in Scotland affected by out-of-hospital cardiac arrest receive appropriate aftercare.
8. Data and Innovation – We will ensure access to timely, high quality data to facilitate open review, discussion, learning and
action planning.
Conclusion and Annexes
9. Conclusion
10. Annex A: Overlapping strategies
11. Annex B: Glossary
12. Annex C: References
1
Strategy Foreword
Mairi Gougeon, Minister for Public Health and Sport
Every year, over 3,000 people in Scotland experience an out-of-hospital cardiac arrest (OHCA). A
cardiac arrest is when the heart stops pumping blood around the body, commonly because of a
problem with the electrical signals in a person’s heart. It is a significant healthcare challenge and
addressing it is a priority for the Scottish Government.
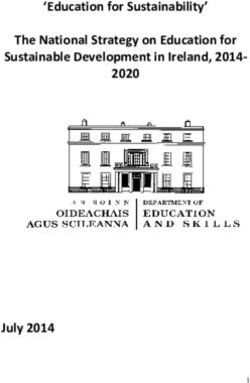
Throughout the last five years, the Save a Life for Scotland (SALFS) partnership has equipped over 640,000
people, around 11% of the population of Scotland, with CPR skills. At the launch of Scotland’s inaugural Out-of-
Hospital Cardiac Arrest Strategy in 2015 only around 1 in 20 people in Scotland who experienced an OHCA
survived to be discharged from hospital. By the end of that strategy in 2020, this had doubled to 1 in 10 Mairi Gougeon, Minister for Public
people. This is significant progress, of which we should be proud. It means that we begin this refreshed Health and Sport
strategy with a solid foundation on which to continue our work.
Whilst we rightly celebrate those achievements, there remains more to do. We know from international experience that even higher rates of
survival are achievable. We can continue to learn from our international colleagues and apply examples of best practice here in Scotland.
Likewise, we can share our experiences of improving bystander CPR rates and survival from OHCA to help other countries do the same.
We also know that there is more that we must do to address inequalities within bystander CPR rates and outcomes from out-of-hospital cardiac
arrest across Scotland. To do this, our refreshed strategy will continue our efforts to equip as many people as possible with the skills necessary
to save the life of someone having a cardiac arrest, but will include a particular focus on reaching communities where we know those
inequalities exist.
In order to ensure as many people as possible survive an OHCA, this strategy follows what is known as the ‘Chain of Survival’. The Chain of
Survival describes the crucial elements required to save a life when someone is in cardiac arrest. These elements are: community readiness
and early recognition that a cardiac arrest is happening; early cardiopulmonary resuscitation (CPR); early defibrillation to restart the heart;
timely hospital care, and appropriate aftercare. Through the implementation of this strategy, we will work to improve all aspects of the Chain of
Survival in Scotland. We will also focus on how the effective use of data can support us in shaping the quality of care delivered to communities
across Scotland.
I would like to offer my thanks and appreciation to all who have been involved in delivering the ambitious aims set out in Scotland’s original Out-
of-Hospital Cardiac Arrest Strategy, to those who have supported this refreshed strategy and, of course, to every
member of the public who has learned CPR and those who have stepped forward to help someone experiencing a
cardiac arrest.
2
Figure 1: A graphic to display the outcomes from the original strategy – Scotland’s Out of Hospital Cardiac Arrest 2015 – 2020.
3
Introduction
Scotland’s Out-of-Hospital Cardiac Arrest Strategy 2021-2026
Each year in Scotland over developed the ‘Out-of-Hospital Cardiac outcomes, co-production (at an
3,000 people have resuscitation Arrest, A Strategy for Scotland 2015 - organisational level), using and sharing
attempted in the community after they 2020’ 5. That strategy was launched by assets (primarily organisational assets)
have a cardiac arrest 1. This is known Maureen Watt, Minister for Public and [adopting] a system-wide
as an Out-of-Hospital Cardiac Arrest Health, in 2015. approach” 8.
(OHCA). Unfortunately only 1 in 10
people survive such an event 2. Since 2015, significant progress has More detail on the achievements of the
been made. Out-of-Hospital Cardiac Arrest, A
We know from other countries around Strategy for Scotland 2015 – 2020 can
the world, with similar populations and We achieved our aim of equipping an be found in the end of strategy report
healthcare systems, that it is possible additional 500,000 people living in at savealife.scot/2015strategyreport .
for more people to survive. In some Scotland with CPR skills, and survival
places 25% of people who have an after OHCA has increased significantly. It takes a system
OHCA will survive to leave hospital 34. Before the launch of the first Strategy
in 2015, only around 1 in 20 people Saving lives after OHCA requires a
With this refreshed strategy, we intend survived to leave hospital after OHCA. whole system of care. The necessary
to further increase survival after OHCA By 2020 this number had doubled to 1 sequence of events starts with
in Scotland. in 10 6. community readiness and bystander
action, continues with trained
The inaugural Out of Hospital Our approach was also recognised as community responders and
Cardiac Arrest Strategy (2015-2020) best practice by international bodies paramedics, and ends with in-hospital
including the Global Resuscitation care and aftercare on returning to the
In 2014 Michael Matheson, then Alliance 7. community. This time-critical sequence
Scottish Government Minister of Public is often described as the Chain of
Health, brought together a Reference Foundational to the success of the Survival 9 (Figure 1).
Group including emergency services, original strategy, was the adoption of
third sector organisations, community the ‘Scottish Approach’ to cross-
groups and academics. This group sectoral working: “a focus on
4
Introduction
Prioritising early links in the Chain University of Edinburgh. A full list of the and to address inequalities that we
of Survival partners can be found in the Strategy know exist in outcomes from OHCA.
Partnership section.
The 2015 – 2020 strategy placed We know from our data linkage reports
particular emphasis on activities at the The key strategic aims of SALFS are and from other sources of information,
start of the Chain of Survival, such as promoting CPR readiness in young such as the Scottish Health Survey 11,
bystander CPR. We sought to people and across a range of and original research from the
consolidate and amplify work already communities and shaping perceptions University of Edinburgh 12,13 that there
being carried out by community groups of OHCA among people living in are certain groups we need to make
and third sector organisations across Scotland. The emphasis we place on sure we reach through the
the country to increase rates of the importance of this work is visible as implementation of this refreshed
bystander CPR in Scotland. an additional ‘readiness’ link at the strategy.
start of what the 2015 OHCA Strategy
To achieve this, key stakeholders described as the ‘augmented Chain of Scope of Scotland’s Out-of-Hospital
came together to form the Save a Life Survival’ 10. Cardiac Arrest Strategy 2021-2026
for Scotland (SALFS) partnership.
In addition to the public facing work of This strategy addresses the needs of
Save a Life for Scotland SALFS, Delivery Group partners those who experience, or may witness,
worked together on a range of a cardiac arrest outside of a hospital
Save a Life for Scotland (SALFS) is a interconnected projects to improve setting.
campaign which brings together the OHCA survival nationally and
work of a range of partners committed regionally. We aim to support partners and other
to saving lives by changing the way we organisations to build on what already
think about OHCA in order to get We intend to carry forward the same works well, to identify and address
Scotland CPR ready. model of partnership working into the gaps in provision, and to introduce
next phase of our plan. innovative ideas to meet the aims of
It is a collaboration between the this strategy.
emergency services, third sector Next steps for SALFS
organisations, Scottish Government This strategy document does not
and academic researchers. The SALFS wishes to build on the address cardiac arrests in children, or
partnership is directed by the successes of the 2015 – 2020 strategy those caused by external physical
Resuscitation Research Group at the injury (so called ‘traumatic’ cardiac
5
Introduction
arrests). Both of these types of cardiac The following chapters address the 6 A chain is a good metaphor for the
arrest are far less common than those elements of the augmented Chain of series of events required to improve a
caused by medical conditions in adults, Survival. The elements, which work person’s chances of survival from
and require a different approach to together to give people the best OHCA. It is a reminder that individual
their management. possible chance of survival after an elements have a reduced value if the
OHCA are as follows: links preceding and following are not
The issue of preventing heart disease, also strong. In particular, those actions
which can lead to cardiac arrest, is ● Getting Scotland OHCA Ready at the beginning of the Chain are
covered by other Scottish Government ● Bystander Action especially important 15. These are
plans, more detail of which can be o Call 999 described below under the umbrella
found in Annex A. o CPR category of Bystander Action.
o Defibrillation
Cardiac arrest can affect anyone, of ● Hospital care Figure 2: The ‘augmented Chain of
any age at any time or place. People of ● Aftercare Survival’ adapted from the 2015 OHCA
all cultural and religious backgrounds Strategy includes community readiness to
and all walks of life. This means that We have also included a Data and respond to an OHCA and the aftercare of
all involved, which are crucial to improving
those affected by OHCA have a wide Innovation chapter which outlines the
outcomes after OHCA across all of the
range of experiences. We are data-led approach we will take to communities in Scotland.
committed to listening to and learning improve the Chain of Survival.
from these experiences.
The Chain of Survival
We continue to structure the aims and
actions of this strategy on the Chain of
Survival, supported by examples of
international best practice, for
example those summarised in the
Global Resuscitation Alliance Call to
Action 14.
6
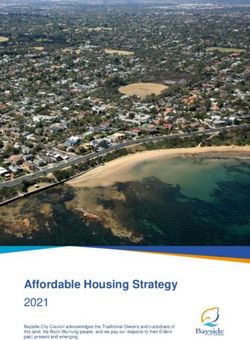
Partners to the Strategy
We would like thank the following partners for supporting the development of Scotland’s Out-of-
Hospital Cardiac Arrest Strategy 2021-2026, and for their commitment to delivery of the strategy:
The role of the Save a Life for Scotland ● Scottish Fire and Rescue Service
Scotland’s Out-of-Hospital Cardiac partnership is to engage as the ● Scottish Government
Arrest Strategy 2021-2026 was public face of the strategy. It is led by ● St John Scotland
conceived by a collaboration of Lisa MacInnes, Resuscitation
organisations committed to improving Research Group at the University of Reference Group
outcomes for those affected by OHCA. Edinburgh.
These partners form the Save a Life The strategy and its delivery is
for Scotland campaign. Delivery Group overseen by the out-of-hospital cardiac
arrest Reference Group, which is
● British Heart Foundation The strategy Delivery Group is chaired by Prof Jason Leitch, the
● British Red Cross responsible for implementing the National Clinical Director of the
● Chest Heart and Stroke Scotland strategy and monitoring the outcomes. Scottish Government. It includes
● Defence Medical Services This group is chaired by Dr Gareth representatives from the Delivery
(Scotland) Clegg, University of Edinburgh and Group partners.
● East Neuk First Responders Scottish Ambulance Service. Delivery
● Lucky2BHere Group Partners include:
● Police Scotland
● Resuscitation Council UK ● British Heart Foundation
● Resuscitation Research Group, ● British Red Cross
University of Edinburgh ● Chest Heart and Stroke Scotland
● Royal Life Saving Society UK ● Convention of Scottish Local
● Scottish Ambulance Service Authorities (COSLA)
● Scottish Fire and Rescue Service ● Defence Medical Services
● Scottish Government (Scotland)
● St Andrew’s First Aid ● Police Scotland
● St John Scotland ● Resuscitation Research Group,
University of Edinburgh
● Scottish Ambulance Service
7
Partners to the Strategy
Writing Group ● Sarah Smith, Chest Heart and
Stroke Scotland We would also like to thank Claire
The writing group which led on the ● Angus Loudon, St John Scotland Fleck Photography for supplying the
development of the strategy on behalf ● Liz Crawford, St John Scotland photograph for the front cover.
of SALFS partnership are as follows:
External expert feedback
● Gareth Clegg, University of
Edinburgh, NHS Lothian and We would like to thank the following
Scottish Ambulance Service subject matter experts for their
● Lisa MacInnes, University of comments on drafts of the strategy
Edinburgh and NHS Lothian document:
● Liz Hasseld, University of
Edinburgh ● Deafblind Scotland
● Diane Lac, University of Edinburgh ● Marcus Ong, Duke-NUS
● Jean Skelton, University of Medical School and Health
Edinburgh Services Research Institute
● Becki MacPherson, Scottish Singapore
Government ● Katie Dainty, University of
● John Wilson, Scottish Government Toronto
● Allan Cowie, Chest Heart and ● Gillian Moreton, Lifelines
Stroke Scotland Scotland
● Jim Ward, Scottish Ambulance ● Sudden Cardiac Arrest UK
Service
● Steven Short, Scottish Ambulance
Service In addition, strategy partners would like
● Naz Lone, Scottish Intensive Care to offer their sincere thanks to the
Society Audit Group individuals and organisations who
● Mark Dunn, NHS Lothian attended consultation events and
● Dave Bywater, Scottish offered their feedback. We also extend
Ambulance Service our thanks to the ALLIANCE, who
● Richie Hall, Scottish Fire and facilitated a lived experience
Rescue Service engagement event.
8Figure 3: A diagram to explain the differences between the Strategy groups – the Reference group, the
Delivery group and the Save a Life for Scotland group.
9Covid-19
Consideration of the short and long-term impact of the Covid-19 pandemic.
cloth.
It is impossible to publish However, we have not done so as we
this strategy without considering Health inequalities, already significant view the implementation of this
the impact of Covid-19. in Scotland, have increased during the strategy as important in the recovery
pandemic as Covid-19 has had a from the Covid-19 pandemic and it is
We know that people who witness an disproportionate impact on people important to us that we do not
OHCA may have concerns around living in areas of socioeconomic minimise our aims. This is reflected in
Covid-19 transmission. The ask of deprivation, and on people from Black, the ambitious aims and actions of this
bystanders to perform CPR or Asian or minority ethnic backgrounds. strategy.
defibrillation is a big one, especially in This reinforces the importance of our
the midst of a pandemic, and it is not efforts to address inequality in
one that we make lightly. outcomes from OHCA.
Since the launch of the inaugural Out- Throughout the pandemic the Scottish
of-Hospital Cardiac Arrest Strategy in Ambulance Service has continued
2015, the position of Save a Life for robust data collection at the scene of
Scotland has been that hands-only OHCA. This will enable analysis of the
CPR is the most appropriate course of impact of the pandemic on OHCA and
action during a cardiac arrest in adults. help us to robustly assess future
This continues to be our planning implications.
recommendation during the Covid-19
pandemic. During the development of this
refreshed strategy, we considered the
SALFS have updated our CPR potential impact of Covid-19 on the
guidance to reflect Covid-19 aims of the strategy. In particular, we
appropriate actions. This now includes considered whether it would be
covering the mouth and nose for the appropriate to reduce the targets in
person in cardiac distress with a loose anticipation of the challenges of
recovering from the pandemic.
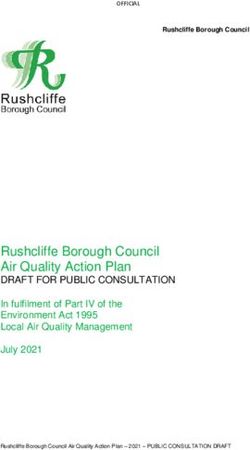
10Figure 4: A diagram to explain the difference between a cardiac arrest and a heart attack.
11Summary of the strategy aims
The top 10 aims of this strategy are that by 2026:
● The SALFS partnership will have equipped 1 million people in Scotland with CPR skills.
● All school aged children in Scotland will have the opportunity to be equipped with CPR skills.
● We will target our work to address key inequalities in OHCA outcomes.
● Bystander CPR rates will be increased to 85%.
● Public Access Defibrillators will be placed optimally and be as accessible as possible.
● 20% of all OHCAs will have a defibrillator applied before the arrival of ambulance service.
● Survival from OHCA will increase to 15%.
● All individuals who are affected by OHCA will be offered support afterwards.
● We will address the challenge of timely communication of anticipatory care plans and decision support for front line
ambulance service crews.
● We will use data to understand and address variation and seek innovative ways to improve outcomes after OHCA.
12Getting Scotland OHCA Ready
We will ensure people in Scotland can identify the signs of a cardiac arrest.
prompt call for help followed by People from more deprived areas in
bystander CPR are key to survival. Yet Scotland are almost twice as likely 21 to
Aims: in a poll of adults living in Scotland have an OHCA and are 60% less likely
more than 20% of respondents felt to survive to leave hospital than those
1. The idea that OHCA can be a they would not know when to use CPR from less deprived areas 22. Around
survivable event is embedded in the and half would not be confident to 11% of the population of Scotland live
public perception. administer it 17. This uncertainty and in a rural area 23 and are 32% less
reluctance to act is exacerbated in likely to survive to leave hospital after
2. There is an increased awareness communities and age groups most OHCA than those living in urban
of signs and symptoms of cardiac affected by OHCA 18. areas 24.
arrest enabling prompt bystander
action. To address this, we will work to ensure We also know that ethnicity can be a
that people understand that OHCA can factor in how likely a person is to
3. Common misperceptions about be a survivable event and are aware of experience an OHCA. For example,
CPR and defibrillation are the symptoms of an OHCA. This will people from South Asian backgrounds
addressed. enable them to act quickly and have up to 50% higher risk of
potentially save a life. developing coronary heart disease
A cardiac arrest occurs when the heart than white Europeans 25. Coronary
stops pumping blood around the body. Inequalities heart disease can lead to a heart
Someone who is having a cardiac attack or cardiac arrest.
We are already aware of inequalities in
arrest will suddenly lose
health 19, particularly affecting In addition, we know from international
consciousness and will either stop
outcomes after OHCA. Over the last studies that women are less likely to
breathing or stop breathing normally.
five years, we have started to have CPR performed on them 26, a
understand more clearly the pattern we also see in Scottish data 27.
It is estimated that every minute of
association between measures of The misconception that breasts make
delay in bystander action reduces the
socioeconomic position and decreased CPR more challenging, fear of doing
likelihood of survival after OHCA by
survival after OHCA 20. harm, fear of inappropriate touching
10% 16. Therefore, early recognition of
cardiac arrest by those nearby and and fear of being accused of sexual
13Getting Scotland OHCA Ready
assault have been given by the public Language concerns may also affect
as reasons for this gender discrepancy the ability of the partners to meet with
28
. It is important that over the next 5 Actions:
certain groups - for example, British
years, the partnership works to combat Sign Language (BSL) users, non-
these fears and embed the knowledge 1. We will continue our public
native English speakers or Gaelic awareness campaign, with a focus
that CPR is a gender neutral life-saving
speakers across Scotland. Partners on increasing awareness of:
technique.
will consider how to address this
barrier. • the signs and symptoms of
We will also work to ensure that we do cardiac arrest.
not exclude disabled people and/or • the importance of prompt
By acknowledging these inequalities
those living with a long-term health and working with communities we can bystander action (calling 999,
condition from the work that we do. ensure that everyone has the best CPR and defibrillation).
Whilst we know that the physical chance of survival. • that CPR is a gender neutral
aspects of CPR may present a intervention.
challenge for those with limited GoodSAM • that aftercare resources are
mobility, everyone can play a role in available for those who intervene
the chain of survival either by calling The GoodSAM smartphone app is a in an OHCA.
999 or by guiding other bystanders to mechanism that can be used to
perform CPR and retrieve a PAD. increase readiness to respond to 2. We will focus our public
OHCA, and allow the ambulance awareness campaign on reaching
service to alert responders in the those who we know experience
As part of this targeted work, the community to a nearby OHCA 29. In inequalities in bystander CPR rates
Scottish Ambulance Service have 2020 the Scottish Ambulance Service and survival from OHCA.
piloted a “CPR skills for disabled began using GoodSAM to alert trained
people” course. It is hoped that, if responders and off duty ambulance 3. We will raise awareness of the
successful, this course can be made service staff. We will develop our use potential of the GoodSAM app to be
available across Scotland in addition to of GoodSAM to enable communities to used to alert responders in the
the development of digital training respond more effectively to OHCA. community.
materials.
14Judy Newton’s husband Gregor walked up the stairs in their
home around 9pm after lighting the log burner. A few
moments later their 11 year old son Harry yelled for help from
upstairs. Gregor had collapsed and his face was blue. Judy
rushed up the stairs to help and Harry’s older sister Eilidh
called for an ambulance. Gregor was fit and well when he
experienced his OHCA.
Judy began CPR, “I knew that I needed to try something and
doing the first compressions, hearing his ribs breaking, I
didn’t realize I had that much strength in my body. I couldn't
remember the ratio, that we get taught, so I made it up as I
went along I just did compressions and was praying to
everybody”
The Newton Family Sandy, a first responder arrived quickly after the 999 call and
brought the defibrillator to deliver a shock to Gregor, about 45
seconds later Gregor gave a cough and regained
“We never thought anything like this consciousness.
would ever happen to us, which is
“And then I kind of knew he was ok when he started to swear
silly, of course it can happen to profusely” said Judy.
anybody.”
From Harry recognising something was wrong and calling for
help, Eilidh calling 999, Judy delivering CPR, Sandy arriving
with a defibrillator, and the ambulance arriving to take Gregor
to hospital, everybody played their part and did it 100%.
“It shows the Chain of Survival is not just some theory, it really
does work if everything takes place.’’Bystander Action (Call 999, CPR and Defibrillation)
We will encourage an increased willingness to deliver CPR and defibrillation among people who
witness an out-of-hospital cardiac arrest.
The first action taken by any bystander they can do is call for help and do CPR
Aims: must be to call 999 and request an as instructed by the Ambulance
ambulance for an OHCA. Service call handler.
1. To equip a total of 1 million
people in Scotland with CPR skills Cardiopulmonary resuscitation (CPR) In some circumstances defibrillation
is a series of actions which artificially within 3 minutes of a cardiac arrest can
2. All school aged children will have circulates blood around the body, increase the chance of survival to
the opportunity to be equipped with buying time before the emergency above 70% 33.
CPR skills. services arrive or until defibrillation can
be attempted 30. If there is a publicly accessible
3. Bystander CPR rates will be defibrillator nearby, and it is possible to
increased to 85%. Public Access Defibrillators (PADs) fetch it without interrupting CPR, the
deliver an electric shock to the heart of Ambulance Service will instruct a
4. Public Access Defibrillators will someone in cardiac arrest, allowing the bystander to collect it. In Scotland,
be as accessible as possible. normal, organised, electrical rhythm of defibrillators are not often used before
the heart to restart 31. the arrival of the Ambulance Service 34.
5. 20% of all cardiac arrests will
have a defibrillator applied before Although these are two distinct actions, Working with communities to
the ambulance service arrive. CPR and defibrillation work hand in familiarise people with both CPR skills
hand to give people the best chance of and the use of PADs, and ensuring
6. Survival from OHCA will increase survival after cardiac arrest. that people who witness an OHCA feel
to 15%. confident in using both of these, is the
Evidence shows that the use of CPR in foundation of ensuring that those who
Prompt bystander action – calling 999, the immediate aftermath of an out-of- experience an OHCA have the best
delivering CPR and defibrillation - are hospital cardiac arrest can increase the chance of survival.
vital to improving a person’s chance of likelihood of survival by 2-3 times 32.
survival from OHCA. Where only one bystander is present at
the scene, the most important thing
1Bystander Action (Call 999, CPR and Defibrillation)
Cardiopulmonary resuscitation address common misconceptions
(CPR) about CPR. Fear of inadvertently doing We will work with youth organisations
harm or making the situation worse to support young people to become
and fear of being sued are some of the CPR ambassadors in their
The most obvious barrier to performing reasons cited for inaction 37. communities and schools.
CPR is the knowledge of how to do it.
Even though Ambulance Service call Much good practice already exists. Equipping young people with these
handlers will instruct bystanders at an Public services and third sector lifesaving skills not only creates the
OHCA in how to do chest organisations have played a vital role basis of a strong long-lasting bystander
compressions, it is those who have in engaging with communities and culture but enables even primary
previously been equipped with CPR equipping 640,000 people across school aged children to support their
skills who are most willing to deliver Scotland with CPR skills through the friends and family to learn these skills
this intervention 35. implementation of the 2015 OHCA too 38,39,40.
Strategy.
We want bystanders who witness an Community-led engagement
OHCA to feel able to take action, and Now we can build on that success. We
to achieve this we aim to familiarise a will use this opportunity to increase the As 80% of cardiac arrests occur at
total of 1 million people in Scotland reach of our work to embed CPR skills home 41, it is vital that we continue to
with CPR skills. in communities across Scotland, and consider ways to increase engagement
ensure that the change is sustained at community-level. Our partners are
We will make a concerted effort to over time. committed to working closely with
target our approach to equipping communities and we will work together
people with CPR skills. This is to to continue this approach.
Schools
ensure that we reach communities who It is important that we continue to
typically face barriers to accessing ensure that our initiatives are as
opportunities to learn CPR skills, or The SALFS partnership is committed accessible as possible. To do this, we
who experience inequities in outcomes to supporting schools and youth will increase engagement with existing
from OHCA 36. organisations to equip young people community organisations (e.g. sports
with CPR skills. We will work with local hubs, local businesses and other
authorities, education colleagues and community groups) to raise awareness
Alongside equipping people with these
partners, to make sure that all school of and offer opportunities to learn
lifesaving skills, we must also make
age children have the opportunity to CPR.
sure that we continue to work to
learn CPR skills.
2Bystander Action (Call 999, CPR and Defibrillation)
the Chain of Survival. By utilising End of Life decision making and
We are not the only partners in trained volunteer emergency anticipatory care planning
Scotland who are working towards responders we can increase the
increasing survival rates after OHCA. resources available to help at an
We will seek out and work in OHCA, relieve the pressure on CPR is a treatment that could be
collaboration with local community bystanders and increase the chances attempted on any individual whose
groups across Scotland who focus on of survival for those in need. heart function stops. Such events are
CPR and defibrillation (both provision inevitable as part of dying and thus,
of equipment and training) to gather People from a number of agencies can theoretically, CPR could be given to
our collective experiences and support be or already are trained to respond to every person when they die.
and amplify each other's work. OHCA. This means there is more
opportunity for a quick initial response, It is therefore essential that emergency
First Responders particularly in some rural and remote responders can more easily identify
areas. The ability to do this is already people for whom cardiac arrest
The strategy partners know that while enshrined in community planning represents the terminal event in their
recognising the signs of a cardiac policy 42, giving partners the scope to illness and for whom CPR would be
arrest may seem straightforward, support local first response solutions. inappropriate because it will not be of
bystanders are not always confident in benefit or they have recorded that they
their ability to do so. It is vital then, that In recent years, smartphone do not want to receive CPR. This helps
Scottish Ambulance Service call applications such as GoodSAM have them to ensure that action taken
handlers are able to quickly recognise facilitated rapid community responder reflects the wishes of that person.
bystander’s description of an OHCA action in response to OHCA, alerting
and encourage the caller to begin nearby off duty doctors, nurses and Guidance is already in place to support
CPR. paramedics to an emergency. Scottish recording of such decisions but the
Ambulance Service has adopted visibility of this can often be difficult in
Supporting bystander action will give GoodSAM for use and the SALFS the emergency situation. We will work
those in need a fighting chance until partnership will work to support its with NHS and emergency response
the appropriate emergency resources effective usage. partners to ensure the systems are in
arrive on scene. place to make information recorded
about such decisions more accessible
Prompt arrival of community to all responders, and so help to
responders is also vital to improving
3Bystander Action (Call 999, CPR and Defibrillation)
reduce unwanted or inappropriate to a nearby PAD, or the lack of a PAD To support effective use of PADs, we
resuscitation attempts. placed within an accessible distance to published Out-of-Hospital Cardiac
the location of the OHCA. Arrest: guide to public access
Defibrillators defibrillators in 2018. This provides
At the time of writing, PADs are only practical advice to those considering a
Public Access Defibrillators (PADs) are used by the public in around 8% of PAD for their local community.
designed for use by members of the arrests in Scotland 46.
public without training. They come with We will update the guide during the
written instructions and can give There are many PADs installed in a lifetime of this strategy to provide the
audible guidance to users. variety of locations across Scotland, most up to date advice and encourage
though not all are registered with the communication between potential PAD
PADs are automatic defibrillators, Scottish Ambulance Service. We will guardians and SALFS partners.
which means that they will only deliver continue to encourage the accessible
a shock where it is required. Despite mounting, clear signposting and PAD location work
this, the public are often still reluctant
registration of PADs.
to use them 43,44,45.
Mathematical modelling can be used to
To address this, we will work to embed The Scottish Ambulance Service uses help ensure that PADs are placed in
the use of PADs within our public ‘The Circuit’, a UK-wide registry of locations that maximise their
awareness campaign outlined in the defibrillators developed by the British usefulness. Using our knowledge of
Getting Scotland OHCA Ready Heart Foundation which allows 999 call where OHCAs are most likely to
chapter. We will draw on examples of handlers to quickly direct bystanders happen we are able to build a tool to
best practice from the partnership and to a registered PAD when it is nearby. show where PADs are most likely to be
other local community groups to We recommend that all PADs are required.
develop our messaging in this regard. registered to increase the opportunities
Another barrier to prompt bystander
for the ambulance service to be aware We are working to make this type of
defibrillation is a lack of accessibility of
of their location and support tool readily available to communities
PADs. This can be a result of a
bystanders to access and use them in and organisations who wish to deploy
combination of factors including; lack
instances of OHCA. PADs for greatest benefit.
of registration limiting the ability for
SAS call handlers to direct a bystander
4Bystander Action (Call 999, CPR and Defibrillation)
Actions: place to make information
recorded about end of life
decisions is available and
1. We will work with Local accessible to responders in
Authorities to give school aged instances of OHCA.
children to opportunity to be
equipped with CPR skills. 5. We will familiarise adults and
children across Scotland with
2. We will work with the Scottish PAD usage.
Ambulance Service to optimise
the interaction with call handlers 6. We will analyse and publish data
as they assist bystanders in to provide members of the public
performing CPR and using PAD. with information as to the most
effective location to place their
3. We will support the development defibrillator.
and deployment of first
responder networks. This will 7. We will develop and implement
include evidence based national PAD
- ensuring first responders guidelines, focusing on optimal
are trained in the delivery placement and public
of high performance CPR. engagement.
- working with communities,
statutory organisations 8. We will continue to encourage
and third sector the accessible mounting, clear
organisations to support a signposting and registration of
coordinated first response PADs with the Scottish
to OHCA. Ambulance Service.
4. We will work with NHS and
emergency response partners to
make sure that systems are in
5On February 15th 2015 Brian Clarke was leaving the gym in
Anstruther when he had a cardiac arrest. He was found in his
car by a passerby who alerted the staff inside the gym. Stuart
Barton, who had spoken to Brian only moments ago was
shocked as he ran outside to see him collapsed. With another
member of the public, he checked for breathing, called 999
and sent for a defibrillator. He also began CPR.
“So there’s me, never used a defibrillator before, panicking,
but it was so simple and you have that horrible thing going in
your mind, am I doing this right? But it was honestly so simple
and speaks so clearly, “analysing patient, shock advised,
shock given”, and then away you go with your CPR again.
And right as we had a pulse, a knight in shining armour, the
first responder showed up.”
Brian Clarke
Gillian Duncan from East Neuk First Responders was now on
the scene and took over from Stuart. Shortly after that, a
“Brian keeps wanting to say Scottish Ambulance paramedic arrived and took Brian to
thank you all the time, but seeing hospital. Brian was on a life support machine for 50 hours and
his family really didn't know what was going to happen, but
him here speaking to us today then, he woke up. He was still Brian. He survived his OHCA
is the best thank you” because of the early actions of these individuals including
early defibrillation.Hospital Care
We will ensure specialist in-hospital care to support recovery
Aims: ICU care is a crucial step in recovery Making better use of the high quality
from OHCA for people who experience information stored in Scotland’s unique
1. We will support continuous a cardiac arrest and their families. healthcare databases could enhance
improvement of specialist in- Scotland has a cohesive, joined-up our audit systems. We will consider
hospital care to improve survival network of highly trained and motivated what is important to measure in order
from OHCA. ICU healthcare professionals, to drive effective improvements in care.
supported by access to high
People who experience a cardiac quality data and information systems. Actions:
arrest and have responded to initial We will build upon these unique
treatment often need advanced strengths to support continuous 1. We will develop a national ICU
hospital care for a period of time after improvement of specialist in-hospital OHCA guideline to include:
the heart has been restarted. care to support the recovery of people
who experience a cardiac arrest. ● Advice on which patients are likely
If they are unconscious or vital organs Sharing innovation and excellence to benefit from treatment in an
need support, frontline doctors, nurses through the network of ICU healthcare Intensive Care Unit.
and other health care professionals professionals will help us to achieve ● How best to coordinate with clinical
working in Intensive Care Units (ICUs) this. staff across relevant hospital
and Coronary Care Units (CCUs) specialties.
provide specialist life support therapies Recent research has driven forward ● What is the best way to deliver
to provide the best chance of recovery. treatments for people admitted to ICUs specialist treatment - such as
after experiencing a cardiac arrest. In temperature management
Despite receiving life support partnership with the Scottish Intensive (initiation, maintenance, rewarming
therapies, high numbers of people Care Society and Scottish Intensive and normothermia, shivering
continue to die each year in ICU after Care Society Audit Group, we will management, physiologic targets
suffering a cardiac arrest but survival develop guidelines, which reflect the during temperature management).
rates with good neurological recovery most up to date evidence on ICU care ● Best practice to determine whether
of up to 60% are possible 47 48. for people after cardiac arrest. ICU treatment is benefittingHospital Care
someone after OHCA (Multi-modal
prognostication).
● Improving pathways for
rehabilitation after discharge from
ICU.
● Advice about organ donation.
2. We will explore the feasibility of
embedding components of
OHCA care in ICU in the
Scottish Intensive Care Society
Minimum Standards and Quality
Indicators.
3. We will share innovation and
best practice about OHCA across
Scotland’s ICUs to promote rapid
translation of new evidence into
practice. We will take a holistic
approach to this work,
encompassing ICU care,
bereavement care and post ICU
rehabilitation and support.
8On Saturday 9th June 2018, Cherill Parry was walking her
dog in Gairloch when she started to feel unwell. After visiting
her doctor, she arrived home only to collapse on the
pavement outside.
“I got out of the car and I don’t remember anything for about
three weeks after that! I was told that I dropped like a stone on
the pavement outside my house, and my neighbour ran
across to the community centre to get the defibrillator and
used it on me. After that, the doctor and the air ambulance
arrived. Apparently I ‘died’ a couple of times, according to
reports.”
After three weeks in Raigmore Hospital in Inverness, Cherill
was transferred to Edinburgh where she underwent heart
surgery to fit a pacemaker. After leaving the hospital she
returned to Raigmore for a further two weeks, but is now
Cherill Parry recovered.
Sadly, Cherill was informed in hospital that her husband
Russell had died at home in Gairloch exactly two weeks after
“I wouldn’t be here if it wasn’t her cardiac arrest. At her husband’s funeral, a collection was
for the defibrillator at the taken for another defibrillator. Little did she know then that this
defibrillator would go on to save the life of another person in
community centre and someone 2020. Despite enduring such serious illness and personal
being able to use it on me. If I could tragedy, Cherill remains positive about the future and was
quick to pay tribute to the role of CPR and defibrillator
tell you one thing it would be that you community groups like Lucky2Bhere. I wouldn’t be here if it
can’t hurt someone, you can only do wasn’t for the defibrillator at the community centre and
someone being able to use it on me”
good.”Aftercare
We will ensure support for people in Scotland after their experience with out-of-hospital cardiac
arrest.
Survivors and their families support for people who experience
Aims: For many survivors, the cause of their
cardiac arrest.
cardiac arrest will have been a We must also recognise that OHCA
1. All individuals who experience an
blockage in one of the blood vessels can have a significant impact on
OHCA are well supported
supplying the heart muscle. This people’s emotional and psychological
afterwards.
causes a heart attack which can wellbeing, and explore how best to
sometimes lead to cardiac arrest. support people in coping with these
2. There is support available for
bystanders who witness an OHCA. impacts.
People who have this underlying cause
for their cardiac arrest will be eligible to Many OHCA survivors can benefit from
3. The wellbeing of emergency access cardiac rehabilitation. Cardiac accessing information and support.
service and volunteer community rehabilitation services provide vital This can take the form of peer support
responders is supported. support to help people get back to such as online forums from Sudden
everyday life as much as possible after Cardiac Arrest UK
It is important to ensure that care and developing heart disease. (https://www.suddencardiacarrestuk.or
support is available for all people who g/get-support), or in some cases,
have been affected by OHCA. This However, for people who experience specialist help, such as the “Life After
includes survivors, their families, cardiac arrest with a different cause – Cardiac Arrest”
bystanders and other responders. for example Spontaneous Coronary (www.lifeaftercardiacarrest.org)
Artery Dissection (SCAD), or an resource for survivors and families
In order to support the aftercare needs inherited heart condition, may not be experiencing loss after OHCA.
of people who have been affected by eligible for referral into these services.
OHCA, it is vital that we listen to the Many of the SALFS partner
lived experience to shape our actions Wider work on improving timely and organisations have information
and develop our support resources. equitable access to rehabilitation for available about cardiac arrest. This
people with heart disease is covered includes support groups for survivors
within the Scottish Government’s Heart and specialist psychological services in
Disease Action Plan. We will work some cases.
collaboratively to improve this kind ofWe will continue to signpost to these Responding to this need for support, Responders affected by psychological
as part of our public awareness SALFS partners have created online trauma. We will work closely with
campaign. We will also seek to identify educational resources aimed at community responder groups, the
and amplify examples of best practice emergency services clinicians and First Scottish Ambulance Service, Police
in order to increase the availability of Responders to provide a space of Scotland, and Scottish Fire and
help to those who need it. further learning to understand OHCA Rescue Service to raise awareness of
post-event. We will signpost to these this resource and support responders
Bystanders resources as part of our ongoing public to access the support they require.
awareness work.
The increasing bystander CPR rate in Case Study: Bystander Support in
Scotland means that more people are We will continue to explore and learn Canada
intervening in an OHCA than ever from national and international
before. initiatives to increase the availability of In Canada, an online Bystander
support to OHCA bystanders. Support Network has been created to
Several studies have explored the
effect of witnessing a cardiac arrest on provide resources alongside an online
Innovations such as the Bystander forum for bystanders affected by
the well-being of bystanders, who are Support Network in Canada have been
often family members of the person in Cardiac Arrest 57. Members are able to
created to provide an opportunity for research, ask questions, share stories,
cardiac arrest. Fear, anxiety, anger, bystanders to find further information
confusion, and even signs of post- and network with others from around
and support. the world who have been affected by
traumatic stress have been reported 49
50 51 52 53 54 55
. Support for Community Responders OHCA. It is a resource for members of
and Emergency Services the public seeking support after an
Research looking at the experience of OHCA but also an evolving piece of
bystanders has also shown wide In addition to the needs of members of research to help clinicians and
variation in individual preference for the public who are bystanders to researchers learn more about the
the support they require from clinical OHCA, we also need to consider the bystander experience and what types
staff. Clinicians involved in those cases mental wellbeing of responders of support is needed.
had a huge impact on individuals' (including community First Responders http://www.bystandernetwork.org/
experience after the cardiac arrest and and those working in emergency
are therefore in a key position to make services).
a difference to individuals after
OHCA 56. The Rivers Centre (www.lifelines.scot)
is a specialist service for First
11Actions:
1. We will provide a range of
aftercare support, including
online, telephone and face-to-
face resources.
2. We will improve signposting to
existing aftercare support.
3. We will develop a referral
pathway for First Responders to
access aftercare support.
4. We will include aftercare in our
public awareness campaign to
ensure that people are aware of
the routes through which they
can access support.
5. We will listen to those with lived
experience of OHCA to better
understand their aftercare needs.
12Data and Innovation
We will ensure access to timely, high quality data to facilitate open review, discussion, learning and
action planning.
in the community, returning people to
Aims: The OHCA Data Linkage Project their families where possible after
OHCA, and supporting them through
As part of the 2015 OHCA Strategy we their survivorship 62 63 requires a multi-
1. Our use of data will help us to established the OHCA data linkage
understand and address faceted approach. In this context
project 60. This gave us an effective survival is not always the most
variation and improve outcomes base upon which to begin to measure
after OHCA. important outcome, and is certainly
progress towards our aims. For underpinned by a range of crucially
example, we were able to show an important process measures over
2. Innovative solutions are used to increasing rate of bystander CPR, and
tackle the key challenges relating which we have more direct influence.
identify trends in public access
to OHCA. defibrillator deployment both of which We will continue to identify key metrics
were key components of the first in the augmented chain of survival and
To support all the ambitions of this strategy.
strategy it is important that we have find ways to measure what is important
access to, and effectively utilise, data to delivering our aims.
The key clinical outcome after OHCA is
to understand the system of care long term patient survival. Our data
required to preserve life and provide By taking this approach our data
linkage reporting helped us show that linkage work has already enabled vital
support for those affected by OHCA 58 across the lifetime of the strategy the
59
. insights about where we should focus
number of people who survived to our attention as we move forward with
leave hospital after an OHCA this refreshed strategy. We now have
Access to this information enables us increased from 1 in 20 to 1 in 10 61.
to understand where inequities exist, the opportunity to develop this further
and where improvements can be by modelling changes to the chain of
Next steps in data analysis survival in Scotland to see where
made. Ultimately, this supports our
ability to direct our actions and improvement will have the most
Survival is an important measure, but
resources in the most effective way to impact.
cannot be considered in isolation.
improve outcomes from OHCA across Preparing communities and
Scotland. responders to intervene appropriately
13We will work collaboratively with the creates particular challenges for
Scottish Cardiac Audit to link SAS data successful prevention and It reinforces the importance of enabling
about OHCA with detailed data held resuscitation. We will endeavour to meaningful conversations between
about cardiac care, to understand the combine OHCA data with insight from people, their families and those who
cardiology care that people who other sources in order to develop more support their care and wellbeing, about
experience an out of hospital cardiac effective systems of care. what they would wish to happen if they
arrest receive and how this impacts on become unwell and face the scenario
their outcomes. Scotland’s communities are where resuscitative interventions may
characterised by variation, including be applied.
Similarly we wish to work with geography, deprivation and age Not only are these conversations to be
Intensive Care colleagues to take demographic. Often these encouraged but their output needs to
advantage of the high quality audit characteristics will have an impact on be captured, and crucially to be
information stored in Scotland’s unique OHCA outcomes, some of which are available to emergency services in the
healthcare databases to facilitate better understood than others, and can minutes between a 999 call being
innovation and excellence in care point us towards bespoke local received and a resuscitation
across Scotland’s ICUs that will considerations to be addressed in commenced. This would help families
promote best practice. terms of the application of the key links cope with bereavement knowing that
in the chain of survival. the wishes of their loved one were
Analysis of Scottish OHCA outcomes respected, help guide the efforts of
has shown that people living in more In addition where communities are clinicians, and most importantly seek to
deprived areas remain more likely to more similarly configured but outcomes preserve dignity in death. We wish to
experience an OHCA and that people vary, this raises the potential for explore innovative digital and
from deprived areas are still less likely learning between systems in an communications solutions to the
to survive following OHCA. Deprivation attempt to improve outcomes. The key challenges this entails.
also has a significant effect on the is intelligent use of data to understand
likelihood of receiving bystander variation and the factors that underlie Technological innovation
CPR 64. this variation.
Our analysis of the whole patient Finally, addressing OHCA lends itself
A weight of international literature also journey after OHCA has also to the application of established and
makes us aware that the intersection illuminated the crucial importance of emerging technologies. These include
between OHCA and gender, ethnicity, respect for the wishes of individuals in using video for real time support,
mental illness, and other comorbidities respect to end of life care 65. effective audit of care delivery,
14technology to support recognition of through linkage with the Scottish
OHCA including application of Artificial Ambulance Service data.
Intelligence, and the use of geospatial
technology to enable resource location 4. We will develop a plan to use
and utilisation (for example locating innovative digital technologies to
PADs or community responder interact with the public and
resources). facilitate bystander action in
response to OHCA.
It is our intention to work closely and
collaborate widely with industry, clinical 5. We will facilitate collaboration
and academic partners in order to between strategy delivery and
make the augmented Chain of Survival academic partners to answer key
in Scotland an international example of questions about OHCA.
best practice with regards to its use of
technological innovation. 6. We will work with colleagues in
Actions: primary care to
implement solutions to the
challenges of timely
1. We will develop a monitoring and
communication of anticipatory
evaluation framework for this
care plans and decision support
strategy which will be focussed
for front line ambulance service
on key process measures of care
crews in dealing with complex
for patients after OHCA.
end of life care decisions.
2. We will link data about OHCA
with data about gender, ethnicity,
mental illness, and other
comorbidities to identify and
address unwarranted variation.
3. We will harness the potential of
data held in Scotland’s national
ICU audit and cardiac audit
15Conclusion
This refreshed strategy marks a refocusing of the aims outlined within the inaugural OHCA Strategy 2015 – 2020. It is an effort to
build on our successes, and to further target our work as we continue to address OHCA in Scotland.
We have made excellent progress throughout the lifetime of the 2015 strategy. Despite this, current survival rates from OHCA in
Scotland are still lower than we want them to be.
At this stage, we must tackle some significant challenges in order to further improve. We must continue with our important work to
get Scotland CPR ready, through raising awareness of OHCA and the importance of bystander action - but as part of this we must
also address some of the misconceptions around CPR. We will also continue, through the excellent work of our partners, to support
communities to prepare themselves to respond effectively to OHCA. We know that there are parts of the country, and groups of
people that we need to make a particular effort to reach because they experience inequalities in outcomes from OHCA. This
targeted approach to tackling inequalities is a continued area of focus for us in this refreshed strategy.
We have also sought within this strategy to support bystander action, improve accessibility of Public Access Defibrillators and
ensure that we do all that we can to encourage seamless and prompt intervention for people who have an OHCA. We have
identified key actions to support continuous improvements within hospital care to support recovery of people after cardiac arrest,
and vitally, we have identified key actions which recognise the importance of providing aftercare support to everyone affected by
OHCA.
Partnership remains at the core of this refreshed strategy. Working together to discover bright spots of best practice and applying it
across our country. Improving by sharing our data and our stories. Creating better systems by understanding each other’s
challenges. Flourishing by celebrating each other’s successes.
We want to learn from the experiences of the last five years in order to do better, equip more communities, help more individuals
and save more lives. Scotland’s Out-of-Hospital Cardiac Arrest Strategy 2021-2026 sets out how we will do that.
16You can also read