Scaling Up Voluntary Medical Male Circumcision for Human Immunodeficiency Virus Prevention for Adolescents and Young Adult Men: A Modeling ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Clinical Infectious Diseases
SUPPLEMENT ARTICLE
Scaling Up Voluntary Medical Male Circumcision
for Human Immunodeficiency Virus Prevention for
Adolescents and Young Adult Men: A Modeling Analysis
of Implementation and Impact in Selected Countries
Emmanuel Njeuhmeli,1 Marjorie Opuni,2 Melissa Schnure,3 Michel Tchuenche,4 Peter Stegman,4 Elizabeth Gold,5 Valerian Kiggundu,1 Nida Parks,1
Kim Seifert Ahanda,1 Maria Carrasco,1,6 and Katharine Kripke4
1
Office of HIV/AIDS, Global Health Bureau, United States Agency for International Development, Washington, District of Columbia; 2Independent Consultant, Geneva, Switzerland; 3Palladium Group
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
and 4Avenir Health, Washington, District of Columbia; and 5Johns Hopkins Center for Communication Programs, and 6Department of Health, Behavior and Society, Johns Hopkins Bloomberg School
of Public Health, Baltimore, Maryland
Background. The new World Health Organization and Joint United Nations Programme on HIV/AIDS strategic framework for
voluntary medical male circumcision (VMMC) aims to increase VMMC coverage among males aged 10–29 years in priority settings
to 90% by 2021. We use mathematical modeling to assess the likelihood that selected countries will achieve this objective, given their
historical VMMC progress and current implementation options.
Methods. We use the Decision Makers’ Program Planning Toolkit, version 2, to examine 4 ambitious but feasible scenarios for
scaling up VMMC coverage from 2017 through 2021, inclusive in Lesotho, Malawi, Mozambique, Namibia, South Africa, Swaziland,
Tanzania, Uganda, and Zimbabwe.
Results. Tanzania is the only country that would reach the goal of 90% VMMC coverage in 10- to 29-year-olds by the end of
2021 in the scenarios assessed, and this was true in 3 of the scenarios studied. Mozambique, South Africa, and Lesotho would come
close to reaching the objective only in the most ambitious scenario examined.
Conclusions. Major changes in VMMC implementation in most countries will be required to increase the proportion of circum-
cised 10- to 29-year-olds to 90% by the end of 2021. Scaling up VMMC coverage in males aged 10–29 years will require significantly
increasing the number of circumcisions provided to 10- to 14-year-olds and 15- to 29-year-olds.
Keywords. HIV; HIV prevention; voluntary medical male circumcision; VMMC.
Voluntary medical male circumcision (VMMC) is a highly effect- 2015 to increase the proportion of circumcised men in this age
ive [1–3] and cost-effective [4–6] intervention to reduce female- group to 80% [6]. By the end of 2015, almost 12 million men and
to-male human immunodeficiency virus (HIV) transmission. It adolescent boys had been circumcised [10].
is recommended in countries with high HIV prevalence and low More recently, in the context of plateauing global resources
levels of male circumcision [7, 8]. Fourteen countries in sub-Sa- for HIV services [11] and international commitment to respond
haran Africa are scaling up service delivery of adult VMMC for more effectively to the epidemic [7, 12–15], additional mode-
HIV prevention [9]. In 2011, the World Health Organization ling was conducted to inform country prioritization of VMMC
(WHO) and the Joint United Nations Programme on HIV/AIDS scale-up [16–24]. Two main insights emerged from these analy-
(UNAIDS) released a strategic framework outlining VMMC ses. First, to focus limited resources, countries are transitioning
implementation objectives in priority countries [9]. The strategy from national scale-up of VMMC service provision to focused
set a target of reaching VMMC coverage of at least 80% among scale-up in a subset of priority subnational locations. Second, in
males aged 15–49 years by 2015. Modeling conducted in 2011 addition to this geographical prioritization, countries are fram-
to inform this strategy indicated that >20 million males aged ing their scale-up targets around reaching high coverage among
15–49 years would need to be circumcised between 2011 and younger men and adolescent boys. Increasing the proportion of
circumcised 15- to 29-year-olds will produce the most immedi-
ate impact on HIV incidence [16–24] compared to circumcising
Correspondence: E. Njeuhmeli, USAID Office of HIV/AIDS, 2100 Crystal Drive, Arlington, VA
22202 (enjeuhmeli@usaid.gov).
other age groups. Increasing VMMC coverage in younger ado-
lescent boys aged 10–14 years contributes to increasing the pro-
Clinical Infectious Diseases® 2018;66(S3):S166–72
Published by Oxford University Press for the Infectious Diseases Society of America 2018. portion of circumcised 15- to 29-year-olds in the near term and
This work is written by (a) US Government employee(s) and is in the public domain in the US. it takes advantage of existing demand for VMMC among 10-
This Open Access article contains public sector information licensed under the Open Government
Licence v2.0 (http://www.nationalarchives.gov.uk/doc/open-government-licence/version/2/).
to 14-year-olds. Whereas the roll-out of VMMC programs has
DOI: 10.1093/cid/cix969 not specifically focused on attracting this age group, more than
S166 • CID 2018:66 (Suppl 3) • Njeuhmeli et al
a third of clients accessing VMMC services to date have been Population by age and year, mortality by age and year, annual
younger adolescents aged 10–14 years, among whom circumci- number of male births, and HIV prevalence by age and year
sion is socially and culturally most acceptable [25, 26]. Indeed were exported from Spectrum/Goals or Spectrum/AIDS
the new WHO/UNAIDS strategic framework for VMMC aims Impact Model (AIM) files for all countries [27]. The HIV inci-
to increase VMMC coverage among males aged 10–29 years in dence was also obtained from Spectrum/Goals or Spectrum/
priority settings to 90% by 2021 [10]. AIM files for all countries except Swaziland. For Swaziland, the
In this article, we use mathematical modeling to examine age-specific HIV incidence was derived from the Swaziland
the impact of 4 hypothetical scenarios for VMMC program Incidence Measurement Survey [28]. The male circumcision
implementation from 2017 through 2021. We explore the prevalence by age group in the model’s base years for each
ways in which annual uptake of circumcision in various age country was derived from Demographic and Health Surveys
groups between 2017 and 2021, inclusive, could affect the or AIDS Indicator Surveys from the most recent years before
proportion of circumcised males aged 10–29 years by the end the start of the VMMC program. Information on the annual
of 2021. Our analyses focus on 9 of the 14 priority countries number of male circumcisions performed since the beginning
scaling up VMMC for HIV prevention: Lesotho, Malawi, of the program was obtained from WHO and the age disag-
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
Mozambique, Namibia, South Africa, Swaziland, Tanzania, gregation of the annual number of VMMCs performed was
Uganda, and Zimbabwe. The purpose of this analysis is to estimated using the US President’s Emergency Plan for AIDS
assess the likelihood that these countries will increase the Relief (PEPFAR) annual reporting [26].
proportion of circumcised 10- to 29-year-olds to 90% by the
end of 2021, given their historical VMMC progress and cur- Scenarios Analyzed
rent implementation options. We explored 4 hypothetical scale-up scenarios representing
ambitious but feasible VMMC program implementation objec-
METHODS tives, given historical trends in scaling up male circumcision in
countries. We defined “aggressive” scale-up as multiplying the
We used the Decision Makers’ Program Planning Toolkit
numbers of circumcisions performed in 2016 by 1.5 and per-
(DMPPT), version 2, to examine 4 scenarios for scaling up
forming that number of circumcisions annually between 2017
VMMC coverage from 2017 through 2021. Our analyses are
and 2021, inclusive. We defined “very aggressive” scale-up as
limited to those countries for which age-disaggregated pro-
doubling the numbers of circumcisions performed in 2016 and
gram data were available for all years of the VMMC program,
performing that number of circumcisions annually from 2017
which excluded 5 of the 14 priority countries scaling up VMMC
through 2021. In scenario 1, no circumcisions were performed
for HIV prevention (Botswana, Ethiopia, Kenya, Rwanda, and
in young adolescent boys aged 10–14 years, and the annual
Zambia) from this study.
number of circumcisions performed in men aged 15–29 years
from 2017 through 2021 was equal to the number of VMMCs
Decision Makers’ Program Planning Toolkit 2 Model
performed in 2016. In scenario 2, the annual number of circum-
The DMPPT 2 model, described in depth elsewhere [22, 26],
cisions performed in boys and men aged 10–29 years from 2017
has been used extensively to assess the epidemiological impact
through 2021 was equal to the number of VMMCs performed
and cost-effectiveness of circumcising different age groups of
in 2016. In scenario 3, the annual number of circumcisions
VMMC clients. In brief, the DMPPT 2 model is a simple com-
performed in boys aged 10–14 years from 2017 through 2021
partmental model implemented in Microsoft Excel 2010. The
was equal to the number of VMMCs performed in 2016 and
model tracks the number of males circumcised as newborns
the number of VMMCs in men aged 15–29 years was scaled up
and in each 5-year age group over time, taking into account
aggressively. In scenario 4, the annual number of VMMCs in
age progression and mortality. The model also calculates dis-
boys aged 10–14 years was scaled up aggressively and the num-
counted VMMC program costs and HIV infections averted in
ber of circumcisions in men aged 15–29 years was scaled up very
the population in each year of user-specified VMMC scale-up
aggressively. In all 4 scenarios, the annual number of circumci-
strategies. These are compared to a baseline scenario in which
sions performed in men aged 30–39 years was kept constant at
male circumcision prevalence is held constant at the level found
2016 levels. The numbers of male circumcisions projected in
prior to the initiation of VMMC services for HIV prevention.
each of the 4 scenarios are shown in Supplementary Table 1.
Data Sources
RESULTS
Key model inputs for Lesotho, Malawi, Mozambique, Namibia,
Swaziland, South Africa, Tanzania, Uganda, and Zimbabwe The numbers of male circumcisions that would be performed
can be found in the Supplementary Appendix 1. The DMPPT from 2017 through 2021 in the 4 scenarios described above are
2 model is populated with population, mortality, and HIV shown in Figure 1 for each country and age group. Figure 1 also
incidence and prevalence projections from an external source. compares these to the numbers of circumcisions performed
Scaling Up VMMC for Boys and Young Men • CID 2018:66 (Suppl 3) • S167
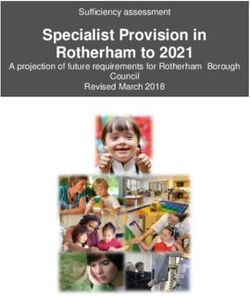
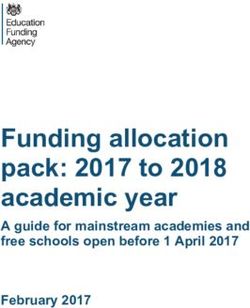
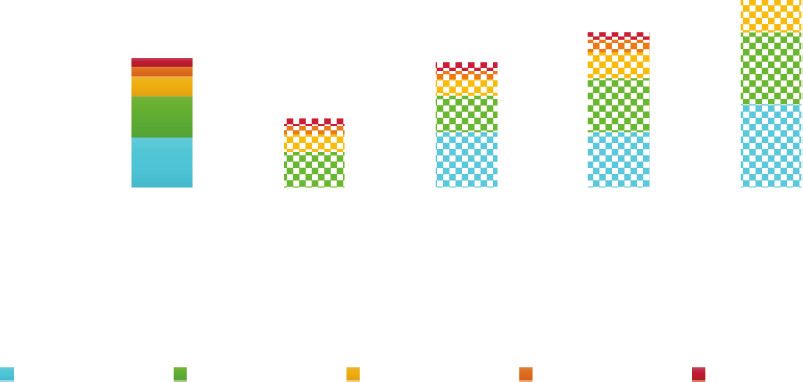
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021 Figure 1. Number of male circumcisions performed. The figure shows the numbers of voluntary medical male circumcisions (VMMCs) performed by age group from the start of each country program through 2016 compared to the estimated total number of VMMCs to be conducted by age group in the 4 scenarios from 2017 to 2021, inclusive. In scenario 1, no VMMCs of boys aged 10–14 years are performed and the annual number of VMMCs of men aged 15–29 years is held constant at 2016 levels. In scenario 2, the annual number of VMMCs of 10- to 29-year-olds is held constant at 2016 levels. In scenario 3, the annual number of VMMCs of boys aged 10–14 years is held constant at 2016 levels, we increase by 50% the number of VMMCs of men aged 15–29 years in 2016, and those numbers are maintained each year thereafter. In scenario 4, we increase by 50% the number of VMMCs of boys aged 10–14 years in 2016 and double the number of VMMCs of men aged 15–29 years in 2016, and those numbers are held constant from 2017 to 2021, inclusive. since the beginning of the VMMC programs in each country for each of the 4 scenarios. Figure 2 also compares these to the and the age distribution of the VMMCs performed to date. male circumcision coverage in these age groups at baseline and Supplementary Figure 1 shows the annual numbers of male cir- by the end of 2016. Figure 2 illustrates that providing circumci- cumcisions performed in scenario 4 and compares these to the sions to boys aged 10–14 years would lead to increased VMMC annual numbers of circumcisions performed since the begin- coverage in the 15- to 29-year age group. In addition, focusing ning of the VMMC programs in each country. These figures on the 10- to 29-year age group, not conducting any VMMCs in highlight that there are notable differences across countries boys aged 10–14 years and holding constant the annual num- in the age distributions of VMMCs provided to date and that ber of VMMCs in men aged 15–29 years at 2016 levels (sce- not performing circumcisions in the 10- to 14-year age group nario 1) would lead to proportions of circumcised males aged would affect countries differently. Whereas circumcisions of 10–29 years in the population by the end of 2021 that range boys aged 10–14 years have made up just 5% of all circumci- from 14% in Malawi to 73% in Tanzania. Holding constant the sions performed to date in Namibia, the proportion of VMMCs annual number of VMMCs in boys and men aged 10–29 years performed in this age group has been between 30% and 50% at 2016 levels (scenario 2) would lead to proportions of cir- in Lesotho, Malawi, Mozambique, Tanzania, Uganda, and cumcised males aged 10–29 years in the population by the end Zimbabwe. These figures also underline that the vast majority of 2021 that range from 18% in Malawi to 93% in Tanzania. of VMMCs performed to date have been circumcisions of ado- Aggressively increasing the annual number of circumcisions lescent boys aged 10–19 years. Seventy percent or more of all of 15- to 29-year-olds and holding constant the annual num- VMMCs performed in Lesotho, Malawi, Mozambique, South ber of VMMCs of boys aged 10–14 years at 2016 levels (sce- Africa, Tanzania, Uganda, and Zimbabwe have been of adoles- nario 3) would lead to proportions of circumcised males aged cent boys aged 10–19 years. 10–29 years in the population by the end of 2021 of ≥60% Figure 2 shows the proportion of circumcised males aged in Lesotho, Mozambique, South Africa, and Tanzania. Very 15–29 and 10–29 years in the population by the end of 2021 aggressively increasing the annual number of circumcisions of S168 • CID 2018:66 (Suppl 3) • Njeuhmeli et al
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
Figure 2. Male circumcision coverage. The figure shows the percentage of males circumcised by the end of 2021 for ages 15–29 years and 10–29 years compared to the
male circumcision coverage for these age groups at baseline and by the end of 2016. In scenario 1, no voluntary medical male circumcisions (VMMCs) are performed in boys
aged 10–14 years, and the annual number of VMMCs in men aged 15–29 years is held constant at 2016 levels. In scenario 1, no VMMCs of boys aged 10–14 years are per-
formed and the annual number of VMMCs of men aged 15–29 years is held constant at 2016 levels. In scenario 2, the annual number of VMMCs of 10- to 29-year-olds is held
constant at 2016 levels. In scenario 3, the annual number of VMMCs of boys aged 10–14 years is held constant at 2016 levels, we increase by 50% the number of VMMCs of
men aged 15–29 years in 2016, and those numbers are maintained each year thereafter. In scenario 4, we increase by 50% the number of VMMCs of boys aged 10–14 years
in 2016 and double the number of VMMCs of men aged 15–29 years in 2016, and those numbers are held constant from 2017 to 2021, inclusive.
15- to 29-year-olds and aggressively increasing the number of VMMC implementation objectives, given historical trends in
circumcisions of 10- to 14-year-olds (scenario 4) would lead to scaling up annual uptake of male circumcision. Tanzania is the
proportions of circumcised males aged 10–29 years in the pop- only country studied that would reach the goal of 90% VMMC
ulation by the end of 2021 of ≥60% in Lesotho, Mozambique, coverage in 10- to 29-year-olds by the end of 2021. It could
South Africa, Tanzania, Uganda, and Zimbabwe. This propor- achieve this goal by maintaining constant the annual number
tion would be ≥80% by the end of 2021 in Mozambique, South of VMMCs in boys and men aged 10–29 years at 2016 levels
Africa, and Tanzania and ≥90% only in Tanzania. (scenario 2). The second country that would come close to
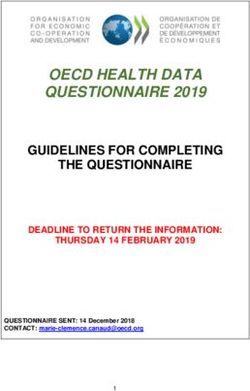
Figure 3 shows historical male circumcision coverage by age reaching the WHO/UNAIDS objective is Mozambique, where
group at the end of each year from the beginning of the VMMC very aggressively increasing the annual number of circumci-
program through 2016 and the projected annual year-end sions of 15- to 29-year-olds and aggressively increasing the
coverage through the end of 2021 for scenario 4, underlining the annual number of VMMCs in boys aged 10–14 years (scenario
contribution of historical coverage in each age group to the cur- 4) would lead to 86% VMMC coverage in 10- to 29-year-olds
rent and future coverage of male circumcision. Baseline VMMC by the end of 2021. South Africa would reach 80% coverage
coverage in most age groups was higher in those countries pro- among 10- to 29-year-olds by the end of 2021 in scenario 4 and
jected to reach the highest coverage levels by the end of 2021, Lesotho would get close to reaching 80% coverage among 10- to
including Lesotho, Mozambique, South Africa, Tanzania, and 29-year-olds in this scenario.
Uganda. Our work highlights the importance of historical num-
Table 1 shows the number of HIV infections averted from 2008 bers of circumcisions conducted and coverage levels in each
through 2025 for each of the 4 scenarios. Whereas scenario 1 led age group to current and future male circumcision coverage.
to the smallest number of HIV infections averted in each country, Baseline VMMC coverage in most age groups was highest in
scenario 4 produced the largest number. Providing circumcisions the countries projected to reach or come close to reaching the
to adolescent boys aged 10–14 years increases both male circum- WHO/UNAIDS target coverage levels by 2021—Tanzania,
cision coverage and VMMC’s impact on HIV infections averted. Mozambique, Lesotho, and South Africa. It is also notewor-
thy that Tanzania, the only country studied that would reach
DISCUSSION
the WHO/UNAIDS target coverage by 2021, is unique in that
The analyses presented in this paper reveal that significant it has had a focused approach to scaling up VMMC since the
changes in VMMC implementation in most countries will beginning of its program [23]. The Tanzania National VMMC
be required to increase the proportion of circumcised 10- to Program has been focusing on scaling up VMMC service deliv-
29-year-olds to 90% by the end of 2021. We explored hypo- ery to males aged 10–34 years since it was launched in 2010 even
thetical scale-up scenarios representing ambitious but feasible though the international guidance at the time recommended
Scaling Up VMMC for Boys and Young Men • CID 2018:66 (Suppl 3) • S169
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
Figure 3. Male circumcision coverage over time. The figure shows historical male circumcision coverage by age group through 2016 and projected coverage until the end
of 2021 in scenario 4, in which we increase by 50% the number of voluntary medical male circumcisions (VMMCs) of boys aged 10–14 years in 2016, we double the number
of VMMCs of men aged 15–29 years in 2016, and those numbers are held constant from 2017 through 2021, inclusive.
scaling up services to males aged 15–49 years [9]. Conversely, Looking forward, these analyses also show the importance of
VMMC coverage levels in certain countries, including Malawi, scaling up VMMC services to adolescent boys aged 10–19 years
Namibia, and Swaziland, have been and continue to be so low and especially of ensuring that circumcision programs include
that attaining WHO/UNAIDS target coverage levels is unlikely young adolescent boys aged 10–14 years. Most of the VMMCs per-
without significant strategic changes in both demand creation formed to date have been circumcisions of adolescent boys aged
and service delivery. 10–19 years and more than a third of clients accessing VMMC
services have been young adolescent boys aged 10–14 years even
Table 1. Human Immunodeficiency Virus Infections Averted Through though roll-out of VMMC programs has not focused on appeal-
Voluntary Medical Male Circumcision, 2008–2025 ing to this age group in most countries. Given the high demand
for services in the 10- to 14-year age group in most countries
Country Scenario 1 Scenario 2 Scenario 3 Scenario 4
and the limited demand for VMMC in men aged ≥20 years [29],
Lesotho 9986 10 622 11 389 12 474
increasing VMMC coverage in younger adolescent boys aged
Malawi 7118 7549 8411 9489
Mozambique 53 993 56 776 62 426 69 886 10–14 years takes advantage of cultural preferences and existing
Namibia 1744 1762 2216 2680 demand for VMMC in this age group. Changing demand creation
South Africa 182 981 187 907 198 056 210 669 and service delivery strategies to explicitly focus on boys aged
Swaziland 7155 7594 8000 8624 10–14 years could lead to further increases in demand for VMMC
Tanzania 43 859 47 019 51 041 56 644
in young adolescent boys. Notably, providing circumcisions to
Uganda 58 616 60 950 66 780 73 777
adolescent boys aged 10–14 years increases male circumcision
Zimbabwe 21 510 22 677 25 681 29 268
coverage in the 10- to 29-year age group and in the 15- to 29-year
The figure shows total human immunodeficiency virus infections averted from 2008
through 2025 for the 4 scenarios. In scenario 1, no voluntary medical male circumcisions age group as well as increasing VMMC’s impact on HIV infections
(VMMCs) of boys aged 10–14 years are performed and the annual number of VMMCs of
men aged 15–29 years is held constant at 2016 levels. In scenario 2, the annual number
averted. Scaling up VMMC coverage in men aged 10–29 years to
of VMMCs of 10- to 29-year-olds is held constant at 2016 levels. In scenario 3, the annual 90% will require significantly increasing the number of circumci-
number of VMMCs of boys aged 10–14 years is held constant at 2016 levels, we increase
by 50% the number of VMMCs of men aged 15–29 years in 2016, and those numbers sions provided to both 15- to 29-year-olds and 10- to 14-year-olds.
are maintained each year thereafter. In scenario 4, we increase by 50% the number of A number of limitations should be kept in mind when inter-
VMMCs of boys aged 10–14 years in 2016 and double the number of VMMCs of men aged
15–29 years in 2016, and those numbers are held constant from 2017 to 2021, inclusive. preting our findings. The DMPPT model’s limitations have been
S170 • CID 2018:66 (Suppl 3) • Njeuhmeli et al
described in detail elsewhere [22]. The model relies on available article are the sole responsibility of projects Supporting Operational AIDS
Research (SOAR) and AIDSFree, the Population Council, and the authors.
national and subnational demographic, epidemiological, and
Financial support. This manuscript was made possible by the gener-
program data and estimates of varying quality and complete- ous support of the American people through PEPFAR with USAID under
ness. The main limitation of this work is its reliance on pro- the cooperative agreement project SOAR (number AID-OAA-14-00026),
gram data. We sought to apply scale-up scenarios representing and cooperative agreement Strengthening High Impact Interventions for an
AIDS-Free Generation (number AID-OAA-A-14-00046).
feasible VMMC program implementation objectives given 2016 Supplement sponsorship. This article appears as part of the supplement
program accomplishments and historical scale-up trends. In “Adolescent Voluntary Medical Male Circumcision: Vital Intervention Yet
addition, due to data availability, our analysis is limited to 9 of Improvements Needed,” sponsored by Johns Hopkins University.
Potential conflicts of interest. All authors: No reported conflicts.
the 14 VMMC priority countries supported by PEPFAR.
All authors have submitted the ICMJE Form for Disclosure of Potential
Although our analysis does not address the financial and other Conflicts of Interest. Conflicts that the editors consider relevant to the con-
resource implications of each scenario, assessments of existing tent of the manuscript have been disclosed.
site capacity reveal that many sites are operating below capacity.
References
Previous work identified substantial differences in unit costs of
1. Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A.
VMMC within and among countries, indicating that substantial
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
Randomized, controlled intervention trial of male circumcision for reduction of
efficiency gains could be made in VMMC service delivery [30]. In HIV infection risk: the ANRS 1265 trial. PLoS Med 2005; 2:e298.
2. Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young
one study, average efficiency scores ranged from 51% in Zambia to men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007; 369:643–56.
70% in South Africa [31]. As a result, 10- to 14-year-olds present- 3. Gray RH, Kigozi G, Serwadda D, et al. Male circumcision for HIV prevention in
men in Rakai, Uganda: a randomised trial. Lancet 2007; 369:657–66.
ing for circumcision in the absence of tailored demand creation 4. Binagwaho A, Pegurri E, Muita J, Bertozzi S. Male circumcision at different ages
programs are readily being accommodated in most settings within in Rwanda: a cost-effectiveness study. PLoS Med 2010; 7:e1000211.
5. Kahn JG, Marseille E, Auvert B. Cost-effectiveness of male circumcision for HIV
the confines of current budgets, and many sites have the capacity prevention in a South African setting. PLoS Med 2006; 3:e517.
to accommodate additional clients. Furthermore, the popular- 6. Njeuhmeli E, Forsythe S, Reed J, et al. Voluntary medical male circumcision:
modeling the impact and cost of expanding male circumcision for HIV preven-
ity of male circumcision among adolescents this age, along with
tion in Eastern and Southern Africa. PLoS Med 2011; 8:e1001132.
growing evidence that adolescent girls and young women are 7. Schwartländer B, Stover J, Hallett T, et al; Investment Framework Study Group.
expressing preference for circumcised sexual partners [32], may Towards an improved investment approach for an effective response to HIV/
AIDS. Lancet 2011; 377:2031–41.
be creating new social norms that could also influence their older 8. World Health Organization/Joint United Nations Programme on HIV/AIDS.
peers aged 15–29 years to come forward for VMMC services. New data on male circumcision and HIV prevention: policy and programme
implications. WHO/UNAIDS technical consultation on male circumcision and
In conclusion, our analysis has important implications for HIV prevention: research implications for policy and programming. Geneva,
countries and their international partners as they consider next Switzerland: WHO/UNAIDS, 2007.
9. World Health Organization/Joint United Nations Programme on HIV/AIDS.
steps in VMMC implementation to meet the WHO/UNAIDS Joint strategic action framework to accelerate the scale-up of voluntary medical
target. Our study highlights that most countries will not male circumcision for HIV prevention in Eastern and Southern Africa, 2012–
2016. Geneva, Switzerland: WHO/UNAIDS, 2011.
increase the proportion of circumcised 10- to 29-year-olds to
10. World Health Organization/Joint United Nations Programme on HIV/AIDS.
90% by 2021 without significant changes in VMMC implemen- A framework for voluntary medical male circumcision: effective HIV preven-
tation. The likelihood of countries achieving the 2021 target is tion and a gateway to improved adolescent boys’ & men’s health in Eastern and
Southern Africa by 2021. Geneva, Switzerland: WHO/UNAIDS, 2016.
influenced partly by the historical numbers of circumcisions 11. Joint United Nations Programme on HIV/AIDS. Prevention gap report. Geneva,
conducted and coverage levels attained, and some countries are Switzerland: UNAIDS, 2016.
12. Anderson SJ, Cherutich P, Kilonzo N, et al. Maximising the effect of combination
unlikely to reach WHO/UNAIDS target coverage levels with- HIV prevention through prioritisation of the people and places in greatest need: a
out significant strategic changes in both demand creation and modelling study. Lancet 2014; 384:249–56.
13. Joint United Nations Programme on HIV/AIDS. Fast track: ending the AIDS epi-
service delivery. Scaling up VMMC coverage in males aged demic by 2030. Geneva, Switzerland: UNAIDS, 2014.
10–29 years will require increasing the number of circumci- 14. Jones A, Cremin I, Abdullah F, et al. Transformation of HIV from pandemic to
low-endemic levels: a public health approach to combination prevention. Lancet
sions provided to 10- to 14-year-olds and 15- to 29-year-olds.
2014; 384:272–9.
15. United States President’s Emergency Plan for AIDS Relief. PEPFAR 3.0—
Supplementary Data Controlling the epidemic: delivering on the promise of an AIDS-free generation.
Supplementary materials are available at Clinical Infectious Diseases online. Washington, DC: Office of the Global AIDS Coordinator, 2014.
Consisting of data provided by the authors to benefit the reader, the posted 16. Awad SF, Sgaier SK, Ncube G, et al. A reevaluation of the voluntary medical male
circumcision scale-up plan in Zimbabwe. PLoS One 2015; 10:e0140818.
materials are not copyedited and are the sole responsibility of the authors,
17. Awad SF, Sgaier SK, Tambatamba BC, et al. Investigating voluntary medical male
so questions or comments should be addressed to the corresponding author.
circumcision program efficiency gains through subpopulation prioritization:
insights from application to Zambia. PLoS One 2015; 10:e0145729.
Notes 18. Kripke K, Chen PA, Vazzano A, et al. Cost and impact of voluntary medical male
Acknowledgments. The authors thank John Stover of Avenir Health, circumcision in South Africa: focusing the program on specific age groups and
provinces. PLoS One 2016; 11:e0157071.
who developed the DMPPT 2 model at the request of the US Agency for
19. Kripke K, Chimbwandira F, Mwandi Z, et al. Voluntary medical male circumci-
International Development (USAID), under the USAID-funded Health
sion for HIV prevention in Malawi: modeling the impact and cost of focusing the
Policy Project. The authors also thank Matt Hamilton of Avenir Health for program by client age and geography. PLoS One 2016; 11:e0156521.
his work in updating the model version used for this manuscript. 20. Kripke K, Hatzold K, Mugurungi O, et al. Modeling impact and cost-effectiveness
Disclaimer. The information provided does not necessarily reflect the of increased efforts to attract voluntary medical male circumcision clients ages
views of USAID, PEPFAR, or the US government, and the contents of this 20-29 in Zimbabwe. PLoS One 2016; 11:e0164144.
Scaling Up VMMC for Boys and Young Men • CID 2018:66 (Suppl 3) • S171
21. Kripke K, Okello V, Maziya V, et al. Voluntary medical male circumcision for HIV 27. Futures Institute. Goals manual: a model for estimating the effects of interven-
prevention in Swaziland: modeling the impact of age targeting. PLoS One 2016; tions and resource allocation on HIV infections and deaths. Glastonbury, CT:
11:e0156776. Futures Institute, 2011.
22. Kripke K, Opuni M, Schnure M, et al. Age targeting of voluntary medical male 28. Ministry of Health. Swaziland Incidence Measurement Survey (SHIMS): first
circumcision programs using the Decision Makers’ Program Planning Toolkit findings report. Mbabane, Swaziland, 2012.
(DMPPT) 2.0. PLoS One 2016; 11:e0156909. 29. Njeuhmeli E, Hatzold K, Gold E, et al. Lessons learned from scale-up of volun-
23. Kripke K, Perales N, Lija J, et al. The economic and epidemiological impact of tary medical male circumcision focusing on adolescents: benefits, challenges,
focusing voluntary medical male circumcision for HIV prevention on specific age and potential opportunities for linkages with adolescent HIV, sexual, and
groups and regions in Tanzania. PLoS One 2016; 11:e0153363. reproductive health services. J Acquir Immune Defic Syndr 2014; 66(Suppl
24. Kripke K, Vazzano A, Kirungi W, et al. Modeling the impact of Uganda’s safe male 2):S193–9.
circumcision program: implications for age and regional targeting. PLoS One 30. Bollinger L, Adesina A, Forsythe S, Godbole R, Reuben E, Njeuhmeli E. Cost
2016; 11:e0158693. drivers for voluntary medical male circumcision using primary source data from
25. Hankins C, Warren M, Njeuhmeli E. Voluntary medical male circumcision sub-Saharan Africa. PLoS One 2014; 9:e84701.
for HIV prevention: new mathematical models for strategic demand cre- 31. Salas-Ortiz A, La Hera-Fuentes G, Nance N, Sosa-Rubi SG, Bautista-Arredondo
ation prioritizing subpopulations by age and geography. PLoS One 2016; S. Efficiency and quality. How management practices influence the provision of
11:e0160699. voluntary medical male circumcision services in four African countries. PLoS
26. Kripke K, Njeuhmeli E, Samuelson J, et al. Assessing progress, impact, and next One. In press.
steps in rolling out voluntary medical male circumcision for HIV prevention in 14 32. Kaufman MR, Dam KH, Sharma, K, et al. Females’ peer influence and support for
priority countries in Eastern and Southern Africa through 2014. PLoS One 2016; adolescent males receiving voluntary medical male circumcision services. Clin
Downloaded from https://academic.oup.com/cid/article/66/suppl_3/S166/4956270 by guest on 29 September 2021
11:e0158767. Infect Dis 2018; 66(Suppl 3):S183–8.
S172 • CID 2018:66 (Suppl 3) • Njeuhmeli et al


You can also read