Safety of transglutaminase-induced corneal collagen cross-linking on the central cornea thickness and intraocular pressure in vivo version 1; ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
F1000Research 2023, 12:48 Last updated: 05 MAR 2024
RESEARCH ARTICLE
Safety of transglutaminase-induced corneal collagen cross-
linking on the central cornea thickness and intraocular
pressure in vivo [version 1; peer review: awaiting peer review]
Puspita Hapsari Sitorasmi , Yuniar Sarah Ningtiyas, Indri Wahyuni,
Yulia Primitasari
Department of Ophthalmology, Airlangga University, Surabaya, East Java, 60286, Indonesia
v1 First published: 12 Jan 2023, 12:48 Open Peer Review
https://doi.org/10.12688/f1000research.129694.1
Latest published: 12 Jan 2023, 12:48
https://doi.org/10.12688/f1000research.129694.1 Approval Status AWAITING PEER REVIEW
Any reports and responses or comments on the
Abstract article can be found at the end of the article.
Background: Corneal collagen cross-linking (CXL) is a procedure for
making bonds that connect polymer chains to one another. Corneal
CXL aims to slow or stop the progression of keratoconus by using
photooxidative therapy so as to increase stromal rigidity.
Transglutaminase enzymes are currently widely used in the food
industry. Recent studies have shown that mRNA, fibronectin, and
transglutaminase were found to be more abundant in human corneal
keratocytes treated with UVA and riboflavin. Transglutaminase is
considered to reduce discomfort caused by UVA irradiation.
Methods: A total of 21 white New Zealand rabbits were divided into
three groups, namely, transglutaminase-induced CXL group,
epithelial-off CXL group, and transepithelial CXL group. The ocular
surface was treated with a 1 U/mL microbial transglutaminase
solution, and both the epithelial-off and transepithelial groups were
exposed to clinical ultraviolet A-riboflavin (UVA/RF). The efficacy of
each group was evaluated on the 14th day after the procedures. The
central corneal thickness (CCT) and intraocular pressure (IOP) were
evaluated using Corneal Visualization Scheimpflug Technology (Corvis
ST).
Results: The transglutaminase-induced CXL group exhibited the
highest mean CCT (370.14 ± 38.85) in comparison with the UVA/RF
epithelial-off group (368.00 ± 25.48) and the UVA/RF transepithelial
group (369.86 ± 23.43). The transglutaminase-induced CXL group had
the highest IOP mean (8.50 ± 3.02) compared with the UVA/RF
epithelial-off (6.50 ± 3.07) and UVA/RF transepithelial groups (7.00 ±
1.90). There were no significant differences in CCT (p = 0.990) or IOP (p
= 0.563) between the groups.
Conclusions: The findings of this study suggest that there are no
significant differences between the transglutaminase-induced CXL
group and the UVA/RF CXL group. The safety of transglutaminase-
induced CXL could be comparable to that of UVA/RF CXL in terms of
Page 1 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
altering CCT and IOP, which are two factors contributing to corneal
rigidity.
Keywords
Central corneal thickness, corneal collagen cross-linking, Corvis ST,
intraocular pressure, transglutaminase
Corresponding author: Yulia Primitasari (yulia-p@fk.unair.ac.id)
Author roles: Sitorasmi PH: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Project Administration,
Resources, Software, Visualization, Writing – Original Draft Preparation, Writing – Review & Editing; Ningtiyas YS: Conceptualization,
Data Curation, Formal Analysis, Investigation, Methodology, Project Administration, Resources, Software; Wahyuni I: Conceptualization,
Formal Analysis, Methodology, Supervision, Validation, Writing – Review & Editing; Primitasari Y: Conceptualization, Data Curation,
Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – Review & Editing
Competing interests: No competing interests were disclosed.
Grant information: This research received a grant of Faculty Excellence in Research Awards from Universitas Airlangga (No.
1331/UN3.1.1/HK/2022).
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Copyright: © 2023 Sitorasmi PH et al. This is an open access article distributed under the terms of the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
How to cite this article: Sitorasmi PH, Ningtiyas YS, Wahyuni I and Primitasari Y. Safety of transglutaminase-induced corneal
collagen cross-linking on the central cornea thickness and intraocular pressure in vivo [version 1; peer review: awaiting peer
review] F1000Research 2023, 12:48 https://doi.org/10.12688/f1000research.129694.1
First published: 12 Jan 2023, 12:48 https://doi.org/10.12688/f1000research.129694.1
Page 2 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
Introduction
One of the most important factors in diagnosing several corneal disorders is the central corneal thickness (CCT).1
Dynamic CCT is considered to contain critical information about several eye conditions linked to endothelial corneal
dystrophies or collagen abnormalities.2 Corneal stroma form 90% of the total thickness of the cornea.3 Intraocular
pressure (IOP) is influenced by changes in CCT. The significant increase in IOP after corneal collagen cross-linking
(CXL) treatment may be due to the increased rigidity of the cornea.4 Corneal Visualization Scheimpflug Technology
(Corvis ST) is a relatively new technology that has been studied for its ability to distinguish between normal corneas and
keratoconus.5 Corvis ST characteristics are also responsible for changes following CXL including CCT and IOP;
consequently, it has the potential to be used to monitor the result of CXL.6
The cornea is a transparent and avascular tissue, and nutrients and oxygenation of the cornea are obtained by diffusion
through the aqueous humor, tear film, and limbal blood vessels.7 Corneal ectasia is a condition where the cornea's
thickness decreases from normal values. Keratoconus, pellucid marginal degeneration, and post-refractive ectasia are a
few examples of corneal ectasia.3 In the general population, keratoconus has been estimated to occur 50–230 times per
100,000 people.4 The prevalence of post-refractive ectasia ranges from 0.04% to 0.6% in the general population, and it is
expected to rise in conjunction with the public's rising appreciation for the procedure.8,9 The use of spectacles and rigid
gas permeable contact lenses is the only non-operative treatment for corneal ectasia.2 In treating progressive keratoconus,
corneal CXL has become the gold standard because it strengthens the corneal structure, preventing ectasia.10
Currently, riboflavin and ultraviolet-A (UVA) are used in conventional CXL. However, the CXL method using riboflavin
and UVA is considered to cause discomfort to patients due to the UVA rays.11,12 Transglutaminase was hypothesized as a
potential way for inducing CXL. Transglutaminase reduces discomfort due to UVA irradiation and inhibits keratocyte
cell death. It is envisaged that using accessible enzymatic products as a treatment technique will be easier and reduce the
cost of CXL therapy.13
In this study, New Zealand rabbits were divided into three groups, namely the transglutaminase-induced CXL group,
Ultraviolet A/riboflavin (UVA/RF) epithelial-off group, and UVA/RF transepithelial group. This study aims to evaluate
the safety of transglutaminase-induced CXL on CCT and IOP in vivo.
Methods
Subject and measures
Ethical approval was obtained from the Animal Care and Use Committee (ACUC) Faculty of Veterinary Medicine,
Universitas Airlangga (No. 2.KEH.071.07.2022). All procedures were performed to ethical standards.
We calculated the sample size using the Lemeshow formula. Twenty-one normal New Zealand white rabbits were
enrolled, and the right eye was treated. All the rabbits were divided into three groups, namely, transglutaminase-induced
CXL group, epithelial-off CXL group, and transepithelial CXL group. There were seven rabbits in each group and we
used random allocation. All rabbits were healthy males, between two and three months of age, and weighed between 3 and
4 kg. All rabbits were provided by the Faculty of Veterinary Medicine, Universitas Airlangga. The experiments were
performed at Veterinary Hospital Universitas Airlangga.
The equipment utilized in this study included individual rabbit cages in an ideal room temperature (24°C), enough
ventilation, and good ad libitum; the portions of food and drink were the same for all rabbits.
Cross-linking procedure
Anesthesia was induced via intramuscular injection of 0.1 mL/kgBW xylazine 2% (Xyla, Interchemie, Netherland)
and 6–10 mg/kgBW ketamine (Ket-A-100®, Agrovet Market s.a. Lima, Peru). The right eyes were treated, and the
contralateral eyes served as untreated controls kept closed during the procedure. The corneal epithelium of the first
group was removed using an 8 mm MacRae Photorefractive Keratectomy (PRK) well and alcohol 20% for 40 seconds,
then the loose epithelium was removed with a hockey knife. After the epithelial-off procedure, transglutaminase solution
1 U/mL (Zedira, Germany) was dripped onto the cornea every two minutes for 30 minutes, for a total of 16 times. The
cornea epithelial of the transepithelial group was not removed, then the riboflavin transepithelial (Peschke TE, Peschke
Meditrade GmbH, Switzerland) was dripped onto the cornea every two minutes for 30 minutes. Subsequently, UVA
exposure (365 5 nm, 3 mW/cm2, 8-mm diameter light spot) was performed using a UVA lamp CCL-Vario System
(Peschke Trade GmbH, Switzerland) while continuously dripping the riboflavin onto the cornea every two minutes for
30 minutes. The cornea epithelial of the epithelial-off group was removed with the same procedure, then the riboflavin
epithelial-off (Ribolink, Aurolab, India) was dripped two times onto the cornea. Subsequently, UVA exposure was
performed using the same technique while continuing to drip the riboflavin onto the cornea every five minutes for
Page 3 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
30 minutes.12,13 Immediately following the procedure, an eye ointment containing chloramphenicol (Cendo, Indonesia)
was used. The ointment was administered every eight hours for 14 days.
CCT and IOP evaluation procedure
Fourteen days after treatment, the CCT and IOP of the rabbits were evaluated using Corvis ST (Oculus Optikgeräte
GmbH, Wetzlar, Germany). Before the procedure, the rabbits were first anesthetized using 0.15 mL/kg xylazine and
6–10 mg/kg ketamine intramuscularly. All examinations were conducted by the same experienced ophthalmology
technician to remove potential interobserver variability. The heads of the rabbits were positioned in front of the
instrument to ensure that the cornea was 11 mm away from the air nozzle. In the instance of improper imaging or
alignment concerns, a retake was performed in order to meet quality standards. The air puff was released and the ultrafast
camera captured 140 horizontal cross-sectional corneal images; subsequently, CCT and IOP were determined.
Statistical analysis
Comparative between data were tested using the one-way ANOVA followed with a post hoc test if the data were normally
distributed. If the data were not normally distributed, they would be analyzed using the Kruskal–Wallis test and continued
by using the Mann–Whitney test. The result is considered significant if the p-value is < 0.05. All statistical data were
processed using SPSS 26.0 software (RRID:SCR_002865) (SPSS, Chicago. IL, USA).
All the protocols are published in protocols.io (https://doi.org/10.17504/protocols.io.261ge3eool47/v1).
Results
Comparison of CCT using Corvis ST
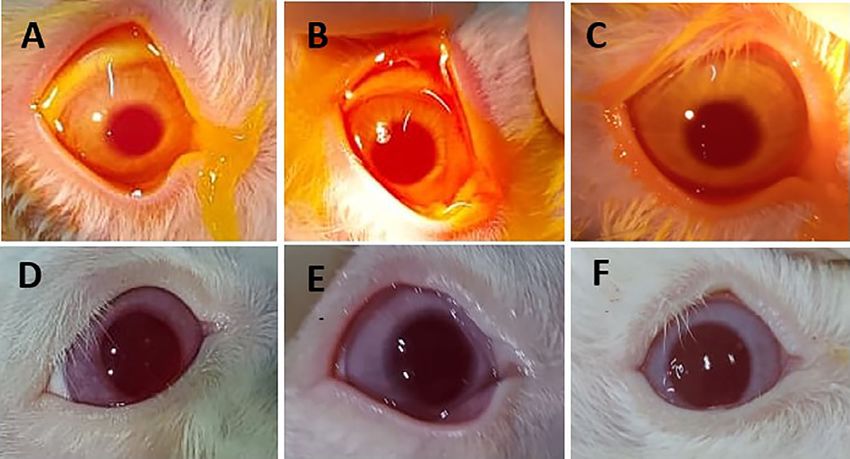
We found no secondary infection in the rabbit's cornea during the observation period and 14 days after cross-linking
(Figure 1). Our study demonstrated that the transglutaminase-induced CXL group had the highest value of CCT at
428 μm. The lowest value was from the UVA/RF epithelial-off group with CCT 321 μm. In comparison with the
UVA/RF epithelial-off CXL group and the UVA/RF transepithelial CXL group, the CCT of the transglutaminase-
induced CXL group displayed the highest mean score, whereas the UVA/RF epithelial-off CXL group had the lowest
mean score (Table 1). Analysis using the one-way ANOVA test revealed no significant differences between any of the
groups (p-value = 0.990).
Comparison of IOP using Corvis ST
The results of the research showed that the IOP was lowest in the UVA/RF transepithelial and the UVA/RF epithelial-off
CXL groups with 5.50 mmHg. The highest IOP was in the transglutaminase-induced CXL group with 13.50 mmHg. The
mean IOP in the transglutaminase-induced CXL group was highest among three groups (Table 2). Analysis using the
Figure 1. Anterior segment of rabbit day 0; (A) Transglutaminase, (B) UVA/RF epithelial-off, (C) UVA/RF
transepithelial. Anterior segment of rabbit day 14; (D) Transglutaminase, (E) UVA/RF epithelial-off, (F) UVA/
RF transepithelial.
Page 4 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
Table 1. Comparison of CCT based on Corvis ST measurement.
Mean Std. Deviation Minimum Maximum p-value
Transglutaminase 370.14 42.51 337.00 428.00 0.990
UVA/RF epithelial-off 368.00 25.48 321.00 423.00
UVA/RF transepithelial 369.86 23.43 330.00 397.00
Table 2. Comparison of IOP based on Corvis ST measurement.
Median Std. Deviation Minimum Maximum p-value
Transglutaminase 8.50 3.02 6.00 13.50 0.563
UVA/RF epithelial-off 6.50 3.07 5.50 13.00
UVA/RF transepithelial 7.00 1.90 5.50 10.50
Kruskal–Wallis test revealed no significant differences between any of the groups with p-value = 0.563. There were no
signs of infection and inflammation in the three groups immediately after treatment and 14 days after treatment.
Discussion
CCT after CXL
This study used two conventional CXL groups, namely, the UVA/RF epithelial-off group and the UVA/RF transepithe-
lial group, compared with the transglutaminase-induced CXL group. In contrast to earlier research by Wu et al.12, which
solely employed UVA/RF epithelial-off techniques, transepithelial procedures were performed more often at the time of
this investigation to prevent possible complications.
According to the results, there were no statistically significant differences in CCT between the groups (p-value = 0.990).
The same result was obtained from the study that Wu et al. conducted in 2019, in which there was insignificant difference
between the CCT of rabbits given CXL and CCT in the control group.12,13 Although epithelial remodeling and stroma
edema disappear a few days after treatment, CCT has been reported to be responsible for corneal thickness changes over a
longer time; this theory may explain why there is currently no significant CCT thickening.14
The CCT decreases in the first few months after the UVA/RF epithelial-off CXL method, and then it will increase in the
following 12 months. The CCT in UVA/RF transepithelial CXL tends to be more stable. The decrease in CCT after
performing CXL with the epithelial-off method can be caused by several factors, including compaction of collagen fibers,
dehydrated corneal stroma, and apoptosis of keratocytes caused by UVA rays. This could explain why, in this study, CXL
using UVA/RF epithelial-off had the lowest CCT, because in this method a corneal epithelial debridement procedure was
performed as well as UVA light irradiation. Factors that trigger an increase in CCT can be caused by repopulation of
keratocytes, where this process requires a longer time, which is around six months.14,15
Transglutaminase is an enzyme that catalyzes the formation of isopeptide bonds between proteins. This can occur through
cross-linking of proteins due to γ-glutamyl lysine bonds or due to the unification of primary amino acids with peptide
bond residues and glutamine. Recent studies have shown that mRNA, fibronectin, and transglutaminase were found to be
more abundant in human corneal keratocytes treated with UVA and riboflavin. This induction by transglutaminase is
proposed as a new mechanism for cross-linking. The CXL transglutaminase treatment did not use UVA irradiation, which
could be the cause of the CCT in the transglutaminase group having the highest average.13,15
IOP after CXL
The group with transglutaminase-induced CXL had the highest IOP among the groups, although there was no significant
difference between groups (p-value = 0.563). The increase in IOP can be one of the factors that explain an increase in
corneal rigidity after transglutaminase administration as CXL. A previous study by Kymionis et al.16 showed a mean rise
of 2–3 mmHg after UVA/RF CXL due to increased corneal stiffness. Several studies stated that there were significant
differences in IOP after CXL. These studies use different measuring instruments from those used in our study, namely
Goldmann Applanation Tonometry and Tonopen.16–18 In addition, these results can be interpreted as the safety of
transglutaminase-induced CXL can be compared with UVA/RF CXL in influencing CCT and IOP, which is one of the
factors in increasing corneal rigidity.12,13
Page 5 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
Cornea CXL is a procedure to create bonds that connect polymer chains. The CXL procedure can change the
biomechanics of the human cornea by increasing corneal rigidity by up to 328.9%.19 Morphologically, the formation
of cross-links increases the distance between molecules because the collagen polypeptide chains are separated.20 In
conventional CXL, two phases are employed. The corneal saturation step acts as a photosensitizer to promote cross-
linking, while the UVA irradiation stage protects the underlying tissues from UVA-induced damage.21 Conventional
CXL will result in cross-linking through two pathways, namely oxidative and glycosylation pathways.22 Activated
riboflavin, in addition to activating oxidative pathways, can also support the occurrence of glycosylated cross-linking in
proteoglycans and collagen fibers through a mechanism mediated by advanced glycation end products.23,24
Recent studies have shown that mRNA, fibronectin, and transglutaminase are more abundant in human corneal
keratocytes treated with UVA and riboflavin. Induction by transglutaminase is proposed as a new mechanism for
cross-linking.9,10 One of the possible advantages of CXL transglutaminase is that it prevents the loss of keratocytes and
the discomfort usually experienced by patients treated with UVA and riboflavin.12,13 Transglutaminase facilitates the
formation of the ε-(γ-glutamyl) lysine isopeptide bond, which mediates the biochemical reaction between glutamic acid
and lysine.25 The cornea is mainly constructed of type I collagen and is rich in glutamic acid and lysine. Corneal collagen
fibers could be cross-linked by transglutaminase, potentially resulting in more rigid mechanical properties.26
Conclusions
The findings of this study demonstrate that there were no significant differences between the transglutaminase-induced
CXL group and UVA/RF CXL group, so the safety of transglutaminase-induced CXL could be comparable with that of
UVA/RF CXL in terms of altering CCT and IOP, which are two factors contributing to corneal rigidity.
Limitations
This study's limitations included the limited follow-up period and the absence of any measurements before the CXL
procedure. Recolonization of stromal keratocytes and enhanced stromal fiber density are complete six months following
CXL; hence, a six-month follow-up may be recommended.27 This study's brief research period was a constraint; if the
research had a longer period and pre-post CXL procedure examination, it might have produced the best results.
Consequently, more research into the use of transglutaminase as a treatment for CXL and corneal ectasia is warranted.
Ethical approval
Ethical approval was obtained from the Animal Care and Use Committee (ACUC) Faculty of Veterinary Medicine,
Universitas Airlangga (No. 2.KEH.071.07.2022).
Data availability
Underlying data
Figshare: Data CCT and IOP. https://doi.org/10.6084/m9.figshare.21754223.28
This project contains the following underlying data
- Dataset of CCT and IOP of rabbits. Data obtained from biomechanical examination with Corvis ST 14 days
after CXL.
Reporting guidelines
Figshare: ARRIVE checklist. https://doi.org/10.6084/m9.figshare.21778649.29
Data are available under the terms of the Creative Commons Attribution 4.0 International license (CC-BY 4.0).
Acknowledgements
The authors thank PT Optik Tunggal Sempurna for lending the Corvis ST (Oculus Optikgeräte GmbH, Wetzlar,
Germany); Surabaya Eye Clinic for lending the CCL Vario System; Dr. Mahmudah, Ir., MKes (Faculty of Public
Health – Universitas Airlangga) for statistical and methodology advice.
Page 6 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
References
1. Lin D, Tian L, Yuan C, et al.: Evaluation of central corneal thickness 38–47.
in keratoconus and normal corneas during air puff indentation. Publisher Full Text
Int. J. Ophthalmol. 2016; 6(1): 130–144. 16. Kymionis GD, Grentzelos MA, Kounis GA, et al.:
2. Krachmer J, Mannis M, Holland E: Cornea: Fundamentals, diagnosis, Intraocular pressure measurements after corneal
and management. 3rd ed. Mosby Elsevier; 2011; 3–15. collagen cross-linking with riboflavin and ultraviolet A
3. Weisenthal R, Daly M, Freitas D, et al.: Basic and Clinical Science. in eyes with keratokonus. J. Cataract Refract. Surg. 2010; 36(10):
Externa Disease and Cornea. AAO. 2021; 161–171. 1724–1727.
Publisher Full Text
4. Kasumovic SS, Mavija M, Kasumovic A, et al.: Intraocular Pressure
Measurements Referring to the Corneal Thickness in 17. Wollensak G, Spoerl E, Seiler T: Riboflavin/ultraviolet-a–induced
Keratoconic Eyes After Corneal Cross-linking with Riboflavin collagen cross-linking for the treatment of keratoconus.
and Ultraviolet A. Med. Arch. (Sarajevo, Bosnia and Herzegovina). Am. J. Ophthalmol. 2003; 135(5): 620–627.
2015; 69(5): 334–338. PubMed Abstract|Publisher Full Text
5. Ambrósio R Jr, Ramos I, Luz A, et al.: Dynamic ultrahigh speed 18. Liaboe C, Kaufman SC, Bogaard J, et al.: Alterations In The
Scheimpflug imaging for assesing corneal biomechnical Measured Intraocular Pressure Following Corneal Collagen
properties. Rev. Bras. Oftalmol. 2013; 72(2): 99–102. Cross Linking. Int. J. Eye Bank. 2020; 8(2): 8–10.
Publisher Full Text 19. Li G, Fan ZJ, Peng XJ: Corneal collagen cross-linking for corneal
6. Jabbarvand M, Moravvej Z, Shahraki K, et al.: Corneal ectasia of post-LASIK: One-year results. Int. J. Ophthalmol. 2012;
biomechanical outcome of collagen cross-linking in keratoconic 5(2): 190–195.
patients evaluated by Corvis ST. Eur. J. Ophthalmol. 2021; 31(4): PubMed Abstract|Publisher Full Text
1577–1583. 20. Sorkin N, Varssano D: Corneal collagen cross-linking:
PubMed Abstract|Publisher Full Text A systematic review. Ophthalmologica. 2014; 232(1): 10–27.
7. Kun Cahyandari O, Komaratih E, Sasono W, et al.: The Effect of Publisher Full Text
Limbal Mesenchymal Stem Cell Secretome on Corneal 21. Ocak SY, Mangan MS, Elçioǧlu MN: The Intraoperative Corneal
Expression of Interleukin-1 in Experimental Model of Corneal Pachymetry Changes during Accelerated Corneal Cross-linking
Alkali Injury. Int. J. Res. Publ. 2022; 95(1): 326–332. in Progressive Keratoconus Patients with Thin Corneas. Korean
Publisher Full Text J. Ophthalmol. 2021; 35(6): 438–442.
8. Bohac M, Koncarevic M, Pasalic A, et al. : Incidence and Clinical PubMed Abstract|Publisher Full Text|Free Full Text
Characteristics of Post LASIK Ectasia: A Review of over 30,000 22. Richoz O, Mavrakanas N, Pajic B, et al.: Corneal collagen cross-
LASIK Cases. Semin. Ophthalmol. 2018; 33(7–8): 869–877. linking for ectasia after LASIK and photorefractive
Publisher Full Text keratectomy: Long-term results. Ophthalmology. 2013; 120(7):
9. Alvani A, Hashemi H, Pakravan M, et al.: Post-LASIK Ectasia Versus 1354–1359.
Keratokonus: An in vivo Confocal Microscopy Study. Cornea. PubMed Abstract|Publisher Full Text
2020; 39(8): 1006–1012. 23. Chunyu T, Xiujun P, Zhengjun F, et al.: Corneal collagen cross-
Publisher Full Text linking in keratokonus: A systematic review and meta-analysis.
10. Abbondanza M, Abbondanza G, De Felice V, et al.: Long-term Sci. Rep. 2014; 4: 25–31.
results of mini asymmetric radial keratotomy and corneal 24. Stachon T, Wang J, Song X, et al. : Impact of cross-linking/
cross-linking for the treatment of keratoconus. Korean riboflavin-UVA-photodynamic inactivation on viability,
J. Ophthalmol. 2020; 33(2): 189–195. apoptosis and activation of human keratocytes in vitro.
11. Wolle MA, Randleman JB, Woodward MA: Complications of J. Biomed. Res. 2015; 29(4): 321–325.
Refractive Surgery: Dctasia After Refractive Surgery. 25. Griffin M, Casadio R, Bergamini CM: Transglutaminases: Nature’s
Int. Ophthalmol. Clin. 2016; 56(2): 127–139. biological glues. Biochem. J. 2002; 368(2): 377–396.
PubMed Abstract|Publisher Full Text|Free Full Text PubMed Abstract|Publisher Full Text|Free Full Text
12. Wu Y, Song W, Tang Y, et al.: Efficacy and safety of 26. Kopsachilis N, Tsaousis KT, Tsinopoulos IT, et al.: A novel
transglutaminase-induced corneal stiffening in rabbits. mechanism of UV-A and riboflavin-mediated corneal cross-
Transl. Vis. Sci. Technol. 2019; 8(6): 1–9. linking through induction of tissue transglutaminases. Cornea.
13. Wu Y, Song W, Tang Y, et al.: Biomechanical Changes after in vivo 2013; 32(7): 1034–1039.
Enzyme-Induced Corneal Cross-linking in Rabbits. Ophthalmic PubMed Abstract|Publisher Full Text
Res. 2020; 63(5): 501–506. 27. Mazzotta C, Balestrazzi A, Traversi C, et al.: Treatment of
PubMed Abstract|Publisher Full Text progressive keratoconus by riboflavin-UVA-induced
14. Cifariello F, Minicucci M, Di Renzo F, et al.: Epi-Off versus Epi-On crosslinking of corneal collagen: Ultrastructural analysis by
Corneal Collagen Cross-Linking in Keratokonus Patients: Heidelberg retinal tomograph II in vivo confocal microscopy in
A Comparative Study through 2-Year Follow-Up. J. Ophthalmol. humans. Cornea. 2007; 26(4): 390–397.
2018; 2018: 1–6. Publisher Full Text
PubMed Abstract|Publisher Full Text|Free Full Text 28. Sitorasmi PH, Ningtiyas YS, Wahyuni I, et al.: Data CCT and IOP.
15. Antonios R, Fattah MA, Maalouf F, et al.: Central Corneal Thickness Dataset. Figshare.
after Cross-linking Using High-Definition Optical Coherence Publisher Full Text
Tomography, Ultrasound, and Dual Scheimpflug Tomography: 29. Sitorasmi PH, Ningtiyas YS, Wahyuni I, et al.: ARRIVE Checklist.
A Comparative Study over One Year. Am. J. Ophthalmol. 2016; 167: Dataset. Figshare.
Publisher Full Text
Page 7 of 8F1000Research 2023, 12:48 Last updated: 05 MAR 2024
The benefits of publishing with F1000Research:
• Your article is published within days, with no editorial bias
• You can publish traditional articles, null/negative results, case reports, data notes and more
• The peer review process is transparent and collaborative
• Your article is indexed in PubMed after passing peer review
• Dedicated customer support at every stage
For pre-submission enquiries, contact research@f1000.com
Page 8 of 8You can also read

















































