Quelles sont les limites du don d'organes après décès circulatoire en 2023? - Pr Olivier Detry - ORBi
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Quelles sont les limites du don d’organes
après décès circulatoire en 2023?
Pr Olivier Detry
Chargé de Cours, Université de Liège
Service de Chirurgie Abdominale et Transplantation
CHU Liège, Belgique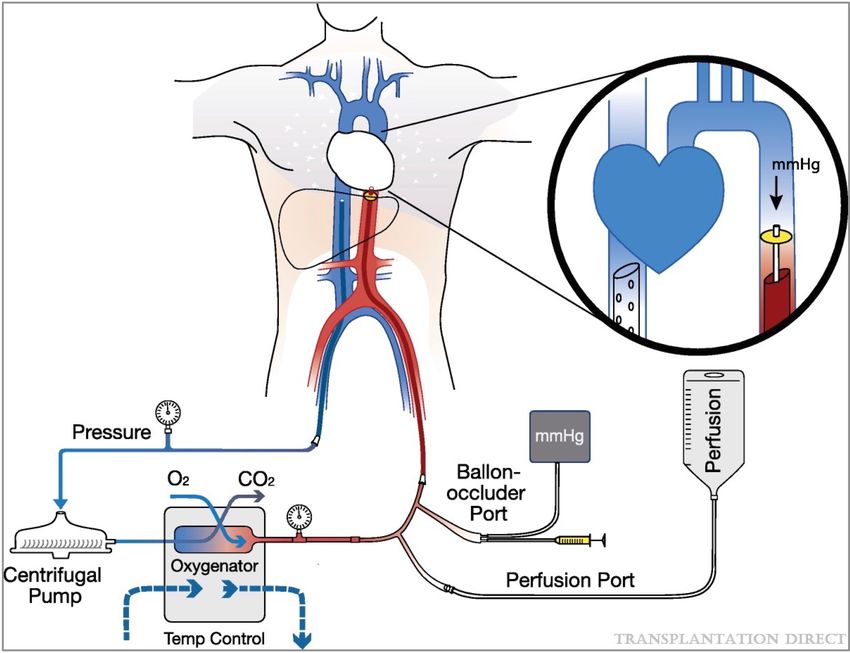
Plan de la présentation •Conflits d’intérêts •Limites médicales •Limites financières •Limites « politiques »

Active waiting list (at year-end) in Belgium, by year, by organ
Active waiting list 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
kidney 791 770 878 871 797 849 824 914 952 1108
heart 76 95 89 118 117 103 111 91 110 111
lung 81 85 82 104 122 143 143 163 106 106
liver 181 184 187 188 174 201 189 172 181 193
pancreas 54 60 70 68 65 61 57 51 48 45
Conflits
Total patients 1138 1141 1248 1288 1217 1292 1269 1341 1350 1514
statistics.eurotransplant.org : 3022P_Belgium : 23.05.2022 : patients waiting for multiple organs are counted for each organ
d’intérêt Waiting list mortality in Belgium, by year, by organ
2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
kidney 30 28 27 44 35 37 36 32 37 34
heart 16 23 19 13 20 18 8 17 10 9
lung 11 16 11 1 7 10 8 7 11 11
liver 52 30 44 63 45 43 35 40 42 38
pancreas 2 4 4 2 4 2 1 2
Total events 109 99 105 125 109 112 89 97 100 94
Total patients 100 95 96 116 101 103 85 94 95 89
statistics.eurotransplant.org : 4512P_Belgium : 23.05.2022 : Reported by year of death. Includes patients with active or
non-active urgency at removal. Includes removals while waiting for living or deceased donor transplants.
DCD: Classification Maastricht – Liège III - V
n Catégorie I: Constat de décès à l’arrivée des secours
n Catégorie II: Réanimation sans succès
n Catégorie III: Retrait des thérapeutiques de support
n Catégorie IV: Arrêt cardiaque chez un patient en
mort cérébrale
Kootstra et al. Transpl Proc, 1995
n Catégorie V: Euthanasie Detry et al. Transpl Proc 2012
DCD contrôlés:
ischémie chaude de prélèvement (pWI)
Arrêt des soins Arrêt Perfusion
Décès
Salle d’opération circulatoire Aortique
5 min Chirurgie
Phase d’arrêt des soins Phase acirculatoire
Arterial pressure < 60, 50, 35mmHg ?
pO2 < 70, 65, 35% ?
DCD contrôlés • Rein: augmentation de DGF et de PNF • Foie: augmentation de EAD, de PNF et de lésions biliaires ischémiques • Pancréas: ? • Poumon: OK • Cœur: ?

Expérience de DCD au CHU de Liège • Limiter les lésions ischémiques (pWI
Limites de DCD au CHU de Liège

Age des donneurs entre 1990 & 2021
42% older 60+
Note number of donors: 1994: 230 vs 2021: 280
nostic factor in DBD liver transplantation6 . Aged
s have less regenerative capacity7 and are more
Original article
eptible to ischaemia–reperfusion injury8 and hepatitis
rus (HCV) 9,10 .
Donor reinfection
age as a risk after liverintransplantation
factor donation after circulatory death
pite these facts, there is noin absolute
liver transplantation limitwithdrawal
a controlled of donor protocol
programme
for DBD liver transplantation11,12 . In DCD liver
splantation, donor age above 50 years has been
O. Detry1 , A. Deroover1 , N. Meurisse1 , M. F. Hans1 , J. Delwaide2 , S. Lauwick3 , A. Kaba3 , J. Joris3 ,
tifiedM.asMeurisse
an additional
1
and P. Honorérisk 1
factor for graft loss in
1 2 3
icentre series such asof Liège,
thatLiège,ofBelgium
the United Network for
Departments of Abdominal Surgery and Transplantation, Hepato-Gastroenterology and Anaesthesiology and Intensive Care, Centre Hospitalier
Universitaire de Liège, University
Correspondence to: Professor O. Detry, Department of Abdominal Surgery and Transplantation, CHU Liège, Sart Tilman B35, B4000 Liège, Belgium
(e-mail: olivier.detry@transplantation.be)
BJS 2014; 101: 784–792
Background: Results of donation after circulatory death (DCD) liver transplantation are impaired by
graft loss, resulting mainly from non-anastomotic biliary stricture. Donor age is a risk factor in deceased
donor liver transplantation, and particularly in DCD liver transplantation. At the authors’ institute, age
is not an absolute exclusion criterion for discarding DCD liver grafts, DCD donors receive comfort Donation after circulatory death liver transplantation
Donation after circulatory death liver transplantation
therapy before withdrawal, and cold ischaemia is minimized.
Methods: All consecutive DCD liver transplantations performed from 2003 to 2012 were studied 100
100
retrospectively. Three age groups were compared in terms of donor and recipient demographics, 90
90
procurement and transplantation conditions, peak laboratory values during the first post-transplant 72 h, 80
80
and results at 1 and 3 years. 70
Graft survival (%)
70
Results: A total of 70 DCD liver transplants were performed, including 32 liver grafts from donors 60
Survival (%)
60 50
aged 55 years or less, 20 aged 56–69 years, and 18 aged 70 years or more. The overall graft survival ≤ 55 years
50 40 56–69 years
Patient survival
rate at 1 month, 1 and 3 years was 99, 91 and 72 per cent respectively, with no graft lost secondary to ≥ 70 years
40 Graft survival 30
non-anastomotic stricture. No difference other than age was noted between the three groups for donor 20
30
or recipient characteristics, or procurement 20
conditions. No primary non-function occurred, but one 10
patient needed retransplantation for10artery thrombosis. Biliary complications were similar in the three
0 12 24 36
groups. Graft and patient survival rates were no different at 1 and 3 years between the three groups Time after transplant (months)
0 12 24 36
(P = 0·605). No. at risk
Time after transplant (months)
Conclusion: Results for DCD liver transplantation from younger and older donors were similar. Donor ≤ 55 years 32 31 22 12
age above 50 years should No. notat risk
be a contraindication to DCD liver transplantation if other donor risk 56–69 years 20 18 13 9
Patients 69 64 43 27 ≥ 70 years 18 17 10 8
factors (such as warm and cold ischaemia
Grafts 70 time) are minimized.
64 43 27
Kaplan–Meier curves comparing survival of grafts from the three donor age groups: 55 years or less, 56–69 years, and 70 years or
Fig. 3
Presented to the
Fig. 1European Society
Overall survival for Organ
for recipients Transplantation
and grafts in the donation after(ESOT)
circulatory2013 Congress, Vienna, Austria,
death cohort more. P = 0·605 (log rank test)
September 2013 Table 4 Characteristics for procurement and transplantation of donation after circulatory death grafts
patients (recurrence of pretransplant cancer, 7; unrelated bilirubin, and rate of primary non-function and hepatic
Donor group
Paper accepted 5 February
cancer, 2014
5) and miscellaneous in five. Overall graft survival artery thrombosis were similar for the three groups.
≤ 55 years 56–69 years ≥ 70 years
ratesin
Published online were 99, 91Online
Wiley and 72 per cent at(www.bjs.co.uk).
Library 1 month, 1 and 3 years Excluding the patient with arterial thrombosis after
DOI: 10.1002/bjs.9488 (n = 32) (n = 20) (n = 18) P†Successful heart transplantation from donation after
euthanasia with distant procurement using normothermic
1 | I NTRO D U C TI
regional O N and cold storage
perfusion To date, DCD he
16006143, 0, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/ajt.17204 by Thirion Paul - Dge, Wiley Online Library on [24/10/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Onli
Received: 27 June 2022 | Revised: 12 September 2022 | Accepted: 14 September 2022
Maastricht donor
DOI: 10.1111/ajt.17204
AJT
CASE REPORT
1 2 3 4
Vincent Tchana-
Transplantation of hearts donated Sato | Gregory
after Hans | Janne
circulatory Brouckaert
death (DCD)| Olivier Detry
V |
Maastricht don
Johan Van Cleemput5 | Steffen Rex6 | Oceane Jaquet2 | Erwin De Troy7 |
Successful heart transplantation from donation
has emerged a after
asMai- valuable strategy to expand pool.6 1 | Isabelle
Linh Nguyen Trung 8
| Arnaud Ancion8 |the
Raf donor
Van den Eynde organ donation
Lievens 9
| f
euthanasia with distant procurement using normothermic
Marc Gilbert Lagny1 | Marie-Hélène Delbouille4 | Jean Olivier Defraigne1 |
regional perfusion and cold storage
Abbreviations: ACR, acute Ledoux10
Didiercellular rejection; Rega3cardiopulmonary bypass; CS, cold storage; DCD, donation after circu
| Filip CPB,
Vincent Tchana-Sato1 assist
| Gregory Hans 2
| device; POD, 3postoperative
Janne Brouckaert | Olivier Detry4 day; | SR, sinus rhythm; TA-NRP, thoraco-abdominal normothermic regional perfusion
5 6 2 7
Johan Van Cleemput | Steffen Rex | Oceane Jaquet | Erwin 1 De Troy
Department of |Cardiovascular Surgery,
Vincent Tchana- Sato and
Mai-Linh Nguyen Trung | Arnaud Ancion | Raf Van den Eynde6 | Liege,
8 8 CHU,
Gregory
Isabelle
Hans contributed
Lievens9 |
Belgium
equally
While to this
euthanasia work.
has been legalized in a growing number of countries, organ donation
Marc Gilbert Lagny1 | Marie-HélèneDidier Ledoux
4
| Jeanand Filip Rega1ofshare the senior authorship of thisis work.
after euthanasia only performed in Belgium, the Netherlands, Spain, and Canada.
2
Delbouille Olivier Department
Defraigne |Anesthesiology, CHU,
Liege, Belgium
Didier Ledoux10 | Filip Rega3 3
Moreover, the clinical practice of heart donation after euthanasia has never been re-
Department of Cardiac Surgery,
1
© 2022 The American Society of Transplantation andWethe
ported before. American
describe Society
the first case
University Hospitals, Leuven, Belgium of a heart of Transplant
donated Surgeons.
after euthanasia, recon-
Department of Cardiovascular Surgery, 4
Department
While euthanasia has been legalized in a growing number of Abdominal
of countries, Surgery and
organ donation
ditioned with thoraco-abdominal normothermic regional perfusion, preserved using
CHU, Liege, Belgium
Transplantation, CHU, Liege, Belgium
2
Department of Anesthesiology, CHU, after euthanasia is only performed in Belgium, the Netherlands, Spain, and Canada. cold storage while being transported to a neighboring transplant center, and then suc-
5
Am J Transplant. 2022;00:1–4.
Moreover, the clinical practice of heart donation Department of Cardiology, University
Liege, Belgium
after euthanasia has never been re-
3
Department of Cardiac Surgery, Hospitals, Leuven, Belgium cessfully transplanted following a procurement warm ischemic time of 17 min. Heart
University Hospitals, Leuven, Belgium ported before. We describe the first case of a heart donated after euthanasia, recon-
4
6
Department
ditioned with thoraco-abdominal normothermic regional of Anesthesiology,
perfusion, preserved using
donation after euthanasia using thoraco-abdominal normothermic regional perfusion
Department of Abdominal Surgery and
University Hospitals, Leuven, Belgium
Transplantation, CHU, Liege, Belgium
cold storage while being transported to a neighboring transplant center, and then suc- is feasible, it could expand the heart donor pool and reduce waiting lists in countries
5 7
Department of Cardiology, University Department
Hospitals, Leuven, Belgium cessfully transplanted following a procurement warm ischemicoftime
Intensive CareHeart
of 17 min. Medicine,
where organ donation after euthanasia can be performed.
University Hospitals, Leuven, Belgium
6
Department of Anesthesiology, donation after euthanasia using thoraco-abdominal normothermic regional perfusion
8
University Hospitals, Leuven, Belgium Department
is feasible, it could expand the heart donor pool and of Cardiology,
reduce waiting CHU, Liege,
lists in countries
7
Department of Intensive Care Medicine, Belgium KEYWORDS
University Hospitals, Leuven, Belgium
where organ donation after euthanasia can be performed. cardiology, cardiovascular disease, clinical researchpractice, donors and donation: deceased,
9
Department of Neurology, CHU, Liege,
8
Department of Cardiology, CHU, Liege, donors and donation: donation after circulatory death (DCD), ethics, ethics and public policy,
Belgium KEYWORDS Belgium
9 cardiology, cardiovascular disease, clinical researchpractice,
10 donors and donation: deceased, heart transplantation, organ procurement, organ procurement and allocation
Department of Neurology, CHU, Liege, Department of Intensive Care Medicine,
donors and donation: donation after circulatory death (DCD), ethics, ethics and public policy,
Belgium
CHU, Liege,
heart transplantation, organ procurement, organ procurement Belgium
and allocation
10
Department of Intensive Care Medicine,
CHU, Liege, Belgium
Correspondence
Correspondence Vincent Tchana-Sato, Department ofnew england
The defined by the rate of the decrease in the serum creatinine n e wlevel,
e ng l aprimary nol
n d j o u r na The
The new england
journal tion, the serum creatinine level and clearance, acute rejection, toxicity of the ca
of medicine
journal established in 1812
of medicinerin inhibitor, the length of hospital stay, and allograft and patient survival.
january 1, 2009 vol. 360
in delaye
no. 1 perfusio 100 Machine-perfusion group
january 1, 2009 90 survival.
established in 1812 vol. 360 no. 1 Cold-storage group
RESULTS The n
Machine Perfusion or Cold Storage 80
tion was
in Deceased-Donor
Machine Perfusion or Cold Storage Kidney Transplantation Machine perfusion significantly reduced the risk of delayed graft function. 70
group D as
Graft Survival (%)
inFrankDeceased-Donor Kidney Transplantation van der Heide,function
van Gelder, Bogdan P. Napieralski, Margitta van Kasterop-Kutz, Jaap J. Homan graft
Cyril Moers, M.D., Jacqueline M. Smits, M.D., Ph.D., Mark-Hugo J. Maathuis, M.D., Ph.D., Jürgen Treckmann, M.D.,
M.D., Ph.D., developed in 70 patients 60
in the machine-perfusion group However
versu
Jean-Paul Squifflet, M.D., Ph.D., Ernest van Heurn, M.D., Ph.D., Günter R. Kirste, M.D., Ph.D., 50 nificant,
van der Heide,the cold-storage group (adjusted odds ratio, 0.57; P = 0.01). Machine perfusio
Cyril Moers, M.D., Jacqueline M. Smits, M.D., Ph.D., Mark-Hugo J. Maathuis, M.D., Ph.D., Jürgen Treckmann, M.D.,
Axel Rahmel, M.D., Ph.D., Henri G.D. Leuvenink, Ph.D., Andreas Paul, M.D., Ph.D., Jacques
Frank van Gelder, Bogdan P. Napieralski, Margitta van Kasterop-Kutz, and Rutger J. Ploeg, Jaap J.M.D.,
Homan Ph.D.*
Pirenne,
M.D., Ph.D.,
M.D., Ph.D., all incide
40
Jean-Paul Squifflet, M.D., Ph.D., Ernest van Heurn, M.D., Ph.D., Günter R. Kirste, M.D., Ph.D., characte
Axel Rahmel, M.D., Ph.D., Henri G.D. Leuvenink, Ph.D., Andreas Paul, M.D., Ph.D., Jacques Pirenne,significantly M.D., Ph.D., improved the rate of the 30 decrease in the serum creatinine lev
and Rutger J. Ploeg, M.D., APh.D.* BS T R AC T lowed to
reduced the duration of delayed graft20 function. Machine perfusion waskidneys asso
BACKGROUND
though e
Static cold storage is generally usedAto BSpreserve
with
T R AC Tkidney allografts from deceased do- From the Department of Surgery (C.M.,
nors. Hypothermic machine perfusion may improve outcomes after transplantation, M.-H.J.M., H.G.D.L.,
lower
R.J.P.) and the
serum
De-
creatinine levels during
10 the first 2 weeks after transplan
ables, as
and a reduced risk of graft failure (hazard 2 ratio, 50.52; 7 P 8= 0.03).
9 10 11One-year mightal
partment of Nephrology (J.J.H.H.), Univer-
BACKGROUND but few sufficiently powered prospective studies have addressed this possibility. 0
Static cold storage is generally used to preserve kidney allografts from deceased do- From the Department
sity Medical Center Groningen, University
of Groningen,
of SurgeryGroningen;
(C.M., the Eurotrans- 0 1 3 4 6 12 fu
METHODS plant International Foundation, Leiden
fusion o
survival was Maas- superior in the machine-perfusion group (94% vs. 90%, P = 0.0
nors. Hypothermic machine perfusion may improve outcomes after transplantation, M.-H.J.M., H.G.D.L., R.J.P.) and the De-
partment (J.M.S.,
of Nephrology M.K.-K.,Univer-
(J.J.H.H.), A.R.); and the Depart- Months since Transplantation
but few sufficientlyIn this international
powered prospective randomized,
studies have controlled
addressed trial,this
we possibility.
randomly assigned one kidney
from 336 consecutive deceased donors to machine perfusion and the of other
ment of Surgery, University Hospital
sity Medical Center Groningen, University
to cold tricht, Maastricht (E.H.) — all in the No. at Risk
In co
significant differences were observed for the other secondary end points. No s
Groningen, Groningen; the Eurotrans-
storage. All 672 recipients were followed for 1 year. The primary end point was de- Netherlands; the Department of General,
METHODS
layed graft function (requiring dialysis in the first week after transplantation).
plant International
Sec- A.R.);
(J.M.S., M.K.-K.,
Foundation,
Visceral, Leiden
and Transplantation
and the Depart-
Surgery, Machine-perfusion 336 323 322 319 317 315 314 314 312 311 310 309 309 hypothe
In this international randomized, controlled trial, we randomly assigned one kidney ment of Surgery, University University Hospital Essen, Essen ( J.T.,
group
cidence
adverse events were directly attributable to machine perfusion.
ondary end points were the duration of delayed graft function, delayed graft function B.P.N., A.P.); Hospital
andMaas-
Deutsche Stiftung Or-
from 336 consecutive deceased
defined by thedonors
rate oftothemachine
decreaseperfusion
in the serum andcreatinine
the otherlevel,
to cold tricht, Maastricht gantransplantation,
primary nonfunc- (E.H.) — all in Frankfurt
the (G.R.K.) — Cold-storage group 336 318 313 308 304 304 304 303 302 302 299 299 296
storage. All 672 recipients
tion, thewere
serum followed
creatinineforlevel
1 year.
and The primary
clearance, acuteend point was
rejection,
Netherlands; the Department of General,
de- of the calcineu- both in Germany; and the Department of
toxicity Visceral, and Transplantation Surgery,Surgery — Trans-
Abdominal Transplant
obtained
layed graft functionrin(requiring
inhibitor,dialysis in the first week after
andtransplantation). Sec-survival.
the length of hospital stay, allograft and patient
ondary end points were the duration of delayed graft function, delayed graft function B.P.N., A.P.); and Deutsche
University Hospital Essen,
plant
Leuven, Leuven
Essen (J.T.,
Coordination,
Stiftung
University Hospital
Or-J.P.); and the De-
(F.G.,
Figure 3. Graft Survival after Transplantation. ceased d
defined by the rate RESULTS
of the decrease in the serum creatinine level, primary nonfunc- gantransplantation,
both in Germany; and CONCLUSIONS
partment
Frankfurt
plantation,
of (G.R.K.)
Abdominal — Surgery and Trans-
Centre Hospitalier
the Department of Universi-
The rate of graft survival at 1 year
AUTHOR: Moers
in the machine-perfusion
RETAKE
group
1st
was sig- duced th
tion, the serum creatinine level and clearance, acutereduced
rejection,thetoxicity
risk of of the calcineu- nificantly higherICMthan the rate in the cold-storage group (94% vs. 90%,
Machine
rin inhibitor, the length
perfusion
of hospital
significantly
stay, and allograft
patientsand patient
delayed
survival.
graft function. Delayed
Abdominal taire Surgery
Transplant
89 in Liège,
Sart Tilman, and the University of
— Trans-
Liège (J.-P.S.) — both in Belgium. FIGURE: 3 of 3 2nd it occurr
theHypothermic machine perfusion was associated with a reduced risk of delaye
graft function developed in 70 in the machine-perfusion groupplant
versusCoordination, University Hospital
P = 0.04). Data REG
on Fgraft survival were censored at the time of death in pa-
the cold-storage group (adjusted odds ratio, 0.57; P = 0.01). Machine perfusion Leuven, Leuven Address
also (F.G.,
reprint requests
J.P.); and the De- to Dr. Moers
University Medical Center Groningen,
at 3rd
a lower
RESULTS significantly improved the rate of the decrease in the serum creatinine
partment of Abdominal Surgery and Trans-
level and Department of Surgery, CMC V, Y2.144, tients who died with a functioning allograft.
CASE Revised
ter tran
function and improved graft survival in the tsfirstH/T year
Line
after
4-C
transplantation. (C
plantation, Centre Hospitalier Universi-
reduced the duration
Machine perfusion significantly reducedofthe delayed
risk ofgraft function.
delayed graft Machine
function.perfusion
Delayed was taireassociated
Sart Tilman, and
Hanzeplein 1, 9713 GZ Groningen, the
the University of EMail SIZE
Netherlands, or at c.moers@chir.umcg.nl. ARTIST:
with lower serum creatinine levels during the
graft function developed in 70 patients in the machine-perfusion group versus 89 in first 2 weeks after transplantation
Liège, Liège (J.-P.S.) — both in Belgium.
Enon
H/T 22p3 neys sho
Controlled Trials number, ISRCTN83876362.)
and (adjusted
a reducedodds risk of graft0.57;
failure Address reprint requests to Dr. Moers at Combo
the cold-storage group ratio, P = (hazard ratio, 0.52;
0.01). Machine P = 0.03).also
perfusion One-year allograft *Trial investigators are listed in the Ap-
significantly improvedsurvival
the was
ratesuperior in the machine-perfusion
of the decrease in the serum creatininegroup (94% levelvs.and
the University Medical
90%,Department
P = 0.04). No
Center Groningen,
pendix.
of Surgery, CMC V, Y2.144,
Nevertheless, there is a higher incidence of de- as comp
AUTHOR, PLEASE NOTE:
significant differences were observed for the other secondary end
reduced the duration of delayed graft function. Machine perfusion was associated Hanzeplein 1, 9713N Engl
adverse events were directly attributable to machine perfusion.
points. No serious GZ Groningen, the
J Med 2009;360:7-19.
Netherlands, or at c.moers@chir.umcg.nl.
Copyright © 2009 Massachusetts Medical Society.
layed
Figure graft
has function
been redrawn among
and type recipients
has been reset. of kidneys cold sto
with lower serum creatinine levels during the first 2 weeks after transplantation Please check carefully.
and a reduced risk CONCLUSIONS
of graft failure (hazard ratio, 0.52; P = 0.03). One-year allograft *Trial investigators are listed in the Ap-
donated after cardiocirculatory death and with
survival was superior in the machine-perfusion group (94% vs. 90%, pendix. n engl j med 360;1 nejm.org
expanded-criteria january
31 Hence,
donation.ISSUE: the 1, 2009
absolute Support
Hypothermic machine perfusion was associated with aPreduced
= 0.04).risk
No of delayed graft
JOB: 36001 01-01-09 Drs. Ma
significant differences were observed for the other secondary end points. Notransplantation.
serious N Engl(Current
function
adverse events wereControlled
and improved
directly attributable
graft
to
survival
machine
in the first
perfusion.
year after J Med 2009;360:7-19. number of patients who would actually benefit Mr. van Ge
Trials number, ISRCTN83876362.) Copyright © 2009 Massachusetts Medical Society.
from The New perfusion
machine Englandmight Journal of Medicine
be larger in these congress tr
CONCLUSIONS n engl j med 360;1 nejm.org january 1, 2009 7 receiving atio for graft failure in the machine-perfusion group of 0.60 tion, the survival of kidneys donated after brain delayed graft function, as compared with cold- only, we decide
dence interval, 0.37 to 0.97; P = 0.04). Panel B shows the post see whether th
s of a subgroup of 588 recipients of kidneys donated after brain
death remained significantly better after machine
A tage would pe
data split according to whether delayed graft function devel- perfusion than after cold-storage preservation,
100
Machine perfusion
In our stud
T h e n e w e ng l a n d j o u r na l o f m e dic i n e randomly assig
recipient. Delayed graft function was defined as the need for especially in kidneys recovered from expanded- 90
80
Cold storage contralateral o
he first week after transplantation. criteria donors. Delayed graft function was asso- For the presen
Machine Perfusion or Cold Storage in Deceased-Donor 70
laborating tra
ciated with a notably lower rate of graft survival
Graft Survival (%)
3-year follow-
Kidney Transplantation 60
consecutive ki
50
after cardiocir
To the Editor: In 2009, we reported the results storage preservation. We also observed that graft 40
set, as well as
of an international randomized, controlled trial in survival at 1 year was significantly better after 30 after cardioci
n engl j med 366;8 nejm.org february 23, 2012
which hypothermic machine perfusion of deceased- machine perfusion.1 Since preservation-related ef- 20 data set. End
donor kidneys significantly reduced the risk of fects have been shown to affect early function patient surviva
delayed graft function, as compared with The cold-New England Journal
only, we decided of Medicine
to extend the follow-up period to
10
performed stat
Downloaded from nejm.org by OLIVIER DETRY on September see whether7, the2022. For personal
substantial useadvan-
graft-survival only. No other uses without permission. 0 that were repo
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
A Copyright © 2012 Massachusetts tage wouldMedical
persist 3 years after transplantation.
Society. All rights reserved. Overall, 3-
Months since Transplantation
100 In our study, one kidney of each donor was machine-perfu
Machine perfusion
90 randomly assigned to machine perfusion, and the B hazard ratio fo
80
Cold storage contralateral organ was assigned to cold storage. 100 Machine perfusion and no delayed graft function 1A). Three-yea
For the present analysis, we contacted all 60 col- fusion was als
70 90 Cold storage and no delayed graft function
laborating transplantation centers. We collected age for kidney
Graft Survival (%)
80
60 3-year follow-up data from all 672 recipients of vs. 86%; adjus
Machine perfusion and delayed graft function
50 consecutive kidneys donated after brain death or 70 not for kidney
Graft Survival (%)
after cardiocirculatory death in the main data 60 The 3-year gra
40 Cold storage and delayed graft function
set, as well as 164 recipients of kidneys donated perfusion was
50
30 after cardiocirculatory death in the extended covered from
20 data set. End points were 3-year graft survival, 40
for donation2
10
patient survival, and serum creatinine level. We 30 tio, 0.38; P = 0
performed statistical analyses using the methods 20 mentary Appe
0 1
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 that were reported previously. this letter at N
10
Months since Transplantation Overall, 3-year graft survival was better for had a profoun
machine-perfused kidneys (91% vs. 87%; adjusted 0 neys donated
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
B hazard ratio for graft failure, 0.60; P = 0.04) (Fig. were no signif
Months since Transplantation
100 Machine perfusion and no delayed graft function 1A). Three-year graft survival after machine per- the rate of sur
90 Cold storage and no delayed graft function
fusion was also superior to that after cold stor- Figure 1. Graft Survival of Deceased-Donor Kidneys at 3 Years. nine levels at
age for kidneys donated after brain death (91% Panel A shows graft survival in 672 recipients in the main data set, with We conclud
80
Machine perfusion and delayed graft function
vs. 86%; adjusted hazard ratio, 0.54; P = 0.02) but a hazard ratio for graft failure in the machine-perfusion group of 0.60 tion, the survi
70 not for kidneys donated after circulatory death. (95% confidence interval, 0.37 to 0.97; P = 0.04). Panel B shows the post
death remaine
Graft Survival (%)
hoc analysis of a subgroup of 588 recipients of kidneys donated after brain
60 Cold storage and delayed graft function
The 3-year graft-survival advantage after machine death, with data split according to whether delayed graft function devel- perfusion tha
50
perfusion was most pronounced for kidneys re- oped in the recipient. Delayed graft function was defined as the need for especially in k
covered from donors who had expanded criteria dialysis in the first week after transplantation. criteria donors
40
for donation2 (86% vs. 76%; adjusted hazard ra- ciated with a n
30 tio, 0.38; P = 0.01) (see the figures in the Supple-4 Department of Abdominal Transplant Surgery – Transplant Coordination, University Hospital Leuven, Belgium
5 Transplant
Department International
of Nephrology, ISSN
University 0934-0874
Medical Center Groningen, University of Groningen, The Netherlands
6 Department of Abdominal Surgery and Transplantation, CHU Sart Tilman, University of Liège, Belgium
7 Department of Surgery, University Hospital Maastricht, The Netherlands Machine perfusion for ECD kidneys
E 8 Deutsche Stiftung Organtransplantation, Frankfurt, Germany
Transplant International ISSN 0934-0874
fusion versus cold storage for preservation of (a)
100
Table 4. C
1 year graft
m expanded
O R I G I N A L criteria
A R T I C L E donors after brain death 95
90
Cyril Moers,2 Jacqueline M. Smits,3 Anja Gallinat,1 Mark-Hugo J. Maathuis,2
op-Kutz,3Machine
Ina Jochmans,perfusion versus cold storage for preservation of
4 5 6 85 Treatment a
Jaap J. Homan van der Heide,
Keywords Jean-Paul Squifflet, CIT
ünter R.kidneys 8
Kirste, Axel from 3
Rahmel, expanded
Henri G. D.donation,
Leuvenink, 2
expandedJacques
donor pool,Pirenne,
4 Summary 80
criteria donors
kidney,
after brain death HLA MM
Andreas Paul1 75
%
organ preservation and procurement, Recent PRA
1 2 outcome. 3 The
1 purpose of this study was to 2 analyze the possible effects of machine perfu-
Jürgen Treckmann, Cyril Moers, Jacqueline M. Smits, Anja Gallinat, sionMark-Hugo
(MP) versus J.cold
Maathuis,
storage (CS) 70 Recipient ag
and Transplantation Surgery, University Hospital Essen,3 Germany 4 5 6 on delayed graft function (DGF) and early
Margitta van Kasterop-Kutz, Ina Jochmans, CorrespondenceJaap J. Homan van dergraft Heide, Jean-Paul
survival in expandedSquifflet,
criteria donor kidneys (ECD). As part of the previ- 65 Donor age
versity Medical Center Groningen, University of Groningen, The 8Netherlands
Ernest van Heurn,7 Günter R. Kirste,
Foundation, Leiden, The Netherlands
Axel
Andreas Paul Rahmel,
3
MD, PhD, ClinicHenri G. Visceral
for General, D. Leuvenink,ously
2
Jacques
reported
4
Pirenne,randomized
international controlled trial 91 consecutive heart- 60
First/re-tran
2 1 MP [n = 91] Duration of
Rutger
Transplant Surgery J. Ploeg
– Transplant and Andreas
Coordination, UniversityPaul
and Transplantation Surgery, University Hospital
Hospital Leuven, Belgium beating deceased ECDs – defined according to the United Network of Organ 55
Essen, Hufelandstraße 55, D-45122 Essen, CS [n = 91]
University Medical Center Groningen, University of Groningen, The Netherlands Sharing definition – were included in the study. From each donor one kidney 50 CIT, cold i
1 Clinic for General, Visceral and TransplantationGermany.
Surgery, Tel.:
University Hospital
+49 201 Essen,
723 1100; fax:Germany
+49 201
Surgery and Transplantation, CHU Sart Tilman, University of Liège, Belgium 0 1 2 3 4 5 6 7 8 9 10 11 12 MM, misma
2 Department of Surgery, University Medical Center Groningen, University of Groningen,
723 5946; e-mail: andreas.paul@uk-essen.de The was randomized to MP and the contralateral kidney to CS. All recipients were
Netherlands
versity Hospital Maastricht, The Netherlands Post-transplant time (months)
3 Eurotransplant International Foundation, Leiden, The Netherlands followed for 1 year. The primary endpoint was DGF. Secondary endpoints
nsplantation, Frankfurt, Germany (b)
4 Department of Abdominal Transplant Surgery –Conflicts
Transplant Coordination, University Hospital Leuven,
of Interest Belgiumprimary nonfunction and graft survival. DGF occurred in 27 patients
included 100 compariso
5 Department of Nephrology, University Medical Drs.Center Groningen,
Maathuis, Moers,University
Paul, andofLeuvenink
Groningen,and The Netherlands
in the CS group (29.7%) and in 20 patients in the MP group (22%). Using the
6 Department of Abdominal Surgery and Transplantation, CHU Sart Tilman,
Mrs. van Kasterop-Kutz reportUniversity
receiving of
oneLiège, Belgium 90 expanded
logistic regression model MP significantly reduced the risk of DGF compared
7 Department of Surgery, University Hospital Maastricht,
congress The Netherlands
travel grant from Organ Recovery that also
with CS (OR 0.460, P = 0.047). The incidence of nonfunction in the CS group 80
8 Deutsche Stiftung Organtransplantation, Frankfurt, Germany
Systems; Dr. Pirenne, receiving a research grant showed n
from the government of Flanders, Belgium, in (12%) was four times higher than in the MP group (3%) (P = 0.04). One-year 70 It is in
cooperation with Organ Recovery Systems to graft survival was significantly higher in machine perfused kidneys compared
60 of DGF in
ol, kidney, Summary study machine perfusion of liver grafts, for which with cold stored kidneys (92.3% vs. 80.2%, P = 0.02). In the present study,
he receives no salary; Dr. Ploeg, receiving 50
main dat
%
ement,
The purpose of this study was to consulting
analyze the possible effectsSquibb
of machine MP preservation clearly reduced the risk of DGF and improved 1-year graft
perfu-
fees from Bristol-Myers and The incid
sion (MP) versus cold storage (CS) grant
onsupport
delayed fromgraft
Nuts Ohra Trust; Dr.
function survival and function in ECD kidneys.
Moers,and early
(DGF) 40 than that
Keywords graft survival in expanded criteriareceiving donorgrant support from the Dutch Kidney MP and no DGF [n = 71]
Summary kidneys (ECD). As part of the previ- 30 One expl
donation, expanded donor pool, kidney,
r General, Visceral
ously reported international randomized
Foundation; Dr. Leuvenink, receiving grant
controlled trial 91 consecutive heart- (Current Controlled Trials number: ISRCTN83876362). MP and DGF [n = 20]
support from the Dutch Kidney Foundation and 20 cold ische
organ preservation and procurement,
versity Hospital
beating deceased ECDs – definedthe The purpose
according ofthethis
topro-donor
Eurotrans-Bio
study
United was to analyze the possible effects of machine perfu-
Network
project; and Drs. of Organ CS and no DGF [n = 64] The h
22 Essen, outcome. 10
Sharing definition – were included sion
in
Ploeg (MP)
the
and versus
study.
Leuvenink, Fromcoldeach
having a storage
donor
patent on (CS)
a one onkidney
delayed graft function (DGF) and early CS and DGF [n = 27] reduced f
00; fax: +49 201
Correspondence graft survival in expanded criteria donor kidneys (ECD). As part of the previ-
uk-essen.de was randomized to MP and the portable preservation
contralateral kidneyapparatus
to CS.forAll
donor
recipients were 0 study wit
Andreas Paul MD, PhD, Clinic for General, Visceral organs. No other potential conflict of interest
followed for 1 year. The primary ously reported
endpoint was international
DGF. randomized
Secondary endpointscontrolled trial 91 consecutive heart- 0 1 2 3 4 5 6 7 8 9 10 11 12
ECD kid
and Transplantation Surgery, University Hospital relevant to this article was reported. Post-transplant time (months)
included primary
Essen, Hufelandstraße 55, D-45122nonfunction
Essen, andbeating deceasedDGF
graft survival. ECDs – defined
occurred in 27according
patients to the United Network of Organ group com
Leuvenink and Received:
Sharing 9definition
May 2010 – were included in the study. From each donor one kidney
in the CS group (29.7%)
Germany. Tel.: +49 201 723 1100; fax: +49 201 and in 20 patients in the MP group (22%). Using the Figure 1 (a) Post-transplant graft survival rates. All consecutive renal ure, in ad
eceiving one Revision requested: 7 June 2010
723 5946;logistic regression model MP significantly
e-mail: andreas.paul@uk-essen.de was randomized
reduced to
theMP riskand
of the
DGF contralateral
compared kidney to CS. All recipients were transplants from heart beating (HB) expanded criteria donor (ECD) burden o
n Recovery Accepted: 17 January 2011
with CS (OR 0.460, P = 0.047). followed
The incidence for of1 nonfunction
year. The primary in the endpoint
CS group was DGF. Secondary endpoints N = 182. Logrank test of equality machine perfusion (MP) versus cold tation. T
research grant Published online: 17 February 2011
s, Belgium, in
Conflicts(12%)
of Interest
was four times higher than included
in the MP primary
group nonfunction
(3%) (P = and
0.04). graft survival.
One-year DGF occurred in 27 patients storage (CS) P = 0.02. (b) Post-transplant graft survival rates. All con- described
Drs. Maathuis, Moers, Paul, and Leuvenink and in theinCS group (29.7%) secutive renal transplants from HB ECD N = 182 – Logrank test of
y Systems to graft survival was significantly higher machine perfusedand
doi:10.1111/j.1432-2277.2011.01232.x in 20compared
kidneys patients in the MP group (22%). Using the For EC
Mrs. van Kasterop-Kutz report receiving one equality. Within CS group delayed graft function (DGF) versus no DGF
grafts, for which logistic regression model MP significantly reduced the risk of DGF compared
congress with coldfrom
travel grant stored
Organkidneys
Recovery (92.3% vs. 80.2%, P = 0.02). In the present study, P < 0.0001. Within MP group DGF versus no DGF P = 0.164. Within
post-tran
receiving withrisk
CS (OR 0.460, ª 2011 The Authors
MP preservation clearly reduced
Systems; Dr. Pirenne, receiving a research grant the of DGF andP improved
= 0.047). The incidence
1-year graft of nonfunction in the CS group
no DGF group MP versus CS P = 0.48. Within DGF group MP versus better if t
rs Squibb and 548 International ª 2011 European Society for Organ Transplantation 24 (2011) 548–554
from the survival
government and function
of Flanders, in ECD
Belgium, (12%) was four times higher than in the MP groupTransplant
in kidneys. (3%) (P = 0.04). One-year CS P = 0.003. CS. These
rust; Dr. Moers,
e Dutch Kidney
cooperation with Organ Recovery Systems to graft survival was significantly higher in machine perfused kidneys compared studies sh
study machine perfusion of liver grafts, for whichPerfusion des organes: questions?
• Hypothermie • Normothermie
- facilité - complexité
- peu de contrôle - contrôle de la fonction
- coût moins élevé - coût très élevé
- solution « simple » - solution sanguine
- sans ou avec oxygène - oxygène
- peu de besoins - substrats
- améliorationMachines de perfusion
• Hypothermiques
3.500€/rein
• Normothermiques
30.000€/organeCoût de la perfusion des organes
• DCD reins hypothermie : 7000€ /2 reins x 125/an = 875.000 €
• DCD foie hypothermie : 4000€ x 125/an= 500.000 €
• DCD foie normothermie: 30.000€ x 125/an= 3.750.000 €
• DCD poumon & cœurs en normothermie:
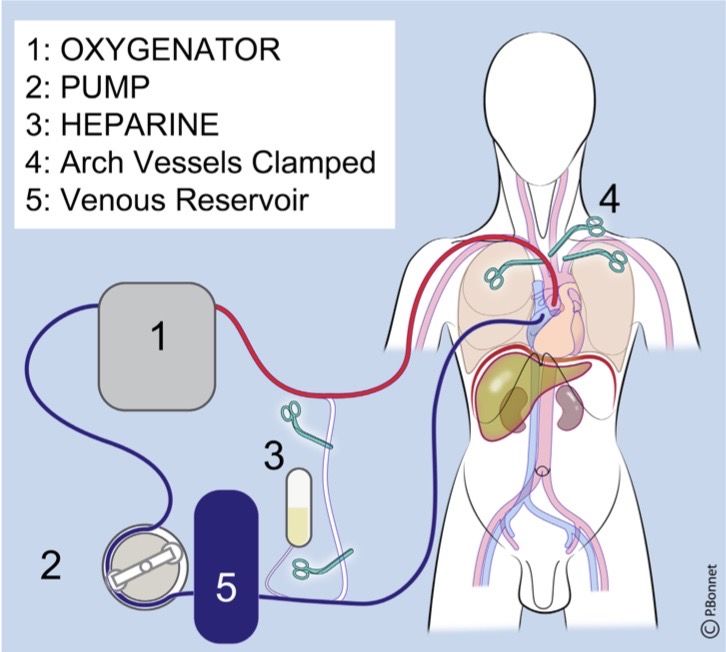
30.000€ x 100/an: 3.000.000 €Prélèvement multiorganes DCD - • Normothermic abdominal regional perfusion (N-ARP)
Prélèvement multiorganes DCD - • Normothermic thoraco - abdominal regional perfusion (N-TARP)
Le futur du DCD est chirurgical et passe par la perfusion régionale normothermique ! • Critères DCD = critères DBD • ECMO: 120 x 3.000€ : 360.000€ • Priorités au bloc opératoire pour réduire les ischémies pWI & CI • Equipes chirurgicales et infirmières expérimentées tant dans les équipes de greffe que les équipes de prélèvement • Mieux rénumérer les professionnels de la chaine de transplantation, de la détection du donneur à la sortie du patient receveur de l’hôpital
0.0
ACTUAL DONORS AFTER 0.7
CIRCULATORY DEATH 2.6
(DCD)
2021 0.0
0.0
0.0
0.0
0.0 1.5
0.0
1.6
8.3 10.1
0.0
0.0
11.6
0.0 1.2
0.0 0.0
1.0 0.0
3.4 0.0 0.0
6.6
0.0 0.0
0.0 0.0
0.0
0.0 0.0
1.5
1.7 0.0
14.2
0.0 0.0
0.0
0.0 SUDAN: 0.0
0.3
9Donneurs d’organes en Belgique • 2021: Belgique: 280 donneurs effectifs, 159 DBD & 121 DCD • 2021: Liège: 58 (20%) donneurs effectifs, 29 DBD (18%) & 29 DCD (24%) • Population Belge: 11.000.638 • Population Province de Liège: 1.082.136 • Taux de donneurs en Belgique: 25,4/million d’habitants • Taux de donneurs en Province de Liège: 53,6/million d’habitants
Limites du DCD? • Médicales: = DBD • Financières: ECMO et perfusion régionale du donneur • « Politique » - professionnaliser et motiver les équipes - donner la priorité aux prélèvements et aux transplantations - augmenter le nombre de prélèvements - informer de la possibilité de don d’organes après euthanasie
You can also read

















































