Robotic surgery in urology Thrombocytopenia in the emergency department Barriers to tobacco smoking in dental students Phenotypic mapping in ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

15 4
Oct-Dec 2019,
Platelets Blokage
Robotic surgery in urology
Thrombocytopenia in the
emergency department
Barriers to tobacco smoking
in dental students
Phenotypic mapping in
autism spectrum disorders

Amrita Journal of Medicine Vol. 15, No: 4
Oct-Dec 2019, Page 1 - 44
CONTENTS
2 Editorial Board en medical support system for the diagnosis and
Review Article management of autism spectrum disorders
3 A Sreeja, K P Vinayan
Role of robotic surgery in Urology - where we
stand. 26 Evaluation of the association between parenter-
Shivraj Barath Kumar, Abhishek Laddha , Appu Thomas, al Noradrenaline and arterial lactate levels in the
Ginil Kumar Pooleri critically ill patients with and without sepsis
Original Article Sruthi Haridas, M Gopalakrishna Pillai, Dhanasekharan
8 Immunization Coverage in a Rural Area of Malap- B S, Gireesh Kumar, Sreekrishnan T P , Sabarish B, Manu
puram District, Kerala: A Cross Sectional Study Sudhi, Renjitha Balakrishnan
Sreelakshmi Mohandas K, Vivin Vincent, Teena Mary joy, 31 To study the clinical profile of patients present-
Dulari Gupta ing with thrombocytopenia in the Emergency
13 Hyperosmolar 25% dextrose with 2% lignocaine Department.
injection for chronic plantar fasciitis treatment- A Vivek. U, Anoop. P, Sreekrishnan T.P, Dhanasekaran B.S,
prospective observational study from a tertiary Gireesh Kumar K.P
care centre, Kerala 35 Barriers to Tobacco Cessation Advice among Clini-
Abhishek.B, George Joseph, Sundaram KR , Remya Sude-
cal Dental Students: A cross-sectional study
van
16 Assessment of 1p19q chromosomal status in glio- R. Venkitachalam,Aishwariya R,Vinita Sanjeevan
mas by Fluorescence in situ hybridization at a ter- Case report
tiary care hospital 42 Pulmonary alveolar hemorrhage: A case report on
Priya Roys, Vidya Jha, M V Thampi rare complication of Ruxolitinib therapy in a mye-
21 Comprehensive phenotypic mapping is essential lofibrosis patient
for the development of an integrated data-driv- Sharon Ann Georgy, Neeraj Sidharthan, Remya Sudevan
1
Amrita
AmritaJournal
JournalofofMedicine
Medicine Vol. 15, No: 4
Oct-Dec 2019, Page 1 - 44
Editorial Board
Advisers
Dr. Prem Nair
Dr. Vishal Marwaha
Editorial Board Chairman
Dr. D M Vasudevan
Chief Editor
Dr. Harish Kumar
Associate Editors
Dr. Manu Raj
Dr. Sandeep Sreedharan
Dr. Unnikrishnan K Menon
Dr. Vijayakumar K
Editorial Board Members
Dr. Anupama R
Dr. Beena K V
Dr. Debnarayan Dutta
Dr. Gireesh Kumar K P
Dr. Hisham Ahammed
Dr. Meenakshi Dhar
Dr. P G Nair
Dr. Rakesh P S
Dr. Sundaram K R
Dr. Venkitachalom R
Administrator
Mrs. Gita Rajagopal
Site Link: http//www.amritahospital.org/amrita- journal
Copyright
Although every possible care has been taken to avoid any mistake and this publication is
being sold on condition and understanding that the information it contains are merely for
guidance and reference and must not be taken as having the complete authority. The Institu-
tion and The Editors do not owe any responsibility for any action taken on the basis of this pub-
lication. The copy rights on the material and its contents vests exclusively with the publisher.
Nobody can reproduce or copy the prints in any manner.
2
Amrita Journal of Medicine vol:15 , No:4
Oct-Dec 2019, Page 1-44
REVIEW ARTICLE
Role of robotic surgery in Urology - where we stand
Shivraj Barath Kumar*, Abhishek Laddha** , Appu Thomas** , Ginil Kumar Pooleri**
ABSTRACT
Urology as a subspecialty of surgery is always driven by rapid adaptation of technological advances, from open surgery to en-
doscopic surgery and laparoscopy. Arrival of robotic system marked a new era in urology. In this comprehensive systemic review
we analysed current status of robotic system in urology as well what we can expect in future. Robotic surgery is now widely use
in urologic oncology and reconstructive urology with excellent outcomes. High initial installation costs with high disposable cost
per surgery combined with lack on insurance are current reasons for slow progression of robotic surgery is India. Advent of new
systems may end monopoly and can bring down cost of robotic systems in future.
Keywords: Robotic surgery, robotic urology.
Corresponding Author: Ginil Kumar Pooleri, Professor, Department of Urology,AIMS ,Kochi.
INTRODUCTION per surgery are major hindrance for wider adaptation
What Hippocrates told to diagnose the diseases holds in the Indian subcontinent. With upcoming newer sys-
true for technology in medicine as well tems the cost of robotic surgery may go down making
“Declare the past, diagnose the present, and fore- it accessible to many parts in Indian subcontinent. In
tell the future.” future it may replace laparoscopic surgery with similar
We all know that the only one thing certain in universe costs and better outcomes for patients and comfort of
is “change”. Advent of robotic surgery marked a new era ergonomic position for surgeon. India is predicted to
in Robotic urology. As it provided better ergonomics, become second largest centre for robotic surgery center
optimal magnification of the operative field, surgeon in world after USA1.
dexterity, and precision of surgical manipulation, it over- The earliest form of Robot involved in a surgical proce-
came many difficulties associated with pure laparosco- dure goes back to 1985 when the PUMA 560 robotic arm
py. Robotic assisted prostatectomy and robot-assisted was used to perform a brain biopsy. Following which, in
partial nephrectomy have been widely considered as 1987, was used for cholecystectomy. The da Vinci (In-
minimally invasive alternatives to open surgery with tuitive Surgical Inc., Mountain View, CA, USA) got FDA
equivalent oncological and probably better function- approval in 2000 and at present there are around 80 da
al outcome. After success in above procedures robotic Vinci system working in India with over 1.7 million ro-
surgery is now commonly used in other genitourinary botic assisted procedure performed worldwide till now2.
diseases such as bladder cancer, upper tract urothelial Intuitive surgical is world leader in robotic surgical sys-
cancer, ureteropelvic junction obstruction, adrenal sur- tems for over 18 years and have grown by 237% over the
gery and reconstructive urology. Expanding evolving last 5 years as per ISRG’s stock report3. Historically they
indications for Robotic urologic surgery also focus on have updated systems every 4 to 6 years with da Vinci Si,
pelvic organ prolpase and Microsurgery in Male Infertil- X , Xi are common models currently in use in India . da
ity and Andrology. Vinci SP is recently launched in USA and initial reports of
METHODOLOGY successful adaptation in urology is coming up. da Vinci
A comprehensive literature search focusing on the has evolved as a comprehensive system with integrated
management of role of robotic surgery in urology was intraoperative ultrasonography (USG), infrared imaging
done. All articles in PUBMED, Medline, EMBASE and the with indocyanine green and energy sources such as ul-
Cochrane Libraries were reviewed. Final selection of ar- trasonic shears and tissue sealers developed over time,
ticles was limited to studies representing high levels of helping surgeons to perform complex minimally inva-
evidence such as prospective comparative studies, ran- sive surgeries.
domised controlled trials, systemic reviews and meta- Alternative to da Vinci systems: The other robots.
nalsysis. Review of past and current robotic system also
REVO I Robotic Surgical System (Meere Company,
included product monograph and details from various South Korea)
websites of relevant companies.
The REVO-I system is a master slave system similar to
Time line of robotic assisted surgery, from past to
the Da Vinci system. They developed the current model
future.
(after working for over 20 different systems) the MSR-
High initial installation cost and high disposable cost
5000 REVO-I which was introduced in 2015. Clinical trail
*
Dept.of Uro-Oncology,, **Dept.of Urology, AIMS, Amrita Vishwa Vidyap-
eetham,Kochi,India. for performing cholecystectomy and prostatectomy
3
Amrita Journal of Medicine Role of Robotic Surgery in Urology
was successful, following which it got Korean FDA ap- A 13 year analysis of Data involving 416 hospitals and
proval in August 20174,5. 24000 patients, needing renal surgery concluded that
Senhance Surgical Robotic System (Transenterix, the number of robotic surgeries have surpassed the
USA) number of laparoscopic procedures in recent times
and there was no difference in the outcomes of the two
Initially developed by the Italian company called
modalities except for longer operative duration and
Sofar, as ALF-X robotic system. The system was later
higher cost per patient. For complex tumors, the opera-
bought by US-based Transenterix Company later re-
tive time was similar between laparoscopy and robotic
naming it as Senhance Surgical Robotic System. It has
approaches. But the higher cost was due to the use of
advantages of being compatible with any 3D vision cart
additional surgical disposables15. The robotic approach
system and with use of laparoscopy instruments help- when compared to laparoscopic partial nephrectomy
ing in significant reduction of cost6. All available data is proved better interms of ability to attempt complex
from gynaecological or colorectal procedures7,8 . cases with better success, less warm ischemia time, less
Hugo RAS - the newly launched Robot from Medtronics conversions rate to open, less positive surgical margins,
Company was unveiled recently and carries more flexi- less complications16.
bility in usage of arms. The Hugo system has 3 compo- Emerging role of additional technology
nents – central tower, console and multiple cart-based
The Firefly technology introduced in da Vinci Si HD
rolling robotic arms. The advantage is cost effective-
vision system helps in incorporating real-time near
ness being comparable to conventional laparoscopy.
infra-red fluorescence imaging with the help of Indo-
The system has incorporated the current standards of
cyanine green for providing excellent delineation of
vision magnification and 3D vision. The system is aim-
ing at CE and FDA approval around 2021 – first quarter9. vascular anatomy. In partial nephrectomy, it ensures
adequate clamping of renal artery prior to tumor dis-
The Versius robot by CMR Company is a machine sys- section and to rule out the presence of additional ac-
tem from Cambridge, UK, similar to Hugo RAS men- cessory arteries. Indocyanine green works by binding
tioned above. The company has received ISO certifica- with plasma proteins which retain it in circulation.
tion in September 2018 for further use of its system for Hence, after declamping, uptake is well in normal re-
practical use. This system has individual robotic arms nal parenchyma and reduced uptake in renal cortical
for use and has more flexibility and could hence be tumors which have reduced expression of the protein.
cost-effective10. This is better appreciated after the initiation of dissec-
Verb surgicals – merger of Johnson & Johnson and Ver- tion of tumor from its bed17,18.
ily (Google’s concern) is working in the lines of produc- The drop down Ultrasound probe provides good ra-
ing another robot in the near future11. diological imaging. It delineates tumor from normal
Components of robots renal parenchyma. Intra-operatively, helps complete
The most commonly used Da Vinci robot has 3 main tumor removal, ensuring negative surgical margin and
components – the console, the vision cart and the pa- helps preserve normal renal parenchyma. All these
tient-side cart. The surgeon console is the place from techniques helps achieve trifecta- (negative margins,
where the surgeon performs the surgery using control- no urologic complications, minimal decrease in renal
lers for hand and feet. This controls the camera and the function) in post operative period. Robotic surgery
operating robotic arms. It has 3D vision with magnifi- when selected for appropriate patients, with a techni-
cation.The vision cart carries all the instruments that cally sound procedure, care guided pathway, peri-op-
are needed for surgery like the camera processor, light erative management, provides good outcomes in most
source, pneumo system and diathermy system. The pa- cases achieving goals of pentafecta (long term cancer
tient side cart has the robotic arms which get attached control and avoidance of all complications). Robotic
with camera and instruments in the four arms and per- surgery when available can replicate oncological out-
form the actions simulated in the console inside the pa- comes of open surgery in complex cases with advan-
tient’s body. Docking is the process by which the robot- tages of minimal access surgery.
ic arms are attached to the ports and arms are aligned Robot assisted Laparaoscopic Radical Prostatecto-
my(RARP)
for surgery12,13.
10 year retrospective single centre, single surgeon ex-
Role of robotic surgery for Partial nephrectomy perience of 902 cases of Radical Prostatectomy surger-
The role of Robotic surgery in partial nephrectomy is ies – open Retropubic Radical Prostatectomy(RRP) vs
well established with many papers. Beyond regular ad- Laparoscopic Radical Prostatectomy (LRP) vs RARP were
vantages of less bleeding, transfusion, hospital stay and compared and found to show RARP had lesser blood
analgesic requirement, the robotic approach provided loss, less transfusion, less hospital stay on comparing
most importantly less eGFR loss and ability to complete the 3 arms and lesser conversion rate to RRP when
procedures for complex renal tumours14. comparing with LRP.Margin positive rate was same in
4
Amrita Journal of Medicine
3 groups. 1 year continence rate was slightly better in Robot Assisted Adrenal surgery
robotic arm when compared to laparoscopic and open Robotic surgery has shown to be feasible and safe for
surgery19. resection of benign as well as malignant conditions of
The conversion rate of LRP all over the world are adrenal gland. When compared to open and laparo-
around 2-8%, whereas for RARP is around 0-1%. The scopic adrenalectomy, robotic adrenalectomy is associ-
complication rate of RARP is lower than LRP or RRP (13% ated with lower blood loss and length of hospital stay
vs 20-28% for LRP and RRP) and minimal Clavien-Dindo but is associated with more cost per surgery. Robotic
grade 4/5 complications20,21.The experience of a sur- surgery can provide distinct advantage in case of par-
geon has been proved to be an important factor for tial resection in patients with familial syndromes. It may
trifecta of results in RP surgeries. The learning curve for provide advantage over conventional laparoscopy is
LRP is steep as compared to RARP. Better vision, dexter- case of large tumors, pheochromocytomas and in obese
ity and accessibility of difficult areas in pelvis has made patients26-28.
RARP preferable option by surgeons over LRP or RRP
Role in reconstructive urology
Robot assisted laparoscopic Radical Cystectomy with
Robotic pyeloplasty is preferred by surgeons over
diversion
laparoscopy for the ease of intra-corporeal suturing
Although the use of Robot improves surgeon comfort and in paediatric patients due to smaller surgical scars
and less blood loss and need for transfusion and less compared to open incision29,30. The first reported case
hospital stay, the oncological outcome of this does not of Robot assisted vesico-vaginal fistula closure was
score over open cystectomy and is comparable on the done in 2004. A single centre retrospective analysis of 4
same level. Additional concerning factor in the Indian years data of patients undergoing Robot assisted lapa-
population is the cost of surgery. The use of Robot in roscopic vesico-vaginal fistula repair was reported. Sur-
cystectomy increases the cost of procedure by double gery was successful and all patients had a 2 year symp-
or triple and may not be suitable for all centres to adapt tom-free follow up31,32.
the same. Even post cervical cancer brachytherapy infra-trigo-
The RAZOR trial was a prospective multicentre ran- nal vesicovaginal fistula was repaired by Robot assisted
domised control trial which evaluated 350 patients transpertoneal transvesical approach and is symptom
with bladder cancer for radical cystectomy under dif- free on follow up33. First simple robot assisted simple
ferent surgical approaches. The study showed similar prostatectomy was performed in 2007. Subsequently
oncological outcomes with progression free survival a small series of cases were treated by the same tech-
rate being similar. The benefits of minimally invasive nique with less complications and better patient com-
surgery of less blood loss, transfusion, hospital stay, an- fort than open procedures. All patients had continence
algesic use and scar were better than the open surgery by 3rd month34.
arm22. Robotic Video Endoscopic Inguinal Lymphadenec-
Literature review comparing open vs robotic cystec- tomy(VEIL) is a relatively newer surgical procedure to
tomy suggested robotic to have lesser blood loss, need adopt robot assistance and is gaining preference due
for transfusion, narcotic need, hospital stay and faster to its precise movements and visualisation with added
GI recovery. However, robot also takes more operative advantages of minimally access surgery. Patients have
time and is more expensive. No differences in positive better recovery with lesser complications. Our Indian
surgical margins or lymph nodes, continence rate or re- data on initial VEIL produced successful outcome and
currence rate were noted. There is still an increased risk good oncological yield35.
of distant metastasis to extra pelvic lymph nodes and
peritoneum associated with robot23. A single surgeon Role of robotic surgery in functional urology
trial comparing outcomes of radical cystectomy with As the ageing population is increasing, the demand
intra corporeal conduit creation vs. open cystectomy for correction of pelvic organ proplase in expected to
was done over a 2 year period including 39 patients grow. Correction of Pelvic Organ Prolapse can be done
concluded that oncological outcomes and complica- vaginally or through abdominal approach. Current
tion rates were similar24. iROC is the only randomised available data supports superiority of abdominal sac-
control trial comparing complete intra corporeal con- rocolpopexy in correction of apical prolapse. Robotic
duit creation vs. ORC. The study is still midway and will sacrocolpopexy may become the preferred treatment
have results close to analyse by 2020. The advantages approach for women with moderate prolapse and an
of this trial being complete intra corporeal anastomo- apical component due to avoidance of mesh and re-
sis as a mandate while most other studies compare lated complications with outcomes matching open
robotic cystectomy with extracorporeal anastomosis counterpart and advantages of minimally invasive sur-
which leads to loss of advantage of minimally invasive gery36-38 .
approach25. Other procedures performed are the correction of
5
Amrita Journal of Medicine Role of Robotic Surgery in Urology
female stress urinary incontinence (artificial urinary in the new millennium. J Urol . 2017; 197(2S):S213–S215. https://
sphincter) and the treatment of chronic pelvic pain (pu- doi.org/10.1016/j.juro. 2016.11.030
dendal nerve neurolysis)39. 3. https://finance.yahoo.com/news/introducing-intuitive-surgi-
cal-nasdaq-isrg-140157595.html ; Accessed on 5th October
Robot-Assisted Microsurgery in Male Infertility and
2019.
Andrology
Role of Robot-Assisted Microsurgery in Male Infer- 4. Pradeep P. Rao World Journal of Urology. 2018; 36:537–541
https://doi.org/10.1007/s00345-018-2213-y
tility and Andrology is still evolving. Early data reports
some benefits. It has been used for Robotic-assisted 5. Abdel Raheem A, Troya IS, Kim DK, Kim SH, Won PD, Joon PS, et
microsurgical vasectomy reversal, Robotic-assisted al.; Robot assisted fallopian tube transection and anastomosis
microsurgical sub-inguinal varicocelectomy, Robot- using the new REVO I robotic surgical system: Feasibility in a
chronic porcine model; BJU Int. 2016;118:604 9.
ic-assisted microsurgical testicular sperm extraction,
Robotic-assisted microsurgical targeted denervation of 6. Bozzini G, Gidaro S, Taverna G ; Robot-assisted laparoscopic par-
the spermatic cord. This area of robotic surgery is still tial nephrectomy with the ALF-X robot on pig models; Eur Urol.
69(2):376–377. https://doi.org/10.1016/j.eurur o.2015.08.031 8.
evolving and future looks promising. But, as with any
other technology, cost and long term outcome in ran- 7. Fanfani F, Restaino S, Gueli Alletti S, Fagotti A, Monterossi G, Ros-
domized controlled studies will define further progress sitto C, Costantini B, Scambia G. TELELAP ALF-X robotic-assisted
in such subspecialties of urology40-45. laparoscopic hysterectomy: feasibility and perioperative out-
comes; J Minim Invasive Gynecol. 2015; 22(6):1011–1017. https://
Role of Bed-Side Surgeon in Robotics (patient side doi.org/10.1016/j.jmig.2015.05.004 9.
surgeon) and learning robotic surgery
8. Fanfani F, Monterossi G, Fagotti A, Rossitto C, Gueli Alletti S, Cos-
The term patient side surgeon (PSS) plays a vital role tantini B, Gallotta V, Selvaggi L, Restaino S, Scambia G. The new
in safe conduct of robotic surgery and is the primary in- robotic TELELAP ALF-X in gynecological surgery: single-cen-
terface among the console surgeon, robot and patient. ter experience. Surg Endosc. 2016; 30(1):215–221. https ://doi.
Role of assistant surgeon is more in robotic surgery as org/10.1007/s00464-015-4187-9
compared to open and laparoscopic surgeries. Transi- 9. h t t p s : / / w w w. m a s s d e v i c e. c o m / m e d t ro n i c - f i n a l l y - u n -
tion to robotic surgery requires laparoscopically trained veils-its-new-robot-assisted-surgery-system. Accessed on 5th
assistants. A laparoscopically trained console surgeon October 2019.
cannot obviate the need for a trained bed side surgeon 10. https://cmrsurgical.com/versius/surgical-teams/. Accessed on
because the bed side surgeon has to assist throughout 5th October 2019.
the procedure. It is not possible for the unscrubbed, re-
11. https://www.fiercebiotech.com/medtech/verb-surgical-taps-
motely located console surgeon to use his or her lapa- new-ceo-as-it-inches-its-digital-surgery-robot-toward-market.
roscopy skills during the surgery. For the same reason, Accessed on 5th October 2019.
trainees who wish to become robotic surgeons have to
12. h t t p s : / / w w w. d a v i n c i s u r g e r y c o m m u n i t y. c o m / d o c u -
learn basic laparoscopy. This training is in addition to ments/10184/10442/1009589rC_da_Vinci_Xi_System_Bro-
training in open surgery that guides all steps performed chure_Europe_low%20res_314841.pdf/819597de-031a-48fc-
during robotic surgery. Accurate port placement, robot ab6a-1d4c4ad8b03e. Accessed on 5th October 2019.
docking and interchange of instruments are other vital
13. https://www.intuitive.com/en-us/products-and-services/da-vin-
learning steps in robotic training46. ci/vision. Accessed on 5th October 2019.
CONCLUSION
14. ShengHan Tsai,PingTao Tseng, Benjamin A. Sherer. Open versus
As robotic system provides three-dimensional, robotic partial nephrectomy: Systematic review and meta-anal-
high-definition images with small instruments with ysis of contemporary studies. Int J Med Robotics Comput Assist
endowrist technology, ergonomic position for surgeon Surg. 2019; 15:e1963.
and ease of teaching to fellows and residents, the in- 15. Hoiwan Cheung, B.A., Ye Wang Ph.D , Steven L Chang, M.D. Adop-
dications of robotic surgery will continue to evolve. tion of robotic assisted partial nephrectomies: A population
Increased cost burden to healthcare provider and pa- based analysis of U.S. surgeons from 2004-2013. Journal of En-
tients who bear most cost of surgery due to lack on dourology. DOI: 10.1089/2017.0174
penetration of insurance, are major problems in adap- 16. Jung Kwon KimID, Hakmin Lee, Jong Jin Oh, Sangchul Lee. Com-
tation of robotic systems in India. parison of robotic and open partial nephrectomy for highly com-
“Life can only be understood backwards; but it must plex renal tumors (RENAL nephrometry score >10; PLOS ONE.
be lived forwards.” Soren Kierkegaard quote defines doi.org/10.1371/journal.pone.0210413; January 10, 2019.
future of robotic surgery in India. 17. Sohrab Arora, MCh and Craig Rogers, MD. Partial Nephrectomy in
Central Renal Tumors. JOURNAL OF ENDOUROLOGY ;Volume 32,
REFERENCES Supplement 1, May 2018. S-63–S-67 DOI: 10.1089/end.2018.0046
1. https://yourstory.com/2017/11/india-second-largest-market-ro-
botic-surgery. Accessed on 5th October 2019. 18. Zachary Klaassen, Qiang Li, Rabii Madi, Martha K. Terris. The Role
of Indocyanine Green for Robotic Partial Nephrectomy: Early Re-
2. Cole AP, Trinh QD, Sood A, Menon M. The rise of robotic surgery sults, Limitations and Future Directions. Robotics 2014, 3, 281-
6
Amrita Journal of Medicine
288; doi:10.3390/robotics303028. Laparoscopic Repair of Vesicovaginal Fistula: A Single-center Ex-
perience. Urology. 2015;08-01,Volume 86, Issue 2, Pages 276-82.
19. Lorenzo Giuseppe Luciani, Daniele Mattevi, William Mantovani,
Tommaso Cai, Stefano Chiodini, et al. Retropubic, Laparoscopic, 33. João Pádua Manzano, Fábio da Silva Crochik, Felipe Guimarães
and Robot-Assisted Radical Prostatectomy: A Comparative Anal- Pugliesi. Case Report Robot-Assisted Infratrigonal Vesicovaginal
ysis of the Surgical Outcomes in a Single Regional Center. Curr Fistula Repair. Case Reports in Urology. Volume 2019, Article ID
Urol. 2017 Nov; 11(1): 36–41. doi: 10.1159/000447192 2845237, 4 pages https://doi.org/10.1155/2019/2845237. Ac-
cessed on 5th October 2019.
20. Ahlering TE. Robotic versus laparoscopic radical prostatectomy.
Nat Clin Pract Urol 2004;1:58–9 34. Sotelo R, Clavijo R, Carmona O. Robotic simple prostatectomy. J
Urol. 2008; Feb;179(2):513-5.
21. Ahlering TE . Robotic versus laparoscopic radical prostatectomy.
Nat Clin Pract Urol. 2004;1:58–9 35. Dogra P N, Saini AK, Singh P, Robotic-assisted inguinal lymph
node dissection: A preliminary report. Indian J Urol. 2011;27:424-
22. Dipen J Parekh, Isildinha M Reis, Erik P Castle et al. Robot-assisted 7.
radical cystectomy versus open radical cystectomy in patients
with bladder cancer (RAZOR): an open-label, randomised, phase 36. Olsen A.L., Smith V.J., Bergstrom J.O., et al. Epidemiology of surgi-
3, non-inferiority trial. Lancet. 2018 Jun 23; 391(10139):2525- cally managed pelvic organ prolapse and urinary incontinence.
2536. doi: 10.1016/S0140-6736(18)30996-6. Obstet Gynecol. 1997; 89: pp. 501
23. Rachel B. Davis, Nicholas J. Farber, Alexandra L. Tabakin. Open 37. FDA safety communication: UPDATE on serious complications
versus robotic cystectomy: Comparison of Outcomes. Investig associated with transvaginal placement of surgical mesh for pel-
Clin Urol. 2016; 57 Suppl 1:S36-43. vic organ prolapse. Available at: http://www.fda.gov/medicalde-
vices/safety/alertsandnotices/ucm262435.htm. Date issued: July
24. Chow K, Zargar H, Corcoran NM. Robotic-assisted radical cystec- 13, 2011.
tomy with intracorporeal urinary diversion versus open: early
Australian experience. ANZ J Surg. 2018 Oct; 88(10):1028-1032. 38. Rosenblum N. Robotic approaches to prolapse surgery. Curr
doi: 10.1111/ans.14361. Opin Urol. 2012; 22: pp. 292
25. James W F Catto, Pramit Khetrapal, Gareth Ambler ; Catto JWF, et 39. Moscatiello P, Sánchez Gallego MD, Carracedo Calvo DRole of ro-
al. Robot-assisted radical cystectomy with intracorporeal urinary botic surgery in functional urology. Arch. Esp. Urol. July 25, 2019;
diversion versus open radical cystectomy (iROC): protocol for a 72 (3); 326-35.
randomised controlled trial with internal feasibility study. BMJ.
40. Trost L., Parekattil S., Wang J., et al. Intracorporeal robot-assisted
2018;8:e020500. doi:10.1136/bmjopen-2017-020500
microsurgical vasovasostomy for the treatment of bilateral vasal
26. Boris RS, Gupta G, Linehan WM, et al. Robot-assisted lapa- obstruction occurring following bilateral inguinal hernia repairs
roscopic partial adrenalectomy: initial experience. Urology. with mesh placement. J Urol. 2014; 191: pp. 1120-25
2011;77(4):775−80.
41. Shu T., Taghechian S., and Wang R. Initial experience with ro-
27. Barbash G, GliedSA. New technology and health care costs—the bot-assisted varicocelectomy. Asian J Androl. 2008; 10:pp.146-
case of robot-assisted surgery. N Engl J Med. 2010;363(8):701– 148
704.
42. Larsen S.M., Benson J.S., and Levine L.A. Microdenervation of the
28. Bodner J, Augustin F, Wykypiel H, et al. The da Vinci robotic sys- spermatic cord for chronic scrotal content pain: single institution
tem for general surgical applications: a critical interim appraisal. review analyzing success rate after prior attempts at surgical cor-
Swiss Med Wkly. 2005;135:674–8. rection. J Urol. 2013;189:pp.554-8
29. Tareq Aro, M.D., Michael Mullerad, M.D., and Gilad E. Amiel, M.D. 43. Gudeloglu A., Brahmbhatt J.V., and Parekattil S.J. Robotic micro-
Expanding the Utilization of Robotic Procedures in Urologic Sur- surgery in male infertility and urology—taking robotics to the
gery. Rambam Maimonides Med J. 2017; Issue 4.Volume 8 Octo- next level. Transl Androl Urol. 2014; 3: pp. 102-112
ber 2017
44. Santomauro M.G., Choe C.H., James O., et al. Robotic vasovasos-
30. Michael V. Hollis, Patricia S. Cho, Richard N. Yu. Pediatric Ro- tomy: description of technique and review of initial results. J Ro-
bot-Assisted Laparoscopic Pyeloplasty. Am J Robot Surg. 2015; bot Surg. 2012; 6: pp. 217-21.
Dec:2(1): 1 –8. doi: 10.1166/ajrs.2015.124
45. Parekattil S.J., Gudeloglu A., Brahmbhatt J., et al. Robotic assist-
31. O.Melamud, L.Eichel, B.Turbow,A.Shanberg. Laparoscopic vesi- ed versus pure microsurgical vasectomy reversal: technique and
covaginal fistula repair with robotic reconstruction. https://doi. prospective database control trial. J Reconstr Microsurg. 2012;
org/10.1016/j.urology.2004.09.052. accessed on 5th October 28:pp.435-44
2019.
46. Menon M, Hemal AK: Robotic urologic surgery: is this the way of
32. Vineet Agrawal, Victor Kucherov, Emma Bendana. Robot-assisted the future? World J Urol. 24:119, 2006.
7
Amrita Journal of Medicine Vol. 15, No: 4
Oct-Dec 2019, Page 1 - 44
ORIGINAL ARTICLE
Immunization Coverage in a Rural Area of Malappuram
District, Kerala: A Cross Sectional Study
Sreelakshmi Mohandas K*, Vivin Vincent**, Teena Mary joy*, Dulari Gupta***
ABSTRACT
BACKGROUND: In India, 5 lakh children under 5 years of age die annually due to vaccine preventable diseases(1). One out of
seven deaths among young children can be prevented with 100% immunization and 100% efficacy of vaccines(2). According to
CES 2009, immunization coverage for children aged 12-23months in Kerala was 81.5%(3). However, in the Northern district of
Malappuram, the immunization coverage was only 63.9%, the lowest in the state(4).
OBJECTIVES: Hence, this study was carried out to assess the immunization coverage and to study the factors associated with
immunization among children between 12-23 months of age in a rural area of Malappuram, Kerala.
MATERIALS & METHODS: A cross sectional study was done in Morayur panchayath in 2014; the minimum calculated sample
size was 172(10), children between 12-23 months of age from Morayur Panchayath were selected by cluster sampling. Data were
collected using a pre tested semi structured questionnaire.
RESULTS: 64.7% of children were fully immunized for age and 2.9% were unimmunized in the study. Vaccination delay was found
to be 88.5% and the major reasons for delaying were occurrence of minor ailments in the child at the time of vaccination and
fear of vaccine side effects like fever and pain. The vaccine coverage for BCG and OPV 0 dose were the highest, 97.5% and 97%
respectively.
CONCLUSION: The immunization status of children below 2 years of age in Morayur, A Panchayath of Malappuram district was
found to be low. Addressing the fear of vaccine side effects may help to increase the vaccination status of the community.
Keywords: immunization, rural area, vaccine coverage
Corresponding Author: Sreelakshmi Mohandas K, Assistant Professor,Dept.of Community Medicine,AIMS,Kochi.
INTRODUCTION try has the largest pool of unimmunised children in the
Immunization is one of the most widely discussed, world, accounting for approximately 4.2 million8.
controversial topics in health care . It is also one of the In Kerala, the state with the highest epidemiological
most successful and effective health interventions ever. transition levels,9 the percentage of fully immunised
It has successfully eradicated small pox, lowered the children in the age group of 12-23 months was 82.5%10.
global incidence of polio and achieved remarkable re- Looking at it from the other side of the spectrum; nearly
ductions in disability, illness and death from diphtheria, 1/5th of children aged 12-23 months in Kerala have not
whooping cough, tetanus and measles. received all the recommended vaccines.
In the last 10 years, great advances have been made The disparity in immunization coverage comes mainly
in developing and introducing new vaccines and ex- from the variations among the districts in Kerala, partic-
panding the reach of immunization programmes. As ularly in the northern districts like Malappuram, where
a result of immunization combined with other health the immunisation cover for children aged between 12-
care and development interventions the annual num- 23 months is at approximately 63.9%, the lowest in the
ber of deaths among children under five years of age state4.
fell from an estimated 9.6 million in 2000 to 7.6 million Hence, the objective of this study was to assess the
in 2010, despite an increase in the number of children immunization coverage among children aged 12
born each year5. months-24 months in a rural area of Malappuram dis-
According to 2016 WHO reports, immunization averts trict and thereby to study the factors associated with
an estimated 2-3 million deaths every year. With 100% immunization coverage and to look for the reasons for
immunization and 100% efficacy of vaccines, 1 out of 7 vaccination delay, if any among them.
deaths among young children can be prevented2. Even MATERIALS AND METHODS
then, approximately 19.4 million infants miss out on ba- A community based cross sectional survey was car-
sic vaccinations globally6. Vaccine preventable deaths ried out between June to November 2014 in Morayur
are usually caused by a failure to obtain the vaccines Panchayath of Malappuram District Kerala. The pancha-
in a timely manner, due to lack of sufficient immunoge- yath has a total population of 33,960 with 6,900 house-
nicity or due to administration of inactivated vaccine. holds and 14.9% of the population being comprised of
Vaccine preventable diseases are responsible for over children less than 6 years of age11. The study popula-
5 lakh under five deaths annually in India1. Our coun- tion included children between 12-24 months of age,
*Dept.of Community Medicine,AIMS,Amrita Vishwa Vidyaeetham,Kochi,In- registered in the anganwadis. However, morbidly sick
dia. **Dept.of Community Medicine,Amala Institute of Medical Scienc-
es,Thrissur. *** Dept.of pediatrics ,CMC Vellore. children and children who are not permanent residents
8Amrita Journal of Medicine Immunization Coverage in a Rural Area of Malappuram District, Kerala: A Cross
Sectional Study
of the panchayath were excluded from the study. RESULTS
The minimum calculated sample size for the study was A total of 173 children were included in the study
1725 and a total of 173 individuals were interviewed. Of with mean age of 17.73+ or - 3.6 months. Due to incom-
the 6 Taluks in Malappuram district, Ernad taluk was pleteness of data, 7 children were excluded. The mean
selected randomly and from the 20 Panchayaths in the age of mother and father were 26.8+ or - 4.9 years
taluk, Morayur panchayath was selected randomly and and 33.4+ or - 5.3 years respectively. The mean age of
each of the 18 wards in the panchayath was taken as a mother at marriage was 18.9+ or - 2.3 years. Majority
cluster. From each cluster 10 children were taken in-or- of fathers (74.6%) had an education between 5th and
der to meet the required sample size. 10th std while 91% of the mothers had a qualification
A pre tested semi structured questionnaire was used above 10th std. Of the 173 participants, 54.9% were
in order to collect information regarding the socio de- males and 83.8% of the study participants belonged to
mographic variables, immunisation history and reasons muslim religion. Based on order of birth, 35.8% of them
for delay in vaccination if there was a delay in admin- were of first and second birth order, each and 28.3%
istering the vaccine. For this study, if any one dose for were of third order or above. Only 19.7% of the mothers
age, if not administered was considered as partially im- had a minimum of 4 ANC visits. Approximately, 70% of
munized; if no vaccine has been administered, it was re- all participants received their immunizations from the
ferred to as unimmunized and if vaccine was not given government sector.
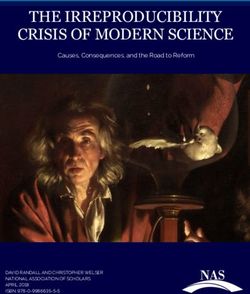
at the appropriate time, i.e within 2 weeks from the pre- The complete vaccine coverage; full immunization;
scribed date it has been considered as delayed immu- was found to be 64.7%. Approximately, 32.4% of the
nization. According to the WHO guideline, “complete or study participants were partially immunized and 2.9%
full immunization” coverage is defined as a child who of them were unimmunized. The immunization cov-
has received a BCG vaccination; three doses of DPT; at
erage for individual vaccines is described in Figure 1.
least three doses of polio vaccine; and one dose of mea-
An Increasing trend was noticed for vaccine coverage
sles vaccine12. The immunization card of the child was
at 6 weeks to the coverage at 14 weeks, from 45.6% to
cross checked to look for delay in vaccination.
91.3%.
The questionnaire was administered in the native lan-
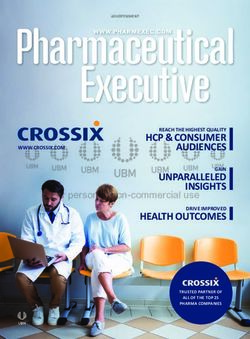
guage with the help of ASHA workers. The informants Around 93.6% of all vaccinations were delayed and
were the mothers, except a few where the information the reasons for delay in vaccination are depicted in fig-
was collected from the grandparents in case of working ure 2. The foremost reason for vaccine delay was non
mothers. Written consent was taken from the informant serious illnesses in the child, 48%.
prior to administration of the questionnaire. Data were Univariate analysis is described in Table 1.
entered and analysed using SPSS. To test the statistical Multivariate logistic regression is described in Table 2.
significance of the association of immunization status Low paternal education showed a statistically signif-
with various factors, chi square test, odds ratio and icant association with full immunization of the child
backward logistic regression analysis were done. (OR=1.98 (1.06-3.68), (aOR= 0.40 (0.22-0.82))
Fig 1: Distribution of study participants based on Immunization Coverage for Individual Vaccines
9Amrita Journal of Medicine
Non serious illnesses in the child (48%)
Fear of vaccine side effects (14.5%)
Ignorance (9.2%)
Objection from any family members
Vaccination not delayed (5.8%)
Multiple reasons (4.6%)
Access to healthcare difficult (4%)
Any c/c illness (1.2%)
Fig 2: Reasons for Partial immunization, Unimmunization and Delay in Vaccination
Sl. No. Variable Fully Immunised Chi Square Odds
Yes (%) No (%) (p Value) Ratio (95%CI)
1 Religion
Muslims 90(62.1) 55(37.9) 2.8 (0.09) 0.45 (0.17-1.16)
Non-muslims 22(78.6) 6(21.4)
2 Mothers Education
10th Std 60 (65.9) 31 (34.1)
3 Fathers Education
10th Std 22 (51.2) 21 (48.8)
4 Professional/semi- 7 (46.7) 8 (53.3) 3.65 (0.16)
professional
Business 33 (73.3) 12 (26.7)
Skilled/unskilled 72 (63.7) 41 (36.3)
5 Income (Rs)
5000/- 79 (66.4) 40 (33.6)
6 No. of ANC Visits
1-4 visits 30 (60) 20 (40) 0.69 (0.41) 0.75 (0.38- 1.47)
5-9 visits 82(66.7) 41 (33.3)
7 Sex of the child
Female 65 (68.4) 30 (31.6) 1.25 (0.26) 1.43 (0.76-2.68)
Male 47 (60.3) 31 (35.3)
8 Birth Order
3 35 (71.4) 14 (28.6)
9 Distance to the nearest
vaccination site
1.6kms 14 (70) 6 (30)
Table 1: Univariate analysis for factors associated with immunisation status
10Immunization Coverage in a Rural Area of Malappuram District, Kerala: A Cross
Amrita Journal of Medicine Sectional Study
Variable Adjusted OR 95 % CI
High Maternal Education 1.36 0.66-2.79
Low Paternal Education 0.49 0.24-0.99
Better Paternal Occupation 1.54 0.4-4.81
Religion 0.52 0.19-1.44
Table 2: Multivariate Logistic Regression model for full immunization
DISCUSSION amounted to 48% followed duly by other reasons like
In a developing country like India, despite the fact that fear of vaccine side effects (14.5%), ignorance (9.2%)
immunization services are provided free of cost in pub- and objection from any family member (8.7%). In a
lic health facilities, immunization coverage remains low study done at Nagpur, negligence (56%) and unaware-
in some areas13, especially in rural compared to urban ness (22.7%) of parents were the major causes for de-
areas. layed immunization20. Ignorance (51.8%) as a cause for
In our study, full immunization coverage was 64.7% delayed immunization was also identified by Ujwala et
with 32.4% partial and 2.9% unimmunized. The full al in their study at Nellimarla town in Andhra Pradesh21.
vaccination coverage is lower than the Kerala DLHS 410 CONCLUSION
coverage, however higher than the national coverage
Although our study was not able to point out statis-
of 54%14. The immunization coverage in this study is
tically significant associations for immunization cover-
lower than that at a study done in Kangra15, HP (94.2%)
age in the area, various reasons for vaccine delay were
and a rural area of Maharashtra16 (67.2%). In a cross sec-
identified. Minor illnesses can be addressed during the
tional study carried out by Vasantha et al in a rural area
vaccination sessions. Health workers need to assure par-
of Trivandrum, 90% of the children were fully immu-
ents about taking timely vaccinations to avoid unneces-
nized, 10% partially17.
sary delays. Therefore, improving the knowledge about
The decreasing vaccine coverage from birth dose to
vaccines and increasing awareness about the benefits
3rd dose at 14 weeks, in our study was from 97.1%-
of vaccination along with addressing the basic fear
87.9% respectively. Similar findings were noticed in
about vaccinations and vaccine side effects may help
a study done by Gupta et al in Pune16, from 98.5%-
to improve the vaccine coverage in the area. Involving
84.76%.
the whole family and/ community, rather than parents
The percentage of unimmunized children in rural
alone might help to bring forward better involvement
Morayur was found to be 2.9%, this is higher than the
of beneficiaries in the utilisation of vaccinations, both
findings from a study done in Bangalore18 (1.82%) and
existing and upcoming.
in rural area of Trivandrum where there were no unim-
munised children17. REFERENCES
As per the analysis of NFHS 2 data by Nilanjan et al for 1. Inequity in Childhood Immunization in India: A Systematic Re-
3 states in India, it was noticed that the chance of being view [Internet]. [cited 2018 Dec 10]. Available from: https://indi-
fully immunized was higher among girls as compared anpediatrics.net/mar2012/mar-203-223.htm
to boys, there was an inverse relationship of full vac- 2. Immunization, Vaccines and Biologicals: WHO | World Health Or-
cination with increasing birth order, a strong positive ganization [Internet]. WHO. [cited 2018 Dec 10]. Available from:
relation with higher maternal education, full ante natal http://www.who.int/immunization/monitoring_surveillance/
care and with Hindu religion19. In this study, although en/
not statistically significant, similar findings were ob- 3. National_Factsheet_30_August_no_logo.pdf [Internet]. [cited
served for gender, increasing birth order and full ante- 2018 Dec 10]. Available from: http://www.indiaenvironmentpor-
natal care. A study by Ughade et al showed a significant tal.org.in/files/National_Factsheet_30_August_no_logo.pdf
association of timely vaccination with gender, maternal 4. District Level Household and Facility survey -3: Ministry of Health
and paternal education20. and Family Welfare, Kerala State Fact Sheet .pdf.pdf [Internet].
In our study, 94% of all vaccines were delayed. This [cited 2018 Dec 10]. Available from: http://rchiips.org/pdf/rch3/
is higher than the findings of 12.8% at Nellimarla21 and report/KL.pdf
31% at rural Goa22. The major reason for delaying was 5. Ministry of Health and Family Welfare. District Level Household
found to be due to the occurrence of non-serious ill- and Facility survey -4: District FAct Sheet- Malappuram: 2012-
nesses in the child; like fever, common cold or minor 2013 [Internet]. Available from: file:///C:/Users/Sreekuti/Down-
ailments at the prescribed time of vaccination which loads/Mallappuram.pdf
11Amrita Journal of Medicine
6. GVAP_Introduction_and_Immunization_Landscape_Today.pdf rchiips.org/pdf/rch3/state/India.pdf
[Internet]. [cited 2016 Nov 21]. Available from: http://www.who.
15. Rajesh Kumar Sood, Anjali Sood, Omesh Kumar Bharti, Vidya
int/immunization/global_vaccine_action_plan/GVAP_Introduc-
Ramachandran,, Archana Phull. High Immunization Coverage
tion_and_Immunization_Landscape_Today.pdf
but Delayed Immunization Reflects Gaps in Health Manage-
7. World Health Organization. Immunization coverage [Internet]. ment Information System (HMIS) in District Kangra, Himachal
Immuization Coverage Fact sheet. [cited 2018 Dec 10]. Available Pradesh, India—An Immunization Evaluation. World J Vaccines
from: https://www.who.int/en/news-room/fact-sheets/detail/ 2015569-78 [Internet]. Available from: http://file.scirp.org/pdf/
immunization-coverage WJV_2015041616214578.pdf
8. gvap_secretariat_report_2015.pdf [Internet]. [cited 2018 Dec 16. Gupta PK, Pore P, Patil U. Evaluation of Immunization Coverage in
19]. Available from: https://www.who.int/immunization/glob- the Rural Area of Pune, Maharashtra, Using the 30 Cluster Sam-
al_vaccine_action_plan/gvap_secretariat_report_2015.pdf pling Technique. J Fam Med Prim Care. 2013;2(1):50–4.
9. India_Health_of_the_Nation’s_States_Report_2017.pdf [Inter- 17. Mallika M C V, Sree Ranga M K S. A Survey on Immunization cov-
net]. [cited 2018 Dec 11]. Available from: https://www.healthda- erage among Children of rural south kerala. J Evol Med Dent Sci.
ta.org/sites/default/files/files/policy_report/2017/India_Health_ 2014 Aug 11;3:9113–23.
of_the_Nation%27s_States_Report_2017.pdf
18. K P, K L, G S, Bs P, Kumar K J. Evaluation of primary immunization
10. District Level Household and Facility survey -4: Ministry of Health coverage of infants under universal immunization programme
and Family Welfare, Kerala State Fact Sheet .pdf [Internet]. [cited in an urban area of bangalore city using cluster sampling and
2016 Dec 1]. Available from: http://rchiips.org/pdf/dlhs4/report/ lot quality assurance sampling techniques. Indian J Community
KE.pdf Med Off Publ Indian Assoc Prev Soc Med. 2008 Jul;33(3):151–5.
11. Morayur Village Population - Ernad - Malappuram, Kerala [In- 19. Nilanjan patra. Universal immunization programme in India: The
ternet]. [cited 2018 Dec 11]. Available from: http://www.cen- determinants of childhood Immunization. Available from: http://
sus2011.co.in/data/village/627456-morayur-kerala.html ssrn.com/abstract=881224
12. Lakew Y, Bekele A, Biadgilign S. Factors influencing full immuni- 20. S. N. Ughade, Zodpey SP, S. G. Deshpande, Jain D. Factors respon-
zation coverage among 12–23 months of age children in Ethio- sible for delayed immunisation among children under 5 years of
pia: evidence from the national demographic and health survey age. J Indian Med Assoc. 2000 Jan;98(1):4–5, 14.
in 2011. BMC Public Health [Internet]. 2015 Jul 30;15. Available 21. Dr. Ujwala U. Ukey , Dr. Padmasree Dantu , Dr. Dhruv S. Chitre ,
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4520202/ Dr. Srinivas Pusuluri. Factors Related To Delayed Immunisation
Among Children Below 5 Years. Int J Biol Med Res [Internet].
13. Abhijit Vinayak Banerjee,Esther Duflo, Abdul Latif, Jameel, Rachel
(2011; 2(4): 1171-1172). Available from: https://pdfs.semantic-
Glennerster, Dhruva Kothari. Improving immunisation coverage
scholar.org/dca2/e52185d6889c00363a7e2808aef5864af7b0.
in rural India: clustered randomised controlled evaluation of im-
pdf
munisation campaigns with and without incentives. BMJ. :BMJ
2010;340:c2220. 22. Noronha E, Shah HK. A study of vaccination delay among un-
der-five attendees at an immunisation clinic in a rural area of Goa.
14. India-DLHS 3(2007-2008) [Internet]. Available from: http:// Int J Community Med Public Health. 2018 Mar 23;5(4):1628–33.
12Amrita Journal of Medicine Vol. 15, No: 4
Oct-Dec 2019,Page 1-44
ORIGINAL ARTICLE
Hyperosmolar 25% dextrose with 2% lignocaine injection for
chronic plantar fasciitis treatment- A prospective observational
study from a tertiary care centre, Kerala.
Abhishek.B*, George Joseph*, Sundaram KR** , Remya Sudevan***
ABSTRACT
Background: Chronic plantar fasciitis is a common cause of foot pain in adults. Real world data with respect to the treatment of the
condition using 25 %hyperosmolar dextrose with 2 % lignocaine is limited from our setting.
Objective: To compare the change in intensity of pain due to plantar fasciitis before and after the injection of 25% dextrose (hy-
perosmolar) with 2% lignocaine using Visual Analogue Scale(VAS) score.
Materials and methods: A prospective observational study was conducted among patients attending the outpatient clinic of
Physical Medicine and Rehabilitation department of a tertiary care centre with confirmed diagnosis of chronic plantar fasciitis.
Patients diagnosed with chronic plantar fasciitis during the study period were consecutively enrolled according to the selection
criteria. After getting consent they were given injections at 3 time points- immediately after diagnosis, 6 weeks after the 1st injec-
tion and 6 weeks after the 2nd injection. The intensity of pain was calculated before and after injection with VAS score. Statistical
Analysis was done using IBM SPSS statistics version 20.
Results: A total of 15 participants completed the study. Mean age of the study group was 50 ±9.50 years. Before injection the mean
VAS score was 7.67± 1.047, and at 6 months follow up, the mean VAS was 3.4±2.063. Here the reduction of VAS score was 4.27±
1.43 with a p valueHyperosmolar 25% dextrose with 2% lignocaine injection for chronic plantar
Amrita Journal of Medicine fasciitis treatment- A prospective observational study from a tertiary care
centre, Kerala
cruited, of whom 15 participants completed the study. 3.4±2.063. The reduction of VAS score was 4.27± 1.43
Patients with unilateral or bilateral heel pain of more with p value < 0.001(Table 1). Among the patients,
than 6 months duration who have not responded to mean VAS score difference of the males was 4.50±0.707
conservative management were included in the study. and that of the females was 4.23±1.535.
Patients with acute plantar fasciitis, associated trauma, DISCUSSION
significant co-morbidities such as: local skin problems, Plantar fasciitis is one of the most commonly encoun-
diabetic neuropathy and previous surgeries in the foot tered musculoskeletal problems8,9. The diagnosis of
were excluded from the study. plantar fasciitis is mainly based on history and physi-
The study was conducted prospectively to assess the cal examination. Obesity, occupations requiring pro-
change in pain intensity with 25% dextrose (hyperos- longed standing and weight-bearing etc, are the main
molar) and 2% lignocaine injection in chronic plantar predisposing factors10. In our study, we analyzed the
fasciitis patients. A 5ml syringe was filled with 1ml of effectiveness of injection of 25% dextrose (hyperosmo-
2% lignocaine and 1ml of 50% dextrose, giving a 25% lar) with 2% lignocaine in reducing the pain associated
dextrose solution. The procedure was performed under with chronic plantar fasciitis.
aseptic precautions using a 26 G needle. The solution Long term overuse cause injury to a tendon which fol-
was injected into the insertion of plantar fascia on the lows a degenerative pathway and results in breakdown
calcaneum3. The procedure was repeated twice more of extracellular constituents, namely type I collagen
at intervals of six weeks apart. The intensity of pain and proteoglycans ultimately leading to tissue disorga-
was measured using Visual Analogue Scale and VAS nization4,5,7. Injection of 25% dextrose at the site of such
score was estimated before giving the injection and 6 tendon injury is supposed to promote fibroblast prolif-
months after the injection. Visual Analogue Scale is a eration and tissue repair, there by relieving the pain and
patient self-reported pain scale, which has demonstrat- improving function6.
ed validity and is useful for documenting incremental Our study was conducted in patients who were diag-
improvements from treatment. VAS score range from nosed with chronic plantar fasciitis. Among the 15 pa-
0-10. No pain marked as 0 and worst imaginable pain tients that were taken into study, 93% were females. An
marked as 106,7. The patient was instructed to refrain earlier study by Michael B Ryan et al also reported sim-
from any heavy loading activity during the week fol- ilar incidence where out of 20 patients, 3 were males
lowing the procedure. and 17 were females3 .
Statistical Analysis was done using IBM SPSS statis- In our study, the mean age of the patients was 50 ±
tics 20 windows (SPSS Inc., Chicago, USA). The summary 9.50 years. This is comparable with other similar studies.
statistics for categorical variables were reported as fre- The average age in Ryan’s et al study was 51 years. All
VAS Score
Variable n p Value
Mean SD
Pre injection 15 7.67 1.047Amrita Journal of Medicine
significant decrease in all mean VAS items from pre-test 4. DeMos M, van El B, DeGroot J, et al. Achilles tendinosis: chang-
to post-test (pVol. 15, No: 4
Amrita Journal of Medicine Oct-Dec 2019, Page 1 - 44
ORIGINAL ARTICLE
Assessment of 1p19q chromosomal status in gliomas by
Fluorescence in situ hybridization at a tertiary care hospital
Priya Roys*, Vidya Jha*, M V Thampi*
ABSTRACT
BACKGROUND:Malignant gliomas are the most common type of primary brain tumors. These are astrocytomas, oligodendro-
gliomas, ependymomas and oligoastrocytomas. Deletions or absence of chromosomes 1p and 19q are frequently seen in oli-
godendroglioma and oligoastrocytoma tumors. Combined deletion of 1p and 19q is a predictor of prognosis and may predict
response to treatment. A comprehensive evaluation and follow-up program is necessary for patients with 1p/19q deletion.
AIM:To study the molecular characterization of 1p36/19q13 chromosome from patients in Amrita Institute of Medical Sciences,
Kochi.
MATERIALS AND METHODS: A retrospective study was conducted over a period of one year which included 50 patients. Flu-
orescent In situ hybridization was used for testing 1p19q deletion. The clinical details and demographic data were collected and
analysed.
RESULT: In a study of 50 patients, the average age that shows a deletion in 1p or 19q arm is 44.65 years. The 1p/19q deletion is
seen predominantly in females and in Hindu religion. Frontal and temporal lobes are the most common locations for these tumors.
The most common symptoms included seizures, headaches and personality changes. Other symptoms vary by location and size of
the tumor. Out of all glioma types, astrocytomas (40 %) predominate in this study.
CONCLUSION: The study reveals that most of the patients of gliomas with 1p/19q deletion are females with a median age of
44.65 years and from Hindu religion. The most common symptoms are seizures, headaches and personality changes. Astrocytomas
are the most common gliomas in this population. The 1p/19q status in glioma will continue to serve as a useful paradigm for the
use of molecular signatures to supplement clinicopathologic data in the diagnosis and management of human gliomas.
Corresponding Author: Vidya Jha, Assistant Professor & Consultant, Dept.of Human Cytogenetics, Amrita Institute of Medical
Sciences,AIMS,Kochi.
INTRODUCTION most common symptoms are seizures, headaches and
Cancer is a genetic disease that could develop either personality changes. Other symptoms vary by location
from a predisposing mutation followed by acquired and size of the tumor and can include weakness, numb-
somatic mutations or from an accumulation of somatic ness, or visual symptoms4.
mutations that develop into a cancer phenotype1. Ma- Comparative genomic hybridization (CGH), fluores-
lignant gliomas are the most common type of primary cence in situ hybridization (FISH), polymerase chain re-
brain tumors. The heterogeneity of gliomas regarding action–based microsatellite analysis, and p53 sequenc-
clinical presentation, pathology and response to treat- ing are the most widely used techniques for detection
ment makes this type of tumor a challenging area of re- of loss of heterozygosity5. Testing for 1p/19q status in
search.Primary malignancies that originate in the brain the clinical setting appears to be most useful in 2 situa-
involve mainly glial cells (42%). Types of tumors are as- tions. The most common is that of a tumor that appears
trocytomas, oligodendrogliomas, ependymomas and as classic oligodendroglioma, where 1p/19q status is
oligoastrocytomas2. The higher the grade, the more used as a prognostic marker and a potential guide to
abnormal the cells and the more aggressive the tumor. patient management. Second is the diagnostic utility
The World Health Organization (WHO) system classifies for cases where a histologic mimic of oligodendroglio-
gliomas into four grades (I, II, III and IV), depending on ma or a morphologically ambiguous tumor is consid-
the histology of the tumor. Treatment and prognosis ered5. The study aims to assess 1p19q chromosomal
vary for different grades of tumors. Malignant or high- deletion status in glioma patients by fluorescent in situ
grade gliomas are grade III (anaplastic astrocytoma, hybridisation. It also aims to find out association of age,
anaplastic oligodendroglioma, anaplastic oligoastrocy- sex and ethnicity with gliomas.
toma, and anaplastic ependymoma) or grade IV (glio-
METERIALS AND METHODS
blastoma); tumors of grade I and II are designated low-
A retrospective study was done over a period of 2
grade gliomas. Grade II tumors may evolve into grade III
months. Data from archives of Dept. of Human Cytoge-
tumors over time. The current update (2016 CNS WHO)
netics was taken for a period of 1 year (2018) which re-
breaks with the century-old principle of diagnosis
vealed 50 patients of Glioma where FISH test for 1p/19q
based entirely on microscopy by incorporating molec-
deletion was done. Ratio of 1p:1q ≤ 0.88 and 19q:19p ≤
ular genetic parameters into the classification of CNS
0.74, indicated a 1p and 19q deletion respectively.
tumor3. When the tumor makes its presence known, the
*
Dept.of Human Cytogenetics,AIMS,Amrita Vishwa Vidyapeetham,Kochi, Statistical test was done using SPSS version 19.
India.
16You can also read