Report to Parliament on the making of a pandemic declaration - Report under section 165AG of the Public Health and Wellbeing Act 2008
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Report to Parliament on the
making of a pandemic
declaration
Report under section 165AG of the Public Health
and Wellbeing Act 2008
OFFICIAL
Contents
Purpose of the report ........................................................................................................................... 3
Provisions under the Public Health and Wellbeing Act 2008 ......................................................... 4
Making of a pandemic declaration by the Premier ...................................................................... 4
Statement of reasons for the pandemic declaration ........................................................................ 4
COVID-19 is a pandemic disease .................................................................................................. 5
A serious risk to public health arises from COVID-19 ................................................................. 6
Attachments to this report
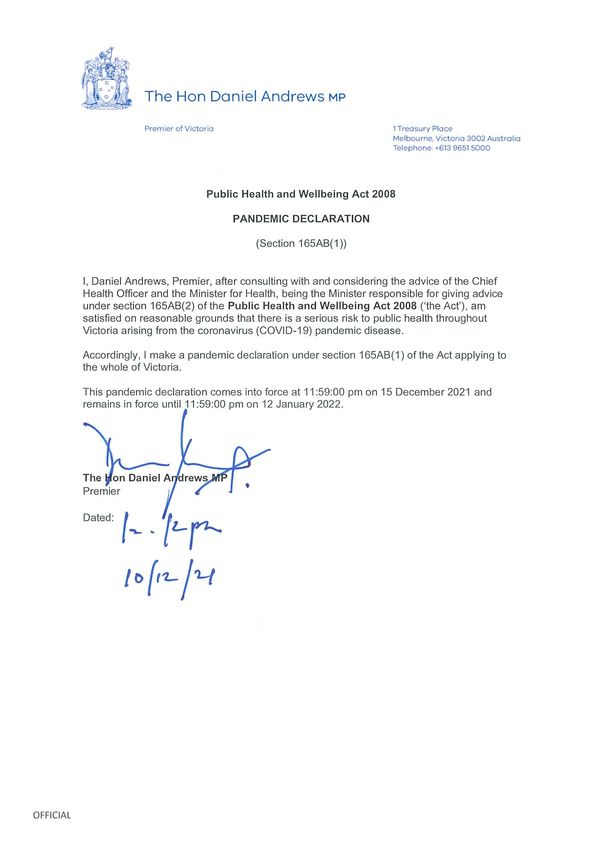
Attachment A – Copy of signed declaration by the Premier, dated 10 December 2021
Attachment B – Copy of the advice of the Chief Health Officer, dated 8 December 2021
Attachment C – Copy of the advice of the Minister for Health, dated 8 December 2021
Report to Parliament on the pandemic declaration 2
OFFICIAL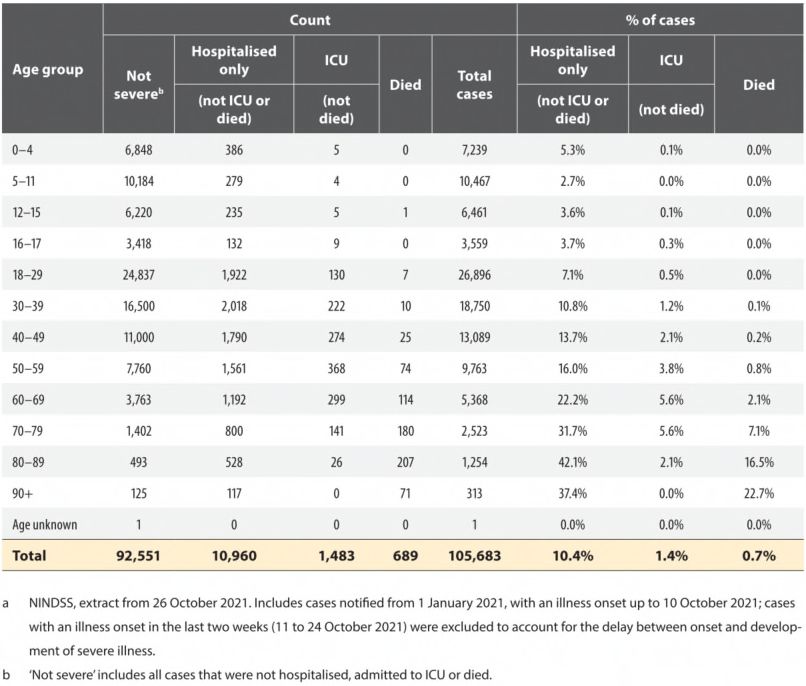
Purpose of the report
This report is provided to Parliament pursuant to section 165AG of the Public Health and
Wellbeing Act 2008 (PHW Act) following the making of a pandemic declaration by the Premier
under section 165AB of the PHW Act, commencing from 11:59pm on 15 December 2021, in
relation to the Novel Coronavirus 2019 (SARS-CoV-2), the virus which causes the coronavirus
disease (COVID-19).
As required under section 165AG of the PHW Act, this report contains a statement of reasons
for the making of a pandemic declaration and a copy of the advice of the Minister for Health,
Martin Foley MP, and the Chief Health Officer, Adjunct Clinical Professor Brett Sutton MBBS
MPHTM FAFPHM FRSPH FACTM MFTM, in respect of the making of the pandemic
declaration.
The making of a pandemic declaration for the State of Victoria has been informed by
consultation with, and advice received from, both the Minister for Health and the Chief Health
Officer.
Report to Parliament on the pandemic declaration 3
OFFICIAL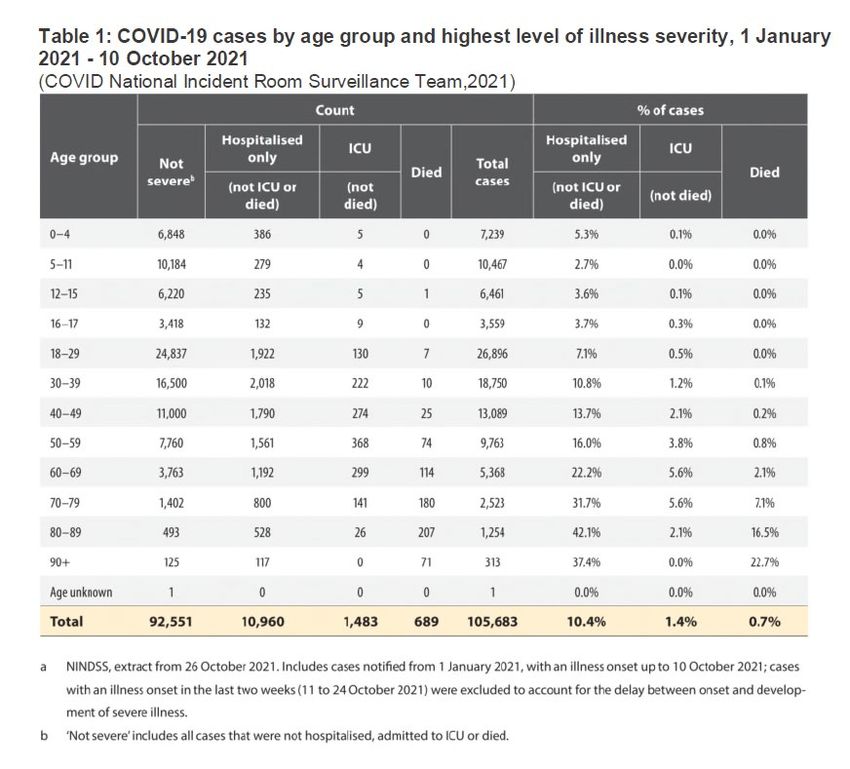
Provisions under the Public Health and Wellbeing Act
2008
Under section 165AB of the PHW Act, the Premier may make a pandemic declaration if the
Premier is satisfied on reasonable grounds that there is a serious risk to public health arising
from a pandemic disease or a disease of pandemic potential. The Premier must consult with,
and consider the advice of, the Minister for Health and the Chief Health Officer before making a
pandemic declaration.
Under section 165AC of the PHW Act, the period for which an initial pandemic declaration
continues in force cannot exceed four weeks. Under section 165AE of the PHW Act, the
Premier may extend a declaration if satisfied that there continues to be a serious risk to public
health arising from the pandemic disease or disease of pandemic potential. There is no limit on
the number of times a pandemic declaration may be extended, but the period of each extension
must not be longer than 3 months.
Under section 165CH of the PHW Act, if a pandemic declaration is made in respect of the same
infectious disease as the subject of an existing State of Emergency declaration, the declaration
of the State of Emergency ceases to be in force in respect of so much of each emergency area
that is, or is within, a pandemic management area.
Making of a pandemic declaration by the Premier
Based on the advice of, and in consultation with, the Minister for Health and the
Chief Health Officer, in response to the serious risk to public health presented by COVID-19,
the Premier made a pandemic declaration on 10 December 2021.
The declaration:
• Commences from 11:59pm, on 15 December 2021, until 11:59pm on 12 January 2022.
• Is made in respect of the coronavirus disease of 2019 (COVID-19), caused by the virus
identified as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
• Is in force throughout the State of Victoria.
The signed declaration is at Attachment A. A copy of the advice of the Chief Health Officer
supporting the making of this declaration is at Attachment B, dated 8 December 2021. A copy
of the advice of the Minister for Health supporting the making of this declaration is at
Attachment C dated 8 December 2021.
Statement of reasons for the pandemic declaration
In deciding to make a pandemic declaration, the Premier has consulted with, and considered
the advice of, both the Minister for Health and the Chief Health Officer.
As required by 165AG(1)(a) of the PHW Act, a statement of reasons for the making of the
pandemic declaration must be provided. This aims to promote additional transparency and
accountability of government and provide a clear explanation for the decision to allow powers to
be exercised under Part 8A of the PHW Act.
Report to Parliament on the pandemic declaration 4
OFFICIAL
A pandemic declaration is required to authorise the use of powers to manage pandemics
through the making and enforcement of pandemic orders and the use of pandemic
management powers across Victoria. This will remain necessary while there remains a serious
risk to public health arising from COVID-19.
After consulting with and considering the advice of both the Minister for Health and the Chief
Health Officer, the Premier was satisfied that there is a serious risk to public health arising from
the pandemic disease, COVID-19. In reaching this conclusion the Premier notes that “serious
risk to public health” is defined in section 3 of the PHW Act as “a material risk that substantial
injury or prejudice to the health of human beings has occurred or may occur, having regard to:
• the number of persons likely to be affected
• the location, immediacy, and seriousness of the threat to the health of persons
• the nature, scale and effects of the harm, illness or injury that may develop
• the availability and effectiveness of any precaution, safeguard, treatment, or other
measure to eliminate or reduce the risk to the health of human beings.”
In making this decision, the Premier took into account the matters set out below.
COVID-19 is a pandemic disease
Based on the advice of the Minister for Health and Chief Health Officer, the Premier was
satisfied that COVID-19 is a pandemic disease.
Section 3(5) of the PHW Act provides that “an infectious disease is a pandemic disease at a
particular time if, at that time, there is a pandemic outbreak of that infectious disease”. An
“infectious disease” is defined in section 3(1), and includes a human illness or condition due to
a specific infectious agent or its toxic products that arises through transmission of that agent or
its products from an infected person, to a susceptible person, either directly or indirectly through
an intermediate plant or animal host, vector or the inanimate environment.
SARS-CoV-2 is the virus that causes COVID-19. The virus first appeared in Wuhan, China, in
December 2019. The World Health Organisation (WHO) declared the outbreak a Public Health
Emergency of International Concern on 30 January 2020 and a pandemic on 11 March 2020.
The WHO has yet to declare an end to the global pandemic.
SARS-CoV-2 is a highly transmissible virus, primarily transmitted from person to person
through respiratory droplets and aerosols carrying infectious viral particles that are inhaled or
come into contact with susceptible hosts. While the disease can also be transmitted by direct
contact and fomite, the risk of transmission via these methods is lower. 1
Since tracking commenced on 30 December 2020, the WHO Coronavirus dashboard had
recorded 265,713,467 cases with 5,260,888 deaths as of 7 December 2021. 2
1
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 24.
2
WHO, WHO Coronavirus (COVID-19) Dashboard, , accessed on 8 December
2021.
Report to Parliament on the pandemic declaration 5
OFFICIALTransmission of the disease across continents is sufficiently widespread to constitute a
pandemic, noting that according to the WHO Coronavirus data table, only seven countries
worldwide have not officially recorded a case of COVID-19 since the pandemic began. 3
The virus can mutate into more transmissible, virulent and difficult to control variants. An
example of this is the Delta variant of concern (B.1.617.2). The Delta variant of concern was
first detected in India in October 2020. 4 Evidence suggests that this variant has increased
transmissibility and virulence, compared to both other variants and the ancestral Wuhan strain
of the virus. 5 A further variant of concern – designated as Omicron by the WHO on 26
November 2021 – was first detected in southern African countries in November 2021. 6
A serious risk to public health arises from COVID-19
Based on the advice of the Chief Health Officer and Minister for Health, the Premier was
satisfied that COVID-19 gave rise to a “serious risk to public health”. In particular, he was
satisfied that COVID-19 gave rise to a “material risk that substantial injury or prejudice to the
health of human beings has occurred and may occur”, having regard to:
• the number of persons likely to be affected
• the location, immediacy, and seriousness of the threat to the health of persons
• the nature, scale and effects of the harm, illness or injury that may develop
• the availability and effectiveness of any precaution, safeguard, treatment, or other
measure to eliminate or reduce the risk to the health of human beings.
The number of persons likely to be affected
Based on the advice of the Chief Health Officer and Minister for Health, the Premier was
satisfied that the Victorian population is potentially vulnerable to infection with COVID-19, with
poor health outcomes reported across all age groups, particularly for people with a wide range
of common pre-existing conditions. 7 Additionally, international experience demonstrates that
uncontained outbreaks of the disease can overwhelm hospital systems to the point of making
healthcare inaccessible to those seeking treatment for reasons unrelated to COVID-19. This
means that the number of people likely to be affected includes, primarily, those who are at risk
of being infected with COVID-19, but also those who are affected by being unable to receive
the care they need for other reasons, should the outbreak overwhelm health system capacity 8.
3
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 22.
4
WHO, Tracking SARS-CoV-2 variants, 2021, , accessed 8 December 2021.
5
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 31.
6
WHO, Tracking SARS-CoV-2 variants, 2021, , accessed 8 December 2021.
7
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 35.
8
Ibid. paragraph 40.
Report to Parliament on the pandemic declaration 6
OFFICIALSARS-CoV-2 is a novel infectious agent to which the global population had not been
exposed prior to late 2019 (and hence had not acquired resistance), meaning that there was
and continues to be significant immunological susceptibility for widespread transmission. 9
SARS-CoV-2 is highly transmissible and can spread easily from person to person through
multiple modes of transmission. 10
SARS-CoV-2, like any virus, has the capacity to mutate into more transmissible and virulent
strains. 11
Infection with SARS-CoV-2 can cause significant disease and death. 12
There have so far been 130,029 confirmed cases in Victoria out of an Australian total of
219,118, 13 and these numbers would have been significantly higher if not for the pandemic
management measures maintained throughout the pandemic so far. This is evidenced by the
case and death rates in other comparable countries. 14
COVID-19 poses a significant risk to public health because a high rate of hospitalisations from
unconstrained transmission of COVID-19 would have the effect of denying treatment to people
with other conditions requiring medical care, as has occurred in other countries where hospital
systems have been overwhelmed. In weighing the number of people likely to be affected,
consideration was given not only to the number of people likely to contract COVID-19, but to
the fact that the pandemic creates a material risk of prejudicing the health of Victorians who do
not have COVID-19 but who require medical care for other reasons and may be denied this
care if the healthcare system is significantly burdened. 15
In considering the number of people likely to be affected by the risk, the Premier has
considered whether high vaccination rates are likely to have diminished the seriousness of the
risk in the current settings. While the considerable protection offered by high vaccination rates
amounts to a significant change in the risk profile, the scale of the COVID-19 pandemic
continues to leave a significant number of people exposed to risk. 16
The location, immediacy, and seriousness of the threat to the health of persons
Based on the advice of the Chief Health Officer and Minister for Health, the Premier was
satisfied that the threat to persons likely to be affected is immediate and serious. The Premier
was also satisfied that the threat existed to persons throughout Victoria, with people in regional
areas of Victoria rendered particularly vulnerable.
COVID-19 is circulating in the Victorian community and accordingly the threat is immediate. As
of 7 December 2021, the seven-day case average is 1192 and there are 297 cases in
hospital. 17 Since November 2020, the proportion of returned positive tests has been between
1.5 and 2 per cent – a higher rate compared to New South Wales – which indicates there is
9
Ibid. paragraph 23(a).
10
Ibid. paragraph 23(b).
11
Ibid. paragraph 23 (c).
12
Ibid. paragraph 23 (d) and paragraphs 34-38.
13
Ibid. paragraph 17.
14
Ibid. paragraph 48.
15
Ibid. paragraphs 65-68.
16
Ibid. paragraphs 54-57.
17
Ibid. paragraph 64.
Report to Parliament on the pandemic declaration 7
OFFICIALlikely to be a significant number of additional cases in the community which are not being
identified. 18
When considering the location of the threat, consideration has been given to the capacities of
regional Victoria’s COVID-19 response where healthcare resources are limited compared to
metropolitan areas. Uncontained outbreaks in regional Victoria could therefore create very
serious threats to health more easily than in metropolitan areas. 19
While acknowledging that hospitalisations for COVID-19 have declined from their peak, the
threat posed by COVID-19 transmission to Victorians and Victoria’s healthcare system is, in the
view of the Chief Health Officer, “serious and ongoing”. 20 Although Victoria has increased its
hospital capacity to respond to the pandemic, there is a finite ceiling to which hospital bed
capacity can be increased, and hospital care is only a partial defence against the risk of serious
illness or death. 21 The Chief Health Officer advised that the available therapeutic interventions
for COVID-19, including antivirals, steroids and supportive care, are only partially effective in
reducing mortality and decreasing hospital stays. 22
The nature, scale and effects of the harm, illness or injury that may develop
Based on the advice of the Chief Health Officer and Minister for Health, the Premier was
satisfied that the nature, scale and effects of the harm posed by COVID-19 across Victoria are
sufficiently grave and significant to merit a designation as a serious public health risk.
COVID-19 displays a spectrum of clinical outcomes, from asymptomatic or mild illness to
serious illness and, in some cases, death. 23 While children tend to display a milder or even
asymptomatic infection, the virus can nonetheless cause severe illness requiring intensive care
treatment among children. 24
As of 10 October 2021, 25 more than 1 in 10 people in Australia across all age groups who
contracted COVID-19 so far this year have been hospitalised. However, the hospitalisation rate
was even higher than this among adults in most age groups, 26 even if they were not elderly.
The table overleaf was provided as part of the Chief Health Officer’s advice on 8 December.
18
Ibid. paragraph 63.
19
Ibid. paragraph 67.
20
Ibid. paragraph 67.
21
Ibid. paragraph 68.
22
Ibid. paragraph 68.
23
Ibid. paragraph 35.
24
Ibid. paragraph 37.
25
Ibid. Table 1 to paragraph 39. Note, cases with an illness onset in two weeks prior were excluded from
the table to account for the delay between onset and development of severe illness.
26
Ibid. Table 1 to paragraph 35.
Report to Parliament on the pandemic declaration 8
OFFICIALVulnerable members of society, including the elderly, those with co-existing medical conditions,
and those in lower socioeconomic groups, have been shown to be disproportionately impacted
and remain at risk. 27
It is not possible to predict with confidence who will have an asymptomatic infection or mild
illness and who will have a more severe illness and poorer outcome, with serious illness
recorded among people across all age groups. 28
Estimates from published literature and epidemiological sources indicate the case fatality rate
for COVID-19 varies. The current estimate of case fatality rates in Victoria is 0.15 per cent for
individuals under 70 and 14.8 per cent for individuals aged over 70. 29
It is important to emphasise that the above figures were collected in an environment of public
health measures that suppressed outbreaks to protect vulnerable people and constrained the
27
Ibid. paragraph 39.
28
Ibid. paragraph 39.
29
Ibid. paragraph 36.
Report to Parliament on the pandemic declaration 9
OFFICIALpossibility of even more lethal outcomes. 30 Without pandemic management measures, the
likely rate of death and hospitalisations in Australia would have been worse. 31
The high transmissibility and risk of death posed by COVID-19 distinguishes it from other
illnesses which commonly circulate in the community and warrant a more stringent response.
By way of comparison, the highest annual number of deaths from confirmed influenza in
Australia in recent years occurred in 2017, which caused 277 deaths in Victoria and 1,255
deaths Australia-wide. 32 Modelling indicates that without public health measures, unrestrained
outbreak of COVID-19 would likely have caused tens of thousands of deaths in Australia over
the course of the pandemic. 33
Long-term impacts of COVID-19 are still being ascertained, with evidence that some people
report persistent symptoms following recovery from the disease. These long-term symptoms
can impact multiple organ systems and cause mild to severe illness. 34
The availability and effectiveness of any precaution, safeguard, treatment, or other
measure to eliminate or reduce the risk to the health of human beings
Based on the advice of the Chief Health Officer and Minister for Health, the Premier considered
the availability and effectiveness of precautions, safeguards, treatments, and other measures to
eliminate or reduce the risk to the health of human beings.
The Premier was satisfied that current vaccination rates alone will not suffice to contain
transmission within health system capacity, and available treatments are only partially effective
in mitigating serious illness or death. 35
Vaccination is a crucial tool to manage the risk posed by COVID-19 and is the most important
pandemic management tool available. 36 While vaccinated people may still contract the virus,
the risk of developing a severe illness – if any symptoms at all – is significantly reduced. 37
Available vaccines have a powerful effect on minimising the risk of serious illness or death. 38
Reported vaccine effectiveness against death from Delta variant infection was 91 per cent for
AstraZeneca and 90 per cent for Pfizer across all age groups. 39 Furthermore, vaccines offer
protection against the risk of ‘long COVID’. 40 They also lower the risk that an infected person
will transmit the virus to others. 41 Vaccination thus serves a dual purpose in combatting the
pandemic: it protects individuals from the harm of severe disease and death, and protects the
community by slowing the spread of the virus to others. 42
30
Ibid. paragraphs 41,47 and 48.
31
Ibid. paragraph 48.
32
Ibid. paragraph 44.
33
Ibid. paragraph 48.
34
Ibid. paragraph 38.
35
Ibid. paragraphs 50-75.
36
Ibid. paragraph 51.
37
Ibid. paragraph 52.
38
Ibid. paragraphs 51 and 53.
39
Ibid. paragraph 53.
40
Ibid. paragraph 52.
41
Ibid. paragraph 52.
42
Ibid. paragraphs 51-52.
Report to Parliament on the pandemic declaration 10
OFFICIALHowever, vaccination alone will not suffice to contain transmission within health system
capacity, and some additional public health measures are needed for an effective response to
the serious health risk posed by COVID-19. 43
Vaccines alone are insufficient because:
• Access to vaccines is not currently available to children under the age of 12 years in
Australia (although the first shipment of childrens’ doses is due to arrive in Australia in
January 2022), as well as other people who for medical reasons cannot be vaccinated. 44
• Despite the current high levels of vaccination coverage in Victoria, many people in the
population will remain susceptible to this highly transmissible infection, and observational
studies indicate vaccine efficacy may wane after a period of approximately 6 months
following vaccination. 45
• The risk of immunity waning in the months following vaccination is an area of ongoing
research. 46 Evidence suggests that vaccine efficacy may wane after a period of
approximately six months following vaccination. 47
• There is a risk that strains of the SARS‑CoV‑2 virus will emerge against which vaccines
are less effective and the use of public health measures will allow us to monitor for, and
mitigate against, this possibility. 48
There are limited preventative and therapeutic interventions to manage COVID-19 and – other
than vaccines – many interventions remain supportive (oxygen, ventilation etc.) rather than
curative or preventive. The available therapeutic interventions of antivirals, steroids and
supportive care, have been shown to be only partially effective in reducing mortality and
decreasing hospital stays. 49
Other countries with high vaccination rates have nonetheless endured increased hospitalisation
rates following relaxation of restrictions, even during the northern summer and among countries
with warm climates. 50 Resurgent outbreaks among highly vaccinated populations are driven by
those who remain unvaccinated, as well as the elderly and vulnerable individuals with co-
morbidities who suffer breakthrough cases and asymptomatic healthy individuals who transmit
the virus. 51 Portugal, Singapore, Chile, Denmark and Ireland have all achieved vaccination
levels above 90 per cent, but have needed to reimpose various health measures, including
mandatory face masks in public settings, limits on gatherings and venue caps, to curtail a
worrying resurgence of hospitalisations and intensive care admissions following the easing of
restrictions. The advice from the Chief Health Officer is that this demonstrates that high
vaccination rates and warm weather will not be sufficient to defend against a resurgence of
COVID-19 in the Victorian summer, and ongoing public health interventions will be needed. 52
43
Ibid. paragraphs 54-57.
44
Ibid. paragraph 55.
45
Ibid. paragraph 56.
46
Ibid. paragraph 61.
47
Ibid. paragraph 56.
48
Ibid. paragraph 57.
49
Ibid. paragraph 68.
50
Ibid. paragraph 59-62 (including Table 2 to paragraph 62).
51
Ibid. paragraph 59.
52
Ibid. paragraphs 70-75.
Report to Parliament on the pandemic declaration 11
OFFICIALEfforts to keep the COVID-19 outbreak within the constraints of the healthcare system will be
most effective if vaccination is complemented by other public health measures such as testing,
contact tracing, isolation of positive cases and quarantine. 53 Proportionate control measures
such as international travel permits, testing requirements and exclusion from sensitive settings
during the period of highest risk will also ensure the serious threat to public health posed by
COVID-19 is managed in a way that protects vulnerable people and mitigates the risk of
uncontrolled transmission. 54
Guiding principles informing the decision to make a pandemic declaration
In determining that COVID-19 is a pandemic disease that gives rise to a serious risk to public
health, the Premier had regard to the following guiding principles outlined at sections 5 – 10 of
the PHW Act.
Evidence-based decision-making
In making the pandemic declaration the Premier had regard to the principle of evidence-based
decision-making (as required under section 5 of the PHW Act).
The advice of the Chief Health Officer was that evidence supports the view that the most
effective and efficient response to the COVID-19 pandemic requires ongoing use of public
health and social measures, rather than relying on vaccine immunity and disease treatment
alone. 55 The Minister for Health likewise advised that powers under the PHW Act were
necessary for the pandemic to be managed effectively. 56 The Premier’s decision to make a
pandemic declaration therefore advances the principle of evidence-based decision-making by
empowering the Minister for Health to use measures under Part 8A of the PHW Act to manage
the COVID-19 pandemic using public health and social measures as a complement to
vaccination and disease treatment, in line with available evidence about the most effective
measures to protect public health and wellbeing.
Precautionary principle
As outlined above, based on the advice of the Chief Health Officer 57 and Minister for Health, 58
the Premier was satisfied that the COVID-19 pandemic poses a serious risk to public health.
The Chief Health Officer noted that understanding of the nature of the SARS-CoV-2 virus
continues to evolve. 59 Consideration has been given this uncertainty but consistent with the
precautionary principle at section 6 of the PHW Act, a lack of full scientific certainty should not
be used as a reason to prevent or control the public health risk, given the COVID-19 pandemic
constitutes a serious threat to public health and wellbeing.
53
Ibid. paragraphs 73-74.
54
Ibid. paragraph 72.
55
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraphs 69 – 75.
56
Minister for Health advice to the Premier – Advice relating to the making of a pandemic declaration –
Section 165AB Public Health and Wellbeing Act 2008, 8 December 2021, paragraph 5.
57
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 76.
58
Minister for Health advice to the Premier – Advice relating to the making of a pandemic declaration –
Section 165AB Public Health and Wellbeing Act 2008, 8 December 2021, paragraph 2.
59
Ibid. paragraph 23(e).
Report to Parliament on the pandemic declaration 12
OFFICIALPrinciple of primacy of prevention
The Premier had regard to the principle of primacy of prevention set out in section 7 of the
PHW Act. The Premier received advice from the Minister for Health that the enlivening of
powers under Part 8A of the PHW Act was necessary for him to eliminate or reduce the serious
risk to public health arising from COVID-19 60 and that the response to COVID-19 would be less
effective without these powers. 61
The advice of the Minister for Health was supported by the advice of the Chief Health Officer,
who was guided by the overarching principle of prevention of disease, illness, injury, disability
or premature death, consistent with the objectives of the Act. 62 In considering the totality of
evidence in pursuit of this aim, the Chief Health Officer concluded that his advice to the Premier
was to make a pandemic declaration in order to make available the relevant powers necessary
to increase the prospects of limiting the transmission of COVID-19 in Victoria and continue to
minimise, as much as possible, the serious risk to public health. 63
Principle of accountability
The Premier had regard to the principle of accountability in section 8 of the PHW Act. He had
regard to the requirement to table this report under section 165AG including a statement of
reasons for making the pandemic declaration and a copy of the advice of both the Minister for
Health and the Chief Health Officer with respect to the making of the pandemic declaration. The
Premier was satisfied that tabling these documents in Parliament ensures his decision is
transparent, systematic and appropriate and provides members of the public access to reliable
information to facilitate a good understanding of the relevant public health issues and the
opportunity to participate in policy and program development.
Principle of proportionality
As outlined in this report, based on the advice of the Chief Health Officer 64 and Minister for
Health, the Premier was satisfied that COVID-19 pandemic poses a serious risk to public
health. 65 He had regard to the principle of proportionality in section 9 of the PHW Act, and was
satisfied that his decision to declare a pandemic was a proportionate response to prevent,
minimise and control the public health risk that COVID-19 presents. Based on the advice of the
Chief Health Officer 66 and Minister for Health, 67 the Premier was satisfied that making a
pandemic declaration was not arbitrary.
Principle of collaboration
60
Minister for Health advice to the Premier - Advice relating to the making of a pandemic declaration –
Section 165AB Public Health and Wellbeing Act 2008, 8 December 2021, paragraph 4
61
Ibid. paragraphs 5-6.
62
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 11.
63
Ibid. paragraph 11.
64
Ibid. paragraph 76.
65
Ibid. paragraphs 33-76.
66
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
December 2021, paragraph 77.
67
Minister for Health advice to the Premier - Advice relating to the making of a pandemic declaration –
Section 165AB Public Health and Wellbeing Act 2008, 8 December 2021, paragraphs 2, 4-5 and 7.
Report to Parliament on the pandemic declaration 13
OFFICIALThe Premier had regard to the principle of collaboration in section 10 of the PHW Act.
The Premier has collaborated at a national level through the National Cabinet in informing the
most appropriate Victorian response to the COVID-19 pandemic and furthering understanding
of the consequences of the COVID-19 pandemic
The advice of the Chief Health Officer has similarly been informed by collaboration with the
Australian Health Protection Principal Committee. 68
Charter of Human Rights and Responsibilities
A pandemic declaration does not itself directly affect the human rights of any person (either
positively or negatively).
Although the making of a pandemic declaration does not itself directly affect the human rights
of any person, it is the necessary first step in enlivening certain other powers under the PHW
Act. Those powers include:
a. the power of the Minister for Health to make a pandemic order (section 165AI);
b. the power of authorised officers to exercise pandemic management order powers
(section 165B);
c. the power of authorised officers to exercise pandemic management general powers
(section 165BA);
d. the power of authorised officers to exercise public health risk powers (section 190).
These powers form part of a framework that is designed to protect public health and wellbeing
in Victoria in the context of pandemics (section 165A(1)).
Noting that the most immediate potential consequence of the making of a pandemic declaration
is that the Minister for Health will be empowered to make pandemic orders, the Premier
recognised that the future exercise of that power may affect and limit human rights. The powers
of authorised officers may also have that effect, but that can only occur if the Chief Health
Officer authorises authorised officers to exercise those powers. A further step is therefore
necessary for that to occur. Further, the Minister’s power is also the power that potentially has
the most far-reaching consequences for human rights, because a pandemic order may to apply
to “all persons” (section 165AK(1)(a)). In contrast, the powers of authorised officers are more
limited (see for example section 165BA(4)).
The Premier gave consideration to how the Minister’s power to make pandemic orders might be
exercised, having regard to the examples in section 165AI(2), and how that exercise may affect
and limit the following human rights: equality (section 8); protection from medical treatment
without full, free and informed consent (section 10 (c)); freedom of movement (section 12);
rights to privacy, family and home (section 13(a)); freedom of thought, conscience, religion and
belief (section 14); freedom of expression (section 15); peaceful assembly and freedom of
association (section 16); protection of families and children (section 17); cultural rights (section
19); property rights (section 20); right to liberty and security of person (section 21); right to
humane treatment when deprived of liberty (section 22 (1)); self-incrimination (section 25(2)(k)).
Chief Health Officer advice to the Premier – Advice relating to the making of a pandemic declaration, 8
68
December 2021, paragraph 11(h).
Report to Parliament on the pandemic declaration 14
OFFICIALHowever, the Premier recognised that, ultimately, whether any exercise of the Minister’s power
will affect and limit human rights — and, if so, how — will ultimately depend on how the powers
are exercised by the Minister and the circumstances in which they are exercised.
The Premier recognised that the Minister for Health is a public authority. The PHW Act
recognises that a public authority must give proper consideration of human rights protected by
the Charter when making decisions, and must act compatibly with human rights (section
165A(2)(c)). Following the making of a pandemic order, the Minister must ensure that a
document, which addresses whether the order limits human rights, and if so, addresses the
matters set out in section 7(2) of the Charter, is published online (section 165AP(2)(c)-(d)).
The Premier also recognised that the Minister’s power to make a pandemic order is expressly
limited by a “reasonably necessary” criterion, which itself requires a “proportionality”
assessment to be undertaken by the Minister.
Ultimately, the Premier recognised that whether the requirements of the Charter are satisfied in
relation to any individual exercise of the Minister’s power will depend on how the power is
exercised and the circumstances in which the power is exercised.
Conclusion to the statement of reasons
Having considered the advice of the Minister for Health and the Chief Health Officer, the
Premier was satisfied on reasonable grounds that COVID-19 is a pandemic disease that gives
rise to serious risk to public health throughout Victoria.
In reaching this conclusion, the Premier considered that COVID-19 is highly transmissible;
causes serious illness and death; and unconstrained outbreaks of this disease across the world
have outpaced hospital capacities to a scale not witnessed in modern memory. An outbreak
beyond the limits of Victoria’s healthcare system would be catastrophic, and imperil the health
of all Victorians who require medical care, whether for COVID-19 or for other reasons.
The Premier considered the safeguards and treatments available and concluded that while
vaccination remains the state’s best defence against COVID-19, it does not supplant the need
for other public health measures. The most effective response to the pandemic requires
vaccines to be complemented by other measures protecting human health, particularly the
health of the most vulnerable.
Report to Parliament on the pandemic declaration 15
OFFICIALAttachment A – Copy of signed declaration by the
Premier, dated 10 December 2021
OFFICIALAttachment B – Copy of the advice of Chief Health Officer,
dated 8 December 2021
OFFICIALCHIEF HEALTH OFFICER ADVICE TO PREMIER
ADVICE RELATING TO THE MAKING OF A PANDEMIC
DECLARATION
Introduction and Summary ...................................................................................... 2
How the Act Informs this Advice ............................................................................ 3
Focus of my advice .................................................................................................. 4
COVID-19 is a pandemic disease ............................................................................ 5
COVID-19 is a serious risk to public health ........................................................... 9
COVID-19 has potential to cause widespread harm to many people ............................. 9
The ongoing risk requires continued public health intervention .................................. 14
Vaccines are crucial but will not eliminate the risk.......................................................... 14
Countries with high vaccination rates still experience outbreaks................................ 15
Uncontained transmission remains a threat ..................................................................... 23
Other public health measures will also play a part .......................................................... 23
Conclusion ...............................................................................................................25
References ...............................................................................................................26
1
OFFICIAL: SensitiveIntroduction and Summary
1. In response to the request from the Premier of Victoria on 7 December 2021, set out below
is my advice as Victoria’s Chief Health Officer, regarding whether the Victorian Premier
should make a pandemic declaration under section 165AB of the Public Health and
Wellbeing Act 2008 (Vic) (the Act) in relation to the coronavirus disease (COVID-19).
2. I advise that there is a serious risk to public health throughout the State of Victoria arising
from a pandemic disease, namely COVID-19. On this basis, I advise the Premier to make a
pandemic declaration.
3. In providing this advice, I am aware of the legislative context in which the Premier’s request
is made. If the Premier makes a pandemic declaration, the Act empowers Victoria’s Minister
for Health to deploy a focused public health response, which may include a combination of
non-pharmaceutical and pharmaceutical interventions. The Act requires that the public
health response be proportionate to the public health risk that the disease (in this case,
COVID-19) poses.
4. I explain my reasons for this advice below, but in summary I consider that, at the time of this
advice, COVID-19 is and remains a serious risk to public health, despite high vaccination
rates in the Victorian population due to the following:
a) Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), the virus which
causes COVID-19, is a novel infectious agent to which the global population had not
previously been exposed, meaning there was no pre-existing immunity and hence
significant immunological susceptibility to infection.
b) SARS-CoV-2 is highly transmissible and can spread easily from person to person
through multiple modes of transmission, and primarily through the airborne route.
c) There is currently widespread community transmission of SARS-CoV-2 across
Victoria.
d) There continues to be a high number of cases reported daily relative to other
Australian jurisdictions, including a significant proportion who require supported
care at home, primary care interventions, hospitalisation, intensive care unit (ICU)
admission, ventilatory support and Extracorporeal Membrane Oxygenation (ECMO)
– sometimes for several weeks - with a consequent significant burden on Victoria’s
health services.
e) The recent easing of restrictions for vaccinated international arrivals may result in
incursions of new variants of concern (VOC) which may pose a greater public health
risk to Victoria.
2
OFFICIAL: Sensitivef) There is an ongoing risk that SARS‑CoV‑2 will mutate into more transmissible,
immune evading and/or more virulent strains (World Health Organisation(a)
2021) that may result in greater morbidity and mortality, which may require a
strengthened public health response. This has been evidenced by multiple VOC,
including the Delta and Omicron variants, which have emerged since the World
Health Organisation (WHO) declared a pandemic. WHO declared the B.1.1.529
variant, now named Omicron, as a VOC on 26 November 2021. Preliminary
evidence suggests that Omicron has a large number of concerning mutations and
that there may be an increased risk of reinfection and immune escape, including to
current vaccines, with the Omicron variant compared with the ancestral COVID-19
strain and other VOCs (WHO(b) 2021).
g) Although vaccines are proven to be effective, they do not guarantee protection to all
individuals. Additionally, vaccine effectiveness appears to wane over time, which
necessitates ongoing review and revision of public health policies, including related
to third or booster doses.
h) Community transmission may persist despite high vaccination coverage, especially
in under-vaccinated cohorts including children, who remain ineligible to receive the
COVID-19 vaccine. Epidemiological evidence from other countries indicates that
infection rates can worsen with new variants or easing of public health
measures, despite high population vaccination coverage, necessitating the
reintroduction or expansion of public health measures.
5. Protective measures are therefore necessary to safeguard against the uncontrolled spread
of SARS-CoV-2 in the Victorian community, to ensure that Victoria’s health system does not
become overwhelmed, and to therefore prevent excess deaths and other harms to the
health and wellbeing of Victorians.
How the Act Informs this Advice
6. Section 165AB of the Act provides that a pandemic declaration may be made if the Premier
is satisfied there is a serious risk to public health arising from a pandemic disease, or the
outbreak or spread of a disease of pandemic potential. The period for which the declaration
may be in force is an initial period of 4 weeks. 1 It can be extended in increments of up to
three months. 2 There is no limit on the number of times a pandemic declaration may be
extended.
7. Section 3 of the Act defines the phrase “serious risk to public health” as:
1 See section 165AC(1)(c).
2 See section 165AE.
3
OFFICIAL: Sensitivea material risk that substantial injury or prejudice to the health of human beings has
occurred or may occur having regard to:
(a) the number of persons likely to be affected; the location, immediacy, and
seriousness of the threat to the health of persons;
(b) the nature, scale and effects of the harm, illness or injury that may develop; and
(c) the availability and effectiveness of any precaution, safeguard, treatment, or other
measure to eliminate or reduce the risk to the health of human beings.
8. If the Premier is considering making a pandemic declaration, the Premier must consult with
and consider the advice of the Chief Health Officer and the Minister for Health before
making a pandemic declaration. 3 This is my advice for the purpose of that provision, and I
have taken the Act’s definition of “serious risk to public health” into account when giving this
advice.
Focus of my advice
9. The primary focus of my advice is the impact that COVID-19 will have on Victorians’ health,
and the flow-on effects that the COVID-19 pandemic will have on the health and wellbeing of
the Victorian community.
10. In making this assessment, I am guided by the experience of the past 22 months of
pandemic management in Victoria and the actions that the Victorian government has
already taken. These actions have been crucial in responding to the pandemic, by
containing SARS-CoV-2 to a degree that prevented thousands of excess deaths and
allowed the health system to operate at tolerable capacity. These actions resulted in the
suppression of SARS-CoV-2 transmission for a prolonged period and ensured that the
majority of Victorians could be immunised against COVID-19 prior to substantial community
transmission of the virus recurring. I am also guided by the experience of other Australian
jurisdictions and other countries in attempting to manage the risks of COVID-19.
11. My advice is guided by the objectives of the Act, most relevantly, protecting public health
and preventing disease, illness, injury, disability, or premature death. 4 It adopts an evidence-
based approach as to the risk that COVID-19 poses and the effectiveness of precautions
that might be used to reduce that risk. 5
12. The evidence I have used to develop my advice includes:
(a) case data and analysis, including regarding disease severity;
3 See section 165AB(2).
4 See section 4.
5 See section 5.
4
OFFICIAL: Sensitive(b) outbreak data and analysis;
(c) results from available predictive, scenario-based and other modelling;
(d) ventilation and air-flow dynamics and modelling;
(e) established and emerging evidence from the scientific literature;
(f) lessons from previous transmission patterns and outbreaks;
(g) experiences from public health interventions implemented in Victoria, Australia and
internationally;
(h) analyses, guidance and statements from national authorities, such as the Australian
Health Protection Principal Committee (AHPPC), Australian Technical Advisory Group on
Immunisation (ATAGI) and Therapeutic Goods Administration (TGA), and international
organisations such as the WHO; and
(i) studies on vaccine effectiveness and COVID-19 vaccination data;
(j) evidence of pharmaceutical and other clinical treatments and supports.
COVID-19 is a pandemic disease
13. Section 3(5) of the Act provides that, for the purposes of this Act, an infectious disease is a
pandemic disease at a particular time if, at that time, there is a pandemic outbreak of that
infectious disease.
14. There has been a pandemic outbreak of SARS-Cov-2.
15. COVID-19 was first described in Wuhan, China, in December 2019. The formal designation
of this infectious disease in Victoria was initially 'Novel Coronavirus 2019 (2019-nCoV)'. The
virus which causes COVID-19 is now known internationally as SARS-CoV-2.
16. Since tracking commenced on 30 December 2020, the WHO Coronavirus dashboard
records 265,194,191 cases with 5,254,116 deaths as at 6 December 2021 6 (WHO(c)2021)
17. Since the first case was reported in Victoria on 25 January 2020 and 7 December 2021,
there have been 130,029 confirmed cases out of an Australian total of 219,118 and 1,385
deaths out of an Australian total of 2,056 (Australian Government Department of Health,
2021).
6 It is also important to consider that cases and adverse health outcomes may be under reported due to either localised low
testing rates or to differences in case ascertainment criteria, and that there may be variable delays to data reporting at state,
national and global levels. For example, case detection, inclusion criteria, testing strategies, reporting practices and data cut-off
and lag times may differ between countries, territories and areas, and some of these jurisdictions may report a combination of
probable and laboratory confirmed cases (WHO(a) 2021).
5
OFFICIAL: Sensitive18. Since the start of the pandemic, Victoria has recorded 4,964 outbreaks involving 34,078
confirmed cases.
19. As of 7 December 2021, Victoria has recorded 1,185 new locally acquired cases and 0 new
overseas acquired cases and 7 deaths within the past 24 hours. There are currently 13,050
active cases, of which 297 are in hospital, with 47 COVID-19 active patients receiving care
in intensive care units, of whom 25 are on ventilatory support.
20. As of 7 December 2021, the 7-day average case rate for Victoria is 124 cases per 100,000
population, which represents a 4.6% 7-day case growth rate compared to the preceding
week. The test positivity rate for the past 7 days is 1.8%, which indicates that there is
significant transmission of the virus in the community.
21. As of 5 December, Victoria has achieved 91.3% full vaccination coverage in those aged 12
years and over, and 93.4% single dose vaccination coverage in this demographic.
22. Across to the WHO Coronavirus data table, only seven countries have not officially recorded
a case of COVID-19 (WHO(c) 2021):
(a) Democratic People’s Republic of Korea, estimated population 25,369,000 (2016)
(b) Federal States of Micronesia, estimated population 105,000 (2016)
(c) Kiribati, estimated population 114,000 (2016)
(d) Nauru, estimated population 11,000 (2016)
(e) Niue, estimated population 2,000 (2016)
(f) Turkmenistan, estimated population 5,663,000 (2016)
(g) Tuvalu, estimated population 11,000 (2016).
23. SARS-CoV-2 has several characteristics that make COVID-19 a pandemic disease:
(a) SARS-CoV-2 is a novel infectious agent to which the global population had not been
exposed prior to late 2019 (and hence had not acquired resistance), meaning that
there was and continues to be significant immunological susceptibility for widespread
transmission.
(b) SARS-CoV-2 is highly transmissible and can spread easily from person to person
through multiple modes of transmission. More detail on this issue is set out in
paragraphs 24 to 28.
(c) SARS, like any virus, has the capacity to mutate into more transmissible and virulent
strains. More detail on this issue is set out in paragraphs 30 to 32.
6
OFFICIAL: Sensitive(d) Infection with SARS-CoV-2 can cause significant disease and death. More detail on this
issue is set out in paragraphs 34 to 38.
(e) The characteristics SARS-CoV-2 and the health effects of infection were largely
unknown, making control difficult. Evidence is still emerging about SARS-CoV-2 and
both the short and long-term effects of COVID-19 on the population.
(f) There are limited preventive and therapeutic interventions to manage COVID-19 (other
than vaccines, which are discussed in more detail below). A number of anti-viral, anti-
inflammatory and antibody therapies have now been granted provisional approval by the
Therapeutic Goods Administration (TGA), however many interventions against
COVID-19 remain supportive rather than curative or preventive.
24. SARS-CoV-2 is highly infectious. It is primarily transmitted from person to person through
respiratory droplets and aerosols carrying infectious viral particles that are inhaled or come
into contact with the mucous membranes in a person’s eyes, nose or mouth. Transmission
may also occur by touching contaminated surfaces and objects, known as fomites, and then
transferring infectious particles to the eyes, nose or mouth. However, the risk of fomite
transmission is much lower than that from droplet and aerosol transmission.
25. Respiratory droplets and aerosols are generated when the virus is expelled from an infected
person whilst talking, coughing, sneezing, shouting, singing or even breathing, and may
infect another person by being inhaled through the mouth or nose or inoculated directly onto
a susceptible person’s mucous membranes. Aerosols can be generated from the routine
behaviours outlined above, as well as by medical procedures, and can spread further than
droplets and remain in the air for longer. Transmission is more likely in enclosed, crowded
and poorly ventilated spaces, and where people cannot maintain physical distancing from
others. While SARS-CoV-2 transmission is far more common indoors, it may also occur
outdoors (Bulfone et al., 2021). These modes of transmission allow for rapid spread through
susceptible populations and are not comprehensively understood, making it challenging to
control the spread of the virus (WHO(d) 2021).
26. In addition, once a person is infected with SARS-CoV-2, certain characteristics of COVID-
19, such as its incubation period and infectious period, make it more difficult to control.
Cases can be infectious up to two days before the onset of symptoms and may be infectious
without ever developing symptoms (it is estimated that at least a third of cases remain
asymptomatic throughout their infection). Pre-symptomatic and asymptomatic cases can
unknowingly transmit infection (WHO 2020).
27. The incubation period varies between people. The median incubation period is 5 to 6 days
and ranges from 1 to 14 days. These features make it difficult to break chains of
7
OFFICIAL: Sensitivetransmission without stringent public health responses, as transmission may have already
occurred to contacts by the time a case develops symptoms and is diagnosed.
28. When determining how far a disease can spread in a population, epidemiologists use the
basic reproduction number (R0 ), which describes how many people each infected person will
infect on average, assuming that there is no pre-existing immunity in the community or other
intervention to stop the spread. It takes into account the duration of contagiousness of an
individual, the likelihood of infection in each contact between a susceptible person and an
infectious person or vector, and the frequency of contact. In contrast, the effective
reproduction number (Reff) refers to the number of people that can be infected by an
individual at any specific time and may be affected by the population becoming increasingly
immune either through natural infection or immunisation, and by mortality from the disease.
The Reff can also be affected by changes in peoples’ behaviour including social distancing
and other public health measures.
29. SARS-CoV-2 has an estimated R0 of around 2.63, however estimates can vary between 0.4
and 4.6 (Mahase 2020). The R0 for Delta VOC varies between 3.2 and 6 (Liu & Rocklöv
2021). By comparison, R0 for measles ranges from 12-18 (Guerra 2017), while the median R0
for seasonal influenza is 1.28 (Biggerstaff 2014).
30. The SARS‑CoV‑2 virus can mutate into potentially more transmissible, virulent, and difficult
to control variants (WHO(a) 2021), as the Delta VOC (B.1.617.2) demonstrates. Since its
initial detection in October 2020, it has gradually spread to become the dominant strain
globally. At the time of writing, all current cases of COVID-19 in Victoria with successful
genomic analysis are caused by Delta VOC, as well as 99.7% of all cases worldwide in the
60 days preceding 14 November 2021 (Agency for Clinical Innovation 2021).
31. There is now accepted evidence that the Delta VOC is more transmissible than ancestral
SARS-CoV-2 strains, as demonstrated by the higher secondary attack rate observed in both
household and non-household contacts of cases infected with the Delta variant. Additionally,
there is evidence that Delta may be more virulent than other strains, as evidenced by the
greater associated risk of hospitalisation, intensive care unit admission and death. According
to Public Health England (PHE) data, the Delta (B.1.617.2) VOC is estimated to be 40 per
cent more transmissible than the Alpha (B.1.17) VOC, which is itself approximately 50 per
cent more transmissible than the ancestral Wuhan strain of SARS-CoV-2. When compared to
the Alpha strain, infection with Delta is almost twice as likely to result in hospitalisation and
almost three times as likely to result in ICU admission (Agency for Clinical Innovation 2021).
32. Most recently, the WHO newly designated the Omicron (B.1.1.529) strain as a VOC on 26
November, just two days after it being initially reported. Omicron was first detected in
samples collected on 11 November 2021 in Botswana, and subsequently in samples
8
OFFICIAL: Sensitivecollected from 14 November and onward in South Africa. This strain is of concern due to its
multiple mutations, some of which affect the spike protein, which is a key immunological
target against the virus, and due to the coinciding surge in cases reported in South Africa
following its detection. Although the impact of these mutations on its transmissibility,
virulence and its capacity to evade host immune responses is not yet comprehensively
understood, preliminary evidence suggests an increased risk of re-infection associated with
this variant (WHO (b) 2021). As of 6 December 2021, Omicron cases have already been
identified in Australia and in 45 other countries across the world.
COVID-19 is a serious risk to public health
33. Section 165AB of the Act provides that the Premier may make a declaration if the Premier is
satisfied that a pandemic disease constitutes “serious risk to public health”. As noted above,
section 3 of the Act defines the phrase “serious risk to public health” as:
a material risk that substantial injury or prejudice to the health of human beings has
occurred or may occur having regard to:
(a) the number of persons likely to be affected; the location, immediacy, and
seriousness of the threat to the health of persons;
(b) the nature, scale and effects of the harm, illness or injury that may develop; and
(c) the availability and effectiveness of any precaution, safeguard, treatment, or other
measure to eliminate or reduce the risk to the health of human beings.
This section addresses these issues.
COVID-19 has potential to cause widespread harm to many people
34. The number of persons likely to be affected, the location, immediacy, the seriousness of the
threat to the health of persons, and the nature, scale and effects of the harm, illness or injury
that may develop are linked, as past experiences illustrate future risk. On this basis, I will
deal with these issues together.
35. The clinical spectrum of COVID-19 infection ranges from asymptomatic infection and mild
respiratory symptoms through to severe illness that requires hospitalisation and may result
in death. Vulnerable members of society, including the elderly, those with co-existing
medical conditions (including hypertension, cardiovascular disease, respiratory disease,
renal disease and malignancy) and those in lower socioeconomic groups, have been shown
to be disproportionately impacted and remain at risk (Taylor et al. 2021).
36. Estimates from published literature and epidemiological sources indicate the case fatality
rate for COVID-19 varies and can depend on the degree to which all cases of COVID-19
9
OFFICIAL: SensitiveYou can also read