Protocol on Assessment of Bruising and Injuries in Non-Mobile Infants and Children - www.bromleysafeguarding.org - Inzu
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Protocol on Assessment of Bruising and Injuries in
Non-Mobile Infants and Children
www.bromleysafeguarding.org
PAGE
1Contents
Page
1. Introduction 3
2. Evidence base 3
3. Initial Response on Identifying an Injury or 4
Bruise
4. Referral to Children’s Social Care 5
5 Outcome of Child Protection Medical 5
Examination
6. Flowchart for assessing injuries or bruises 7
Ratified: August 2021
For Review: August 2024
PAGE
2Bromley Safeguarding Children Partnership
Protocol on Assessment of Bruising and Injuries in Non-Mobile
Infants and Children
1. Introduction
Bruising and injuries in non-mobile children are rare; therefore, there is a significant
risk that this may indicate physical abuse or neglect. Non-mobile infants and disabled
children are extremely unlikely to have accidental injuries as they have limited
independent mobility and are also more vulnerable as they are unable to verbally
communicate their experiences. Any injuries in non-mobile babies and children,
however minor, are a cause for concern including bruising, fractures, bleeding or burns
and require a safeguarding assessment.
A simple bruise may be the hallmark of a non-mobile child who has sustained
significant internal injuries such as fractures, eye, brain trauma and intra-abdominal
injuries. Serious Case Reviews document many cases where bruising was not
responded to appropriately by Health and Social Care staff, resulting in children being
left at risk, sustaining further injuries with serious harm or death.
This protocol is to ensure that bruising and injuries in non-mobile infants and children
are referred to Children’s Social Care and assessed by Paediatricians. For clarity a
non-mobile/not independently mobile baby or child with a disability may be able to roll
or sit independently, but are not crawling, bottom shuffling, pulling to stand, cruising
or walking independently. (Injuries and bruising in mobile children will also need
careful consideration under the usual safeguarding policies).
2. Evidence base
Bruises in Infants and Toddlers - “those who do not cruise rarely bruise” is one of the
earliest pieces of prevalence evidence from 1999 identifying that bruises are rare in
non-mobile children and children under nine months which should be assessed for
abuse as a cause. 1
NICE guidance: Child maltreatment: when to suspect maltreatment in under 18s
updated 2017 states:
Suspect child maltreatment if there is bruising or petechiae (tiny red or purple spots)
…. Examples include bruising in a child who is not independently mobile 2
RCPCH Child Protection Evidence Systematic review on Bruising updated 2020
states: Research shows that it is very unusual for pre-mobile babies to sustain bruises
accidentally and bruising in this age group raises significant concerns about physical
abuse. Young babies and infants are extremely vulnerable and at greatest risk of death
or severe injury with significant associated mortality in physical abuse. Bruising is also
a widely reported “sentinel” injury in babies and younger and its recognition is vital in
prevention of more severe abuse. 3
1
JAMA Pediatrics 1999 Bruises in Infants and Toddlers: Those Who Don't Cruise Rarely Bruise
2
NICE Guidance 2017 Overview | Child maltreatment: when to suspect maltreatment in under 18s
3
RCPCH 2020 Child Protection Evidence- Systematic Review on Bruising
PAGE
33. Initial Response on Identifying an Injury or Bruise
Professionals observing any injury including bruising on a non-mobile baby or child
must suspect nonaccidental injury. The professional must ask for further information
and details of the history, timeline, and any explanation. These should be recorded
directly into the child record together with a body map.
Any injuries are significant in this group and even small injuries may be significant:
• Single or multiple bruises on any site
• Cut, grazes or scars
• Bite marks
• Burns and scalds
• Bleeding from ear, nose, or throat
• Pain, tenderness, or reluctance to move an arm or a leg (which may suggest
pain from underlying fracture)
• Injuries to the eye or bleeding in the white of the eyes
• Torn frenulum (web of skin joining the upper and lower lip to the gum in the
midline of the mouth)
• Single scratches may be innocent, such as caused by the child’s fingernails,
however multiple or deep scratches are of concern
An immediate referral to MASH Children’s Social Care should be made which will
result in arrangements for paediatric assessment (which would be at the hospital for
children under two years, and at the Phoenix Centre for children over two years). There
is a need for an urgent assessment, although a small percentage of bruising in non-
mobile children will have an innocent explanation.
If a child is seriously injured, they should be taken to the hospital urgently, usually by
ambulance, and should be referred directly by the concerned professional to the on
call Paediatric Specialist Registrar or Consultant at Princess Royal University Hospital
(PRUH) via switchboard on 01689 863000 regardless of what time of the day they
present. The referral to MASH Children’s Social Care can be made simultaneously.
It is the responsibility of the acute or community paediatricians to assess and decide
whether the cause may be innocent or due to maltreatment, referring to Children’s
Social Care as appropriate. Children should not be referred to GPs for an opinion or
decision on injuries as they are not trained for this level of assessment.
Rarely there may be a medical cause such as associated with documented birth injury
or medical processes in the neonatal period. Health professionals with experience and
training who can evidence that the bruise or injury is not a cause for concern, using
access to records etc, should discuss this with peers and in this very limited situation
may use professional judgement not to refer an injury and document this decision in
the records this.
PAGE
4On occasions, it may be difficult to know if a skin finding may be innocent such as a
Mongolian blue spot or haemangioma. In this situation the child should be reviewed
without delay by a health professional with training and experiencing in assessing this
such as the GP or a Paediatrician and some Health Visitors. If this opinion is not readily
available (i.e. Immediately available in the same building), then the child should be
referred to MASH Children’s Social Care in order to access a paediatric assessment.
If there is any doubt whether this may be an innocent birthmark, there should be an
immediate referral to MASH.
Suggestions that a non-mobile infant has injured themselves should not be accepted
without a referral to Children’s Social Care and detailed assessment by a
paediatrician. Additionally, suggestions that a non-mobile infant has been injured by a
sibling is unusual but occasionally can happen, however physical abuse will need to
be investigated. In these circumstances there should still be a referral to MASH
Children’s Social Care for paediatric assessment, and assessment of the social
situation and parental ability to supervise children.
4. Referral to Children’s Social Care
There should be an immediate phone referral to MASH confirmed by referral form sent
by email preferably on the same day and certainly within 24 hours. This will result in a
strategy discussion and arrangement of an urgent paediatric assessment. For children
under two years of age, Children’s Social Care will contact the on-call Paediatric
Specialist Registrar or Consultant at Princess Royal University Hospital (PRUH). The
Social Worker must accompany the child to Accident and Emergency with a parent or
carer. For children over two years of age Children’s Social Care will contact the
community paediatricians at the Phoenix centre.
Parents and carers should be involved in the decision-making where possible; the
professional should explain why bruises and injuries in non-mobile children must be
formally assessed and referred to Children’s Social Care. A copy of the leaflet
explaining the local processes should be given to parents and carers, this is available
on the Bromley Safeguarding Children Partnership website. 4
If parents are not cooperative or refuse then Children’s Social Care should be
contacted immediately and where possible the child kept under supervision until their
safety can be assured. If the child’s safety cannot be secured, it may be necessary to
contact the police.
4
LINK to BSCP website for information leaflet http://www.bromleysafeguarding.org/articles.php?id=609
PAGE
55. Outcome of Child Protection Medical Examination
The Child Protection Medical Examination will be carried out by a suitably qualified
hospital or community paediatrician. The assessment will take into account the context
of medical and social history, developmental stage, explanation given, full clinical
examination and relevant investigations. Further medical investigations will be carried
out if there is evidence of significant injury which may include a skeletal survey, CT
brain scan, retinal assessment, and blood clotting testing under national guidance. 5 6
• If the medical examination concludes there is evidence of nonaccidental injury,
Children’s Social Care should be informed of this outcome on the same day in
order to carry out a section 47 investigation
• If the medical examination is inconclusive, or there are concerns about the
cause of the bruise or injury, Children’s Social Care should convene a
multiagency Strategy Discussion to consider any further investigations and how
to safeguard the child and any other children.
• If the medical examination concludes the injury has a medical explanation, is
accidental or consistent with the explanation, this should be discussed with
Children’s Social Care who will consider if any further intervention or support is
required.
• Where a child is admitted to hospital, there will need to be a multiagency
decision about supervision of the parental access to the child and how contact
will be managed.
• Where there is any professional disagreement about how to respond to bruising
and injuries in a non-mobile child, this should be referred to senior managers
using the Bromley Safeguarding Children Partnership escalation policy.
• If there is concern about significant injury to the index case, arrangements
should be made for other siblings/ children living in the same household under
the age of two years to have the same recommended imaging as the index
case, all siblings under the age of four years to have a Child Protection Medical
Assessment, and for older children to be interviewed and examined if they
disclose physical abuse.
• Where there is evidence of nonaccidental injury, or inconclusive findings, there
will need to be a multiagency discussion prior to discharge to discuss how to
safeguard the child, including supervision and access /contact arrangements
with parents, carers or others who may be of risk to the child, particularly while
further police and social care investigations are carried out.
5
RCR RCPCH 2018 The radiological investigation of suspected physical abuse in children
6
NICE 2009 When to suspect child maltreatment
PAGE
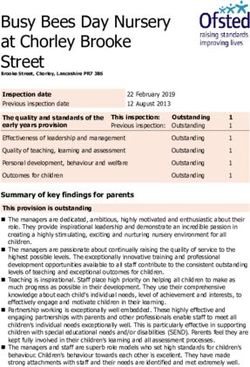
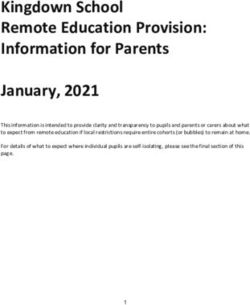
6BROMLEY SAFEGUARDING PARTNERSHIP PROTOCOL FOR
ASSESSMENT OF INJURIES IN NON-MOBILE CHILDREN
Professional observes an
BRUISE, INJURY or SUSPICIOUS MARK
YOU MUST SUSPECT CHILD MALTREATMENT
Is the child seriously ill / need emergency medical treatment?
YES NO
A child who is seriously Seek an explanation, examine (within
ill should be referred your limits) and record accurately. This
immediately should include details of social history
to hospital and including other children, carers and
CONTACT POLICE ‘significant others’
Explain to carers (if no safety risk), the reason for immediate
referral to Children’s Social Care (CSC) and Paediatrics
Refer child immediately to Children’s Social Care
Use Bromley Safeguarding Children’s Partnership Child Protection
Procedures @ bromleysafeguarding.org
Bromley MASH Tel: 0208 461 7364 / 7379 (Mon-Fri 9am-5pm)
Emergency Duty Team (Out of Hours & Weekends)
Tel: 0300 303 8671 Email: mash@bromley.gov.uk
If 2 years and under refer to On-Call Paediatric team:
Bromley - PRUH 01689 863000
Bexley - Darent Valley Hospital via switchboard 01322 428100
Bexley - Queen Elizabeth Hospital 0208 836 6000
Definitions: A Non-Mobile / Non-Independently Mobile infant or child may be able
to sit or roll but are not yet crawling, shuffling, pulling to stand, cruising or walking
independently. This guidance also applies to older immobile children for example
immobility due to disability or illness.
PAGE
7www.bromleysafeguarding.org
PAGE
8You can also read