Post IAS 2021 Les complications métaboliques (incluant le gain pondéral) et les comorbidités - Jean-Guy Baril
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Post IAS 2021 Les complications métaboliques (incluant le gain pondéral) et les comorbidités Jean-Guy Baril
2
Conflits d’intérêts potentiels
Consultant ponctuel, ou conférencier lors d'activités supportées par les compagnies suivantes:
– ViiV healthcare, Merck et Gilead.
Membre d’institutions (CRCHUM, FRSQ, Clinique du Quartier latin) ayant reçu des fonds de recherche de:
– Glaxo Smith Kline, ViiV healthcare, Merck et Gilead.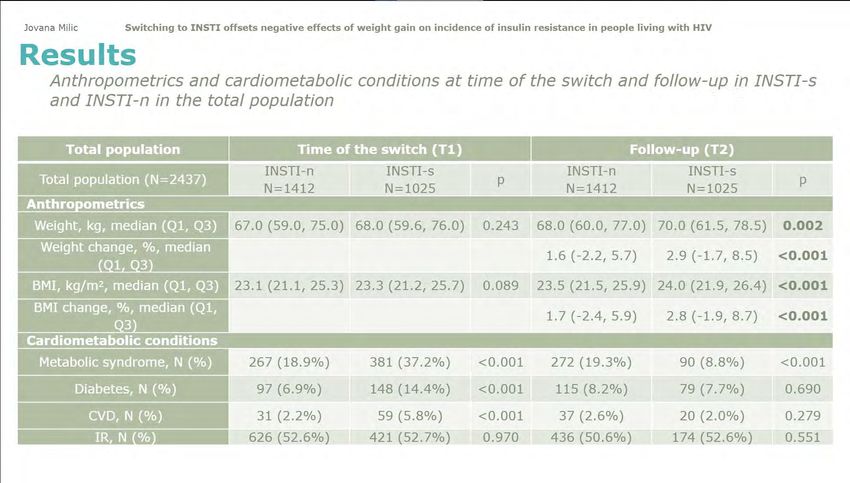
Introduction
Les nouveaux régimes thérapeutiques à base de TAF ou
d’INSTI ont été associés à un gain de poids et à l’obésité
Ce gain de poids pourrait être associé à un risque accru de
complications métaboliques comme le diabète,
l’hypertension et les maladies cardiovasculaires
Ce risque accru pourrait réduire les bénéfices associés aux
nouveaux traitements
3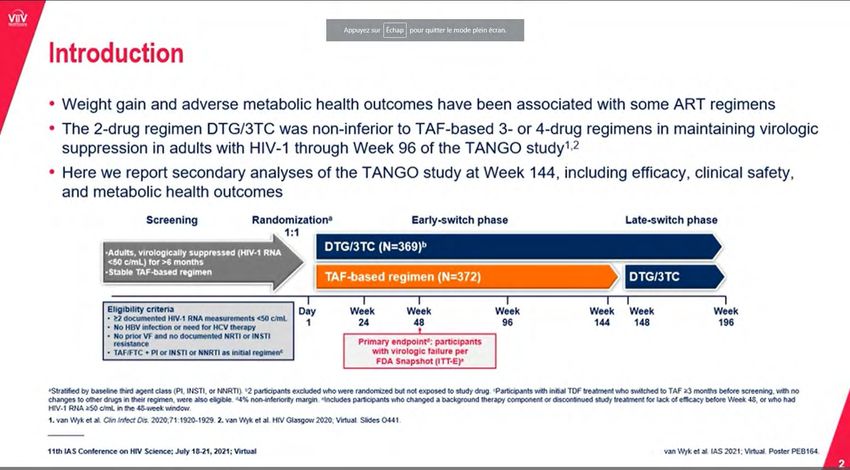
ADVANCE: DTG + FTC/TAF, DTG + FTC/TDF or EFV/FTC/TDF (South Africa) ‡
Changes in Body Weight
Mean Change in Weight (kg) in Men Mean Change in Weight (kg) in Women
12 12
TAF/FTC+DTG TDF/FTC+DTG TDF/FTC/EFV TAF/FTC+DTG TDF/FTC+DTG TDF/FTC/EFV
Mean Weight Change (kg)
Mean Weight Change (kg)
10 10
+9 kg
8 8
+6 kg
6 6
+5 kg +6 kg
+5 kg
4 4 +3 kg
+3 kg
+3 kg +3 kg
2 2
+0.5 kg +1 kg +2 kg
0 0
0
-2 0 4 12 24 36 48 60 72 84 96 0
-2 0 4 12 24 36 48 60 72 84 96
Week Week
n= 430 418 403 387 376 374 369 356 308 243 n= 622 604 586 561 546 530 516 509 439 347
DTG was associated with increases in body weight in both men and women vs EFV.
Increases in weight with DTG were higher in women when used with FTC/TAF, but not in men.
For this analysis, only 55% of study population had reached W96.
McCann K, et al. EACS 2019. Basel, Switzerland. Oral PS3/3 Venter W, et al. N Engl J Med 2019; epub July 24 and supplementary appendix 4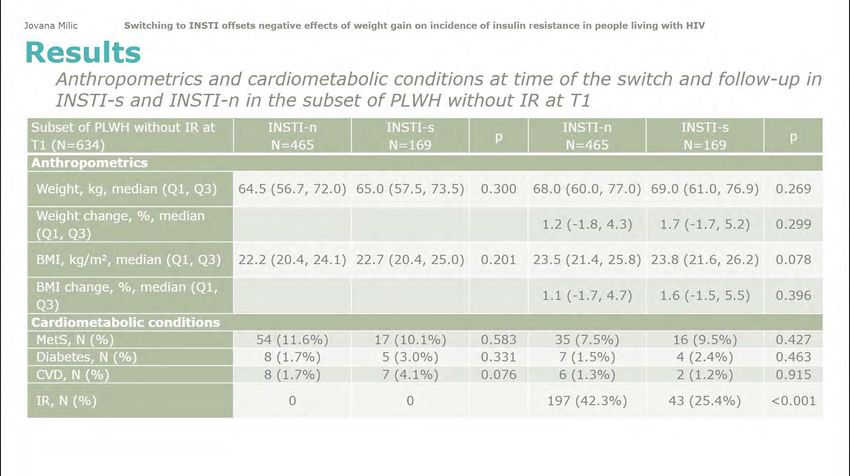
Questions relatives au gain de poids chez les VIH + Est-ce un retour à la santé? – Comparaison des populations VIH+ avec les populations VIH- Est-ce relié à l’arrêt des médicaments qui ont un effet négatif sur le poids (weight supresssive treatment) ? – Études de substitution de traitement Quelles sont les conséquences cliniques du gain pondéral ? – Association avec le syndrome métabolique
Questions relatives au gain de poids chez les VIH + Est-ce un retour à la santé? – Comparaison des populations VIH+ avec les populations VIH- Est-ce relié à l’arrêt des médicaments qui ont un effet négatifs sur le poids (weight supresssive treatment) ? – Études de substitution de traitement Quelles sont les conséquences cliniques du gain pondéral ? – Association avec le syndrome métabolique
Obesity, raised blood pressure and diabetes in women with and without HIV: a
pooled analysis of 17,450 women in four countries in sub-Saharan Africa
De Vlieg R.
7
Obesity, raised blood pressure and diabetes in women with and without HIV: a
pooled analysis of 17,450 women in four countries in sub-Saharan Africa:
Rebecca A. de Vlieg
8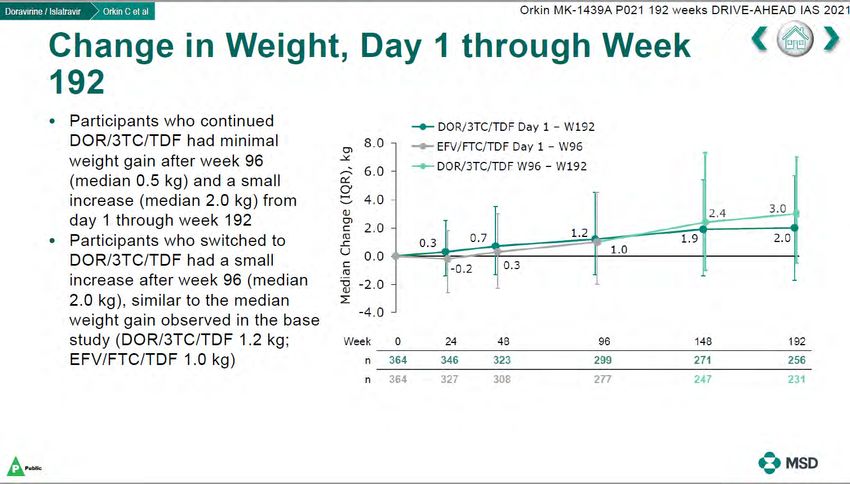
Obesity, raised blood pressure and diabetes in women with and without HIV: a
pooled analysis of 17,450 women in four countries in sub-Saharan Africa
De Vlieg R.
In multivariable models, WLHIV had CONCLUSIONS:
– a lower odds of overweight/obesity [AOR=0.62 WLHIV in SSA had high rates of
(0.55-0.71)], overweight/obesity and hypertension prior to
– but without significant difference in the odds of the switch to new generation ART.
raised BP [AOR:0.90 (0.78-1.04)] or
HIV is still associated with a lower BMI,
DM [AOR:0.75 (0.44-1.02)].
however, this gap seems to be narrowing
with high rates of overweight/obesity in
WLHIV.
Future research should focus on
approaches to prevent weight gain and its
associated cardiovascular risk factors.
9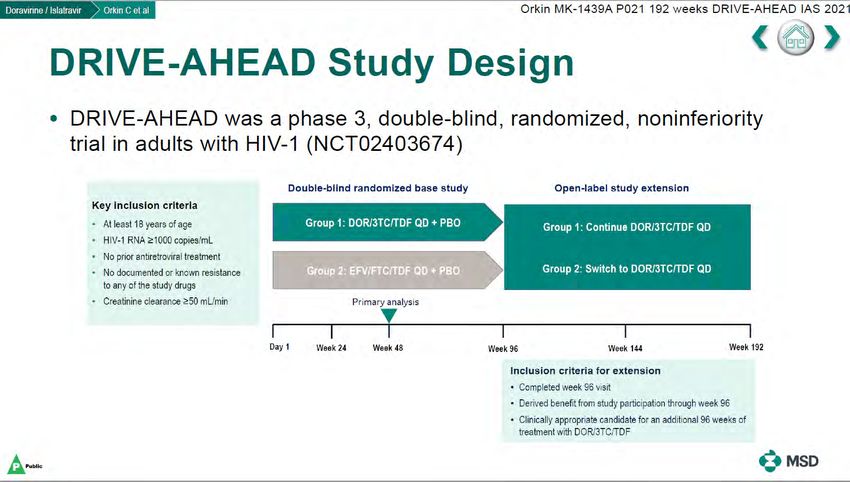
Weight gain or “return to health”? - Changes in body weight in aging people living
with HIV compared with the general population from the German Ruhr-area over
5 years L. Mavarani (appariés pour age et sexe)
10Questions relatives au gain de poids chez les VIH + Est-ce un retour à la santé? – Comparaison des populations VIH+ avec les populations VIH- Est-ce relié à l’arrêt des médicaments qui ont un effet négatifs sur le poids (weight supresssive treatment) ? – Études de substitution de traitement Existe-t-il un effet indépendant du f TAF ? Ou des INSTIs ? Et quelles sont les conséquences cliniques du gain pondéral ? – Association avec le syndrome métabolique
Effet de TDF à long terme avec EFV ou DOR
12Effet de TDF à long terme avec EFV ou DOR
13HIV Treatment TDF→TAF
Dat’AIDS: Retrospective, Multicenter Cohort (France)
Impact of Switch From TDF to TAF on Weight of Virologically Suppressed PLWH
Outcomes Jan 2014–
Virologically N=587 R/F/TDF R/F/TAF
suppressed E/C/F/TDF E/C/F/TAF
Mean weight and BMI during 12 months before Dec 2019
N=597
and after switch
Factors Associated with Weight Change 6- to 12-months Impact of TDF-to-TAF Switch, by Sex and Race/Origin1*
after switch from TDF to TAF (Multivariate Model)1
All Caucasian African origin
PDISCOVER: Week 48 Open-Label Phase
‡
Study Design
Primary Week 96 Current analysis:
Week 0 analysis analysis W 48 OL
F/TAF 200/25 mg qd
Randomized Primary analysis:
N=2694
1:1
MSM or TGW F/TAF HIV incidence/100 PY when
Adults ≥18 y Double blinded, open-label option 100% complete Week 48
active controlled F/TDF 200/300 mg qd & 50% complete Week 96
N=2693
Week 96 analysis:
Eligibility: high sexual risk of HIV acquisition 100% complete Week 96
2+ episodes condomless anal sex in past 12W or rectal gonorrhea/chlamydia, or syphilis in past 24W
HIV & HBV negative, eGFRCG ≥60 mL/min
Current analysis:
Prior use of PrEP allowed Week 48 OL Phase
Study conducted in Europe, North America in cities/sites with high HIV incidence
Assessments
Safety (AEs, AE-related discontinuation, BMD, renal biomarkers)
Adherence (self-report, pill counts, drug levels and DBS)
HIV lab testing (rapid HIV testing on-site, Central lab)
HIV risk behavior (confidential CASI questionnaire, STI assessment at every visit [GC/CT: rectum, urethra, oropharynx (NAAT) and syphilis testing])
At EOBP, participants had the option to receive F/TAF in the OL phase
AE, adverse event; BMD, bone mineral density; CASI, computer-aided self-interview; DBS, dried blood spots; DXA, dual energy X-ray absorptiometry; eGFRCG, estimated glomerular filtration rate by Cockcroft-
Gault; GC/CT, gonococcus/chlamydia trachomatis; NAAT, nucleic acid amplification test; PY, person-year; STI, sexually transmitted infection; OL, open label; EOBP, end of blinded phase. 16
Spinner C, et al. vIAS 2021. Oral OALC0501DISCOVER: Week 48 Open-Label Phase
‡
Changes in Fasting Lipids, Glucose, and Weight
Stay on F/TAF F/TDF→F/TAF
Total LDL HDL Total
Weight
Cholesterol Cholesterol Cholesterol Triglycerides Fasting Glucose Cholesterol:HDL PBRAAVE 2020: Switch to B/F/TAF in Suppressed African American Adults – Week 72 (NCT03631732) ‡
B/F/TAF in Virologically Suppressed African-American PLWH
Phase 3b, randomized, open label, multicenter, active-controlled study
1° Endpoint 2° Endpoint 2° Endpoint
Week 0 24 48 72
HIV Suppressed Black Adults on
n=330
2 NRTIs + 3rd agent* Switch to B/F/TAF QD
Self describes as Black, AA or mixed race, 2:1
including Black
Stay on baseline Delayed Switch
Suppressed ≥ 6 months
n=165 regimen (SBR) B/F/TAF QD
eGFRCG ≥ 50 mL/min
Primary Endpoints
• HIV-1 RNA ≥50 c/mL at Week 24 by FDA snapshot ARV Resistance Criteria at Baseline
Excluded Allowed
Secondary Endpoints
• HIV-1 RNABRAAVE 2020: Switch to B/F/TAF in Black American Adults, W72 (End of Study) ‡
Baseline Characteristics
ART Regimens at Baseline by Treatment Group
B/F/TAF SBR
n=330 n=165
B/F/TAF SBR
Age, years 49 (18–79) 49 (19–70)
Female at birth, % 31 33
1 15 F/TAF
Hispanic/Latinx, % 5 3 13 F/TDF
Weight, kg 88 (79, 103) 89 (76, 104) NRTI ABC/3TC
17 Other
backbone 21 65
HBV co-infection, % 5 2 68
747 758
CD4 count, cells/μL
(570, 922) (494, 969)
EVG/c
110 107 8 DTG
eGFRCG, mL/min 5 7 5
(88, 132) (86, 132) RPV
10 13 35 EFV
ARV resistance, %† Third 38
DRV/c
NRTI resistance 13 16 agent or DRV/r
M184V/I 9 12 19 16 Other
NNRTI resistance 21 19 24
20
PI resistance 11 15
NOTE. Median (Q1, Q3), except for age median (range)
Baseline characteristics were well balanced between the two groups
†Assessed by cumulative historical or retrospective baseline proviral DNA genotypes
CD4, cluster of differentiation 4; eGFRCG, estimated glomerular filtration rate by Cockcroft-Gault equation; Q, Quartile; SBR, stay on baseline regimen
Kumar P, et al. vIAS 2021, PEB161; Hagins D, et al. CROI 2020, Oral 2979 19BRAAVE 2020: Switch to B/F/TAF in Suppressed African American Adults – Week 72 (NCT03631732) ‡
Fasting Lipid and Weight Changes from Baseline at Week 72
B/F/TAF (Week 72) Delayed switch to B/F/TAF (48 weeks after switch)
15 TC LDL HDL TG 1,5 TC:HDL Weight (All B/F/TAF)
Median Change From Baseline
Median Weight Change
From BL, kg (Q1, Q3)
From Baseline, mg/dL*
10 1
Median Change
5 0,5 0, 0,
1 1 1
0 0
-2 -0,5
-5 -3 -3 -3 -3
-4
-10 -1
-9
-15 -1,5
BL, mg/dL 181 169 111 102 54 53 98 95 3.3 3.1 B/F/TAF: n= 330 320 315 229
Delayed switch: n= 163 158 119
Small reductions from baseline in cholesterol fractions and triglycerides
with stable weight through 72 weeks in African American men and women
*Baseline is median value at time of 1st B/F/TAF dose
TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglycerides
20
Kumar P, et al. vIAS 2021. PEB161BRAAVE 2020: Switch to B/F/TAF in Suppressed African American Adults – Week 72 (NCT03631732) ‡
Weight Changes through Week 72 (by sex at birth)
B/F/TAF SBR Delayed switch to B/F/TAF (through 48 weeks after switch)*
5 Female 5 Male
Median Weight Change From Baseline,
4 4 p=0.56†
p=0.027†
3 3
1.4
2 2 1.9
kg (Q1, Q3)
1.2 1.7 0.8
0.9
1 1.3 1 0.7
1.0 0.5
0 0 0.5
-0.4
-1 -1
-2 -2
-3 -3
0 12 24 36 48 60 72 0 12 24 36 48 60 72
Week Week
B/F/TAF: n= 101 101 99 98 98 84 79 229 224 221 220 217 193 150
SBR: n= 55 54 55 110 109 109
Delayed switch: n= 55 53 51 49 37 108 106 107 100 82
Weight changes were similar between African American men and women
*Baseline for delayed switch: time of 1st B/F/TAF dose; †From 2-sided Wilcoxon rank-sum test comparing B/F/TAF vs SBR at Week 24. 21
Kumar P, et al. vIAS 2021. Poster #PEB161BRAAVE 2020: Switch to B/F/TAF in Suppressed African American Adults – Week 72 (NCT03631732) ‡
Weight Changes through Week 72
By Baseline NRTIs
SBR Switch to B/F/TAF from a regimen containing: TAF TDF ABC
9 9
Median Weight Change From Baseline,
SBR vs B/F/TAF Delayed Switch*
6 p=0.012† 6
4.6
kg (Q1, Q3)
p=0.84†
3 2.8 3
1.4 TDF
1.3 1.3 ABC
0.2 0.7 TAF
0 0
-3 -3
0 12 24 36 48 60 72 0 12 24 36 48
Week Week
TAF: n=224 222 218 217 217 186 164 106 105 104 98 83
TDF: n= 57 56 56 55 54 51 37 33 33 33 31 21
ABC: n= 44 43 42 42 40 36 26 24 21 21 20 15
More weight gain was observed in participants switching from TDF- and ABC-containing
regimens compared to those with TAF in their baseline regimen 22
*Baseline for delayed switch: time of 1st B/F/TAF dose; †From 2-sided Wilcoxon rank-sum test comparing baseline regimens containing TAF vs TDF and ABC.
Kumar P, et al. vIAS 2021. Poster #PEB161HIV Treatment TAF
TANGO: Phase 3, Randomized, Open-label, Multicenter, Noninferiority Study
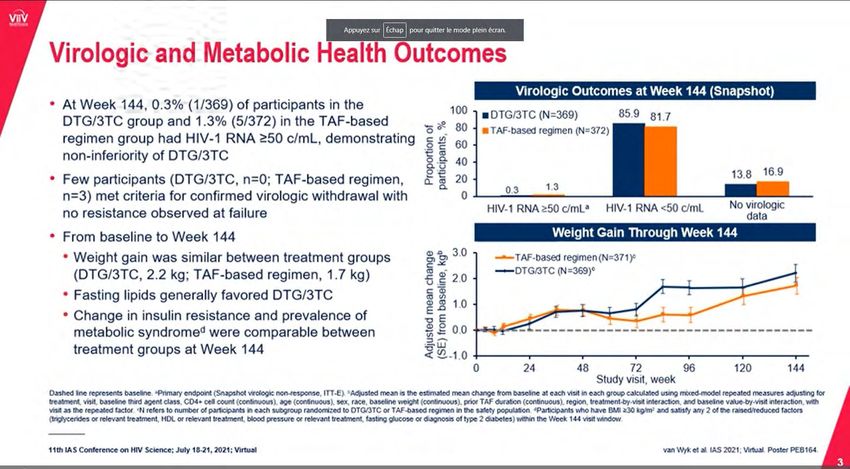
DTG/3TC vs. TAF-based Regimen in PLWH:
Metabolic Health Outcomes at Week 144 (2 of 2)
Change in HOMA-IR From BL to Week 144* Change in Fasting Lipids From BL to Week 144*
TAF-based regimen† (n=371) TAF-based regimen (n=230) †
DTG/3TC (n=369) DTG/3TC (n=243)
-7.2 -6.1 -7.2 -11.7
1.20 (-9.6, -4.8) (-9.1, -2.9) (-10.8, -3.6) (-18.1, -4.7) -1.2
Estimated adjusted ratio of
10 (-4.7, 2.4)
2.2
Adjusted change from BL
1.15 11.0% 3.9 4.6
4.2
visit over BL (95% CI)
5
1.10 11.2% 0.3
(95% CI), %‡
1.05 0
1.00 -5 -0.9
-3.3 -2.4 -3.0
0.95 -10
0.90
-15 -9.7
0.85
-20
0.80 BL 5.0 4.9 1.3 1.3 2.9 2.8 1.3 1.2 3.7 3.6
0 24 48 72 96 120 144
TC HDL-C LDL-C TG TC:HDL
Weeks (mmol/L) (mmol/L) (mmol/L) (mmol/L)
Participants with Metabolic Syndrome, W144: Initiated Lipid-Lowering Agents through W144:
15% DTG/3TC vs. 16% TAF-based group 12% DTG/3TC vs. 11% TAF-based group
After 3 years, switching to DTG/3TC didn’t lead to better metabolic outcomes (insulin resistance, metabolic
Change from baseline was calculated using mixed-model repeated measures applied to change from baseline in log-transformed data with multiple adjustments for treatment, visit, baseline third agent class, CD4, age, sex,
syndrome, use of lipid-lowering agents) compared with continuing on baseline TAF-based regimens
race, BMI (and presence of hypertension for HOMA-IR).
*Change from baseline was calculated using mixed-model repeated measures applied to change from baseline in log-transformed data with multiple adjustments for treatment, visit, baseline third agent class, CD4, age, sex,
race, BMI (and presence of hypertension for HOMA-IR); † the TANGO study included only individuals treated with TAF-based regimens, mostly EVG/c/FTC/TAF or RPV/FTC/TAF; ‡n=342 for both groups
BL, baseline; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment for insulin resistance; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides
van Wyk J, et al. vIAS 2021, PEB164 27HIV Treatment DTG/3TC
SALSA: Global, Randomized, Controlled, Open-Label Study
Switching to DTG/3TC vs. Continuing Current ART in PLWH (1 of 2)
N=493
virologically suppressed PLWH; Switched to DTG/3TC FDC (n=246) Outcome
no prior VF or documented Remained on current ART* (n=247) HIV-1 RNA ≥50 c/mL at Week 48 (FDA Snapshot)
NRTI/INSTI resistance
DTG/3TC CAR
Baseline Antiretrovirals, n (%)
(n=246) (n=247)
Virologic Outcomes at Week 48 (Snapshot Analysis) Baseline third agent class
INSTI 98 (40) 98 (40)
NNRTI 123 (50) 124 (50)
100 94 93 PI 25 (10) 25 (10)
DTG/3TC (n=246) Baseline NRTIs in ≥30% participants
FTC 149 (61) 156 (63)
80 CAR (n=247)
Individuals, %
TDF 109 (44) 109(44)
3TC 96 (39) 89 (36)
60 TAF 83 (34) 91 (37)
40
DTG/3TC CAR
Adverse Events Through W48, n (%)
(n=246) (n=247)
20 DRAEs 48 (20) 16 (6)
5 6 Weight increase 14 (6) 0HIV Treatment DTG/3TC
SALSA: Global, Randomized, Controlled, Open-Label Study ‡
Switching to DTG/3TC vs. Continuing Current ART in PLWH (2 of 2)
Adjusted Mean Weight Change From Adjusted Mean Change in BMI From
Baseline to Week 48 Baseline to Week 48
3 2
Change in weight, kg
Change in BMI, kg/m2
2,5
+2.1 1,5
2
1,5 1
+0.7
1
+0.6 0,5
0,5 +0.2
0 0
DTG/3TC CAR DTG/3TC CAR
Median weight (kg) at baseline (range) Median BMI (kg/m2) at baseline (range)
DTG/3TC (n=246) 73 (43–154) DTG/3TC (n=246) 25 (17–51)
CAR (n=247) 75 (36–160) CAR (n=247) 26 (14–69)
After 48 weeks, there was a higher mean weight and BMI increase with DTG/3TC
CAR, current ART regimen
Llibre J, et al. vIAS 2021, OALB0303 29Questions relatives au gain de poids chez les VIH + Est-ce un retour à la santé? – Comparaison des populations VIH+ avec les populations VIH- Est-ce relié à l’arrêt des médicaments qui ont un effet négatifs sur le poids (weight supresssive treatment) ? – Études de substitution de traitement Quelles sont les conséquences cliniques du gain pondéral ? – Association avec le syndrome métabolique
Comorbidities
UK Matched Cohort Study (THIN)
Risk of CVD in PLWH
PLWH ≥18 yrs., N=9,233 PLWH
matched HIV-neg Outcomes Jan 1, 2000–
controls (1:4 ratio) N=35,721 Matched Controls Risk of composite CVD* in PLWH Jan 1, 2020
Composite CVD Risk
54% increased risk of composite CVD in Male
PLWH vs. Controls Female
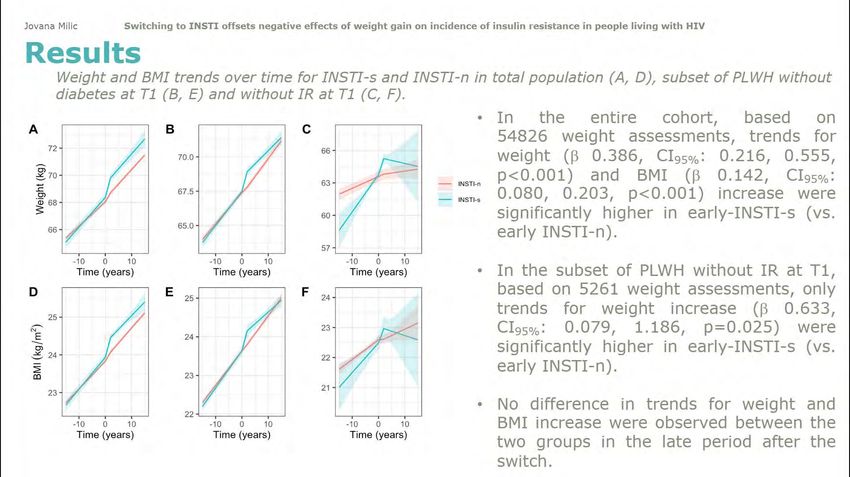
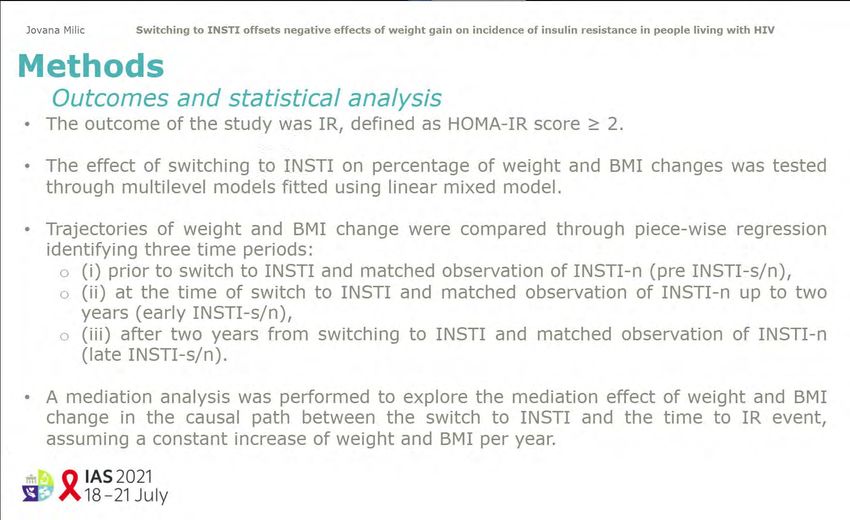
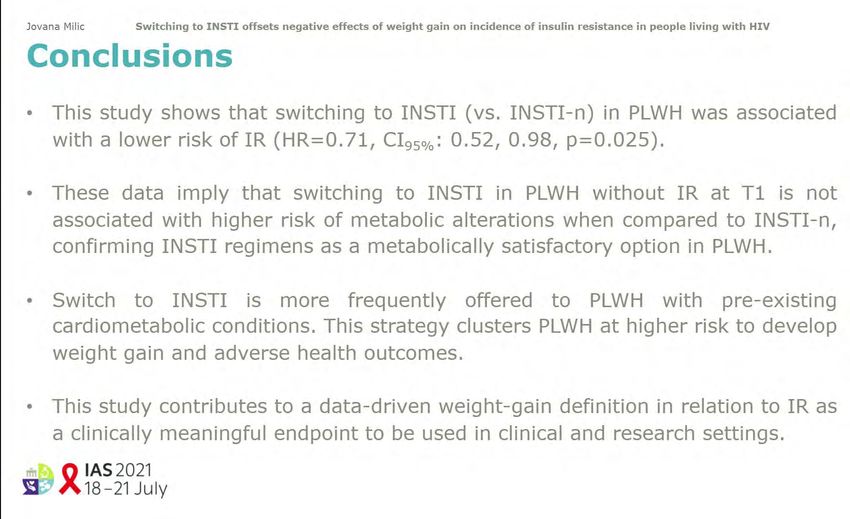
HR: 1.54; 95% CI: 1.3–1.83Switch to INSTI more than offset negative effects of weight gain on
incidence of insulin resistance in people living with HIV
33Switch to INSTI more than offset negative effects of weight gain on
incidence of insulin resistance in people living with HIV
39Does weight gain on Bictegravir/Emtricitabine/Tenofovir Alafenamide (B) lead to metabolic syndrome? Presenter: Jihad Slim Study Design Methods A single centre retrospective cohort study on We stratified the cohort into 2 groups: all patients living with HIV (PLWH) at our – those that gained ≥10% weight, and
Does weight gain on Bictegravir/Emtricitabine/Tenofovir Alafenamide (B) lead to
metabolic syndrome?
Of the 243 patients: There was no statistical difference between
the 2 groups on:
69 (28.4%) gained ≥10% weight
– New initiation of blood pressure medication
174 (71.6%) gainedÉtude EMERALD
48En résumé Les personnes vivant avec le VIH présentent dans certaines cohortes, un poids inférieur à une population de référence VIH- L’effet d’un possible retour à la santé doit être pris en compte dans l’analyse des causes de la prise de poids avec les régimes thérapeutiques bien tolérés L’effet du TAF sur le poids pourrait être imputable à l’effet suppresseur sur le poids des régimes comparateurs à base de TDF: – Passage de TDF à TAF augmente le poids – Passage de TDF à Dolu/3TC amène augmentation de poids – Passage de TAF à à la bithérapie Dolu/3TC n’a pas d’effet sur le poids La prise de poids sous TAF ou INSTI ne semble pas associée à des complications cardiométaboliques L’excès de poids au départ et la résistance à l’insuline pourraient favoriser la prise de poids sous ARV Les données présentées sont préliminaires et ne permettent pas d’en arriver à des conclusions fermes sur le sujet de la prise de poids 52
You can also read