Pathogenic Amoebae Human Pathogen II - Assoc. Prof. Dr. Anchalee Wannasan - Med.CMU
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pathogenic Amoebae
Human Pathogen II
Assoc. Prof. Dr. Anchalee Wannasan
1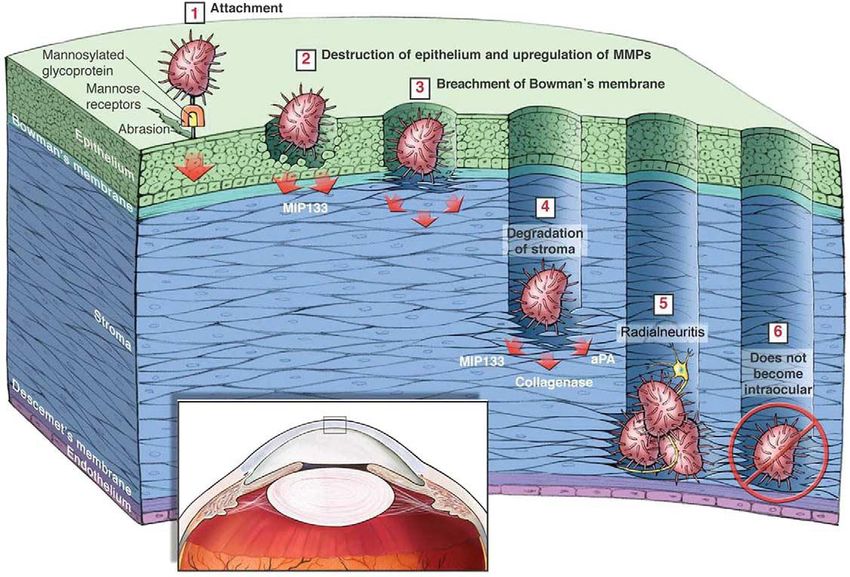
Objectives
• be able to identify and describe the
pathogenic amoebae in terms of
morphology, life cycle, pathology,
symptoms, transmission and diagnosis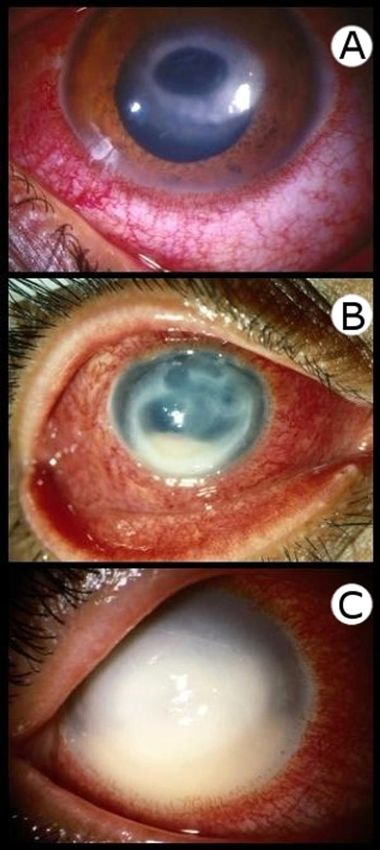
Entamoeba histolytica
• Disease: amoebiasis
• Distribution: worldwide
- second leading cause of death after malaria
- developing countries: poor sanitation areas
- developed countries :
immigrants or travelers from endemic areas
• Transmission:
- fecal-oral route
- venereal transmission (homosexuals)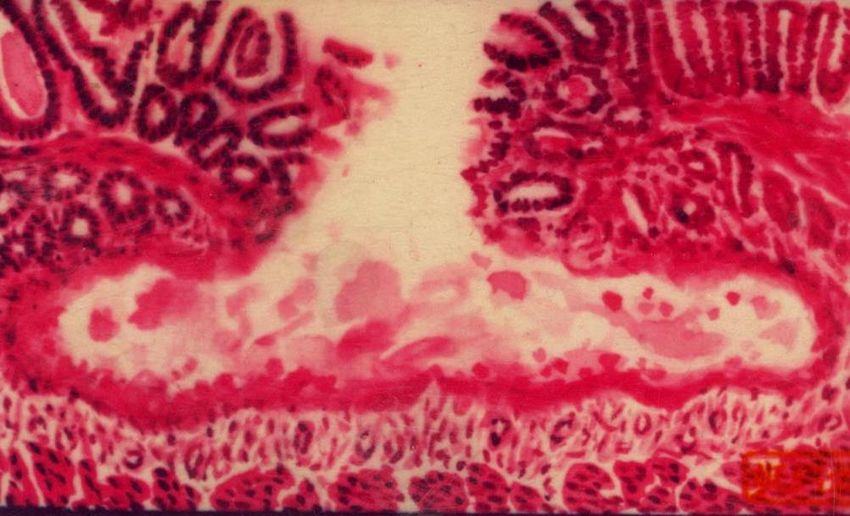
• 2 stages in the life cycle
Cyst (dormant form) Trophozoite (active form)
• Infective satge: mature cyst with 4 nuclei
www.medical-labs.net
karyosome
Chromatoid body
Peripheral chromatin www.medical-labs.net 5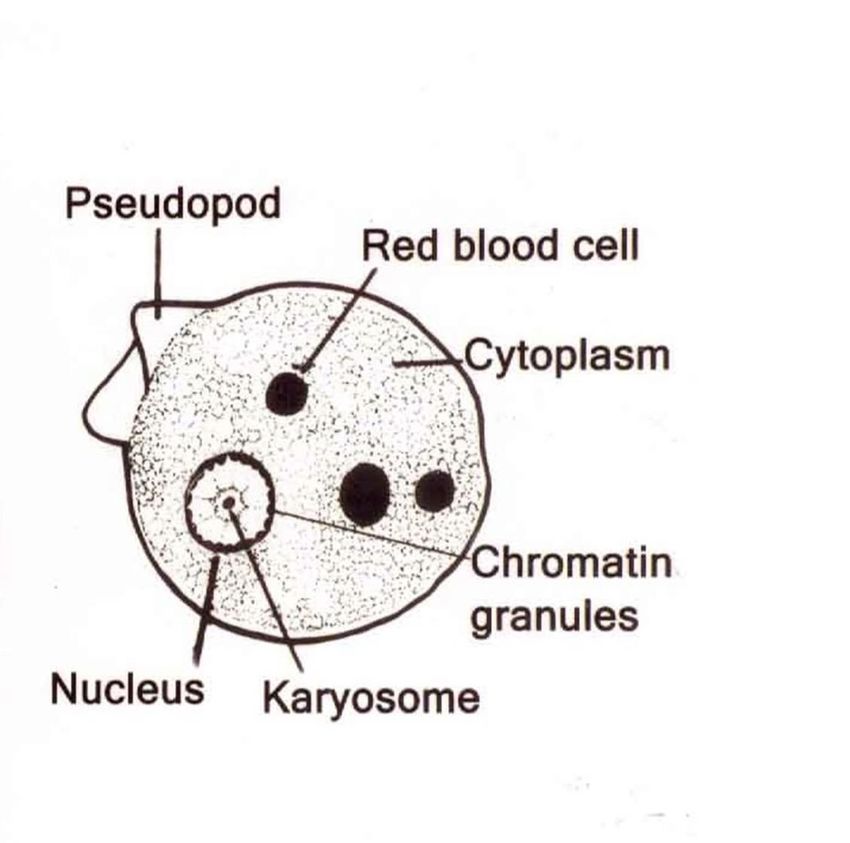
Cyst ~10-20 µm • round or oval shape • thin and tough cyst wall • contains 1, 2 or 4 nuclei • centric karyosome • peripheral chromatin • chromatoid bar with rounded ends (Cigar-like)
7

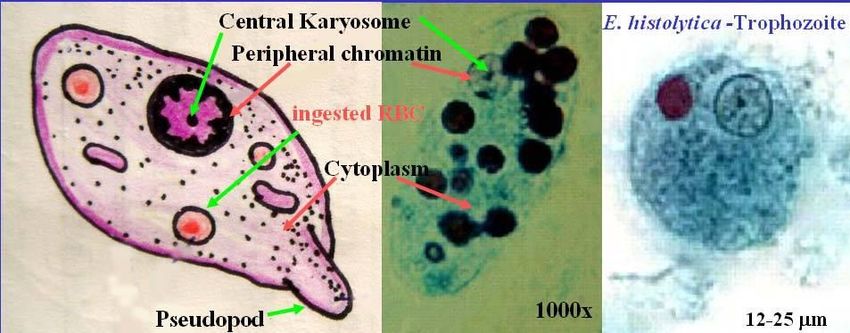
Trophozoite ~15-60 µm • irregular shape • a round nucleus • small, centric karyosome • peripheral chromatin scattered evenly throughout the inner nuclear membrane • fine granular endoplasm (food vacuoles + RBC)
10
Rapid movement by finger-like pseudopodia
12
Pathology and symptoms
• Amoebiasis is a disease caused by E. histolytica.
• Forms of amoebiasis
1) Intestinal amoebiasis
- 90% is asymptomatic cyst passers (E. dispar ?)
- 10% is symptomatic (Invasive amoebiasis)
2) Extraintestinal amoebiasis1. Intestinal amoebiasis (Invasive amoebiasis) ❑ incubation period is variable, (mostly 1-4 w) ❑ characterized by 4 markers: o amoebic dysentery (mucus and bloody diarrhea) o trophozoites with ingested RBC (feces, rectum biopsy) o amoebic colitis (endoscopy) o positive serological test for specific Ab
❑ Other clinical manifestations
o increasing diarrhea progressing to mucous-bloody
o lower abdominal pain, tenesmus
o weight loss, fever
o similar to other colonic diseases
o WBC are rarely seen in stools
o progressive involvement
- Fulminant necrotitizing colitis, toxic megacolon
- Acute rectocolitis
- Amoebic appendititis
- Amoeboma (immune response to trophozoites)
15Ameboma
https://www.wjgnet.com/1007-9327/full/v22/i36/8234.htm
• Granulation tissue and fibrotic thickening caused by
host immune response to trophozoites, Fig A, B) 16Amebic colitis
http://
intranet.tdmu.edu.ua/data/kafedra/internal/med_biologia/classes_stud/en/med/prophylactic%20medicine/ptn/medical%20biology/1%2 0course/theme%2008.htm
• Severe dysentery with multiple ulcers in the large
bowel, and a bloody diarrhea
17Intestinal amebic ulcers
https://cmr.asm.org/content/13/2/318/figures-only
https://link.springer.com/chapter/10.1007/978-4-431-55200-0_23
1) Nodular lesion (0.1- to 0.5-cm in diameter)
o rounded and small ulcer with slightly elevated rims
o necrotic center
- appears dimpled or hemorrhagic
- filled with yellowish mucous
182) Irregular lesion (1- 5 cm in length)
o shallow but broad
with elevated rims
o filled with fibrin and
yellow exudates
https://www.researchsquare.com/article/rs-29990/v1
Irregular cecum 19
lesionsFlask-shape amoebic ulcer
4.bp.blogspot.com
20Pathogenesis
• glandular hyperplasia
• stromal edema
• atrophy of villi & epithelium
• infiltration of neutrophils
• deep into submucosa
• 2nd bacterial infection
21
(flask-shape amoebic ulcer)2. Extraintestinal amoebiasis
• Hematogenously spread to liver and other
organs (lung, pericardium, brain, skin, and
genitourinary tract, etc.)
• Liver is the most common involvement site
• 3–9 % of all intestinal amebiasis cases develop
to amoebic liver abscess (ALA)Amoebic liver abcess (ALA)
▪ capillary obstruction in portal system (necrosis)
▪ pin head-like lesion, then enlarged and became abscess
acute - right upper quadrant abdominal pain
- fever
- liver tenderness and hepatomegaly
chronic - weight loss, vague abdominal symptoms
Rupture of abscesses into the abdomen or chest may
lead to death.https://www.researchgate.net/publication/221929027_Amoebiasis_in_the_Tropics_Epidemiology_an
Amoebic liver abcess
d_Pathogenesis/figures?lo=1
https://en.wikipedia.org/wiki/Amoebic_liver_abscess
https://www.sciencephoto.com/media/250192/view/liver-abscessDiagnosis
Intestinal amebiasis
• Microscopic examination (stool or rectal smear)
- dysenteric stool : trophozoites
- nondysenteric stool : cysts
- differential diagnosis from E. dispar
using isozyme analysis, serological methods, PCR
• Biopsy from colonoscopy / sigmoidoscopy
25• Extraintestinal amebiasis
• stool exam may not be helpful
• aspirates from abscess may not find amoebae
• biopsy from liver abscess rims (recommended)
• imaging procedure (ultrasound/ CT / MRI)
• serological methods (ELISA)
- discriminate ALA from pyogenic liver abscess
- negative in Entamoeba dispar infected patient
• PCR
26http://medicinembbs.blogspot.com/2013/01/amoebic-liver-abscess.html Charateristics of pus from ALA: anchovy paste-liked color without smell
Treatment
drugs of choice :
Metronidazole - effective to both intestinal and
tissue amoebiasis
Nitroimidazole derivatives such as secnidazole,
nimorazole and tinidazole
ALA - Percutaneous drainage or surgical aspiration
E. dispar infection does not require the treatment
28Pathogenic free-living amebae
Naegleria fowleri
o Primary amoebic meningoencephalitis (PAM)
Acanthamoeba spp.
o Granulomatous amoebic encephalitis (GAE)
o Acanthamoebic keratitis (AK)
Balamuthia mandrillaris
o GAE
Sappinia pedata
o GAE
29Common features (pathogenic FLA)
• facultative free-living parasites
• generally found in the
environment
• mortality rate approach 100%
• no specific therapeutic agents
30Naegleria fowleri
• known as the brain-eating amoeba
• Distribution : worldwide
(water and soil resources)
• Disease : primary amebic meningoencephalitis
most cases were immunocompetent host
• Most clinical isolates are thermophilic (> 45°C).
• 3 stages in LC: cyst , trophozoite
and flagellate (Amoeboflagellate)
31Morphology
Cyst ~ 8-20 µm
https://www.si.mahidol.ac.th/th/department/parasitology/articledetail.asp?ac_id=7&pageno=1
• round with double cyst walls
• big karyosome surrounded by halo
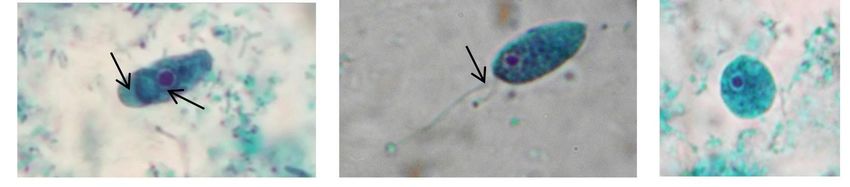
• never found cyst stage in host tissueTrophozoite Flagellate
~ 10-35 µm ~ 10-16 µm
reversible
(Lobopodia) (flagellum)
• Enflagellation test: In distilled water or nutrients depriving
condition, trophozoite transforms into flagellate (2 flagella)
33Life cycle
34Risk activities:
• Diving or swimming
in fresh water
resources
• Performing ‘neti’
(nasal rinse)
https://www.insider.com/neti-pot-tap-water-is-it-dangerous-brain-eating-amoeba-2018-12
• a ritual cleansing that
includes nasal
passages
36Clinical manifestation
Incubation period: 3-7 days
acute common cold-like symptoms:
fever, rhinitis, stiff neck, sore throat and severe headache
similar to that of acute bacterial and viral meningitis
Rapidly progression with high fever, vomiting, seizure,
edema of lung and brain, respiratory failure, coma
Death within 10 days
37Diagnosis
immunocompetent host (mainly children & young adult)
history of water exposure (exp. swimming)
CSF sedimentation : found only trophozoite
o culture on non-nutrient agar with gram (-ve) bacteria
o enflagellation test, PCR
• brain tissues: found only trophozoite
o staining
o IFA, Immunohistochemistry
o PCRTreatment
no specific therapeutic agents
Combination of available drugs which can cross blood-
brain barrier
Miltefosine or combination anti-microbial therapy:
amphotericin B, Azithromycin, rifampin, and azole drugs
Intensive supportive care is required
Only a few from hundred cases survive
39Prevention
Chlorine in swimming pool 1-2 ppm
Avoid swimming in fresh natural resources
Wear the nose clip during swimming
Blow the nose using sterile reagent
40Acanthamoeba
• Free-living protozoan (facultative) parasites
- worldwide distribution : soil, air, dust, fresh and sea water,
Jacucci tubs, dental irrigation unit, contact lens, etc.
- usually concentrate at the bottom of the lake
• Pathogenic to man (thermophilic)
• Exp. A. castellani, A. culbersoni, A. diviornensis,
A. hatchetti, A. healyi, A. polyphaga, A. rhysodes, etc.
41Morphology
A) Cyst ~ 5-25 µm
- uninucleated
- thick-wall polygonal , stellate,
oval or spherical endocyst
with ostioles
- wrinkle ectocyst
~ 10-45 µm
B) Trophozoite
- uninucleated
- irregular shape
- acanthopodia (thorn-liked)www2.le.ac.uk www.med-chem.com
ww.labor-spiez.ch
Trophozoite, 10-45 µm Cyst, 5-25 µm
43Disease
1. Granulomatous Amoebic Encephalitis (GAE)
- common in immunocompromised hosts
- primary infection at the skin ulcer or lung, then
spread hematogenously to brain
- no evidence of infection via olfactory nerves
2. Acanthamoeba keratitis (AK)
- mostly in healthy persons (contact lens wearers)
3. Cutaneous infection
- subacute granulomatous dermatitis
- immunocompromised hosts
451. Granulomatous Amoebic Encephalitis (GAE)
Symptoms
▪ subacute (IP 8-30 days) with no specific symptoms
▪ resemble viral, bacterial or tuberculosis meningitis
▪ mental status changes (86%), seizures (66%)
hemiparesis (53%), fever (53%), stiff neck
headache (53%), meningismus (40%), etc.
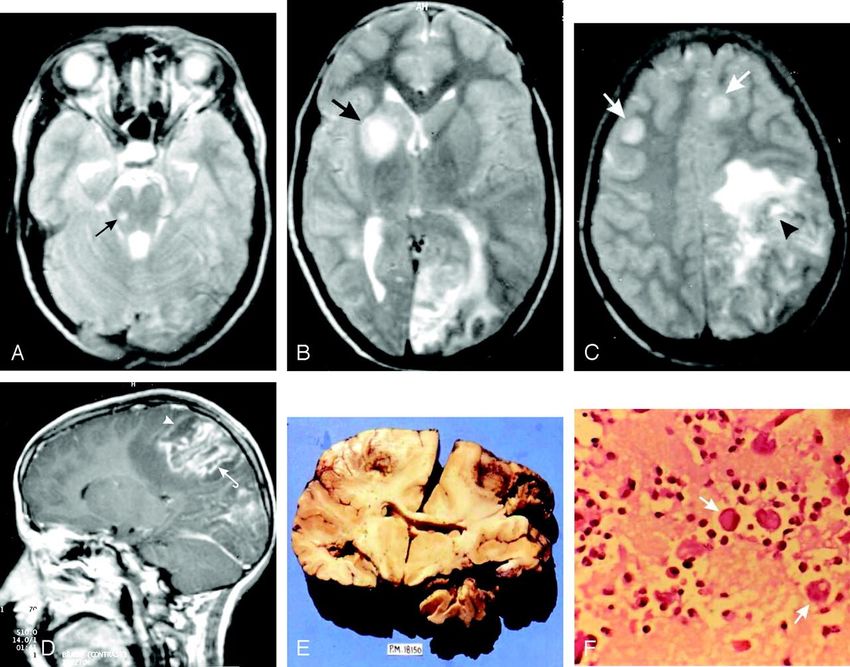
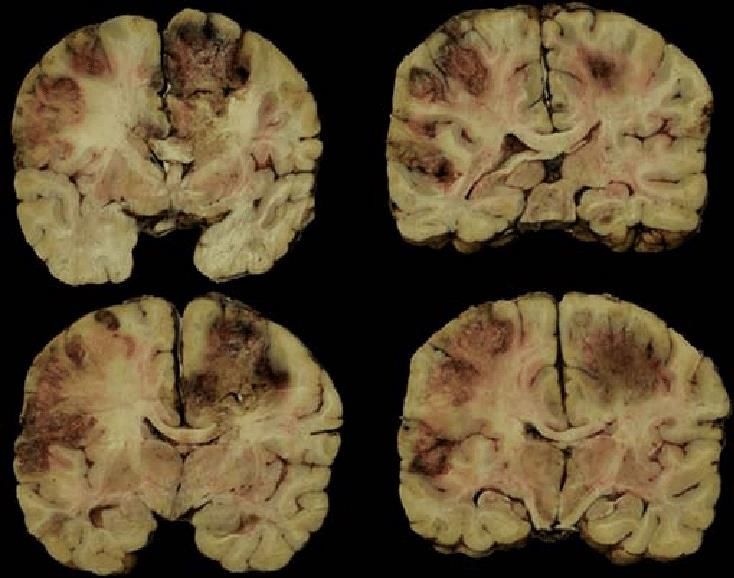
46GAE
DOI: 10.5005/jp-journals-10028-1080 P. Singh, R. Kochhar, R.K. Vashishta, N. Khandelwal, S. Prabhakar, S. Mohindra and P.
Singhi American Journal of Neuroradiology June 2006, 27 (6) 1217-1221;
•The terms “ granulomatous” indicates hemorrhagic necrotizing
lesions or brain abscess (detected by neuroimaging scans) with
severe meningeal irritation and encephalitis.
(NA Khan - Am J Infect Dis: 79-83, 2005)GAE
http://www.med-chem.com/para-site.php?url=org/acantham
GAE: spread hematogenously, possible distribute in frontal lobe, temporal lobe, parietal lobe,
likely through middle-cerebral artery (as these cortices are among the main regions supplied by
middle cerebral artery) Ong et al JCM, 2017 48GAE
Diagnosis
- difficult (similar symptoms as other CNS infection)
- historical exposure to water or soil
- CT, MRI : not specific
- brain biopsy
o staining (trophozoites and cysts)
o IFA, culture, PCR
- CSF
o rarely find amoebae by microscopy
o culture, PCR
- Serological test : may not be useful
49GAE- Acanthamoeba
ruby.fgcu.eduTreatment GAE
- Brain surgery of multi focal areas is difficult.
- combination drugs
azoles drugs, pentamidine,
amphothericin B, chlorhexidine,
rifampin, miltefosine, etc.
- Most GAE cases were proven after death.
512. Acanthamoeba Keratitis (AK)
a painful vision-threatening
infection
Corneal ulceration, visual loss, and
blindness
healthy person, esp. contact lens
wearers
Developed countries (83% AK cases)
(Carvalho et al. 2009)
Non-developed countries
mostly related with agricultural-based
activities
(Clarke and Niederkorn 2006; Gopinathan et al. 2009)AK
Symptoms
➢ Incubation period : a few days to several weeks
- begins with a foreign-body sensation
- tearing, epithelial defects and photophobia
- inflammation with redness, stromal infiltration,
stromal opacity with extreme pain (radial neuritis),
stromal abscess and finally blindness
➢ Frequent misdiagnosis to other keratitis from
common pathogens (Pseudomonas, Staphylococcus,
Herpes, or Adenovirus, etc.)
54Clinical AK appearance (Barratt JLN, et al., 2010)
(A) ring infiltration (most cases)
(B) multiple ring infiltrates and hypopyon
(C) near-total suppuration
(Barratt JLN., 2010)Diagnosis • history of using contact lens • confocal microscopy • corneal scraping, corneal biopsy from the infiltrate areas - staining / culture - IFA / specific PCR • unrecommended tests : Ab detection or amoebae isolation from lens case
Vivo Confocal Microscopy
Staining from corneal scrapings (Barratt JLN., et al, 2010) Calcofluor white Giemsa stain Gram stain Giemsa stain
AK
Treatment
▪ early infection:
combination drugs + epithelial debridement
▪ combination drugs
biguanides : chlorhexidine,
polyhexamethylene biguanide (PHMB)
diamidines : propamidine, hexamidine
▪ late infection: permanent damage, drug resistance
hypopyon, secondary infection
→ cornea transplantation
- 593. Cutaneous infection
• Vary clinical signs
depended on underlying
immunologic status.
• Both cysts and trophozoites
can be found on skin.
• very rare and self-limiting in
immunocompetent host
60Cutaneous acanthamoebiasis
https://www.labce.com/spg931637_illness_and_symptoms_continued_acanthamoeba_specie.aspx
• Hematogenous spreading to other tissues in
immunocompromised host
• Involvement of CNS leads to death within weeks
• early treatment : topical combination drugs
(antimicrobials and azoles drugs) or surgery
61Lab Demonstration
62Glycogen vacuole
63Trichrome stain Uninucleated cyst
Iron-hematoxylin stain
64Trichrome stain Binucleated cyst
Fresh smear
6566
10 µm
67Naegleria fowleri
Trichrome stain
Cyst
• ~ 8-20 µm in diameter
• round with unstained double cyst walls
• big karyosome surrounded by halo
• never found cyst stage in host tissue
68Naegleria fowleri
Fresh smear from CSF
Trophozoite
Lobopodia
• ~ 10-35 µm , irregular shaped
• big karyosome surrounded by halo
• often seen in host tissue
Flagellate
Trichrome stain
• ~ 10-16 µm, pear-shaped
flagellum • In depriving condition such as distilled
water, trophozoite can transform into
flagellate within 1 hr. at 37°C.
• The process is reversible.
69Acanthamoeba castellanii Cyst Fresh smear from the culture
• uninucleated
• Thick-wall wrinkle ectocyst
• Endocyst with various shapes e.g., polygonal , stellate, oval or spherical
• Endocyst meet ectocyst at the ostioles (cyst pore).
70Acanthamoeba castellanii Trophozoite
Fresh smear from culture
5 µm
• uninucleated
• irregular shape
• acanthopodia (thorn-liked)
E-mail: kdantra@gmail.com 71You can also read

















































