Pacemakers/défibrillateurs et IRM - Estelle Gandjbakhch, Paris Recommandations de l'interface SFR-SFC pour la bonne pratique - Groupe ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Pacemakers/défibrillateurs et IRM
Recommandations de l’interface SFR-SFC pour la bonne pratique
Estelle Gandjbakhch, Paris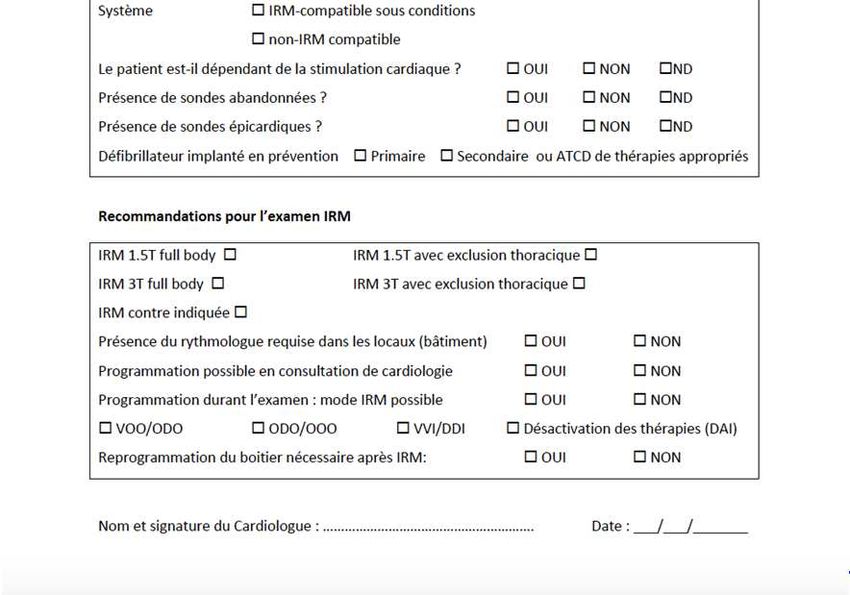
Parc IRM - France
PM/ICD implantations in numbers
4 millions worldwide
1.2 millions patients in USA
∾ 400 000 patients in France
60 000-70 000 PM implantations /year
15 000 ICD implantations /year
2% increase /year
50% of PM/ICD carriers would need a MRI during follow-up *
Within one year follow-up, 17% of patients with PM/ICD would need a MRI**
*Roguin A. Europace 2008; 10: 336–346
**Sakakibara et al., Japanese Heart J 1999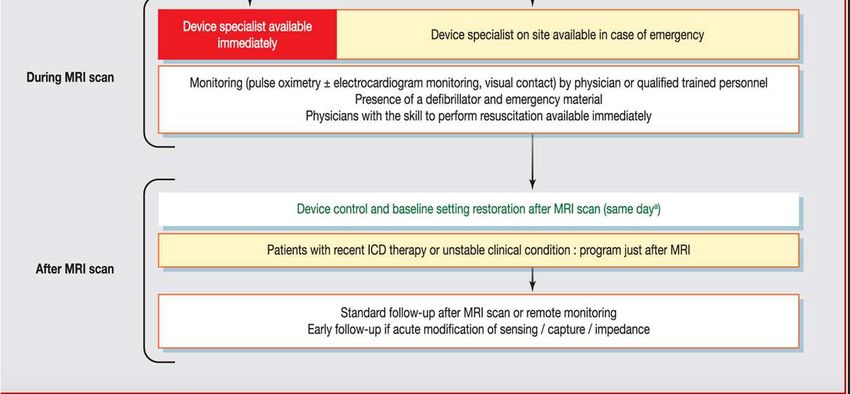
IRM/PM evolution
70 000 examens
IRM / million habts
800 PM/million habts
- 1000 PM/million habts en France
Bhuva AN et al. Eur Radiol 2020; 30:1378-84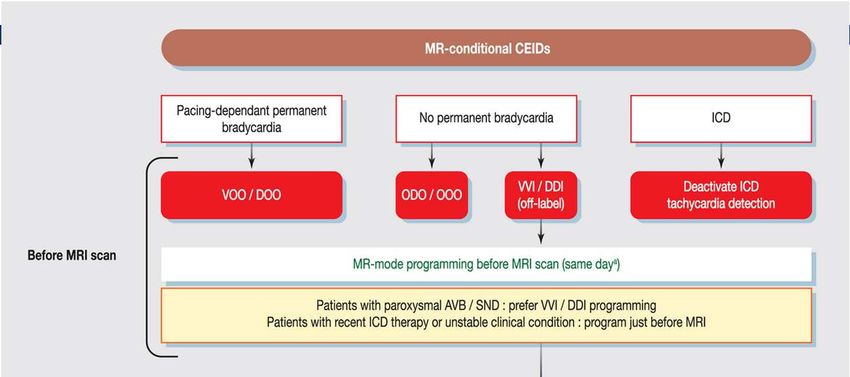
Patients with PM/ICD have a difficult access to MRI Exemple with ICDs – Source ACR Turakhia M, Reynolds M, Wolff S, et al. Medtronic Data on File 2013. Data from 2011 MarketScan® Commercial and Medicare database, Truven Analysis, Inc. were used for this research.
Two opposite tendencies
Since development of conditional And yet,
PM/IRM,
– Wrongly referred in France as – Implanted patients are refuted in
"compatible" MRI at most MRI centers in
– Some trends to trivialize the use Europe
of PM/ICD in MRI – An implanted patient is 50 times
– Despite a non-zero risk less likely to get an MRI VR
than a non-implanted one
– especially with the development
of high magnetic fields – Increased machine time
– No financial recognition
Nazarian S et al. J Magn Res Imaging 2016; 43: 115-27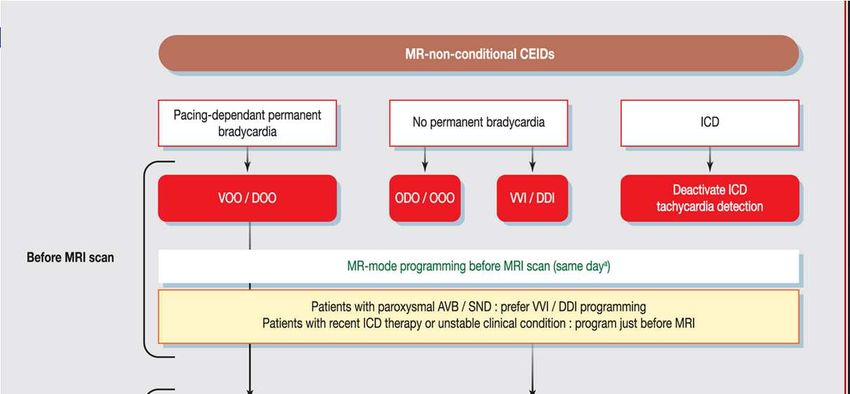
Les risques existent toujours
• Les risques sont moindres avec les
systèmes MR conditionnels
– Dans les conditions d’utilisation
recommandées
• L’expression pacemaker « IRM- compatible »
est impropre
• Chaque séquence d’IRM est une nouvelle
« expérience » induisant un risque propre
– Patient
– Matériel implanté
– Séquence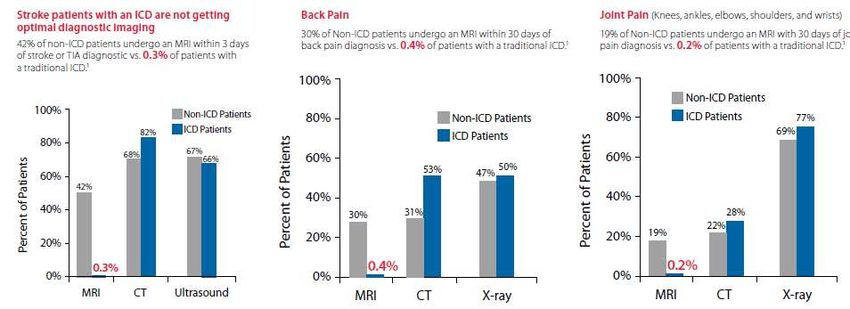
Multiparametric interactions
Main field (B0) Gradients RF field (B1)
Force / Torque
Vibration
Arrhythmias
Potential risk(s)
Surdetection
Heating
Pacing inhibition
PM/DAI malfunction
(reset mode, battery
depletion)
ICD Tachycardia detection inhibition
Risks of MRI on PM/ICDs (conditional and non-conditional)
For the patient, For the device,
• Oversensing • Migrating or moving components
– Pacing inhibition (Purely theoretical risk)
– Bradycardia in pacing-dependent • Battery depletion
patient • Deprogramming
– Inappropriate shock
• Switching to Reversion Mode (VVI)
• Ventricular arrhythmia
• Permanent failure
– Risk of asynchronous mode VOO,
DOO (the main cause of death • Thresholds changes
describe)
– Non-detection of ventricular arrhythmia
(inhibition of ICD therapy)
• Burns (RF)
– abandoned leads There is no "MR safe" device
Prospective registries of non MRI-conditional devices
Magnasafe Regsitry John Hopkins Registry
• 1500 patients • 1509 patients
• 2/3 PM- 1/3 DAI • 58% PM- 48% DAI
• IRM 1.5 T extra thoracic • IRM 1.5 T thoracic /extra thoracic
• 0.3% in« back up » mode • 0.5% in« back up » mode
• 1 mute ICD change • 1 mute PM (end of life battery)
• Sensing/pacing thresholds • Sensing/pacing thresholds
modifications : non significant modifications : 4% but non significant
Nazarian et al. NEJM 2017
Russo et al. NEJM 2017The latest reported deaths are related to old models
• 6 deaths following MRI in patients with PM
• patients not monitored during the examination
• Risk contexts (SCA, advanced heart disease, hydro-electrolyte
disorders)
• examined outside hospital, no cardiological supervision
• all not pacing-dependent
• Essential cause: VT, VF
• All standard field ≤1.5T
• The MRI department was not informed of the PM; communication
+++
• No deaths reported in selected and monitored patients
Irnich W. Europace 2005; 7: 353-365PM/DAI conditionnels
• Les risques sont minorés mais non • Innovations technologiques
nuls
– Sondes amagnétiques
– Surdétection
– Nouveaux interrupteurs
• Inhibition du pacing ou choc
inapproprié – Diminution de la composante ferro
– Arythmie magnétique du générateur
• Mode asynchrone (VOO,
DOO)
– Bradycardie
• Mode ODO, OOO
– Inactivation du DAI: non
traitement d’une TV/FV
Gandjbakhch E et al. Arch Cardiovasc Dis.2020
Dacher JN et al. Diagn Interv Imaging 2020Dedicated Protocols +++ Gandjbakhch E et al. Arch Cardiovasc Dis.2020
Dacher JN et al. Diagn Interv Imaging 2020
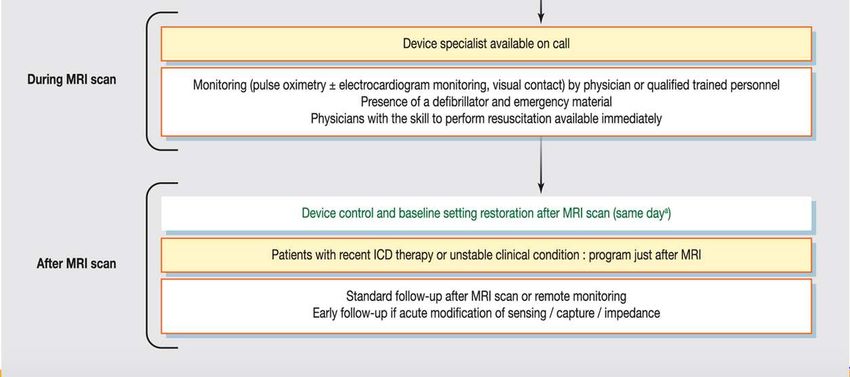
Prescription Pre-MRI Post-MRI
MRI
Discussion with cardiologist programming programming
• Determine if the system is IRM • What mode? • Monitoring: Who? How? • Restoration of
conditional • Where? • Reduce the number of standard settings
• Benefit/risk? • Surveillance? sequences to the minimum and device control
• Can MRI be substituable? • Who? How? • Never exit the standard • Where?
• No contra-indications mode (SAR control) • Who? How?
• Indication of PM/DAI
• Pacing-dependency?
• History of VA (ICD)Essential data
• Lead and can model: MR conditional?
• Pacing-dependent +++
• ICD or PM
• History of appropriate therapies for ICD
• No contra-indications:
– Abandoned leads/ epicardial leads/connectors : interrogate the patient,
scars, chest Xray if necessary
– Device malfunction: elevated pacing thresholds, battery close to end of
life
• Device implantation > 4-6 weeks (except emergencies)
• Clinical state of the patient: no fever or acute medical problem
Gandjbakhch E et al. Arch Cardiovasc Dis.2020
Dacher JN et al. Diagn Interv Imaging 2020Determine if the system is MR conditional
www.irm-compatibilite.comGandjbakhch E et al. Arch Cardiovasc Dis.2020 Dacher JN et al. Diagn Interv Imaging 2020 PM/ICD MR-conditional
Gandjbakhch E et al. Arch Cardiovasc Dis.2020 Dacher JN et al. Diagn Interv Imaging 2020 PM/ICD non MR-conditional
Check list ++ Gandjbakhch E et al. Arch Cardiovasc Dis.2020 Dacher JN et al. Diagn Interv Imaging 2020
Remaining issues
Patients Practitioners
Patient Safety/ Organizational problem ++++
Risks associated to lack Time-consuming ++
of access to MRI
Availability of device specialists
Devices Organization of MR departments
Mode auto-detect No financial valuation
No patient with implantable electrical cardiac devices should be formally contra-indicated
from an MRI because of their device if the MR is vital• Respecter les indications
– Guide de bon usage
• http://gbu.radiologie.fr
• Substituer l’IRM quand cela est possible (par la
TDM en général)
• Quand l’IRM doit être faite
Que peut faire le – Déterminer l’IRM compatibilité
• www.irm-compatibilite.com
radiologue pour – Respecter les recommandations
constructeurs et se limiter à 1.5T/3T selon les
réduire le risque? modèles
– Monitorer le patient / médicaliser l’examen
– Réduire le nombre de séquences au strict
minimum
– Ne jamais sortir du mode standard (contrôle
du SAR)
• Communiquer au mieux avec la cardiologie +++ (
– Détecter les (rares) cas de CI
– Evaluer le bénéfice/risque de l’examenCas particulier de l’IRM
cardiaque
• Les artéfacts liés aux DAI rendent
illusoire la réalisation d’examens IRM
cardiaques de qualité
• Une indication de DAI posée peut être
une raison de réaliser une IRM en
urgencePerspectives • Généralisation du mode d’auto-activation en mode IRM après détection du champ magnétique limite le risque d’évènement pendant la reprogrammation en mode IRM Facilite le circuit avant/après • Délégation de taches /protocoles de coopération • Simplification du parcours patient a l’échelon de chaque établissement : coordination entre radiologues et cardiologues
Autres données essentielles
• Stimulo-dépendance+++
• Absence de sondes abandonnées/épicardiques/
adaptateurs/connecteurs : interroger le patient, cicatrices,
RP
• DAI: prévention Iaire/II aire
• Implantation depuis au moins 6 semaines
• Etat clinique du patient: absence de fievre, …
• Le carnet de pace maker souvent ne suffit pas quand le
patient n’est pas suivi dans le centreYou can also read

















































