Original Investigation Niacinamide May Be Associated with Improved Outcomes in COVID-19-Related Acute Kidney Injury: An Observational Study ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Investigation
Niacinamide May Be Associated with Improved
Outcomes in COVID-19-Related Acute Kidney Injury: An
Observational Study
Nathan H. Raines,1 Sarju Ganatra,2 Pitchaphon Nissaisorakarn,1 Amar Pandit,1 Alex Morales,1 Aarti Asnani,3
Mehrnaz Sadrolashrafi,4 Rahul Maheshwari,5 Rushin Patel,2 Vigyan Bang,2 Katherine Shreyder,2 Simarjeet Brar,2
Amitoj Singh,2 Sourbha S. Dani,2 Sarah Knapp,6 Ali Poyan Mehr,7 Robert S. Brown,1 Mark L. Zeidel,1 Rhea Bhargava,1
Johannes Schlondorff,1 Theodore I. Steinman,1 Kenneth J. Mukamal,5 and Samir M. Parikh1
Abstract
Background AKI is a significant complication of coronavirus disease 2019 (COVID-19), with no effective therapy.
Niacinamide, a vitamin B3 analogue, has some evidence of efficacy in non-COVID-19-related AKI. The objective
of this study is to evaluate the association between niacinamide therapy and outcomes in patients with COVID-
19-related AKI.
Methods We implemented a quasi-experimental design with nonrandom, prospective allocation of niacin-
amide in 201 hospitalized adult patients, excluding those with baseline eGFR ,15 ml/min per 1.73 m2 on or
off dialysis, with COVID-19-related AKI by Kidney Disease Improving Global Outcomes (KDIGO) criteria, in
two hospitals with identical COVID-19 care algorithms, one of which additionally implemented treatment
with niacinamide for COVID-19-related AKI. Patients on the niacinamide protocol (B3 patients) were
compared against patients at the same institution before protocol commencement and contemporaneous
patients at the non-niacinamide hospital (collectively, non-B3 patients). The primary outcome was a com-
posite of death or RRT.
Results A total of 38 out of 90 B3 patients and 62 out of 111 non-B3 patients died or received RRT. Using
multivariable Cox proportional hazard modeling, niacinamide was associated with a lower risk of RRT or death
(HR, 0.64; 95% CI, 0.40 to 1.00; P50.05), an association driven by patients with KDIGO stage-2/3 AKI (HR, 0.29;
95% CI, 0.13 to 0.65; P50.03; P interaction with KDIGO stage50.03). Total mortality also followed this pattern
(HR, 0.17; 95% CI, 0.05 to 0.52; in patients with KDIGO stage-2/3 AKI, P50.002). Serum creatinine after AKI
increased by 0.20 (SEM, 0.08) mg/dl per day among non-B3 patients with KDIGO stage-2/3 AKI, but was stable
among comparable B3 patients (10.01 [SEM, 0.06] mg/dl per day; P interaction50.03).
Conclusions Niacinamide was associated with lower risk of RRT/death and improved creatinine trajectory
among patients with severe COVID-19-related AKI. Larger randomized studies are necessary to establish a causal
relationship.
KIDNEY360 2: 33–41, 2021. doi: https://doi.org/10.34067/KID.0006452020
Introduction stressors. Consequences of COVID-19-related AKI in-
Coronavirus disease 2019 (COVID-19) has led to clude severe shortages of dialysis machines and fluids,
.1,250,000 deaths worldwide and affects a host of strained nursing resources, and increased mortality (2,3).
organs, including the kidneys. The etiology of COVID- Previous work links non-COVID-19 AKI arising in
19-related AKI is likely multifactorial, but most often the context of renal ischemia and acute tubular necrosis
exhibits an acute tubular injury pattern (1). Acute tubular to an acquired renal deficiency of the energy metabo-
injury arises from inflammatory, ischemic, or nephrotoxic lism intermediate NAD1, a rate-limiting substrate for
1
Division of Nephrology, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston,
Massachusetts
2
Division of Cardiovascular Medicine, Department of Medicine, Lahey Hospital and Medical Center, Burlington, Massachusetts
3
Division of Cardiology, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston,
Massachusetts
4
Department of Pharmacy, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts
5
Division of General Medicine, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston,
Massachusetts
6
Division of Endocrinology, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston,
Massachusetts
7
Department of Nephrology, Kaiser Permanente San Francisco Medical Center, San Francisco, California
Correspondence: Dr. Samir M. Parikh, Division of Nephrology, Department of Medicine, Beth Israel Deaconess Medical Center, 330
Brookline Avenue, RN 330C, Boston, MA 02215. Email: sparikh1@bidmc.harvard.edu
www.kidney360.org Vol 2 January, 2021 Copyright © 2021 by the American Society of Nephrology 3334 KIDNEY360
oxidative metabolism in mitochondria, through acceler- trials for other indications (4,5). Given its safety, immediate
ated hydrolysis and decreased biosynthesis (4,5). In the availability, and limited, but encouraging, evidence of effi-
mitochondria-rich renal tubule, a stress-induced NAD1 cacy in non-COVID-19 AKI, we implemented a niacinamide
shortage curtails ATP production, which, if unchecked, protocol for patients with AKI, at a single hospital in Boston,
can culminate in tubular dysfunction and cell death (5). A designed to prevent progression of AKI and development of
pilot, randomized, placebo-controlled trial suggested that related complications.
oral niacinamide could safely increase NAD1 and poten- In this report, we compare rates of progression to RRT and
tially prevent AKI among patients who were perioperative, death and trends in serum creatinine among patients with
but it has not been tested in COVID-19-related AKI (4). COVID-19-related AKI on the niacinamide protocol with
There are no therapies for AKI prevention approved by the patients both admitted at the niacinamide hospital before
US Food and Drug Administration (FDA). implementation and contemporaneously admitted at a nonin-
Niacinamide, the base form of vitamin B3, is a supplement tervention hospital. We hypothesized that administration of
(considered by the FDA as “generally recognized as safe”) oral niacinamide would prevent progression and reduce com-
whose safety at chronic high doses has been established in plications associated with COVID-19-related AKI.
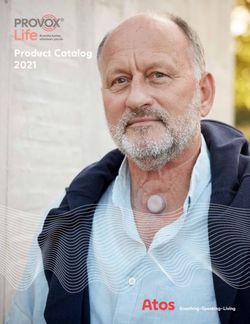
A
441 adult inpatients with COVID-19 during
study period to B3 hospital
29 with CKD V or ESRD
6 with ≤ 1 creatinine value
406 screened daily for persistent AKI
288 did not develop AKI
118 with persistent AKI
5 made comfort measures ≤ 48h
3 with ALT > 200IU/L
20 developed 90 developed 79 received ≥ 1
AKI before AKI between B3 doses
April 1 April 1 and 20 (B3 per -
(Pre-B3 group) (B3 group) protocol)
B
412 adult inpatients with COVID-19 during
study period to sister hospital
6 with CKD V or ESRD
29 with ≤ 1 creatinine value
377 screened daily for persistent AKI
285 did not develop AKI
1 made comfort measures ≤ 48h
0 with ALT > 200IU/L
91 with persistent AKI
(SH group)
Figure 1. | Patient flow at niacinamide protocol hospital (top) and sister hospital (bottom). ALT, alanine aminotransferase; B3, niacinamide
protocol; COVID-19, coronavirus disease 2019; SH, sister hospital not implementing niacinamide protocol.KIDNEY360 2: 33–41, January, 2021 Niacinamide in COVID-19-Related AKI, Raines et al. 35
Materials and Methods none was available, the lowest creatinine value within the
Setting first 96 hours of hospitalization was used. Severity of AKI
We conducted this study at two large tertiary acute-care was defined according to Kidney Disease Improving Global
teaching hospitals within the Beth Israel Lahey Health Sys- Outcomes (KDIGO) creatinine-based criteria (12). Further
tem (BILH) that admitted comparable numbers of patients details are provided in Supplemental Materials 1 and 2
with COVID-19 during the study period (Figure 1). One (Supplemental References).
hospital implemented the niacinamide protocol as a routine
part of clinical care on the basis of data in postoperative AKI
Exposure and Comparison Group Designation
(4). Both hospitals otherwise used a single COVID-19 care Eligible patients developing AKI on or after April 1, 2020
algorithm common to BILH. in the niacinamide protocol hospital were designated the
“B3” group; those who developed AKI before April 1 were
Study Design and Oversight designated the “pre-B3” group. Eligible patients at the sister
We used a quasi-experimental design, chosen for its abil- hospital not implementing the niacinamide protocol were
ity to be rapidly implemented using existing resources and designated the “SH” group. The pooled pre-B3 group and
to preserve eligibility for other potential life-saving thera- SH group was designated the “non-B3” group.
pies available only through clinical trials (6). Oversight is
described in Supplemental Materials 1 and 2.
End Points
The primary end point was the time in days from date of
Eligibility Criteria eligibility to RRT or death, whichever occurred first, during
We included hospitalized patients who developed per- the hospitalization (13). Data collection was censored at time
sistent AKI, were at least 18 years old, had a laboratory- of hospital discharge or on May 1, 2020; censoring events are
confirmed PCR test positive for severe acute respiratory reported in Figure 2. Secondary end points were time in days
syndrome coronavirus 2 from a nasopharyngeal swab, and from date of eligibility to death alone and RRT alone and
were admitted to either hospital between March 15 and change in serum creatinine over the 10 days after the date of
April 20, 2020. “Persistent AKI” was defined as a $0.3 mg/dl eligibility, with censoring at time of RRT, death, or discharge.
increase in serum creatinine over baseline, excluding indi-
viduals with AKI on admission that resolved to baseline
with routine supportive care within 96 hours. These AKI Statistical Analyses
criteria were used to enable implementation in a pragmatic Multivariable Cox proportional-hazards regression mod-
fashion, with a 96-hour cutoff chosen to decrease the likeli- els were used to estimate the adjusted association between
hood of including patients with prerenal azotemia. Individ- B3 group and the primary composite end point, and sec-
uals with baseline eGFR ,15 ml/min per 1.73 m2 both on ondary end points of death alone and RRT alone. Models
and off dialysis, or those who elected to receive comfort included age, sex, comorbid conditions, medications taken
measures only up to 48 hours after development of AKI before admission, laboratory values on day of eligibility,
were excluded. Given the hepatic metabolism of niacin- and whether individuals received intensive care unit (ICU)–
amide, individuals with alanine aminotransferase (ALT) level care. Variables included in the multivariate model
more than five times the upper limit of normal (200 IU/L) were selected on the basis of biologic plausibility and clinical
were excluded. relevance. Laboratory measurements were taken from dis-
tinct samples. Analyses were performed on an intention-to-
treat basis. Two patients missing one or more covariates
Protocol Implementation were excluded from multivariate analyses.
The dose of niacinamide was informed by trials with long- We designed one a priori subgroup analysis, comparing
term exposure in patients without kidney disease (7–9) individuals with KDIGO stage-1 versus KDIGO stage-2 or -3
and in patients with advanced kidney disease (10,11) that AKI using a multiplicative interaction term. One additional
affirmed its safety. Beginning April 2, 2020, nephrologists at patient with missing baseline creatinine was excluded from
the niacinamide protocol hospital performed daily chart these analyses.
review of all inpatients positive for COVID-19 to determine Our secondary analysis used a generalized estimating
whether they met eligibility criteria. Once a patient became equation model with an exchangeable correlation matrix
eligible, care teams were contacted via a templated note and to evaluate the secular trend in serum creatinine in the
by pager with the elective recommendation to begin oral 10 days after the day of eligibility. Similar to the primary
niacinamide, 1 g once daily, for a 7-day course; patients analysis, we evaluated patients in KDIGO stages 2 and 3
could receive doses through orogastric or nasogastric feed- separately from patients with stage 1 AKI. Additional
ing tubes if needed. A total of 79 out of 90 eligible patients details, including sensitivity analyses, are reported in Sup-
(88%) received one or more niacinamide doses. Niacinamide plemental Material 1. Statistical analyses were performed
was stopped in patients whose ALT rose more than three with SAS software, version 9.4.
times their respective values on the day of eligibility. Care
teams could also discontinue niacinamide at their discretion.
Results
Data Sources and Variables Assessed Characteristics of Cohorts
Data were obtained by review of the electronic medical A total of 441 patients with COVID-19 were admitted to
record. Baseline creatinine was defined as the most recent the intervention hospital and 412 patients were admitted to
serum creatinine in the 7–365 days before admission; when the nonintervention hospital between March 15 and April36 KIDNEY360
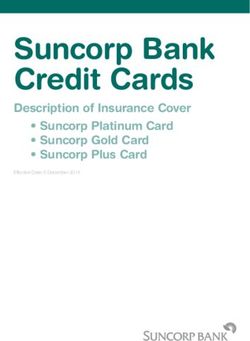
100 All patients
Crude hazard ratio 0.62
p = 0.02, [95% CI 0.42 - 0.94]
RRT-free survival (%)
75
Adjusted hazard ratio 0.64
p = 0.05, [95% CI 0.40 - 1.00]
50
25
B3
Non B3
0
0 5 10 15 20 25 30
Days since eligibility
No. at risk
B3 90 72 50 25 16 9 1
Non B3 111 75 45 26 12 6 3
100 KDIGO 2/3 only
Crude hazard ratio 0.49
RRT-free survival (%)
75 p = 0.04, [95% CI 0.25 - 0.97]
Adjusted hazard ratio 0.29
50 p = 0.003, [95% CI 0.13 - 0.65]
25
B3
Non B3
0
0 5 10 15 20 25 30
Days since eligibility
No. at risk
B3 21 14 10 6 5 3 1
Non B3 26 13 6 5 3 1 0
Figure 2. | Freedom from composite end point of RRT or death. Niacinamide was associated with lower risk of RRT or death over the 30-day
period following development of AKI, an association driven by patients with KDIGO stage-2/3 AKI.
19, 2020 (Figure 1). Of these, approximately a quarter de- Primary End Point
veloped persistent AKI at each hospital. Following exclu- Over a median follow-up of 11 days after the date of
sions, 90 patients were included in the B3 group and 111 eligibility (13 days in the B3 group, 9 days in the non-B3
were included in the non-B3 group, of which 20 were from group), 71 of 201 patients (35%) died and 46 of 201 (23%)
the pre-B3 group and 91 were from the SH group. received RRT across all groups. Table 2 reports the pro-
Baseline creatinine and the proportion of patients with portion of patients meeting the primary end point, along
a baseline eGFR ,45 ml/min per 1.73 m2 were similar with each component separately in each group. Unadjusted
between the B3 and non-B3 groups (Table 1). The frequency time-to-event analysis demonstrated a significantly lower
of AKI and distribution of AKI severity at the time of hazard for the composite end point of RRT or death in the B3
eligibility were also similar. Groups differed according to group compared with the non-B3 group, with particularly
age, race, chronic obstructive pulmonary disease/asthma, lower risk in the subset of patients with KDIGO AKI stage 2
smoking history, and administration of other COVID-19- or 3 (among all patients, hazard ratio [HR], 0.62; 95% CI,
targeted therapies during the same hospitalization. On the 0.42 to 0.94; among patients with KDIGO stage-2/3 AKI,
date of meeting eligibility, creatinine and AKI stage were HR, 0.29; 95% CI, 0.13 to 0.65; Figure 2, Table 2). The
similar across groups. Groups differed by hemoglobin, corresponding multivariable HR for all patients was 0.64
platelet count, potassium level, requirement for ICU-level (95% CI, 0.40 to 1.00; Table 2).
care, and vasopressor medication support. Supplemental The adjusted association between risk of RRT or death and
Table 1 shows the baseline characteristics with the pre-B3 niacinamide implementation was significantly modified by
and SH groups separated. KDIGO stage at the time of eligibility (P interaction50.03).KIDNEY360 2: 33–41, January, 2021 Niacinamide in COVID-19-Related AKI, Raines et al. 37
Table 1. Characteristics of patients in the B3 group and non-B3 group
Characteristics Non-B3 (n5111) B3 (n590)
Age (yr), mean (SD) 73.1 (12.4) 65.6 (15.2)
Female, n (%) 44 (40) 40 (44)
Race, n (%)
White non-Hispanic 91 (82) 27 (30)
Black non-Hispanic 11 (10) 31 (34)
Hispanic 5 (5) 13 (14)
Asian 2 (2) 3 (3)
Other 2 (2) 16 (18)
BMI (kg/m2), mean (SD) 30.4 (7.8) 32.2 (7.9)
Baseline creatinine (mg/dl), mean (SD) 1.17 (0.47) 1.20 (0.55)
eGFR ,45 ml/min per 1.73 m2 at baseline, n (%) 24 (22) 22 (25)
Past diagnoses, n (%)
COPD/asthma 30 (27) 13 (14)
Diabetes mellitus 49 (44) 50 (56)
Hypertension 94 (85) 70 (78)
HF with reduced EF 10 (9) 5 (6)
Malignancy 17 (15) 20 (22)
Current or former tobacco use 62 (56) 34 (39)
Baseline medications, n (%)
Statin 76 (69) 62 (69)
ACEi/ARB 48 (43) 33 (37)
In-hospital medications, n (%)
Hydroxychloroquine 80 (72) 40 (44)
Azithromycin 73 (66) 51 (57)
Remdesivira 2 (2) 11 (12)
Sarilumaba 0 (0) 18 (20)
Tocilizumab 13 (12) 10 (11)
Characteristics at day of eligibility
Creatinine (mg/dl), mean (SD) 2.02 (1.35) 2.10 (1.32)
KDIGO AKI stage, n (%)
Stage 1 85 (77) 68 (76)
Stage 2 16 (14) 13 (15)
Stage 3 10 (9) 8 (9)
Hemoglobin (g/dl), mean (SD) 11.4 (1.90) 10.7 (2.19)
WBC count (K/ml), mean (SD) 8.62 (4.16) 9.41 (5.20)
Platelet count (K/ml), mean (SD) 216 (108) 255 (130)
Bicarbonate (mEq/L), mean (SD) 22.6 (4.93) 23.5 (4.97)
Potassium (mEq/L), mean (SD) 4.22 (0.61) 4.38 (0.56)
On vasopressors, n (%) 34 (31) 52 (58)
On mechanical ventilation, n (%) 46 (41) 56 (62)
In ICU, n (%) 53 (48) 63 (70)
Non-B3, individuals not receiving niacinamide; B3, individuals receiving niacinamide; BMI, body mass index; COPD, chronic
obstructive pulmonary disease; HF, heart failure; EF, ejection fraction; ACEi, angiotensin-converting enzyme inhibitor; ARB,
angiotensin receptor blocker; KDIGO, Kidney Disease Improving Global Outcomes; WBC, white blood cell; ICU, intensive care unit.
a
Patients were enrolled in a clinical trial of remdesivir or sarilumab, and it is unknown if they were receiving study drug or placebo.
Among patients with KDIGO stage-1 AKI, we observed no Creatinine on the day of eligibility was similar between
reduced hazard for death or RRT. In contrast, niacinamide the B3 and non-B3 groups (Table 1). Over the 10 days after
was associated with lower risk of the primary outcome eligibility, we did not observe an overall significant differ-
among patients with more severe AKI (Table 2). ence in creatinine trends between the B3 and non-B3 groups
(P50.54). However, like the primary composite end point
and mortality, there were apparent differences on the basis
Secondary End Points of AKI severity.
When components of the composite end point were an- Among patients with KDIGO stage-2/3 AKI, creatinine
alyzed separately, the association with death was similar to values were similar in both groups on the day of eligibility
that for the combined end point. As with the primary out- (3.16 mg/dl in B3; 3.17 in non-B3; P50.99). These values
come, the association of niacinamide with mortality was increased significantly over the ensuing 10 days in the non-
significantly modified by KDIGO stage (P interaction50.008), B3 group by an average of 0.20 (SEM, 0.08) mg/dl per day,
with no significant association among patients with KDIGO whereas they remained flat in the B3 group (change of 0.01
stage-1 AKI, but approximately 80% lower hazard among [SEM, 0.06] mg/dl per day; P50.89). The adjusted difference
patients with KDIGO stage-2/3 AKI in the B3 group com- in these trends was statistically significant (P50.03). In
pared with the non-B3 group. The corresponding estimates contrast, creatinine demonstrated no significant linear trend
for RRT alone were all nonsignificant. over 10 days among patients with KDIGO stage-1 AKI,38 KIDNEY360
Table 2. Association between niacinamide use group and primary and secondary end points in the entire cohort and among KDIGO
subgroups
End Point Non-B3 (n5111) B3 (n590) P
RRT or death, n (%) 62 (56) 38 (42)
Unadjusted HR (95% CI) Ref 0.62 (0.42 to 0.94) 0.02
Adjusted HR (95% CI)a Ref 0.64 (0.40 to 1.00) 0.05
Adjusted HR (95% CI)
In patients with KDIGO stage-1 AKIb Ref 0.88 (0.51 to 1.53) 0.66
In patients with KDIGO stage-2/3 AKIc Ref 0.29 (0.13 to 0.65) 0.003
KDIGO interaction 0.03
Death alone, n (%) 49 (44.1) 22 (24.4)
Unadjusted HR (95% CI) Ref 0.45 (0.27 to 0.74) 0.002
Adjusted HR (95% CI)a Ref 0.59 (0.33 to 1.05) 0.07
Adjusted HR (95% CI)
In patients with KDIGO stage-1 AKIb Ref 1.06 (0.53 to 2.11) 0.87
In patients with KDIGO stage-2/3 AKIc Ref 0.17 (0.05 to 0.52) 0.002
KDIGO interaction 0.008
RRT alone, n (%) 23 (21) 23 (26)
Unadjusted HR (95% CI) Ref 1.11 (0.62 to 1.99) 0.72
Adjusted HR (95% CI)a Ref 1.02 (0.52 to 2.02) 0.95
Adjusted HR (95% CI) Ref
In patients with KDIGO stage-1 AKIb Ref 1.09 (0.46 to 2.78) 0.84
In patients with KDIGO stage-2/3 AKIc Ref 0.73 (0.25 to 2.16) 0.57
KDIGO interaction 0.56
Non-B3, individuals not receiving niacinamide; B3, individuals receiving niacinamide; HR, hazard ratio; KDIGO, Kidney Disease
Improving Global Outcomes.
a
Model adjusted for age; sex; history of diabetes, hypertension, malignancy, and heart failure with reduced ejection fraction; he-
moglobin, leukocyte count, platelet count, serum creatinine, potassium, and bicarbonate on the day of eligibility; preadmission use of
hepatic hydroxymethyl glutaryl–CoA reductase inhibitors, angiotensin-converting enzyme inhibitors, and angiotensin receptor
blockers; and requirement of the intensive care unit on day of eligibility. N5109 in the non-B3 group; N590 in the B3 group.
b
Model adjusted for the same variables as above. N583 in the non-B3 group; N568 in the B3 group.
c
Model adjusted for the same variables as above. N526 in the non-B3 group; N521 in the B3 group.
regardless of treatment group (change of 0.003 [SEM, 0.04] event analysis when compared with the non-B3 group
mg/dl per day in the non-B3 group; 0.007 [SEM, 0.02] mg/dl (Supplemental Table 4).
in the B3 group; P50.93). Repeated primary analyses with additional adjustment or
exclusions to ensure robustness yielded highly concordant
results (Supplemental Table 5), as did analyses using a single
Safety prognostic score covariate in place of separated covariates in
Nine of 79 (11%; 95% CI, 5% to 21%) individuals receiving the model (Supplemental Table 6). Baseline characteristics of
niacinamide in the B3 group had the medication stopped the B3 and non-B3 groups in the subset of individuals with
because of a three-fold increase in ALT compared with the KDIGO stage-2/3 AKI are shown in Supplemental Table 7.
first day they received niacinamide. Transaminitis (ALT
.200 IU/L) occurred in 13 out of 88 individuals (15%;
95% CI, 7% to 22%) in the B3 group who had at least one
ALT value measured post-AKI. No other adverse events Discussion
were reported in the B3 group. Whereas ALT was measured In this quasi-experimental study conducted in two large
within 24 hours of the day of eligibility and at least once in hospitals, implementation of a niacinamide protocol among
the 10 days afterward in 88 of 90 (98%) patients in the B3 patients with COVID-19-related AKI was associated with
group, these data were available in only 49 out of 91 (54%) lower risk for the composite of RRT or death, driven pri-
patients in the SH group. marily by a lower risk among the subset of patients with
KDIGO stage-2 or -3 AKI. Secondary end point analysis
showed that the difference in composite outcome was
Sensitivity Analyses driven by mortality and not RRT. Patients with KDIGO
Supplemental Table 2 repeats the time-to-event analyses stage-2/3 AKI in the B3 group demonstrated stable creat-
in Table 2, but with the pre-B3 and SH groups analyzed inine in the 10 days after diagnosis, whereas those in the
separately. We observed no significant difference between non-B3 group had increasing creatinine by an average of
the pre-B3 and SH groups for any outcome. 0.2 mg/dl per day.
We examined the association of calendar date with out- COVID-19 AKI affected 27% of patients hospitalized with
come in each treatment group and found no confounding by COVID-19 across the two institutions in this study. This
ongoing secular trends (Supplemental Table 3). proportion is between the 22% and 36% described among
Analysis of the 79 patients within the B3 group who hospitalized patients in reports from New York City (14,15).
actually received niacinamide showed a similarly reduced Given the substantial increase in mortality reported with
hazard for the primary end point in the adjusted time-to- AKI in patients hospitalized with COVID-19, the highKIDNEY360 2: 33–41, January, 2021 Niacinamide in COVID-19-Related AKI, Raines et al. 39 frequency of AKI represents a profound risk among patients precluding placebo controls. Our comparators were, there- who are already vulnerable. fore, either historical from the same hospital or contemporary The renal tubule is a known target of non-COVID-19 AKI, from another hospital. This precludes determination of cau- requiring constant energy from mitochondria for active solute sality. There was a significant age disparity between the B3 transport. Ischemic, inflammatory, and toxic stressors reduce and non-B3 groups, and there was disparity in race, certain renal NAD1, compromising transport function (5,16). Part of comorbidities, concurrent therapies, and rates of ICU utili- this shortfall may result from a local decrease of niacinamide zation. We performed statistical adjustments to address these and other biosynthetic precursors (4,5,17). If this energetic differences and, although age and certain comorbidities were deficit persists, acute tubular injury arises. Our results dem- significantly associated with outcomes, they did not substan- onstrate that niacinamide supplementation had no significant tially alter the association between B3 and our composite end association with measured outcomes in patients with KDIGO point, mortality alone, or creatinine trends after AKI. Of note, stage-1 AKI. On average, these individuals had no net in- the age discrepancy was mitigated in the subset of patients crease in serum creatinine after meeting eligibility regardless with KDIGO stage-2/3 AKI, among whom the associations of niacinamide administration, suggesting they were likely to were strongest. We also performed separate sensitivity anal- recover on their own regardless of therapy. Although spec- yses for variables of interest that could not be included in the ulative, individuals with mild AKI may not be sufficiently primary multivariate model, all of which yielded similar NAD1 deficient to benefit from NAD1 boosting. Consis- results. Unmeasured confounding is, nonetheless, still likely tently, experimental AKI models exhibit a proportional re- to have affected our results; the majority of patients in the lationship between renal NAD1 reduction and AKI severity non-B3 group were not at the same hospital as the B3 group, (5). Of note, results from the RECOVERY Trial demonstrate introducing different processes of care despite the use of the a similar trend for dexamethasone and mortality, with benefit same COVID-19 care algorithm. Availability of prior creat- seen only among patients who are sicker (18). inine values to determine an accurate baseline was variable, The absence of association between niacinamide and RRT and may have led to misclassification of AKI, particularly is notable. Three potential factors may have contributed to in the KDIGO stage-1 AKI group. Furthermore, whereas this finding. First, all patients in our study have AKI and, KDIGO guidelines support the use of a baseline creatinine hence, mortality among patients with AKI is essentially against which to evaluate in-hospital changes, we acknowl- a test of AKI prognosis. Second, as we discuss in our edge that application of a 0.3 mg/dl change could include too limitations below, timing of RRT may be less objective than many individuals with modest creatinine elevation that is not mortality. Third, although we observed a strong association consistent with AKI. However, inclusion of such individuals with mortality, we also observed a statistically significant is balanced between the groups and would tend to bias the association with improved creatinine trend. Creatinine results toward the null. Timing of RRT initiation can be trend and death may provide objective bookend indicators subjective, which, in the context of an open-label trial, intro- of the true effect, which is likely to be moderate. duces the potential for bias. However, mean serum creatinine Experimental results suggest that NAD1 augmentation at the time of RRT initiation was indistinguishable between may not only protect the kidney, but also fortify brain, heart, the groups. Moreover, mortality was the primary driver of lung, liver, and even vasculature against disease (19). Safety the composite end point rather than time to RRT initiation, analyses showed that, despite the subset of patients with which did not significantly differ between institutions. The AKI being sicker than the overall patient population hos- large effect size on the composite outcome and mortality pitalized with COVID-19, rates of transaminitis in individ- alone we report in the KDIGO stage-2/3 AKI group should uals receiving niacinamide were comparable with those not be considered definitive evidence of the magnitude of reported previously, although true rates of liver injury from niacinamide’s effect in this group. Finally, the number of COVID-19 remain poorly understood (20). Although this patients was relatively small, increasing the likelihood that study was focused on renal outcomes, the association of the large differences observed here may not hold when niacinamide with a reduction in mortality among patients applied to a broader population. Only a large randomized who are severely ill supports further investigation of NAD1 trial can establish whether niacinamide positively affects augmentation in preventing and treating extrarenal com- outcomes in COVID-19-related AKI. plications of COVID-19. This quasi-experimental study found that niacinamide Until an effective vaccine for COVID-19 is available, mod- administered for the prevention of COVID-19-related AKI ulating host susceptibility to adverse outcomes will also re- progression was safe and associated with reduced estimated main important. Compared with pharmacologic modulation risk of death or the need for RRT compared with historical of host susceptibility—e.g., with IL-6 inhibition—niacinamide controls and contemporaneous patients from a sister hos- is distinguished by its unique safety profile as a nutritional pital. The association was strongest in severe AKI. Creati- supplement generally recognized as safe and its inexpensive- nine levels also stabilized among patients with severe AKI ness. High-dose niacinamide has been safely administered for receiving niacinamide. Larger randomized studies of nia- months to patients with advanced CKD (10). Compared with cinamide in patients with COVID-19 are needed to confirm other NAD1 precursors, niacinamide also has the theoretic these apparent benefits. advantage of inhibiting stress-induced enzymes such as CD38 and poly-ADP ribose polymerases that hydrolyze Disclosures NAD1 and may be deleterious to organ function (19). A. Asnani reports being a scientific advisor or members of Sarnoff Our study has important limitations. Niacinamide out- Cardiovascular Research Foundation, and receiving honoraria from comes reflect a single-center experience. We made a practi- UpToDate. R.S. Brown received royalties from Börm Bruckmeier cal decision to offer niacinamide as standard treatment, Publishing LLC for a book and two applications, Nephrology Pocket
40 KIDNEY360
and Acid Base and Electrolytes, on smartphones, with the second Acknowledgments
edition of Nephrology Pocket to be published by Elsevier, Inc. In R.S. The authors would like to thank members of the Division of
Brown’s role at Harvard Medical Faculty Physicians (HMFP) at Beth Nephrology at Beth Israel Deaconess Medical Center for out-
Israel Deaconess Medical Center, he serves as an associate medical standing patient care under duress, generous input, and enthusi-
director of DaVita Dialysis Center (Brookline, MA). All income paid astic support of this protocol. They also thank the Department of
by this facility goes directly to HMFP, from which he receives a fixed Pharmacy and the Pharmacy and Therapeutics Committee at Beth
salary. He also reports receiving honoraria from Harvard Medical Israel Deaconess Medical Center.
School Department of Continuing Education, Beth Israel Deaconess
Medical Center; having ownership interest in Innovative Wellness
Systems, Inc.; being a member of the medical advisory board of the Author Contributions
National Kidney Foundation of New England; and being on the A. Asnani, R.S. Brown, S.M. Parikh, M. Sadrolashrafi, and M.L.
board of directors and president of The Organization for Renal Care Zeidel were responsible for resources; A. Asnani, S. Ganatra, A.
in Haiti (TORCH) Inc., a nonprofit, charitable corporation in Mas- Morales, P. Nissaisorakarn, A. Pandit, S.M. Parikh, N.H. Raines, and
sachusetts. No income is received from any of these entities. K. M. Sadrolashrafi were responsible for project administration; V.
Mukamal reports having other interests/relationships with US Bang, S. Brar, S.S. Dani, R. Maheshwari, A. Morales, P. Nissaisor-
Highbush Blueberry Council and Wolters Kluwer. S.M. Parikh is akarn, A. Pandit, S. M. Parikh, R. Patel, N.H. Raines, M. Sadro-
listed as an inventor on patent filings from Beth Israel Deaconess lashrafi, K. Shreyder, and A. Singh were responsible for in-
Medical Center related to NAD1. S.M. Parikh reports having con- vestigation; R. Bhargava, S. Ganatra, P. Nissaisorakarn, S.M. Parikh,
sultancy agreements with Aerpio, Alkermes, Astellas, Cytokinetics, N. H. Raines, J. Schlondorff, and T. I. Steinman provided super-
Hope Pharmaceuticals, Janssen, Leerink Swann, Mission Therapeu- vision; R.S. Brown, S.M. Parikh, A. Poyan Mehr, N.H. Raines, and
tics, and Mitobridge; being a scientific advisor for or member of M.L. Zeidel conceptualized the study; S. Ganatra, K.J. Mukamal,
Aerpio, JASN, Kidney360, and Raksana; receiving consulting fees in S.M. Parikh, and N.H. Raines wrote the original draft; S. Knapp,
the last 3 years from Alkermes, Astellas, Cytokinetics, Daiichi Sankyo, K.J. Mukamal, S.M. Parikh, and N.H. Raines were responsible for
Janssen, and Mission Therapeutics; receiving honoraria from data curation; K.J. Mukamal, S.M. Parikh, A. Poyan Mehr, and N.H.
American Society of Nephrology; receiving research funding from Raines were responsible for methodology; K.J. Mukamal, S.M.
Baxter; and having ownership interest in Eunoia and Raksana. Work Parikh, and N.H. Raines reviewed and edited the manuscript;
in S.M. Parikh’s laboratory is supported by National Heart, Lung, and K.J. Mukamal and N.H. Raines were responsible for formal analysis;
Blood Institute grant R35-HL139424, National Institute of Diabetes and S.M. Parikh was responsible for funding acquisition.
and Digestive and Kidney Diseases grant R01-DK095072, and Na-
tional Institute on Aging grant R01-AG027002. A. Poyan Mehr reports
receiving research funding from ASN Carl W. Gottschalk Research
Data Sharing Statement
Scholar Grant (2018) and Retrophin; being the site principle in-
The data that support the findings of this study are available on
vestigator for the DUPLEX Study (a phase-3 randomized trial in
request from the corresponding author S.M. Parikh, pending ap-
primary FSGS); having industry-sponsored clinical trial agreements
proval from our institutional review board. The data are not
with OMEROS, Roche, and Vertex; being the director of the GlomCon
publicly available because they contain information that could
Project, an initiative to enhance education about glomerular dis-
compromise research participant privacy.
orders. This project is collaborating closely with the NephCure
Foundation, which has provided financial and in-kind support for
a continuing medical education–accredited conference series focused Supplemental Material
on clinical trials. A. Poyan Mehr has additional educational collab- This article contains the following supplemental material online
orations with the Renal Pathology Society and the European Renal at http://kidney360.asnjournals.org/lookup/suppl/doi:10.34067/
Association. A. Poyan Mehr’s employer does not permit serving on KID.0006452020/-/DCSupplemental.
any speaker bureau, advisory board, perform consultancy, or receive Supplemental Table 1. Baseline characteristics of the B3, Pre-B3,
industry honoraria. N.H. Raines reports being a scientific advisor for and SH groups
or member of La Isla Network. J. Schlondorff reports being a scientific Supplemental Table 2. Associations among B3 group, pre-B3
advisor for or member of the Alport Syndrome Foundation Medical group, and sister hospital (SH) for composite endpoint of RRT or
Advisory Committee and having patents and inventions with Part- death, death alone, and RRT alone.
ners Healthcare. T.I. Steinman reports being a reviewer for CJASN Supplemental Table 3. Association between AKI date and pri-
and a member of the editorial board for Nephrology News and Issues; mary and secondary outcomes in B3 hospital and sister hospital.
receiving research funding from Kadmon, Reata, and Retrophin; Supplemental Table 4. Adjusted time-to-event analysis in subset
receiving honoraria from Mallinkrodt and Otsuka; being on the of B3 group receiving one or more doses of niacinamide (per-pro-
medical advisory board for the National Kidney Foundation of tocol) compared to non-B3 group.
Supplemental Table 5. Additional sensitivity analyses exploring
Massachusetts, Rhode Island, New Hampshire, and Vermont; and
the association between niacinamide use group and primary and sec-
having other interests/relationships with National Kidney Founda-
ondary endpoints in the entire cohort and among KDIGO subgroups.
tion and Polycystic Kidney Foundation. M.L. Zeidel reports being
Supplemental Table 6. Association between niacinamide use
a scientific advisor for or member of the Beth Israel Deaconess
group and primary and selected secondary endpoints in the entire
Medical Center and Hebrew Senior Life. All remaining authors have
cohort and among KDIGO subgroups using prognostic scoring.
nothing to disclose.
Supplemental Table 7. Characteristics of patients with KDIGO
stage 2 or 3 AKI in B3 group and non-B3 groups.
Funding Supplemental Material 1. Supplemental Methods.
N.H. Raines is supported by National Institute of Diabetes and Supplemental Material 2. Study protocol.
Digestive and Kidney Diseases grant T32-DK007199. Supplemental References.KIDNEY360 2: 33–41, January, 2021 Niacinamide in COVID-19-Related AKI, Raines et al. 41
References niacinamide for reduction of phosphorus in hemodialysis
1. Su H, Yang M, Wan C, Yi LX, Tang F, Zhu HY, Yi F, Yang HC, Fogo patients. Clin J Am Soc Nephrol 3: 1131–1138, 2008 https://
AB, Nie X, Zhang C: Renal histopathological analysis of 26 doi.org/10.2215/CJN.04211007
postmortem findings of patients with COVID-19 in China. Kidney 12. Kidney Disease: Improving Global Outcomes (KDIGO): 2012
Int 98: 219–227, 2020 https://doi.org/10.1016/ Kidney Disease: Improving Global Outcomes (KDIGO) Clinical
j.kint.2020.04.003 Practice Guideline for Acute Kidney Injury (AKI). Available at:
2. Abelson R, Fink S, Kulish N, Thomas K: An overlooked, possibly https://kdigo.org/guidelines/acute-kidney-injury/. Accessed
fatal coronavirus crisis: A dire need for kidney dialysis. New York March 25, 2020
Times, 2020 13. Palevsky PM: Endpoints for clinical trials of acute kidney injury.
3. Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, Li J, Yao Y, Nephron 140: 111–115, 2018 https://doi.org/10.1159/
Ge S, Xu G: Kidney disease is associated with in-hospital death of 000493203
patients with COVID-19. Kidney Int 97: 829–838, 2020 https:// 14. Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL,
doi.org/10.1016/j.kint.2020.03.005 Hazzan AD, Fishbane S, Jhaveri KD; Northwell COVID-19 Re-
4. Poyan Mehr A, Tran MT, Ralto KM, Leaf DE, Washco V, Messmer search Consortium; Northwell Nephrology COVID-19 Research
J, Lerner A, Kher A, Kim SH, Khoury CC, Herzig SJ, Trovato ME, Consortium: Acute kidney injury in patients hospitalized with
Simon-Tillaux N, Lynch MR, Thadhani RI, Clish CB, Khabbaz KR, COVID-19. Kidney Int 98: 209–218, 2020 https://doi.org/
Rhee EP, Waikar SS, Berg AH, Parikh SM: De novo NAD1 bio- 10.1016/j.kint.2020.05.006
synthetic impairment in acute kidney injury in humans. Nat Med 15. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T,
24: 1351–1359, 2018 https://doi.org/10.1038/s41591-018-0138- Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL,
z Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-
5. Tran MT, Zsengeller ZK, Berg AH, Khankin EV, Bhasin MK, Kim Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk
W, Clish CB, Stillman IE, Karumanchi SA, Rhee EP, Parikh SM: DA, Kim EJ, Kozel ZM, Marrast LM, Mogavero JN, Osorio GA,
PGC1a drives NAD biosynthesis linking oxidative metabolism to Qiu M, Zanos TP; the Northwell COVID-19 Research Consor-
renal protection. Nature 531: 528–532, 2016 https://doi.org/ tium: Presenting characteristics, comorbidities, and outcomes
10.1038/nature17184 among 5700 patients hospitalized with COVID-19 in the New
6. Goldman JD, Lye DCB, Hui DS, Marks KM, Bruno R, Montejano York city area [published correction appears in JAMA 323: 2098,
R, Spinner CD, Galli M, Ahn MY, Nahass RG, Chen YS, SenGupta 2020 10.1001/jama.2020.7681]. JAMA 323: 2052–2059, 2020
D, Hyland RH, Osinusi AO, Cao H, Blair C, Wei X, Gaggar A, https://doi.org/10.1001/jama.2020.6775
Brainard DM, Towner WJ, Mu~ noz J, Mullane KM, Marty FM, 16. Lynch MR, Tran MT, Ralto KM, Zsengeller ZK, Raman V, Bhasin
Tashima KT, Diaz G, Subramanian A; GS-US-540-5773 Inves- SS, Sun N, Chen X, Brown D, Rovira II, Taguchi K, Brooks CR,
tigators: Remdesivir for 5 or 10 days in patients with severe covid- Stillman IE, Bhasin MK, Finkel T, Parikh SM: TFEB-driven lyso-
19. N Engl J Med 383: 1827–1837, 2020 https://doi.org/10.1056/ somal biogenesis is pivotal for PGC1a-dependent renal stress
NEJMoa2015301 resistance. JCI Insight 5: e126749, 2019 https://doi.org/10.1172/
7. Gale EA, Bingley PJ, Emmett CL, Collier T; European Nicotin- jci.insight.126749
amide Diabetes Intervention Trial (ENDIT) Group: European 17. Katsyuba E, Mottis A, Zietak M, De Franco F, van der Velpen V,
Nicotinamide Diabetes Intervention Trial (ENDIT): A randomised Gariani K, Ryu D, Cialabrini L, Matilainen O, Liscio P, Giacchè N,
controlled trial of intervention before the onset of type 1 diabetes. Stokar-Regenscheit N, Legouis D, de Seigneux S, Ivanisevic J,
Lancet 363: 925–931, 2004 https://doi.org/10.1016/S0140- Raffaelli N, Schoonjans K, Pellicciari R, Auwerx J: De novo
6736(04)15786-3 NAD1 synthesis enhances mitochondrial function and improves
8. Knip M, Douek IF, Moore WP, Gillmor HA, McLean AE, Bingley health. Nature 563: 354–359, 2018 https://doi.org/10.1038/
PJ, Gale EA; European Nicotinamide Diabetes Intervention Trial s41586-018-0645-6
Group: Safety of high-dose nicotinamide: A review. Diabetologia 18. Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L,
43: 1337–1345, 2000 https://doi.org/10.1007/s001250051536 Staplin N, Brightling C, Ustianowski A, Elmahi E, Prudon B,
9. Chen AC, Martin AJ, Choy B, Fernández-Pe~ nas P, Dalziell RA, Green C, Felton T, Chadwick D, Rege K, Fegan C, Chappell LC,
McKenzie CA, Scolyer RA, Dhillon HM, Vardy JL, Kricker A, St Faust SN, Jaki T, Jeffery K, Montgomery A, Rowan K, Juszczak E,
George G, Chinniah N, Halliday GM, Damian DL: A phase 3 Baillie JK, Haynes R, Landray MJ; RECOVERY Collaborative
randomized trial of nicotinamide for skin-cancer chemo- Group: Dexamethasone in hospitalized patients with covid-19 –
prevention. N Engl J Med 373: 1618–1626, 2015 https://doi.org/ preliminary report [published online ahead of print July 17,
10.1056/NEJMoa1506197 2020]. N Engl J Med
10. Ix JH, Isakova T, Larive B, Raphael KL, Raj DS, Cheung AK, 19. Katsyuba E, Auwerx J: Modulating NAD1 metabolism, from
Sprague SM, Fried LF, Gassman JJ, Middleton JP, Flessner MF, bench to bedside. EMBO J 36: 2670–2683, 2017 https://doi.org/
Block GA, Wolf M: Effects of nicotinamide and lanthanum car- 10.15252/embj.201797135
bonate on serum phosphate and fibroblast growth factor-23 in 20. Zhang C, Shi L, Wang FS: Liver injury in COVID-19: Management
CKD: The COMBINE trial. J Am Soc Nephrol 30: 1096–1108, and challenges. Lancet Gastroenterol Hepatol 5: 428–430, 2020
2019 https://doi.org/10.1681/ASN.2018101058 https://doi.org/10.1016/S2468-1253(20)30057-1
11. Cheng SC, Young DO, Huang Y, Delmez JA, Coyne DWA: A
randomized, double-blind, placebo-controlled trial of Received: October 28, 2020 Accepted: November 20, 2020SUPPLEMENTARY APPENDIX for “Niacinamide may be Associated with Improved
Outcomes in COVID-19 Related Acute Kidney Injury: An Observational Study”
Authors: Nathan H. Raines MD MPH1, Sarju Ganatra MD2, Pitchaphon Nissaisorakarn MD1,
Amar Pandit MD1, Alex Morales MD1, Aarti Asnani MD3, Mehrnaz Sadrolashrafi PharmD4, Rahul
Maheshwari MD5, Rushin Patel MD2, Vigyan Bang MD2, Katherine Shreyder MD2, Simarjeet Brar
MD2, Amitoj Singh MD2, Sourbha S. Dani MD2, Sarah Knapp MD6, Ali Poyan Mehr MD7, Robert
S. Brown MD1, Mark L. Zeidel1, Rhea Bhargava MD1, Johannes Schlondorff MD1, Theodore I
Steinman MD1, Kenneth J. Mukamal MD MPH5, Samir M. Parikh MD1
1
Division of Nephrology, Department of Medicine, Beth Israel Deaconess Medical Center and
Harvard Medical School, Boston MA
2
Division of Cardiovascular Medicine, Department of Medicine, Lahey Hospital, Burlington MA
3
Division of Cardiology, Department of Medicine, Beth Israel Deaconess Medical Center and
Harvard Medical School, Boston MA
4
Department of Pharmacy, Beth Israel Deaconess Medical Center and Harvard Medical School,
Boston MA
5
Division of General Medicine, Department of Medicine, Beth Israel Deaconess Medical Center
and Harvard Medical School, Boston MA
6
Division of Endocrinology, Department of Medicine, Beth Israel Deaconess Medical Center and
Harvard Medical School, Boston MA
7
Division of Research, Kaiser Permanente, San Francisco, CA
1TABLE OF CONTENTS Page
Supplemental Table 1. Baseline characteristics of the B3, Pre-B3, and SH groups 3
Supplemental Table 2. Associations among B3 group, pre-B3 group, and sister
hospital (SH) for composite endpoint of RRT or death, death alone, and RRT alone. 5
Supplemental Table 3. Association Between AKI date and primary and secondary
outcomes in B3 hospital and sister hospital. 7
Supplemental Table 4. Adjusted time-to-event analysis in subset of B3 group
receiving one or more doses of niacinamide (per-protocol) compared to non-B3 group 8
Supplemental Table 5. Additional Sensitivity Analyses Exploring the Association
between Niacinamide Use Group and Primary and Secondary Endpoints in the Entire
Cohort and among KDIGO Subgroups. 9
Supplemental Table 6. Association between Niacinamide Use Group and Primary
and Selected Secondary Endpoints in the Entire Cohort and among KDIGO
Subgroups using Prognostic Scoring 12
Supplemental Table 7. Characteristics of patients with KDIGO stage 2 or 3 AKI in
B3 group and non-B3 groups. 13
Supplement 1. Supplemental Methods 15
Supplement 2. Study Protocol 18
Supplemental References. 22
2Supplemental Table 1. Baseline characteristics of the B3, Pre-B3, and SH groups
B3 (n = 90) Pre-B3 (n = 20) SH (n = 91)
Age (y) - mean (SD) 65.6 (15.2) 65.9 (14.3) 74.6 (11.5)
Female - no. (%) 40 (44) 8 (40) 36 (40)
Race - no (%)
White non-Hispanic 27 (30) 11 (55) 80 (88)
Black non-Hispanic 31 (34) 3 (15) 8 (9)
Hispanic 13 (14) 2 (10) 3 (3)
Asian 3 (3) 2 (10) 0 (0)
Other 16 (18) 2 (10) 0 (0)
BMI - mean (SD) 32.2 (7.9) 31.0 (6.9) 30.3 (8.0)
Baseline Creatinine (mg/dL) - 1.20 (0.55) 0.94 (0.39) 1.22 (0.48)
mean (SD)
GFRCreatinine (mg/dL) - mean (SD) 2.10 (1.32) 1.75 (1.16) 2.09 (1.38)
KDIGO AKI stage - n (%)
Stage 1 68 (76) 15 (75) 70 (77)
Stage 2 13 (15) 3 (15) 13 (14)
Stage 3 8 (9) 2 (10) 8 (9)
Hemoglobin (g/dL) - mean (SD) 10.7 (2.2) 11.4 (2.0) 11.4 (1.9)
WBC count (K/uL) - mean (SD) 9.4 (5.2) 10.1 (4.3) 8.3 (4.1)
Platelet count (K/uL) - mean (SD) 255 (130) 210 (126) 217 (104)
Bicarbonate (mEq/L) - mean (SD) 23.5 (5.0) 22.6 (6.0) 22.6 (4.7)
Potassium (mEq/L) - mean (SD) 4.38 (0.56) 4.39 (0.61) 4.18 (0.61)
On vasopressors - n (%) 52 (58) 9 (45) 25 (28)
On mechanical ventilation - n (%) 56 (62) 11 (55) 35 (39)
In ICU - n (%) 63 (70) 12 (60) 41 (45)
aPatients were enrolled in a clinical trial of remdesivir or sarilumab, and it is unknown if they were
receiving study drug or placebo.
Abbreviations: SD, standard deviation; BMI, body mass index; eGFR, estimated glomerular filtration rate;
COPD, chronic obstructive pulmonary disease; HF with reduced EF, heart failure with reduced ejection
fraction; ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; KDIGO,
Kidney Disease Improving Global Outcomes; AKI, acute kidney injury. WBC, white blood cell; ICU,
intensive care unit.
4Supplemental Table 2. Associations among B3 group, pre-B3 group, and sister hospital
(SH) for composite endpoint of RRT or death, death alone, and RRT alone.
SH (n=91) Pre-B3 (n=20) p B3 (n=90) p
RRT or Death 52 (57.1) 10 (50.0) 38 (42.2)
HR (95% CI) Unadjusted ref 0.87 (0.44 to 1.72) 0.70 0.61 (0.40 to 0.93) 0.02
HR (95% CI) adjusteda ref 0.80 (0.37 to 1.74) 0.57 0.61 (0.38 to 0.98) 0.04
HR (95% CI) adjusted:
In patients with KDIGO1b ref 0.77 (0.48 to 1.50) 0.57 0.83 (0.48 to 1.46) 0.42
In patients with KDIGO 2 or 3c ref 0.55 (0.17 to 1.82) 0.33 0.26 (0.11 to 0.60) 0.002
KDIGO interaction 0.65 0.02
Death 41 (45.1) 8 (40.0) 22 (24.4)
HR (95% CI) Unadjusted ref 0.94 (0.44 to 2.01) 0.88 0.44 (0.26 to 0.74) 0.002
HR (95% CI) adjusteda ref 1.07 (0.44 to 2.59) 0.89 0.59 (0.33 to 1.09) 0.09
HR (95% CI) adjusted:
In patients with KDIGO1b ref 1.20 (0.38 to 3.79) 0.76 1.05 (0.53 to 2.11) 0.88
In patients with KDIGO 2 or 3c ref 0.69 (0.17 to 2.75) 0.60 0.16 (0.05 to 0.52) 0.002
KDIGO interaction 0.53 0.008
RRT 17 (18.7) 6 (30.0) 23 (25.6)
HR (95% CI) Unadjusted ref 1.59 (0.63 to 4.02) 0.33 1.23 (0.66 to 2.31) 0.52
HR (95% CI) adjusteda ref 1.26 (0.38 to 4.20) 0.71 1.09 (0.51 to 2.31) 0.83
HR (95% CI) adjusted:
In patients with KDIGO1b ref 1.56 (0.35 to 6.89) 0.56 1.11 (0.45 to 2.75) 0.82
In patients with KDIGO 2 or 3c ref 0.68 (0.12 to 3.88) 0.66 0.75 (0.23 to 2.43) 0.64
KDIGO interaction 0.44 0.58
a
Model adjusted for age; sex; history of diabetes, hypertension, malignancy, and heart failure with reduced
ejection fraction; hemoglobin, leukocyte count, platelet count, and serum creatinine, potassium, and
bicarbonate on the day of eligibility; pre-admission use of HMG-CoA reductase inhibitors, angiotensin
converting enzyme inhibitors, and angiotensin receptor blockers; and intensive care unit requirement on
day of eligibility. N = 89 in the SH group, 20 in the pre-B3 group, and 90 in the B3 group.
5b
Model adjusted for same variables as above. N = 68 in the SH group, 15 in the pre-B3 group, and 68 in
the B3 group.
c
Model adjusted for same variables as above. N = 20 in the SH group, 5 in the pre-B3 group, and 21 in the
B3 group.
Abbreviations: RRT, renal replacement therapy; HR, hazard ratio; CI, confidence interval; KDIGO, Kidney
Disease Improving Global Outcomes.
6Supplemental Table 3. Association between AKI date and primary and secondary
outcomes in B3 hospital and sister hospitals.
HR (95% CI) per 1 day increase in date p
B3 Hospital (During B3 Protocol) (n=90)
Death or RRT 1.06 (0.99 to 1.13) 0.10
Death alone 1.03 (0.95 to 1.12) 0.60
RRT alone 1.04 (0.96 to 1.13) 0.34
B3 Hospital (Pre- B3 Protocol) (n=20)
Death or RRT 1.12 (0.92 to 1.36) 0.25
Death alone 1.10 (0.89 to 1.37) 0.38
RRT alone 1.04 (0.83 to 1.31) 0.73
Sister Hospital (n=91)
Death or RRT 0.99 (0.96 to 1.03) 0.75
Death alone 1.01 (0.97 to 1.05) 0.61
RRT alone 0.96 (0.90 to 1.02) 0.17
Abbreviations: RRT, renal replacement therapy; HR, hazard ratio; CI, confidence interval.
7Supplemental Table 4. Adjusted time-to-event analysis in subset of B3 group receiving
one or more doses of niacinamide (per-protocol) compared to non-B3 group
Non-B3 B3 receiving niacinamide p
RRT or Death
All patients - HR (95% CI)a ref 0.55 (0.34 to 0.89) 0.02
KDIGO 1 Patientsb ref 0.75 (0.41 to 1.34) 0.34
KDIGO 2/3 Patientsc ref 0.27 (0.12 to 0.64) 0.03
KDIGO Interaction 0.06
Death Alone
All patients - HR (95% CI)a ref 0.46 (0.24 to 0.86) 0.02
KDIGO 1 Patientsb ref 0.75 (0.34 to 1.68) 0.49
KDIGO 2/3 Patientsc ref 0.20 (0.07 to 0.61) 0.005
KDIGO Interaction 0.07
RRT Alone
All patients - HR (95% CI)a ref 0.95 (0.48 to 1.89) 0.88
KDIGO 1 Patientsb ref 1.13 (0.48 to 2.69) 0.78
KDIGO 2/3 Patientsc ref 0.57 (0.19 to 1.74) 0.32
KDIGO Interaction 0.34
a
Model adjusted for age; sex; history of diabetes, hypertension, malignancy, and heart failure with reduced
ejection fraction; hemoglobin, leukocyte count, platelet count, and serum creatinine, potassium, and
bicarbonate on the day of eligibility; pre-admission use of HMG-CoA reductase inhibitors, angiotensin
converting enzyme inhibitors, and angiotensin receptor blockers; and intensive care unit requirement on
day of eligibility. N = 109 in the Non-B3 group, 79 in the B3 group.
b
Model adjusted for same variables as above. N = 83 in the Non-B3 group, 60 in the B3 group.
c
Model adjusted for same variables as above. N = 26 in the Non-B3 group, 18 in the B3 group.
Abbreviations: RRT, renal replacement therapy; HR, hazard ratio; CI, confidence interval; KDIGO, Kidney
Disease Improving Global Outcomes.
8Supplemental Table 5. Additional sensitivity analyses exploring the association between
niacinamide use group and primary and secondary endpoints in the entire cohort and
among KDIGO subgroups.
Non-B3 B3 p
Adjusted model,a with addition of race
Death or RRT, KDIGO 1 patients - HR (95% CI)b ref 0.77 (0.42 to 1.42) 0.41
Death or RRT, KDIGO 2/3 patients - HR (95% CI)c ref 0.25 (0.11 to 0.58) 0.001
KDIGO Interaction 0.02
Death alone, KDIGO 1 patients - HR (95% CI)b ref 1.32 (0.63 to 2.77) 0.47
Death alone, KDIGO 2/3 patients - HR (95% CI)c ref 0.23 (0.07 to 0.74) 0.01
KDIGO Interaction 0.01
RRT alone, KDIGO 1 patients - HR (95% CI)b ref 0.87 (0.34 to 2.25) 0.78
RRT alone, KDIGO 2/3 patients - HR (95% CI)c ref 0.52 (0.17 to 1.65) 0.27
KDIGO Interaction 0.46
Adjusted model,a with addition of BMI
Death or RRT, KDIGO 1 patients - HR (95% CI)d ref 0.85 (0.48 to 1.49) 0.56
Death or RRT, KDIGO 2/3 patients - HR (95% CI)e ref 0.35 (0.15 to 0.81) 0.01
KDIGO Interaction 0.08
Death alone, KDIGO 1 patients - HR (95% CI)d ref 0.77 (0.55 to 2.26) 0.77
Death alone, KDIGO 2/3 patients - HR (95% CI)e ref 0.17 (0.05 to 0.56) 0.004
KDIGO Interaction 0.009
RRT alone, KDIGO 1 patients - HR (95% CI)d ref 1.08 (0.45 to 2.60) 0.87
RRT alone, KDIGO 2/3 patients - HR (95% CI)e ref 0.80 (0.26 to 2.42) 0.69
KDIGO Interaction 0.68
Adjusted model,a with addition ever smoking and
COPD/asthma
Death or RRT, KDIGO 1 patients - HR (95% CI)f ref 0.85 (0.48 to 1.53) 0.59
9Death or RRT, KDIGO 2/3 patients - HR (95% CI)g ref 0.30 (0.13 to 0.68) 0.004
KDIGO Interaction 0.04
Death alone, KDIGO 1 patients - HR (95% CI)f ref 1.06 (0.52 to 2.19) 0.87
Death alone, KDIGO 2/3 patients - HR (95% CI)g ref 0.16 (0.05 to 0.48) 0.001
KDIGO Interaction 0.006
RRT alone, KDIGO 1 patients - HR (95% CI)f ref 1.15 (0.45 to 2.93) 0.77
RRT alone, KDIGO 2/3 patients - HR (95% CI)g ref 0.75 (0.26 to 2.22) 0.61
KDIGO Interaction 0.55
Adjusted model,a excluding individuals taking or
in trials of remdesivir, sarulimab, or tociluzimab
Death or RRT, KDIGO 1 patients - HR (95% CI)h ref 0.96 (0.46 to 1.95) 0.91
Death or RRT, KDIGO 2/3 patients - HR (95% CI)i ref 0.19 (0.06 to 0.61) 0.005
KDIGO Interaction 0.02
Death alone, KDIGO 1 patients - HR (95% CI)h ref 1.17 (0.50 to 2.73) 0.72
Death alone, KDIGO 2/3 patients - HR (95% CI)i ref 0.11 (0.02 to 0.62) 0.01
KDIGO Interaction 0.02
RRT alone, KDIGO 1 patients - HR (95% CI)h ref 1.10 (0.32 to 3.79) 0.89
RRT alone, KDIGO 2/3 patients - HR (95% CI)i ref 1.13 (0.24 to 5.33) 0.88
KDIGO Interaction 0.98
a
Model adjusted for age; sex; history of diabetes, hypertension, malignancy, and heart failure with reduced
ejection fraction; hemoglobin, leukocyte count, platelet count, and serum creatinine, potassium, and
bicarbonate on the day of eligibility; pre-admission use of HMG-CoA reductase inhibitors, angiotensin
converting enzyme inhibitors, and angiotensin receptor blockers; and intensive care unit requirement on
day of eligibility.
b
N = 83 in the Non-B3 group, 68 in the B3 group.
c
N = 26 in the Non-B3 group, 21 in the B3 group.
d
N = 83 in the Non-B3 group, 65 in the B3 group.
e
N = 25 in the Non-B3 group, 18 in the B3 group.
f
N = 83 in the Non-B3 group, 66 in the B3 group.
g
N = 26 in the Non-B3 group, 21 in the B3 group.
h
N = 73 in the Non-B3 group, 40 in the B3 group.
i
N = 22 in the Non-B3 group, 11 in the B3 group.
10Abbreviations: RRT, renal replacement therapy; HR, hazard ratio; CI, confidence interval; KDIGO, Kidney
Disease Improving Global Outcomes; BMI, body mass index; COPD, chronic obstructive pulmonary
disease.
11You can also read