Oncology Care Model (OCM) Overview - The Physicians Advocacy Institute's Medicare Quality Payment Program (QPP) Physician Education Initiative
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Physicians Advocacy Institute’s
Medicare Quality Payment Program (QPP)
Physician Education Initiative
Oncology Care Model (OCM) Overview
1|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/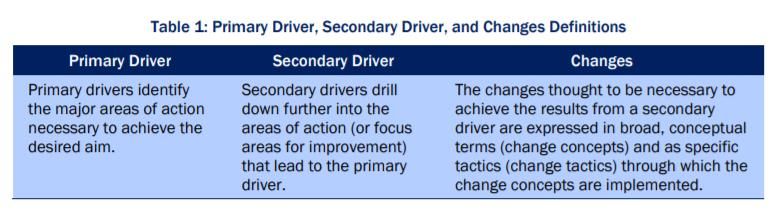
MEDICARE QPP PHYSICIAN EDUCATION INITIATIVE
Oncology Care Model Overview
IMPORTANT NOTE: The Oncology Care Model (OCM) is set to sunset in June 2022. The Model was
originally set to conclude in June 2021 but due to the COVID-19 public health emergency (PHE), it was
extended for an additional year. CMMI has introduced a new payment and service delivery model that
builds on and is set to replace OCM called Oncology Care First (OCF). CMMI has not yet released the
Request for Applications (RFA) for OCF. The information below has been updated to reflect changes for
performance year 2022.
An Advanced Alternative Payment Model (APM) is one of two pathways physicians can choose
under the Quality Payment Program (QPP), which was established as part of the Medicare Access
and CHIP Reauthorization Act (MACRA). Under the Advanced APM pathway, physicians may be
exempt from participation in the Merit-based Incentive Payment System (MIPS) and be eligible to
receive a 5% incentive payment. For successful participation in an Advanced APM, physicians need
to consider three core building blocks:
Understanding the Understanding the
Understanding the
variables and rules relevant QPP rules
basic principles of
impacting performance relating to participation
population health
under specific thresholds and
models
Advanced APMs requirements
This resource focuses on the second of these three building blocks: understanding the variables
and rules impacting performance under specific Advanced APMs, specifically the OCM. The OCM
2|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/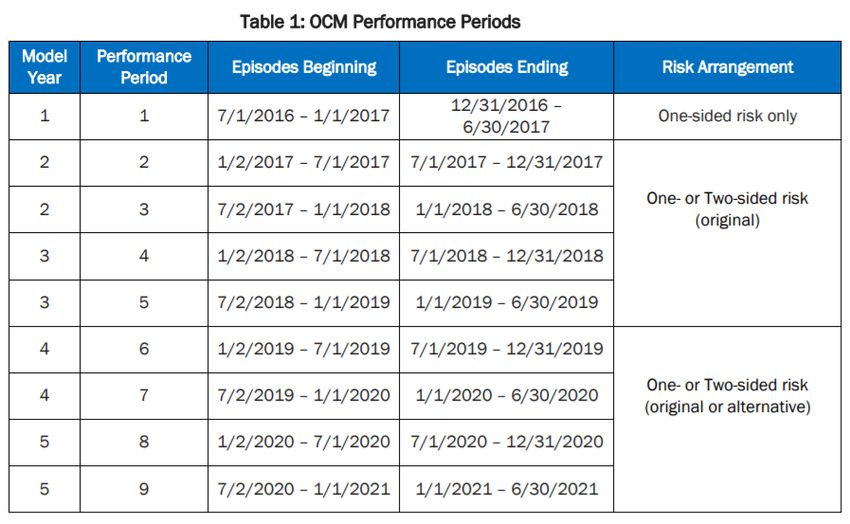
is a 5-year model focused on increasing the coordination of oncology care through financial and
performance accountability for chemotherapy episodes of care. There are currently 126 practices
and 5 commercial payers participating in the OCM.
Under the OCM, participation is at the practice level, and practices participating in the model
commit to providing enhanced care coordination, navigation, and treatment guidelines for cancer
patients receiving chemotherapy. The OCM is structured as a 6-month episode-based payment
model that begins when a patient receives a qualifying chemotherapy treatment, and includes the
total care provided to the patient during that 6-month period, including non-oncology care. The
performance period of this model began on July 1, 2016, and is slated to end June 30, 2022.
While the OCM is a two-part model and engages with payers outside of Medicare, the focus of this
overview is on the Medicare component of the model for the QPP Advanced APM pathway.
What is the goal of the OCM?
The goal of the OCM is to provide higher quality and coordinated oncology care. Through its
financial incentives, the OCM encourages practices to work collaboratively with other clinicians to
address the complex needs of cancer patients receiving chemotherapy.
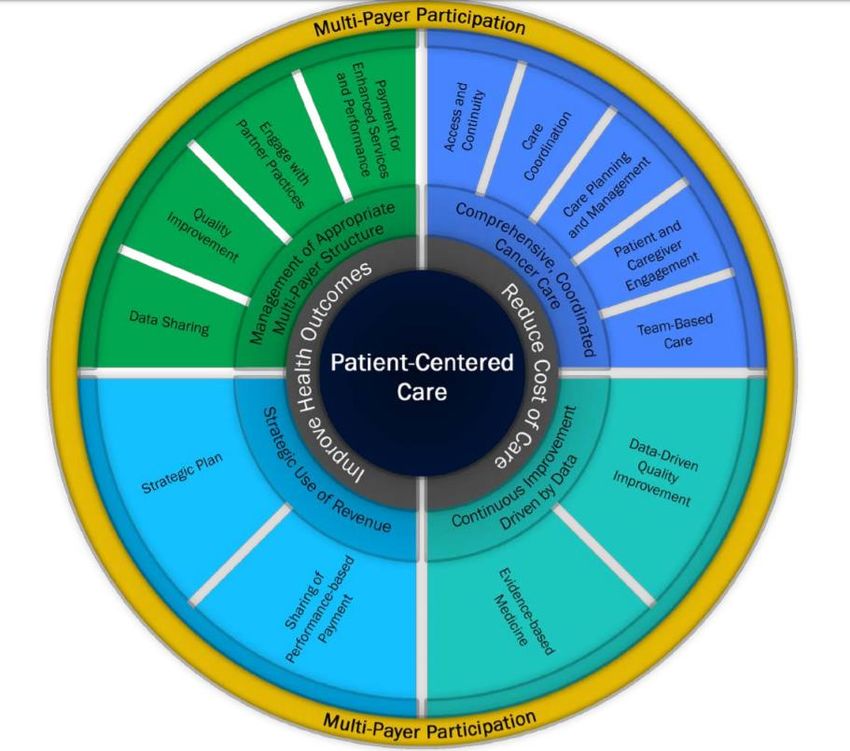
To achieve this goal, CMS utilizes a “Key Drivers and Changes” framework for participating
practices to use as an assessment tool for redesigning their care approach. There are two key
components to this framework: primary drivers and secondary drivers.
The CMS diagram below provides a visual representation of how CMS intends for practices to
use the Key Drivers and Changes framework to meet the aim of the OCM.
3|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/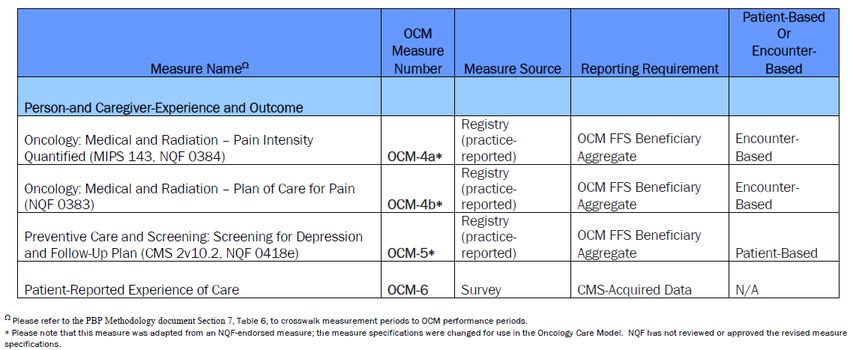
For additional information, see the revised June 1, 2020 Center for Medicare and Medicaid
Innovation’s OCM Key Drivers and Change Package.
OCM Patient Eligibility
Only those patients who meet the following criteria will be included in the OCM 6- month episode:
• Are enrolled in Medicare Parts A and B
• Do not have end-stage renal disease (ESRD)
• Have Medicare fee-for-service (FFS) as their primary payer
• Are not covered under Medicare Advantage or other group health program
• Receive an included chemotherapy treatment for cancer under management of an OCM
participating practice, and
Have at least one evaluation and management visit (CPT® codes 99201-99205 and 99211-
99215) with an included cancer diagnosis during a 6 month period that begins with receipt
of chemotherapy treatment.
4|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/
OCM Qualifying Treatment Episodes
A patient’s episode of care begins on the date of an initial Medicare Part B or Part D chemotherapy
claim; it does not include services provided prior to that date. Once the episode begins, it includes
all Medicare Part A and Part B services and costs that the patient receives during the 6-month
episode period. Certain Part D expenditures are also included in the total cost of care for the
episode. A list of qualifying chemotherapy drugs can be found here.
A single episode of care, for purposes of the OCM, ends 6 months after the patient first begins
chemotherapy. If the patient receives chemotherapy after the end of the episode (after the 6-
month period), that will begin a new 6-month episode for the OCM.
Note: A hospital inpatient chemotherapy claim (billed under the OPPS) will not initiate an OCM
care episode. Additionally, cancer types treated exclusively with surgery, radiation, or topical
chemotherapy are excluded from the model.
Payment Mechanisms
During their participation in the OCM, practices will continue to be paid through Medicare FFS,
but they will receive a two-part payment. The two-part payment includes a per-beneficiary-per-
month (PBPM) payment, known as the Monthly Enhanced Oncology Services (MEOS) payment,
and a performance-based payment (PBP).
MEOS Payment PBP
•A flat payment of $160 per-beneficiary-per- •Calculated retrospectively on a semi-annual
month or $960 per six-month episode. basis.
•Provided to the OCM practice for managing and •Based on a practice's OCM quality measure
coordinating the patient's care. performance and how much money it saves
relative to a target price established by CMS.
Calculating the Benchmark
CMS calculates a benchmark episode for each OCM practice based on risk-adjusted historical data
that is trended forward to the performance period and that includes a novel therapies adjustment.
This benchmark is then discounted to arrive at a target price for the OCM episodes. The amount
of the discount applied is determined by the risk arrangement chosen by the practice.
Risk Arrangements
5|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/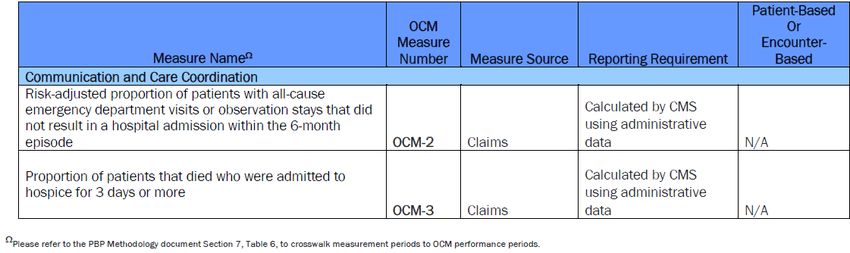
The OCM features three risk arrangements: a one-sided risk model, and a two-sided risk model
(original), and a two-sided risk model (alternative).
One-Sided Risk Model Two-Sided Risk Model (Original) Two-Sided Risk Model (Alternative)
•Medicare discount = 4% •Medicare discount = 2.75% •Medicare discount = 2.5%
•OCM practice receives a PBP if •OCM practice receives a PBP if •OCM practice receives a PBP if
total actual expenditures for total actual expenditures for total actual expenditures for
episodes are below the target episodes are below the target episodes are below the target
price price price
•OCM practice not responsible if its •OCM practice receives no PBP and •OCM practice receives no PBP and
total actual expenditures for the the practice is responsible for total practice is responsible for the total
episodes exceed the target price actual expenditures that exceed expenditures that exceed the
•Must qualify for PBP by mid-2019 the target price (capped at 20% of target price (capped at 8% of Total
to remain in the one-sided risk benchmark) Part B revenue)
model
Under the two-sided risk model, if a practice’s total actual expenditures exceed the target price,
the practice must pay back to CMS the difference between the target price and the actual
expenditures (called a recoupment). The recoupment will be adjusted for geographic variation and
reduced for sequestration (if applied). A performance multiplier is not applied to the recoupment.
Due to COVID-19, OCM practices can elect to forgo upside and downside risk for performance
periods affected by the PHE. For OCM practices that remain in one- or two-sided risk for the
performance periods affected by the PHE, COVID-19 episodes will be removed from reconciliation
for those performance periods.
To learn more about the OCM payment methodology and risk arrangements, please access the
OCM Performance Periods 1 and 2 Payment Methodology and Performance Period 3 and Forward
Payment Methodology resources.
Performance Based Payment
There are three components to the PBP: a benchmark target price, the actual price, and a
performance multiplier (based on quality performance). There are 9 performance periods used
for the PBP, each generally lasting about 6 months each.
6|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/
Following the end of one of the 9 performance periods, the actual expenditures are calculated and
then compared to the target amount. The difference between the target amount and the actual
expenditures are then multiplied by the performance multiplier, calculated based on a quality
performance.
PBP = (Target Episode Price – Actual Episode Price) * Performance Multiplier * Geographic
Adjustment * Sequestration (if applied)
The performance multiplier allows for practices to receive 0%, 50%, 75%, or 100% of the difference
between the target and actual expenditures. More detailed information about these calculations
can be found here.
Quality Measurement
Practices participating in the OCM will be evaluated on a series of six quality measures, across two
National Quality Strategy (NQS) Domains. CMS also uses a multi-item survey to assess patients’
experience with chemotherapy care at each participating practice. Survey items used in the
calculation of the patient-reported experience measure for the performance-based payment will
be based on items recommended in the first Consumer Assessment of Healthcare Providers and
Systems (CAHPS) for Cancer Care field test report. Additional survey items will be drawn from
7|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/various validated instruments (e.g., CanCORS) to support evaluation of OCM, but these items will
not be used for scoring purposes.
`
Based on a practice’s performance relative to the national performance standard for a particular
measure, a practice can receive up to 10 points per measure for the OCMs listed above (these are
considered pay-for-performance measures), and up to 2.5 points for the other OCMs (these are
considered pay-for-reporting measures). The performance multiplier is then determined by the
percentage of how many points a practice has received compared to the maximum score. For
example, if a practice receives a total of 50 points out of 120 possible points, then it will receive a
performance multiplier of 50% because they received 42% of all possible points. The table below
provides a summary of this calculation.
8|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/1
It is important to note that in response to COVID-19, aggregate quality measure reporting will be
optional for PP7, PP8, and PP9. If a practice has elected to not report aggregate quality measure
results for OCM-4a, OCM-4b, AND OCM-5 for the affected measurement periods, the practice
must manually enter the value of “8888” in the denominator and numerator (and denominator
exclusions and exceptions, if applicable) for each measure in the OCM Data Registry to indicate
non-reporting by the submission deadline for the measurement period. Practices must report all
three measures if they elect to report for a measurement period, otherwise the practice-reported
measures will not be used for AQS.
If a practice participating in one or two-sided risk elects not to report aggregate measure results
for either of the measurement periods used to determine the AQS in PP7, PP8, and PP9, the
practice’s AQS and Performance Multiplier will be based on claims-based and patient survey
measures only.
OCM Participants and the Quality Payment Program
Under the QPP, only OCM practices participating in the two-sided risk arrangement are Advanced
APM participants., Practices participating in the one-sided risk arrangement are considered to be
in an MIPS APM.
Physicians and other eligible clinicians2 can receive one of three Advanced APM determinations
for their participation.
1
From CMS OCM Performance-Based Payment Methodology, available at: https://innovation.cms.gov/Files/x/ocm-
pp3beyond-pymmeth.zip
2
For 2021, eligible clinicians are defined as physicians, physician assistants, osteopathic practitioners,
chiropractors, nurse practitioners, clinical nurse specialists, and certified registered nurse anesthetists, physical &
occupational therapists, qualified speech-language pathologists, qualified audiologists, clinical psychologists,
registered dietitians or nutrition professionals, dentists and dental surgeons, and optometrists.
9|Page
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/Qualifying Advanced APM Partially Qualifying Neither a QP or Partially
Participant (QP) Advanced APM Participant Qualifying
•Eligible to receive a 5% •Not eligible to receive a •Subject to MIPS
incentive payment 5% incentive payment participation using the
•Exempt from MIPS •Exempt from MIPS APP
(however, the APM Entity
could elect to participate
in MIPS using the APM
Performance Pathway
(APP) and be eligible to
receive a positive
payment adjustment)
While the QP and partially qualifying determinations apply at the individual level, they are
determined at the APM Entity level. In this case the APM Entity is the OCM practice, and all
physicians and other eligible clinicians on the OCM’s Participant List must collectively meet the
thresholds for becoming a QP or PQ. Unlike QPs, partially qualifying participants would not be
eligible to receive a 5% incentive payment, but they would be exempt from MIPS participation.
However, the practice may elect to participate in MIPS using the APM Performance Pathway (APP).
Under the APP, all physicians and other eligible clinicians in the practice would be evaluated as a
group in three of the four MIPS categories: quality would be 50% of the MIPS score, promoting
interoperability would be 30%, and improvement activities would be 20%. The Improvement
activities performance category score will be automatically assigned based on the requirements
of the MIPS APM in which the MIPS eligible clinician participates; in 2022, all APM participants
reporting through the APP will earn a score of 100%. The Promoting Interoperability performance
category will be reported and scored at the individual or group level, as is required for the rest of
MIPS. The cost category is reweighted to 0% because physicians are already subject to a cost
assessment under the model. To learn more about the MIPS APM scoring methodology, please
see PAI’s MIPS APM Scoring Overview resource.
Continuing in 2022, physicians who are participating in APM arrangements with other payers (e.g.,
Medicare Advantage plans), “Other Payer Advanced APMs,” can have that participation count
towards the requirements for the QPP Advanced APM pathway. There are four ways for physicians
or other eligible clinicians to meet the QP and partially qualifying thresholds:
10 | P a g e
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/Medicare Payment Medicare Patient All Payer Payment All Payer Patient
Count Count Count Count
•based on the •based on the •based on the •based on the
percentage of percentage of percentage of percentage of
Medicare payments Medicare patients payments received patients seen
received through a seen through a through a Medicare through a Medicare
Medicare Advanced Medicare Advanced Advanced APM and Advanced APM and
APM APM Other Payer Other Payer
Advanced APM Advanced APM
Under the Medicare Option, only payments and patients from Medicare FFS patients are
considered. For the All-Payer Combination Option, there is a minimum threshold for Medicare
patients/payments that must be met before the All Payer options kick in. The All-Payer options,
therefore, do not replace or supersede the Medicare Option. Rather, they utilize a pair of
calculations using first the Medicare Part B patient/payment count method, and then the All-
Payer patient/payment count method for services furnished through Other Payer APMs.
Medicare Payment Amount Method Medicare Patient Count Method
QP At least 50% of Medicare Part B payments At least 35% of Medicare Part B
are received through a Medicare patients are seen through a Medicare
Advanced APM Advanced APM
Partial At least 40% of Medicare Part B payments At least 25% of Medicare Part B
QP are received through a Medicare patients are seen through a Medicare
Advanced APM Advanced APM
All Payer Payment Amount Method All Payer Patient Count Method
QP Step 1: Receive 25% of Medicare Part B Step 1: 20% of Medicare Part B patients are
payments are received through a Medicare seen through a Medicare Advanced APM
Advanced APM
Step 2: 50% of all payments are received Step 2: 35% of all patients are seen through
through a Medicare Advanced APM and Other a Medicare Advanced APM and Other Payer
Payer Advanced APM Advanced APM
Partial Step 1: Receive 20% of Medicare Part B Step 1: 10% of Medicare Part B patients are
QP payments are received through a Medicare seen through a Medicare Advanced APM
Advanced APM
Step 2: 25% of all patients are seen through
Step 2: 40% of all payments are received a Medicare Advanced APM and Other Payer
through a Medicare Advanced APM and Other Advanced APM
Payer Advanced APM
11 | P a g e
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/Where can I go for more information?
For additional information on the QPP requirements for Advanced APM participation please see
the QPP Advanced APM Overview resource, available on PAI’s website under the Advanced APM
Pathway page. Additional resources are available on the CMS OCM website.
12 | P a g e
© 2022 Physicians Advocacy Institute
www.physiciansadvocacyinsitute.org
Source: https://innovation.cms.gov/initiatives/oncology-care/You can also read