DIAGNOSI E TERAPIA DELL' EP - NUOVE PROSPETTIVE DI PAOLO PRANDONI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PAOLO PRANDONI
NUOVE PROSPETTIVE DI
DIAGNOSI E TERAPIA DELL’EP
ALBA, 29/11/2019
Disclosures of: Paolo Prandoni
Employment No conflict of interest to disclose
Research support No conflict of interest to disclose
Scientific advisory board No conflict of interest to disclose
Consultancy and lectures fees Bayer Pharma, Pfizer, Sanofi, Daiichi-Sankyo,
Rovi Pharmaceuticos
Speakers bureau No conflict of interest to disclose
Major stockholder No conflict of interest to disclose
Patents No conflict of interest to disclose
Honoraria No conflict of interest to disclose
Travel support No conflict of interest to disclose
Other No conflict of interest to disclose
Presentation includes discussion of the following off-label use of a
drug or medical device: N/A
ASPETTI DIAGNOSTICI
RIDURRE L’INDICAZIONE ALL’ANGIO-TC IN
PAZIENTI CON SOSPETTA EP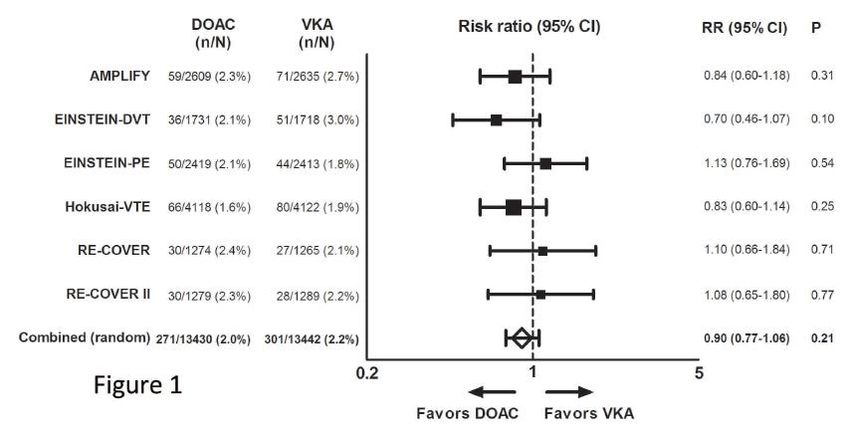
Algoritmo diagnostico convenzionale in
pazienti con sospetta EP
PTP (sec Wells
D-Dimero
o Geneva)
alta bassa negativo positivo
Esclusa EP
angioTC o scintigrafia
polmonare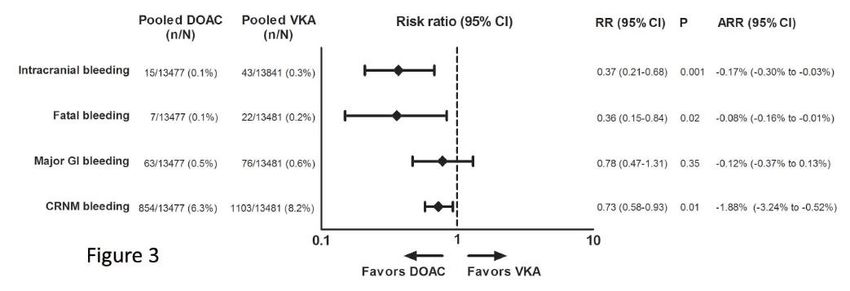
Riduzione dell’indicazione all’imaging
(ESC 2019)
ADJUSTED-DD: esclusione dell’EP in soggetti con
bassa PTP (secondo Wells) e DD inferiore ad un cut-
off che in soggetti > 50 a si ottiene moltiplicando
l’età per 10 [Righini M et al. JAMA 2014]
YEARS: esclusione dell’EP in soggetti con DD < 1000
se – la probabilità di EP è inferiore a quella di altre
condizioni, - è assente emottisi, - non ci sono
manifestazioni cliniche di TVP [van der Hulle T et al,
Lancet 2017; van der Pol et al, NEJM 2019]
ASPETTI TERAPEUTICI STRATIFICAZIONE DEL RISCHIO DI EVENTI AVVERSI TERAPIA DOMICILIARE IN PAZIENTI A BASSO RISCHIO RUOLO DEI DOAC IN PAZIENTI CON E SENZA NEOPLASIE
Classification of PE based on early mortality risk
Indicators of risk
Clinical
Elevated
Early mortality risk Haemo- parameters of PE RV
cardiac
dynamic severity/ dysfunction on
troponin
instability comorbidity: PESI TTE or CTPA
levels
III–V or sPESI ≥1
High + (+) + (+)
Interme- Intermediate–high - + + +
diate Intermediate–low - + One (or none) positive
Assessment
optional; if
Low - - -
assessed,
©ESC
negative
CTPA = computed tomography pulmonary angiography; PESI = Pulmonary Embolism Severity Index; TTE = transthoracic echocardiography.
2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism
www.escardio.org/guidelines
(European Heart Journal 2019 - doi/10.1093/eurheartj/ehz405)
SCORE DI BOVA PER LA STRATIFICAZIONE
DEL RISCHIO IN PAZIENTI NORMOTESI CON EP
Predictor Points
SBP 90-100 mm Hg 2
Elevated cardiac troponin 2
RVD (echocardiogram or 2
CT scan) and/or increased BNP
Heart rate > 110/min 1
Stage I: 0-2 points (30-day complic = 4.2%)
Stage II: 3-4 points (30-day complic = 10.8%)
Stage III: > 4 points (30-day complic = 29.2%)
Bova et al, Eur Respir J 2014
Home treatment in PE patients: the HOT PE Study
PrimaryEfficacy
Primary Outcomeaa
EfficacyOutcome
Recurrentsymptomatic
Recurrent symptomaticVTE
VTEor
orfatal
fatalPE
PE(ITT
(ITTpopulation)
population) 3/525(0.6%)
3/525 (0.6%)
One-sided99.6%
One-sided 99.6%upper
upperconfidence
confidencelimit
limit 2.1%
2.1%
Recurrent PE
Recurrent PE(two-sided
(two-sided 95%
95% CI)
CI) 3/525 (0.6%;
3/525 (0.6%; 0.1-1.7%)
0.1-1.7%)
Recurrent deep
Recurrent deepvein
vein thrombosis
thrombosis 00
Deathrelated
Death related to
toPE
PE 00
Recurrent symptomatic
Recurrent symptomatic VTE
VTE or
orfatal
fatal PE
PE (Per-protocol
(Per-protocol
2/497 (0.4%)
2/497 (0.4%)
population)
population)
1.3%
1.3%
One-sided 99.6%
One-sided 99.6% upper
upper confidence
confidencelimit
limit
Recurrent symptomatic
Recurrent symptomatic VTE
VTE or
orfatal
fatal PE
PE (worst
(worstcase
casescenario)
scenario) 5/525 (0.95%)
5/525 (0.95%)
One-sided 99.6%
One-sided 99.6% upper
upper confidence
confidencelimit
limit 1.99%
1.99%
a Adjudicated by an independent clinical events committee.
Barco S et al, Eur Heart J 2019Recidive tromboemboliche sintomatiche
Emorragie maggiori (1)
Emorragie maggiori (2)
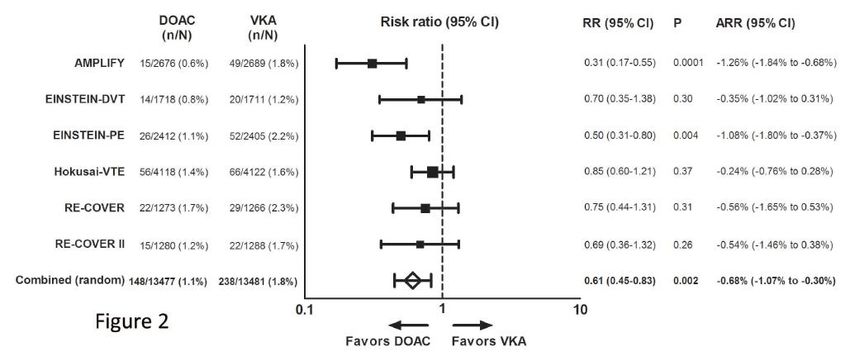
Table 2 Main new recommendations 2019 (3)
Treatment in the acute phase
When oral anticoagulation is initiated in a patient with
PE who is eligible for a NOAC (apixaban, dabigatran, I
edoxaban, or rivaroxaban), a NOAC is the recommended
form of anticoagulant treatment.
Set-up of multidisciplinary teams for management of high-risk and selected cases of
intermediate-risk PE should be considered, depending on the resources and expertise available IIa
in each hospital.
©ESC
ECMO may be considered, in combination with surgical embolectomy or catheter-directed
IIb
treatment, in refractory circulatory collapse or cardiac arrest.
2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism
www.escardio.org/guidelines
(European Heart Journal 2019 - doi/10.1093/eurheartj/ehz405)N Engl J Med 2018; 378: 615-624
Caratteristiche dei pazienti
Edoxaban Dalteparin
Characteristic (N = 522) (N = 524)
Age 64 ± 11 64 ± 12
Male sex 277 (53%) 263 (50%)
PE ± DVT 328 (63%) 329 (63%)
Symptomatic VTE 355 (68%) 351 (67%)
Active cancer 513 (98%) 511 (98%)
Metastatic disease 274 (53%) 280 (53%)Incidenza cumulativa degli eventi tromboembolici e/o emorragici
Incidenza cumulative degli eventi
tromboemboliciIncidenza cumulative degli eventi
emorragiciTable 2 Main new recommendations 2019 (5)
Pulmonary embolism in patients with cancer
Edoxaban or rivaroxaban should be considered as an alternative to
IIa
LMWH, with the exception of patients with gastrointestinal cancer.
Pulmonary embolism in pregnancy
Amniotic fluid embolism should be considered in a pregnant or
postpartum woman with unexplained haemodynamic instability or IIa
respiratory deterioration and disseminated intravascular coagulation.
Thrombolysis or surgical embolectomy should be considered for
IIa
pregnant women with high-risk PE.
NOACs are not recommended during pregnancy or lactation.
©ESC
III
2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism
www.escardio.org/guidelines
(European Heart Journal 2019 - doi/10.1093/eurheartj/ehz405)Lancet Haematology 2019
ASPETTI PROGNOSTICI RUOLO DELLA RIPETIZIONE DELL’ANGIO-TC A SCOPI PROGNOSTICI DURATA OTTIMALE DELLA TERAPIA ANTICOAGULANTE
E’ utile l’imaging di controllo a scopi prognostici? Dopo 6 mesi di terapia anticoagulante l’angio-TC appare completamente normalizzata nell’85% dei pazienti, e negli altri dimostra alterazioni di scarso significato e non correlate con lo sviluppo di eventi successivi [Pesavento R et al, AJRCCM 2014; den Exter PL et al, Thromb Haemost 2015] Più utile (e meno invasiva) a scopi prognostici la scintigrafia polmonare [Pesavento R et al, Eur Respir J 2017]
Haematologica 2007; 92: 199-205
The clinical course of 1626 patients with DVT and/or PE
Patients (number) 1626
Age (median, range) 66 (16,96)
Gender (n., % males) 735 (45.2)
Modality of clinical presentation
- DVT alone 1073 (66.0)
- DVT + PE 292 (18.0)
- PE alone 261 (16.0)
Patients categories
- Unprovoked 864 (53.1)
- Secondary to acquired risk factors 762 (46.9)
Risk factors for thrombosis
- Recent trauma or surgery 553 (72.6)
- Hormonal treatment, pregnancy or puerperium 109 (14.3)
- Medical diseases 100 (13.1)
Thrombophilic abnormalities 229/953 (24.0)
Duration of oral anticoagulation
- Three months or less 540 (33.2)
- Between three and six months 811 (49.9)
- Between six and twelve months 196 (12.0)
- Between one and two years 67 (4.1)
- Between two and three years 12 (0.7)The clinical course of 1626 patients with DVT and/or PE
Adjusted HR = 2.30
(95% CI, 1.82 - 2.90)
Prandoni, Hematologica 2007Risk of recurrence as PE
(7 prospective studies, 2554 patients)
Baglin T, J Thromb Haemost 20102011, online first
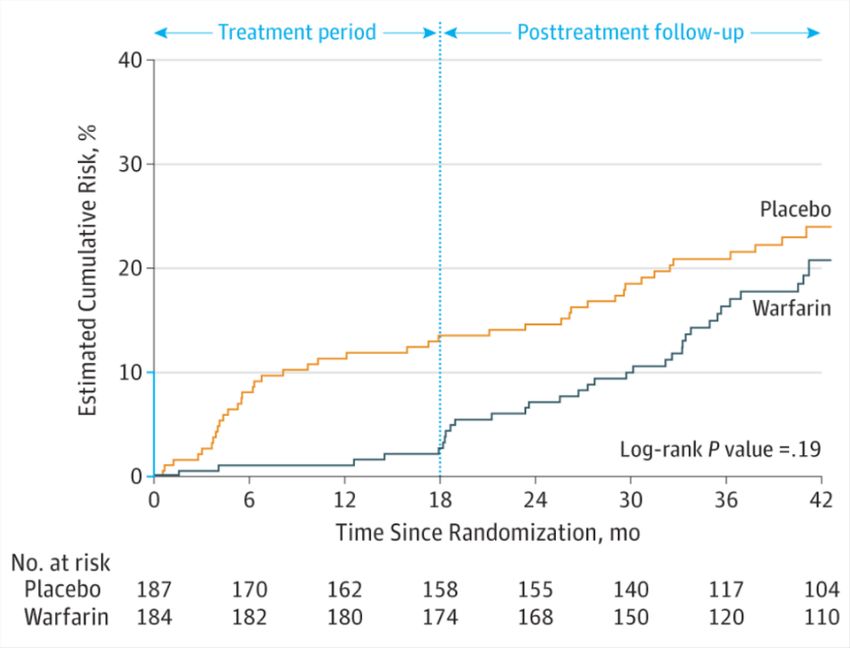
From: Six Months vs Extended Oral Anticoagulation After a First Episode of Pulmonary Embolism: The PADIS-
PE Randomized Clinical Trial
JAMA. 2015;314(1):31-40. doi:10.1001/jama.2015.7046
Figure Legend:
Probability of the Composite Outcome of Recurrent Venous Thromboembolism and Major Bleeding Throughout the Study PeriodThe
unadjusted hazard ratios for warfarin-placebo were 0.23 (95% CI, 0.09-0.55) during the treatment period and 0.74 (95% CI, 0.47-
1.17) for the entire study period. The y axis that is shown in blue indicates the range of estimated cumulative risk from 0% to 10%.
Copyright © 2015 American Medical
Date of download: 10/21/2015
Association. All rights reserved.Extension of anticoagulant treatment
beyond 3 to 6 months for VTE with the VKA
For 1,000 patient-years
Death by
PE recurrence
80 VTE recurrences Death by
Case-fatality rate 2.6-4% major bleed
3 – 10 deaths 20 – 60 bleeds
Case-fatality rate 11%
2 – 6 deaths
Van der Wall SJ, et al. Eur Respir Rew 2019
Douketis JD, et al. Ann Intern Med 2007
Linkins LA, et al. Ann Intern Med 2003In pazienti con TEV idiopatico o associato a fattori di rischio deboli (permanenti o transitori) Durata fissa della terapia anticoagulante Terapia indefinita con i VKA
Overview of extended treatment studies with
NOACs/ ASA
Study Study treatment Experimental Experimental
Placebo/Aspirin
duration high low
(planned)
RVTE MB RVTE MB RVTE MB
RESONATE1 6 months 0.4% 0.3% 5.6% 0%
AMPLIFY EXT2 12 months 1.7% 0.1% 1.7% 0.2% 8.8% 0.5%
EINSTEIN
6 or 12 months 1.3% 0.7% 7.1% 0%
Extension3
EINSTEIN Choice Up to 12 months 1.5% 0.5% 1.2% 0.4% 4.4%** 0.3%**
WARFASA/
Up to 48 months 5.1% 0.5% 7.1% 0.4%
ASPIRE pool4*
Caveat: Incidences as reported and not annualized (Except ASA Studies), mean Tx
duration may differ from planned
**Comparison with ASA
RVTE: recurrent VTE, MB: Major Bleeding according to ISTH,
Experimental high/ low refer to dose of NOAC used for AMPLIFY Ext and Einstein Choice
1. Schulman et al. N Engl J Med 2013; 2. Agnelli et al. N Engl J Med 2013; 3. The
EINSTEIN Investigators. N Engl J Med 2010; 4. Simes et al. Circulation 2014Prins MH et al, Blood Adv 2018;2:788–796
EINSTEIN CHOICE and EINSTEIN EXT Pooled Analysis:
Provoked VTE Risk Factor Classification
Classification of risk factors according to index venous thromboembolic event
Persistent Transient
Major
Active cancer excluding basal cell or squamous Major surgery/trauma
cell skin cancer; APS Cesarean section
Inflammatory bowel disease Immobilization
Lower extremity paralysis or paresis Travel >8 hours
Congestive heart failure Pregnancy
Body mass index >30 kg/m2 Puerperium
Minor
Calculated CrClRecurrent VTE – Crude Incidences by Risk Factor Prins MH et al, Blood Adv 2018;2:788–796
Table 2 Main new recommendations 2019 (4)
Chronic treatment and prevention of recurrence in patients without cancer
Indefinite treatment with a VKA is recommended in patients with the antiphospholipid
I
antibody syndrome.
Extended anticoagulation should be considered for patients with no identifiable risk factor for
IIa
the index PE event.
Extended anticoagulation should be considered in patients with a persistent risk factor other
IIa
than the antiphospholipid antibody syndrome.
Extended anticoagulation should be considered for patients with a minor transient/reversible
IIa
risk factor for the index PE event.
©ESC
Reduced dose of apixaban or rivaroxaban should be considered after the first 6 months. IIa
2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism
www.escardio.org/guidelines
(European Heart Journal 2019 - doi/10.1093/eurheartj/ehz405)Models to predict recurrent VTE
Men continue and Vienna Prediction DASH-score DAMOVES score
HER D002 Model
Study design Prospective cohort Prospective cohort Patient level meta- Prospective cohort
analysis
Patients 646 929 1818 398
Predictive Men: none - Sex - Abnormal D-dimer - Age
variables Women: - Location of first VTE after anticoagulation - Sex
- age > 60 years - D-Dimer after - Age < 50 years - Obesity
- signs of PTS anticoagulation - Male sex - D-dimer during
- BMI > 30 kg/m2 - Hormonal therapy anticoagulation
- D-dimer > 250 μg/l - F VIII
during anticoagulation - Thrombophilia
- Varicose veins
Increased risk of >1 point > 180 points (according > 1 point > 11.5 (according to
recurrent VTE to a nomogram) a nomogram)
Recurrence rate 1.6% (95% CI, 0.3- 4.4% (95% CI, 2.7-6.2) 3.1% (95% CI, 2.3- 2.9% (95% CI, 2.13-
in patients at 4.6) 3.9) 4.35)
low riskCommento Negli ultimi anni sono stati raggiunti significativi successi in tutti i campi dell’embolia polmonare Ora si tratta di promuoverne l’applicazione nella pratica clinica
Vi aspetto sulla mia pagina di aggiornamento
bibliografico e culturale sulle malattie trombotiche:
Paolo Prandoni facebookYou can also read