NPA MEDICATION SAFETY UPDATE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

j
NPA MEDICATION SAFETY UPDATE
Analysis of incidents reported during Q1 2020.
Medication and patient safety information and guidance, including
during COVID-19.
© NATIONAL PHARMACY ASSOCIATION
MALLINSON HOUSE, 38-42 ST PETER’S STREET, ST ALBANS AL1 3NP
Tel: 01727891800
Email: pharmacyservices@npa.co.uk
Website: https://www.npa.co.uk/services-and-support/patientsafety
1
NPA MEDICATION SAFETY UPDATE
Contents Page
Medication Safety Officer (MSO) 1
Analysis of patient safety incidents reported during Q1 2020 2
Look alike sound alike (LASA) analysis 5
Drug monitoring during the COVID-19 pandemic 6
Medicines safety – COVID-19 6
Delivery of medicines 7
Ranitidine supply 8
Valproate- Pregnancy Prevention Programme 8
Medicines compliance aid discontinuation leading to compliance issues 9
Yellow Card reporting 9
Reporting patient safety incidents 9
Relevant links 10
Contact your MSO 11
Medication Safety Officer (MSO)
In 2014, NHS England and the Medicines and Healthcare products Regulatory Agency (MHRA) issued a national
Directive NHS/PSA/D/2014/005 (patient safety alert) to improve medication and error incidents reporting and
learning. This Directive established the role of the Medication Safety Officer (MSO).
Role of the MSO
Promoting safe use of medicines
Supporting pharmacy teams in improving patient safety
Implementing local and national medication safety initiatives
Improving reporting, and learning from patient safety incidents
Sharing learnings from incidents submitted to the NPA with the community
pharmacy sector, the Community Pharmacy Patient Safety Group (PSG) and
other relevant organisations
Each of the largest multiples, and the National Pharmacy Association (NPA) on behalf of
independent pharmacies, has appointed a named person who is committed to making a difference, sharing
learning and experiences. The NPA holds the role of Medication Safety officer (MSO) for all independent
community pharmacies in England with fewer than 50 branches. Jasmine Shah, NPA Head of Advice and
Support Services, currently holds the role of MSO at the NPA. As part of this role, we are working together with
the wider pharmacy sector on the patient safety agenda, and in particular, playing our full part in the work of
the sector-wide Community Pharmacy Patient Safety Group (PSG).
NPA patient safety update Q1 2020
This update contain a summary of the most common types of dispensing errors reported to the NPA during the
quarter, and guidance for minimising patient safety incidents and information on current hot topics in patient
safety, including guidance on maintaining patient safety during the COVID-19 pandemic
During the coronavirus (COVID-19) pandemic, since March 2020, there has been a marked decrease in the
number of patient safety incidents being reported. It is important to continue to report these incidents.
© NATIONAL PHARMACY ASSOCIATION, 20202
Analysis of patient safety incidents reported during Q1 2020
Overall, there was a 3.34% increase in the number of incidents reported during Q1 2020, compared to Q4 2019.
Compared to the same quarter in 2019, there was a 13.9% decrease in the number of incidents reported during
Q1 of 2020. We have shared some of the key findings and statistics from our analyses below from incidents
reported during Q1 2020.
1) Number of patient safety incidents during Q1 of 2020
There has been a 13.9% decrease in incidents reported in Q1 2020 compared to Q1 2019; this significant
reduction may be due to the increased workload and pressure on pharmacy teams due to COVID-19, whereby
pharmacy teams may not be prioritizing reporting of patient safety incidents, or due to other, as yet unknown,
reasons.
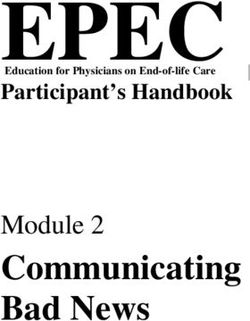
2) Origin of patient safety incidents during Q1 of 2020
92% of incidents reported originated from the pharmacy
4% of errors reported were prescribing errors – this is a 2% increase from Q4 2019 — it is important to
report prescribing errors because increased reporting allows identification of trends and increases
learning
Other (3%)
Pharmacy error (92%)
Prescriber error (4%)
Both prescriber and pharmacy error (1%)
3) Type of incident reported during Q1 of 2020
The most common type of incident reported during Q1 was ‘dispensing error’, which accounted for 81% of all
reported incidents. Whilst reporting of dispensing errors is encouraged, all types of incidents and near misses in
the pharmacy can be reported.
These may include, but are not limited to:
• Counselling errors
• Treatment procedure/administration error
• Patient abuse
• Delivery/collection errors
• Supply of over-the-counter (OTC) medication error
Delivery/collection errors accounted for 7% of the incidents reported; an increase in 1% since Q4 2019. Further
guidance and learnings from these incidents is provided later in the report.
© NATIONAL PHARMACY ASSOCIATION, 20203
Delivery/collection error Dispensing error (81%) Prescribing/prescriber Other (8%)
(7%) error (4%)
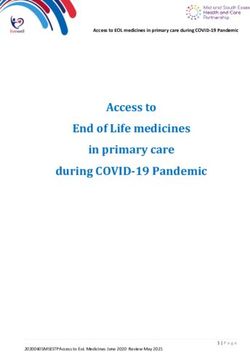
4) Medication error categories and incidents reported during Q1 of 2020
The main categories of errors reported were those involving medication errors such as wrong drug, strength or
formulation, these accounted for 60% of errors reported – this is a 6% decrease from Q4 2019:
‘Wrong strength’ incidents (22%)
‘Wrong drug/medicine’ incidents (26%)
‘Wrong formulation’ incidents (12%)
Wrong drug/medicine (26%)
Wrong strength (22%)
Wrong formulation (12%)
Mismatching patients (12%)
Wrong quantity (9%)
Other (8%)
Mismatching between patient and medicine (3%)
Wrong/unclear dose (2%)
Omitted medicine/ingredient (1%)
Wrong/transposed/omitted label (1%)
Wrong brand/generic (1%)
Wrong frequency (1%)
Patient allergic to treatment (1%)
Wrong method of preparation/reconstitution (1%)
Unknown (0%)
Wrong/omitted verbal patient directions (0%)
Wrong storage (0%)
Focus on mismatching
Mismatching patients or mismatching between patient and medicine accounted for a total of 15% of errors
reported this is a 6% increase from Q4 2019. Please see below key points to assist pharmacy teams in reducing
these types of error. Always confirm the patient’s identity to ensure that the requested details correspond to
those on the prescription; this could be the name, address and/or date of birth
Check the bag label against the prescription
Before bagging up the medication ensure all items correspond to the patient’s name and expected number
of items on the prescription
Take care when handing out prescriptions for patients with similar or same names/surnames
Confirm that the contents of the bag matches the patients expectation
Do not leave prescription bags open once they are ready for collection
Avoid printing additional bag labels
© NATIONAL PHARMACY ASSOCIATION, 20204
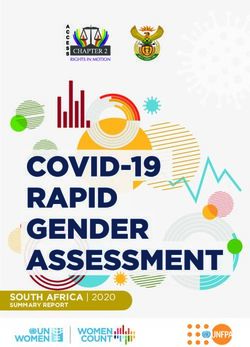
4. Degree of harm caused to patients by incidents reported during Q1 of 2020
The degree of harm caused to patients reported as ‘none’ (60%) and ‘near miss’ (27%) continues to make up
the majority of reports.
The data reported over Q1 2020 highlighted both good and poor reporting. There were no reports
submitted where the degree of harm was reported as ‘severe’ or ‘death’.
None (60%)
Near miss (27%)
Low (12%)
Moderate (1%)
Severe (0%)
Death (0%)
Actions for pharmacy teams when recording degree of harm
Please ensure you report the actual degree of harm caused to the patient and not the potential harm that
could have happened.
Please ensure you complete a detailed outcome if an incident did lead to moderate or severe harm to the
patient – this is to allow a thorough analysis to be undertaken by us.
Please ensure the incident form is fully completed, is accurate and includes sufficient details to allow
meaningful analysis of the incident.
5. Self-checking during Q1 of 2020
‘Self-checking’ is defined as a pharmacist carrying out all steps in the dispensing process themselves. It includes
the clinical check of the prescription as well as the accuracy check of the assembled items. There was a 4%
decrease in the incidents involving self checking compared to Q1 2019.
Not applicable (5%) Yes (11%) No (84%)
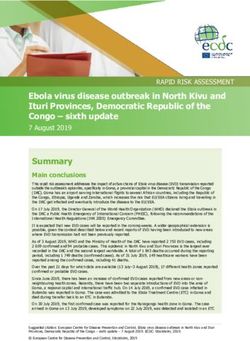
6. Contributing factors to patient safety incidents during Q1 of 2020
‘Work and environment factors’ (35%) continues to be the main contributing factor reported. This category
includes time pressures, understaffing and poorly organised working environments.
‘LASA’ (22%) as a contributing factor was the second largest contributing factor to the errors reported. See
more analyses on LASA errors below.
© NATIONAL PHARMACY ASSOCIATION, 20205
Work & environment factors (35%)
LASA (22%)
Other (describe) (17%)
Task factors (5%)
Communication factors (5%)
Medication factors (5%)
Prescriber error (3%)
Education & training factors (2%)
Organisation & strategic factors (2%)
Team & social factors (2%)
Equipment & resources factors (1%)
Patient factors (1%)
Unknown (0%)
Look-alike sound-alike (LASA) errors
The percentage of each of the top LASA errors (as identified by NHS Improvement) reported in Q1 2020 are
listed below.
Top LASA errors as identified by NHS Improvement Percentage from total number of LASA errors
Amlodipine Amitriptyline 8%
Atenolol Allopurinol 5%
Carbamazepine Carbimazole 0%
Propranolol Prednisolone 2%
Rosuvastatin Rivaroxaban 2%
In addition to the LASA errors highlighted as high risk by NHS improvement, 4% of all reported LASA errors
involved gabapentin and pregabalin. The reclassification of these medicines as Schedule 3 Controlled Drugs
(CDs) in April 2019 has raised more awareness of their reporting. However, even in Q1 2020, the trend continues
and a significant amount of incidents reported involve these medicines. Schedule 3 CDs do not need to be kept
in a CD cabinet, therefore, it is essential they are separated out in the dispensary with clear reminders for staff
to double check the item they pick.
Reminder on LASA definition - The Centre for Pharmacy Postgraduate Education (CPPE) training providers
indicate that a LASA can be due to similar packaging, names or strengths; in fact if a person feels two medicines
look or sound similar at all this can be classified as a LASA error.
Actions to take when reporting LASA errors
To enable LASAs to be identified as a root cause of the problem, when reporting such errors, please report
them under one of the following depending on how much the LASA contributed to the error:
‘What was the main contributing factor’, or
‘Were there other important
Additionally, the word ‘LASA’ should be included in the ‘Describe What Happened’ section of the incident
report
© NATIONAL PHARMACY ASSOCIATION, 20206
Actions pharmacy teams can take to reduce/prevent LASA errors
Discuss the potential for these types of errors with the whole pharmacy team; e.g. at the weekly team
huddle, including locums
Separate the different strengths of medicines with similar packaging
Separate medicines with similar spellings
Highlight the medicines using appropriate means such as different coloured stickers or note on dispensing
shelf/drawer
Add a note to the PMR to flag up an alert for these medicines
Pay particular attention when dispensing in monitored dosage systems (MDS)
Barcode scanning / FMD scanning can help reduce LASA errors significantly as a means of accuracy checking
Avoid self-checking
Hot topics in patient safety identified during Q1 2020
In this patient safety update, we would like to highlight some key topics and resources available to pharmacy
teams to ensure patient safety is maintained during the COVID-19 pandemic.
Drug monitoring for a range of medicines during the COVID-19 pandemic
The Specialist Pharmacy Service (SPS) has produced a range of resources that provide guidance on the
management of drugs requiring monitoring and factors to consider when making monitoring decisions during
the COVID-19 pandemic. Due to a lot of GP practices operating a closed door policy, patients may be presenting
in community pharmacies with queries on how monitoring of their medicines will continue during the pandemic.
It is important to reassure patients there are procedures in place to ensure they can take their medicines safely.
Clinicians should be made aware of the advice available on the following medicines that require monitoring:
Azathioprine, leflunomide, mercatopurine, and Penicillamine
methotrexate Warfarin
Sulfasalazine Lithium
Hydroxychloroquine Clozapine
Ciclosporin
Medicines safety – current advice for COVID-19
Advice on ibuprofen/NSAIDs and COVID-19
The Commission on Human Medicines (CHM) has determined that there is currently insufficient evidence to
establish a link between use of ibuprofen, or other non-steroidal anti-inflammatory drugs (NSAIDs), and
susceptibility to contracting COVID-19 or the worsening of its symptoms. Therefore, patients can be advised to
take paracetamol or ibuprofen when self-medicating for symptoms of COVID-19, such as fever and headache,
and should follow NHS advice if they have any questions or if symptoms get worse.
Advice on high blood pressure medication and COVID-19
The MHRA has confirmed there is no evidence from clinical or epidemiological studies to suggest angiotensin-
converting enzyme inhibitors (ACE inhibitors) or angiotensin-receptor blockers (ARBs) worsen COVID-19.
Therefore, patients must be advised to continue taking their medicines as usual.
Chloroquine and Hydroxychloroquine not licensed for COVID-19 treatment
The MHRA has issued guidance that chloroquine and hydroxychloroquine are not licensed to
treat coronavirus (COVID-19)-related symptoms or prevent infection. Further NPA advice on the sale/supply of
these medicines is available on the NPA website.
© NATIONAL PHARMACY ASSOCIATION, 20207
Delivery of medicines
There have been several incidents throughout Q1 2020 resulting through delivery of medicines to patients.
Below are some examples learnings that can be taken away to help pharmacy teams reduce these types of
incidents. This is of particular importance due to the increase in demand under the current unprecedented
climate.
Example 1: Patient A was delivered Patient B’s medicine bag – it involved an MDS tray – items were retrieved
and corrected before the patient took any medicine
Learnings: Ensure whole pharmacy team, including those delivering, are aware of the importance to always
check patient’s name and address when handing over medicines against the label on the bag, delivering book,
and prescription, as required. This applies for both collection and delivery. Sometimes MDS patients are more
vulnerable so extra care must be taken. There has been a potential GDPR breach of confidentiality and
appropriate remedial action should be taken.
Example 2: The delivery driver went to deliver medication to a patient’s home; however, the patient did not
answer the door and the delivery driver posted the medication through the letterbox instead. When the patient
returned home, she had discovered that her pet dog had eaten all her medication.
Learnings: Ensure pharmacy has robust processes in place before starting a delivery service. Standard Operating
Procedures (SOPs) should be in place for the delivery of medicines, which includes the process for posting
medicines through a letterbox. Consent must be sought from the patient confirming they have authorised for
their medicines to be posted through their letterbox and there are no pets, young children or vulnerable
patients present at the property and understand potential risks associated with this type of delivery. Consent
should also be updated periodically. It is important you check with your indemnity insurance provider to ensure
your service would be covered. The responsible pharmacist would be accountable until the medicines physically
reach the patient.
Example 3: The delivery driver collected the medicines (a large item) from the pharmacy and did not realise it
had not been checked by the pharmacist. He took the package and delivered to the patient. Pharmacy realised
the error and contacted the patient’s representative. The item was collected back and checked by the
pharmacist.
Learnings: Ensure there is a process where medication ready for delivery has a specified area and is handed
over to the delivery driver. Brief whole pharmacy team on procedures and process to only hand over to delivery
driver when medication is checked by the pharmacist on duty.
NPA support
Dedicated GDPR page with a suite of resources, which can be downloaded
Template essential SOPs including handing out and clinical and legal check
During the COVID-19 pandemic: We have created a dedicated page for Training you and your workforce -
examples of resources on this page include:
o Pharmacy staff training guide
This is a pandemic training guide for pharmacy staff. It can be used by existing trained or trainee
healthcare staff to understand the changes that may take place in their pharmacy and operational
practices and how these will affect them.
o SOP – Delivering pharmacy items This SOP aims to give staff and volunteers a clear process for delivery
during the COVID-19 pandemic. The SOP covers social distancing precautions, hygiene measures and
other good practice
© NATIONAL PHARMACY ASSOCIATION, 20208
Ranitidine
The Department of Health and Social Care (DHSC) issued a Medicine Supply Notification MSN/2020/025 in May
2020 updating healthcare professionals on all formulations of ranitidine following the ongoing regulatory
investigations on the presence of N-nitrosodimethylamine (NDMA) contaminant:
All pharmacies should have received this in the NHSmail inbox
Ranitidine injection 50mg/2ml is anticipated to be out of stock from the end of May 2020 until further notice
All strengths of ranitidine film-coated tablets, effervescent tablets and oral solution are out of stock with no
availability date
Clinical advice on alternatives for adults and children was shared in the Supply Disruption Alert
SDA/2019/005 (U2) issued in December 2019;
Further information is available on the NPA website.
Valproate- Pregnancy Prevention Programme
Valproate is known to be highly teratogenic at all strengths. Exposure during pregnancy carries a 10% risk of
children being born with congenital malformations and 30-40% risk of neurodevelopmental delays. The MHRA
has issued temporary guidance for management of the Valproate Pregnancy Prevention Programme (PPP)
during the coronavirus (COVID-19) pandemic to assist specialists in initiating valproate in female patients,
undertaking annual reviews, and pregnancy testing procedures during the COVID-19 pandemic. Although the
temporary guidance is intended for specialists, pharmacy teams should read the new guidance and be aware of
the temporary processes in place due to the pandemic, as well as understand and implement the full MHRA
guidance. Pharmacy teams should already be aware and implementing the guidance for pharmacists on
dispensing prescriptions for valproate.
Actions when dispensing valproate:
1. Supply in whole, original packs where possible, with the relevant accompanying patient information leaflet,
even if a split pack is given
2. Include a warning sticker if dispensed in a ‘white dispensing box’ or carton
3. Provide a Patient Card every time valproate is dispensed. Confirm the patient has received a Patient Guide
(this does not need to be supplied every time valproate is dispensed) – valproate information materials can
be downloaded from the May 2018 Drug Safety Update or by contacting Sanofi Medical Information on
0845 372 7101 or email UK-Medicalinformation@sanofi.com
4. Remind patients of the risks in pregnancy and the need for highly effective contraception.
5. If the patient of childbearing potential is not taking a highly effective contraception, and has not been seen
by her GP/Specialist in the past year, dispense their medicine and refer them to their GP (including by
contacting the GP if necessary).
6. Remind patients of their annual review with the specialist
7. Report any suspected adverse reactions associated with valproate and any adverse pregnancy outcomes via
the Yellow Card Scheme
NPA support
The following valproate resources are available from the NPA to support patient safety:
Valproate standard operating procedure (SOP)
Medicines in pregnancy and patient safety– this includes a link to the “Valproate dispensing checklist”
© NATIONAL PHARMACY ASSOCIATION, 20209
Medicines compliance aid discontinuation leading to compliance issues
Further to our previous update on dispensing medicines in monitored dosage systems (MDS), we would like to
remind pharmacy teams on the importance of continually reviewing procedures in the pharmacy during the
pandemic. Pharmacy teams are well-placed to promote patients compliance of prescribed medicines and discuss
non-compliance issues even if this is conducted remotely. Patients should be encouraged to discuss any
concerns they may have regarding their health or medicines with their healthcare professionals including
pharmacists. For patients who are eligible under the Equality Act 2010 to receive reasonable adjustments, other
than MDS, there may be other reasonable adjustments that can be discussed to ensure they take their
medicines safely. Alternatives may prove to be less time-consuming for pharmacy teams but may still improve
compliance, for example, supplying original packs with MAR charts or using larger font labels to assist patients
with partial -sight. The NPA will continue to support pharmacists when exercising their professional judgement
when deciding if they can supply via MDS or dispensing medicines in their original packs.
Yellow Card Reporting
Yellow Card reporting during the COVID-19 response
The MHRA has reported a decrease in Yellow Card reporting especially from healthcare professionals during the
COVID-19 pandemic. We encourage pharmacists to use the Yellow Card Scheme as it is an essential tool that the
MHRA uses to monitor the safety of medicines, medical devices and herbal or complimentary medicines. It is
crucial to report problems with these products in order to improve patient safety by identifying issues such as
side effects, as well as defective and counterfeit medicines or medical devices.
Reports should be submitted electronically instead of on paper. Further information is available on the NPA
website.
COVID-19 Yellow Card reporting site
The MHRA has issued a Central Alerting System (CAS) alert to highlight the launch of a dedicated Yellow Card
reporting site for healthcare products that are used in Coronavirus (COVID-19) treatment to be easily reported:
https://coronavirus-yellowcard.mhra.gov.uk/.
Healthcare professionals, patients and carers are asked to report all suspected side effects to medicines or
medical device adverse incidents related to COVID-19 treatment. This also includes medicines that patients and
healthcare professionals are using off-label to treat COVID-19. Reporting for clinical trials should be in line with
the trial protocol.
Reporting patient safety incidents
Community pharmacies are required to report all patient safety incidents, as well as analyse and learn from the
incidents and share learnings. We appreciate you are all extremely busy with a massively increased workload
currently. However, patient safety incidents may occur in the course of your practice. It is important to continue
to manage and report all patient safety incidents in line with you pharmacy process. This includes completing
the recording of the incident details carefully and fully.
NPA Incident reporting platform (IRP)
To support independent community pharmacies, the NPA Incident Reporting Platform (IRP) is available for use
by all community pharmacies in England with fewer than 50 branches for reporting patient safety incidents; this
applies to NPA members as well as non-members. The NPA IRP can be accessed via this link:
https://irp.npa.co.uk/
© NATIONAL PHARMACY ASSOCIATION, 202010
Ensure that the form is filled in accurately and includes sufficient details to allow meaningful analysis of the
incident.
DO NOT include personal identifiable information in your incident report including staff, patient, carer or
relative names or addresses and patient hospital numbers.
In order to use the NPA IRP, you will need to use one of the following supported browsers with JavaScript
enabled:
Microsoft Internet Explorer 11 Google Chrome
Microsoft Edge Mozilla Firefox
NPA patient safety Incident Reporting Platform (IRP) — user information
1. Details or information that can identify patients or healthcare professionals must not be included when
completing the report — this is especially important since the implementation of the General Data
Protection Regulation (GDPR) on 25 May 2018. Use anonymous descriptions such as ‘Patient A’ or Patient B’
instead of patient’s name(s), and ‘Pharmacist’ or ‘Pharmacy Technician’ instead of their name(s).
2. Where the pharmacy is reporting an error that involves a Look-alike-sound-alike (LASA) error, include the
word ‘LASA’ in the ‘Describe What Happened’ section of the incident report.
3. The incident report receipt is sent via email, helping to reduce administrative time as it can be kept for
pharmacy record keeping requirements. Currently there are multiple receipts not reaching the pharmacies
who have submitted the report because incorrect email addresses have been submitted; before submitting
the report, check the email address for correspondence submitted is accurate.
4. When documenting the degree of harm caused to patients, the actual degree of harm should be
documented, not the potential harm that could have arisen.
5. The NPA IRP can be used to document near misses. Although it is not a requirement to report near misses,
it is a requirement to record them. Reporting near misses is encouraged as learning can occur which can
help prevent future events occurring.
6. It is important that a detailed description of the patient safety incident in the ‘describe what happened’ field
is provided (think about the sequence of events and how the error was concluded). Simply writing a brief
description, for example, ‘wrong strength given’ is not enough as it does not provide sufficient information
for us to conduct a full and complete data analysis which is a key part of the NPA’s role as the MSO.
Reporting patient safety incidents via NRLS
Community pharmacies can also report incidents via the National Reporting and Learning System (NRLS) e-form:
https://www.eforms.nrls.nhs.uk/staffreport/ — select ‘Community pharmacy’ from the drop-down list under
the ‘Start reporting here’ section, and click on ‘Start’
Ensure that the form is filled in accurately and includes sufficient details to allow meaningful analysis of the
incident.
DO NOT include personal identifiable information in your incident report including staff, patient, carer or
relative names or addresses and patient hospital numbers.
Relevant links mentioned in this update & signposting
NPA patient safety resources: https://www.npa.co.uk/services-and-support/patientsafety
NPA incident reporting platform (England): https://irp.npa.co.uk/
Community Pharmacy Patient Safety Group (PSG): https://pharmacysafety.org/
NPA Dispensing process – best practice guidance which includes guidance for self-checking prescriptions.
Community pharmacy patient safety group (PSG) COVID-19: https://pharmacysafety.org/corona-virus-covid-
19/
© NATIONAL PHARMACY ASSOCIATION, 202011
NRLS e-form: https://www.eforms.nrls.nhs.uk/staffreport/
MHRA Yellow Card: https://yellowcard.mhra.gov.uk/
https://coronavirus-yellowcard.mhra.gov.uk/
MHRA guidance during COVID-19: https://www.gov.uk/government/collections/mhra-guidance-on-
coronavirus-covid-19#medicines-and-covid-19
MHRA : https://www.gov.uk/government/news/commission-on-human-medicines-advice-on-ibuprofen-
and-coronavirus-covid-19
https://www.gov.uk/government/news/coronavirus-covid-19-and-high-blood-pressure-medication
https://www.gov.uk/government/news/chloroquine-and-hydroxychloroquine-not-licensed-for-coronavirus-
covid-19-treatment
MHRA Valproate PPP: https://www.gov.uk/drug-safety-update/valproate-medicines-epilim-depakote-
contraindicated-in-women-and-girls-of-childbearing-potential-unless-conditions-of-pregnancy-prevention-
programme-are-met
SPS: https://www.sps.nhs.uk/articles/drug-monitoring-in-primary-care-for-stable-patients-during-covid-19/
https://www.sps.nhs.uk/articles/drug-monitoring-factors-to-consider-during-covid-19/
PHE COVID-19 guidance: https://www.gov.uk/government/collections/coronavirus-covid-19-list-of-guidance
HSE COVID-19 guidance: https://www.hse.gov.uk/coronavirus/working-safely/index.htm
Contact your MSO
NPA members
Independent community pharmacies in England, who are NPA members, can contact the NPA MSO through the
Pharmacy Services Team at the NPA for further information, advice and/or support on any patient safety or
pharmacy topic/matter by:
Tel: 01727 891800 (9am-6pm Mon-Fri, 9am to 1pm Sat)
Email: pharmacyservices@npa.co.uk (anytime)
Non-members
Independent community pharmacies in England with fewer than 50 branches who are currently not members of
the NPA can contact the MSO by:
Email: pharmacyservices@npa.co.uk
Include your pharmacy name, ODS code, name of the owner/superintendent pharmacist and their
telephone/mobile number, pharmacy’s NHSmail email address
State ‘Non-member MSO query’ in the subject field
Disclaimer: The information published is, to the best of our knowledge, correct at the time of publication.
However, no responsibility will be accepted for any consequences of decisions made using this information.
© NATIONAL PHARMACY ASSOCIATION
MALLINSON HOUSE, 38-42 ST PETER’S STREET, ST ALBANS AL1 3NP
Tel: 01727891800
Email: pharmacyservices@npa.co.uk
Website: https://www.npa.co.uk/services-and-support/patientsafety
© NATIONAL PHARMACY ASSOCIATION, 2020You can also read