NOVITA' SULLA RIANIMAZIONE NEONATALE - Fabrizio Ciralli, Mara Vanzati UO Neonataologia e Terapia Intesiva Neonatale - MCA ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NOVITA’ SULLA RIANIMAZIONE
NEONATALE
Fabrizio Ciralli, Mara Vanzati
UO Neonataologia e Terapia Intesiva Neonatale
Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico
Università degli Studi di Milano
POPOLAZIONE TOTALE NEONATALE
Il 5 al 10% dei neonati richiede qualche forma di
assistenza per iniziare a respirare (es. stimolazione)
3% richiede PPV
1% richiede EET
0.1% richiede MCE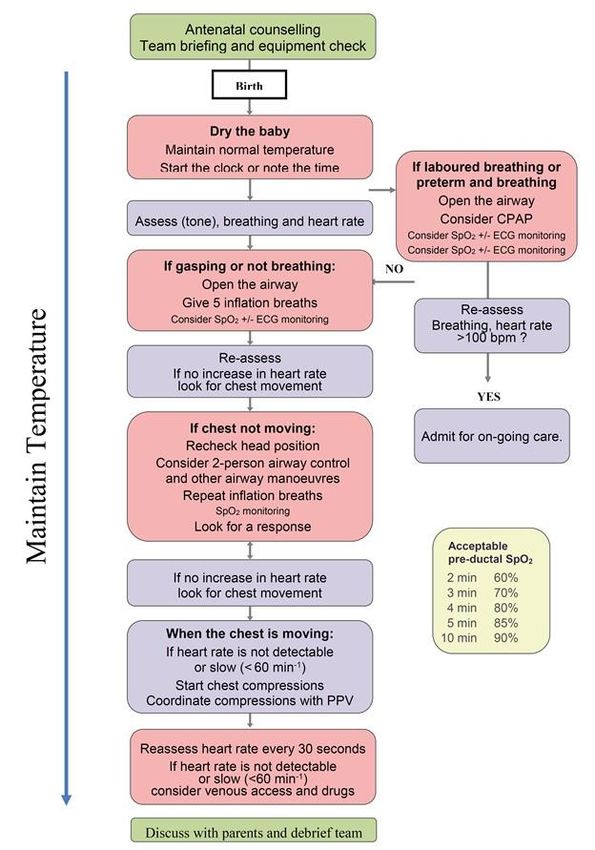
Neonatology 2008

Antenatal counselling
Team briefing and equipment check
2015 American Heart Association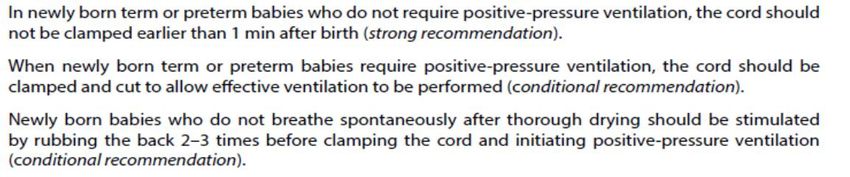
Antenatal counselling
Team briefing and equipment check
Discuss
2015withERC
2015 ERC Guidelines parents and debrief team
Guidelines
2015 ERC Guidelines
CONCETTI NUOVI…a chi applichiamo le linee guida?
• Newly born: neonato al momento della nascita; durante il processo
ditransizione da vita intrauterina a vita extrauterina
• Newborn: neonato che ha completato il processo di transizione e richiede
rianimazione nelle prime settimane di vita
RIANIMAZIONE DEL NEONATO ALLA NASCITA E
DURANTE LA FASE INIZIALE DI OSPEDALIZZAZIONE
2015 American Heart Association
2015 ERC Guidelines
LINEE GUIDA: cambiamenti maggiori • Valutazione iniziale • MAS Sindrome da aspirazione di meconio • Ossigenazione • Ventilazione • Cord clamping • Etica • Educazione

LINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Cord clamping
• Etica
• Educazione
DETERMINAZIONE DELLA FREQUENZA CARDIACA
PULSAZIONE CORDONE AUSCULTAZIONE ECG
OMBELICALE
2005 2010 2015
DETERMINAZIONE DELLA FREQUENZA CARDIACA
Treatment Recommendation
In babies requiring resuscitation we suggest ECG can
be used to provide a rapid and accurate estimation
of heart rate. (Weak suggestion, very low quality of
evidence).
2015 American Heart Association
2015 ERC GuidelinesMcCarthy L, Pediatriscs 2013
Trevisanuto D, Resuscitation 2
Temperatura in Jia
salaYS, J Perinatol 2013
Infant warmer Mathew B, J Perinatol 2013
Materasso riscaldante
parto Kent A, Jpaed Child Health 2008 Simon P, J Perinatol 2013
Miller SS, J Perinatol 2011
CapCappellino in polietilene Sacchetto in polietilene
Plastic bag
Vohra S, J Pediatr 1999
Vohra S, J Pediatr 2003ROOM TEMPERATURE
TEMPERATURA IN SALA PARTO
> 25° C
World Health Organization 2003Uso di sacchetti di polietilene per la prevenzione della perdita di calore
Use of polyethylene bags/wrap for thermal
60
loss prevention54%
pTesta: 20.8% della superficie Il cappellino copre il 75% del 20.8% pari al 15.6% di tutta la superficie
TEMPERATURA (linee guida 2015)
• Ipotermia (< 36,5 C) come outcome predittivo negativo
• L’ipotermia aumenta il rischio di IVH, problemi respiratori, ipoglicemia, sepsi
tardiva
• Si raccomanda di evitare l’ipotermia mantenendo la temperatura del neonato
tra 36,5 e 37,5 gradi centigradi dopo la nascita
Per ogni grado di riduzione della temperatura
• I neonati prematuri
cutaneasono
si haa un
maggior rischio
aumento di ipotermia
di mortalità del 28%
• Per tutti i neonati con EG < 32 wks utilizzo di calore radiante, sacchetti di
plastica, cappellino, materassini termici, gas per la rianimazione riscaldati ed
umidificati, aumento della temperatura della stanza adibita alla rianimazione
2015 American Heart Association
2015 ERC GuidelinesLINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Cord clamping
• Etica
• EducazioneAspirazione orofaringea e nasofaringea del neonato con liquido tinto
prima di liberare le spalle:
studio multicentrico randomizzato controllato
Meconium aspiration syndrome
Conclusions
Routine intrapartum oropharyngeal and
I ntubation Expectant
nasopharyngeal suctioning of term-gestation
management
infants born through MSAF does not prevent
Neonates ( n.)
MAS. Consideration 1051
should be given to revision1043
of present recommendations
MAS 34 (3.2%) 28 (2.7%)
Other 40 (3.8%) 47 (4.5%)
respiratory Vain NE et al, Lancet 2004Endotracheal Suction for Nonvigorous
61
Neonates Born through Meconium
61
Stained Amniotic Fluid: A Randomized
Controlled Trial
Endotracheal suctioning did not significantly reduce the risk
of MAS in non vigorous babies born through MSAF
The current practice of routine endotracheal
suctioning for non-vigorous neonates born
through MSAF should be further evaluated
Chettri S et al, J Pediatr 2015LINEE GUIDA 2015
Meconium aspiration syndrome
I ntubation Expectant
management
Neonates ( n.) 1051 1043
MAS 34 (3.2%) 28 (2.7%)
Other 40 (3.8%) 47 (4.5%)
respiratory
disordersGestione del neonato in sala parto in presenza di liquido
amniotico tinto di meconio (linee guida 2015)
Meconium: Tracheal intubation should not be routine in the presence of
meconium and should only be performed for suspected tracheal obstruction. The
emphasis should be on initiating ventilation within the first minute of life in non-
breathing or ineffectively breathing infants and this should not be delayed
The presence of thick, viscous meconium in a non-vigorous baby is the
only indication for initially considering visualising the oropharynx and
suctioning material, which might obstruct the airway
2015 American Heart Association
2015 ERC GuidelinesLINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Cord clamping
• Etica
• EducazioneIntrauterine (liquid)
Ambiente intrauterino Extrauterine
Ambiente (air)
extrauterino
(liquido)
environment environment
(aria)
[SaO2=50%]
SatO2 50% [SaO2=
SatO2 59% a59%
1 min(1 min)
68% a 2 min
68% (2 min)
82% a 5 min
82% (5 min)
90% a 15 min
House JT et al, JHouse
Clinic JT, J Clin
Monit Monit 1987
1987 SaO2= 90% (15 min) ]TrevisanutoOxygen to initiate resuscitation
in preterm infants
FiO2 per iniziare la rianimazione nel neonato pretermine
Oxygen (%) 90%
30% 30%
21%
2010 2015LINEE GUIDA 2015
Resuscitation of preterminfants less than 35 weeks gestation at birth should be
initiated in air or low concentration oxygen (21–30%)
In a meta-analysis of seven randomized trials comparing initiation of resuscitation
with high (>65%) or low (21–30%) oxygen concentrations, the high concentration
was not associated with any improvement in survival, bronchopulmonary dysplasia,
intraventricular haemorrhage or retinopathy of prematurity. There was an increase
in markers of oxidative stress
Vento M, et al. Pediatrics 2009;4
Kapadia VS, et al. Pediatrics 2013;132:e1488–96
Lundstrom KE, et al. Arch Dis Child Fetal Neonatal Ed 1995;73. F81-F6.
Rabi Y, et al. Pediatrics 2011;128:e374–81 2015 American Heart Association
Wang CL, et al. Pediatrics 2008;121:1083–9
2015 ERC GuidelinesLINEE GUIDA 2015
In term infants receiving respiratory support at birth with positive pressure
ventilation (PPV), it is best to begin with air (21%) as opposed to 100%
oxygen. High concentrations of oxygen are associated with an increased
mortality and delay in time of onset of spontaneous breathing, therefore, if
increased oxygen concentrations are used they should be weaned as
soon as possible
Davis PG, et al. Lancet 2004;364:1329–33
Vento M, et al. Pediatrics 2009;4 2015 American Heart Association
2015 ERC GuidelinesLINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (SLI e maschera laringea)
• Cord clamping
• Etica
• EducazioneSustained Lung Inflation at Birth for Preterm Infants: A
Randomized Clinical Trial
Our study found that SLI followed by early CPAP in the delivery room decreased the need for MV
in the first 72 hours of life in extremely preterm infants compared with nCPAP alone but did not
decrease the need for respiratory support and the occurrence of BPD
Lista G, Dani C et al, Pediatrics 2015Sustained Lung Inflation at Birth for Preterm Infants: A
Randomized Clinical Trial
Lista G, Dani C et al, Pediatrics 2015Sustained Lung Inflation at Birth for Preterm Infants:
A Randomized Clinical Trial
We believe that other clinical studies are necessary to
investigate the effectiveness of SLI in improving outcomes
in extremely preterm infants. Until these studies are
available, the SLI maneuver cannot be recommend as
routine prophylactic assistance in preterm infants in the
delivery room
Sustained Aeration of I nfant Lungs Trial ( SAI L)
- 23-26 weeks gestation (end of study: 2017)
Lista G, Dani C et al. Pediatrics 2015
Lista G, Dani C et al, Pediatrics 2015SLI IN SALA PARTO
There are insufficient data regarding short and long-term safety
and the most appropriate duration and pressure of inflation to
support routine application of sustained inflation of greater than 5
seconds’ duration to the transitioning new- born (Class IIb, LOE B-
R). Further studies using carefully designed protocols are needed
2015 American Heart Association
2015 ERC GuidelinesSupreme Laryngeal Mask Airway versus Face Mask during
Neonatal Resuscitation: A Randomized Controlled Trial
In this RCT, we assessed the effectiveness and the safety of the neonatal
SLMA in administering PPV at birth. The SLMA was more effective than
face mask in preventing endotracheal intubation in newborns with
gestational age >= 34 weeks and/ or expected birth weight >= 1500 g
needing resuscitation at birth. It is safe and effective in clinical practice
after a short-term educational program
Trevisanuto D et al, J Pediatr 2015MASCHERA LARINGEA
• A laryngeal mask may be considered as an alternative to tracheal intubation if
face-mask ventilation is unsuccessful in achieving effective ventilation
• A laryngeal mask is recommended during resuscitation of term and preterm
newborns at 34 weeks or more of gestation when tracheal intubation is
unsuccessful or is not feasible
• Use of the laryngeal mask has not been evaluated in the setting of meconium
stained fluid, during chest compressions or for administration of emergency
medications
2015 American Heart Association
2015 ERC GuidelinesPROSPETTIVE FUTURE
CAFFEINA The AIM of the study was to evaluate the respiratory effort of preterm infants at birth when caffeine was either administered directly after birth in the delivery room or after admittance to the neonatal intensive care unit (NICU)
RESULTS: respiratory effort parameters
MV at 7– 9 min after birth was significantly greater in the caffeine
delivery room group than in the control group.
Parameters assessing respiratory effort Vti, RoR, and the percentage
of recruitment breaths (except for respiratory rate) increased
significantly by caffeine administrationCONCLUSIONS
We observed a direct positive effect of administering
caffeine on the respiratory effort in preterm infants at
birth. The results of this study provide evidence,
indicating that caffeine could play a role in stimulating
breathing in preterm infants during the transition
Arjan B. te Pas et Al
Pediatric RESEARCH Volume 82 | Number 2 | August 2017LINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Cord clamping
• Etica
• EducazioneLINEE GUIDA 2010: Delay cord clamping
Treatment Recommendation
Delay in umbilical cord clamping for at least 1 minute is
recommended for new- born infants not requiring resuscitation.
There is insufficient evidence to support or refute a
recommendation to delay cord clamping in babies requiring
resuscitation
Perlman JM et al, Pediatrics 2010Delayed cord clamping
Delaying cord clamping
until ventilation onset
improves cardiovascular
function at birth in preterm
lambs
Bhatt S et al, J Physiol 2013Delaying cord clamping until ventilation onset improves
cardiovascular function at birth in preterm lambs
In conclusion, we have demonstrated that ventilation prior to umbilical cord
occlusion improved cardiovascular function and stability during the immediate
transition to neonatal life after birth in preterm lambs. We showed that the
initiation of ventilation prior to cord clamping mitigated most of the adverse
cardiovascular responses to cord clamping, indicating that the decrease in
pulmonary vascular resistance prior to cord clamping has a profound influence
on cardiovascular function after birth
Bhatt S et al, J Physiol 2013Neonatal Resuscitation 2015 American Heart Association
Guidelines Update for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care
DCC for longer than 30 seconds is reasonable for
both term and preterm infants who do not require
resuscitation at birth
There is insufficient evidence to recommend an approach to cord
clamping for infants who require resuscitation at birth, and more
randomized trials involving such infants are encouraged
2015 American Heart AssociationNeonatal Resuscitation 2015 American Heart Association
Guidelines Update for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care
In light of the limited information regarding the safety of
rapid changes in blood volume for extremely preterm infants,
we suggest against the routine use of cord milking for
infants born at less than 29 weeks of gestation outside of a
research setting
Further study is warranted because cord milking may improve initial mean
blood pressure and hematologic indices and reduce intracranial hemorrhage,
but thus far there is no evidence for improvement in long-term outcomes
2015 American Heart AssociationEuropean Resuscitation Council Guidelines for
Resuscitation 2015. Resuscitation and support of
transition of babies at birth
Delaying umbilical cord clamping for at least 1 min is
recommended for newborn infants not requiring resuscitation. A
similar delay should be applied to preterm babies not requiring
immediate resuscitation after birth
Until more evidence is available, infants who are not breathing or crying
may require the umbilical cord to be clamped, so that resuscitation
measures can commence promptly
2015 ERC GuidelinesEuropean Resuscitation Council Guidelines for
Resuscitation 2015. Resuscitation and support of
transition of babies at birth
Umbilical cord milking may prove an alternative in these infants
although there is currently not enough evidence available to
recommended this as a routine measure
Umbilical cord milking produces improved short term haematological outcomes,
admission temperature and urine output when compared to delayed cord clamping
(>30 s) in babies born by caesarean section, although these differences were not
observed in infants born vaginally
2015 ERC GuidelinesLINEE GUIDA 2015: Delay cord
Guidelines 2015 clamping
Delayed cord clamping
Treatment Recommendation
We suggest delayed umbilical cord clamping for
preterm infants not requiring immediate resuscitation
after birth. (Weak recommendation, very low quality
of evidence)
There is insufficient evidence to recommend an approach to
cord clamping for preterm infants who do receive resuscitation
immediately after birth, as many babies who were at high risk of
2015 American Heart Association
requiring resuscitation were excluded from or withdrawn from
the studies. 2015 ERC GuidelinesLINEE GUIDA 2015: Cord
Guidelines 2015milking
Cord milking
Treatment Recommendation
We suggest against the routine use of cord milking for
infants born at less than 29 weeks of gestation because
there is insufficient published human evidence of benefit.
Cord milking may be considered on an individualized basis
or in a research setting as it may improve initial mean
blood pressure, hematological indices and intracranial
hemorrhage. There is no evidence for improvement or Association
2015 American Heart
safety in long-term outcomes. (Weak recommendation,
2015 ERC GuidelinesApproccio fisiologico alla transizione feto-neonatale
PRIMA RESPIRARE!
2012RACCOMANDAZIONI ITALIANE PER LA GESTIONE DEL CLAMPAGGIO ED
IL MILKING DEL CORDONE OMBELICALE NEL NEONATO A TERMINE E PRETERMINE
Neonatologo bedside
Come implementare le pratiche del ritardato clampaggio rispettando le
indicazioni delle linee guida della rianimazione neonatale?
La presenza del neonatologo al letto della madre in tutti i parti con possibile
necessità di rianimazione permette di:
• individualizzare il clampaggio del cordone ombelicale attraverso la
valutazione del neonato all’estrazione
• garantire i primi passi della rianimazione prima del clampaggio del cordone
ombelicale.RACCOMANDAZIONE
Nel caso in cui il ritardato clampaggio con
valutazione bed-side da parte di personale ALL’ESTRAZIONE Neonatologo bedside
esperto non sia possibile, si suggerisce
l’esecuzione del milking a cordone intatto
(Raccomandazione debole) (2C). • Temperatura
• Posizione First step stabilization
• Aspirazione bedside
• Stimolazione
Valutazione a 30 secondi dalla nascita
FC < 100 BPM e/o FC > 100 BPM E
APNEA/GASPING PIANTO/SFORZO
RESPIRATORIO
Clampaggio del cordone ombelicale e inizio rianimazione Clampaggio a 60”
(raccomandazione forte) (raccomandazione forte)*LINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Cord clamping
• Etica
• EducazioneLINEE GUIDA 2015: SOSPENSIONE DELLA RIANIMAZIONE
If the heart rate of a newly born baby is not detectable and remains
undetectable for 10 min, it may be appropriate to consider
stopping resuscitation. The decision to continue resuscitation
efforts for longer than 10 min is often complex and may be
influenced by issues such as the presumed aetiology, the gestation
of the baby, the potential reversibility of the situation, the
availability of therapeutic hypothermia and the parents’ previous
expressed feelings about acceptable risk of morbidity. The decision
should be individualised
2015 American Heart Association
2015 ERC GuidelinesLINEE GUIDA 2015: SOSPENSIONE DELLA RIANIMAZIONE
In cases where the heart rate is less than 60 min 1 at birth and
does not improve after 10 or 15 min of continuous and
apparently adequate resuscitative efforts, the choice is much
less clear. In this situation there is insufficient evidence about
outcome to enable firm guidance on whether to withhold or
to continue resuscitation
2015 ERC GuidelinesLINEE GUIDA: cambiamenti maggiori
2010-2015
• Valutazione iniziale (FC e Temperatura)
• MAS Sindrome da aspirazione di meconio
• Ossigenazione
• Ventilazione (CPAP e SLI)
• Etica
• Cord clamping
• EducazioneEfficacy of the neonatal resuscitation program (NRP) course on
knowledge retained by residents:
Comparison among pediatrics, anesthesia and gynecology
Parrotto M et al. Resuscitation 2010LINEE GUIDA 2015: INSEGNAMENTO
The 2010 Guidelines suggested that simulation should become a
standard component in neonatal resuscitation training
Studies that explored how frequently healthcare providers or healthcare
students should train showed no differences in patient outcomes but were able
to show some advantages in psychomotor performance and knowledge and
confidence when focused training occurred every 6 months or more frequently.
It is therefore suggested that neonatal resuscitation task training occur more
frequently than the current 2-year interval
2015 American Heart Association
2015 ERC GuidelinesGRAZIE
You can also read