NAVICULA SURGICAL TECHNIQUE - Adlerortho
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ANTEA
NAVICULA
PROTESI DI
SCAPHOID CAPITELLO RADIALE
PROSTHESIS
SURGICAL TECHNIQUE
1
NAVICULA
SCAPHOID PROSTHESIS
Anatomically Distal stem designed to
shaped for an stabilize the implant into the
optimal fit. Trapezoid.
Ceramic
TiNbN Coating
improves
implant Surface
hardness and
biocompatibility.
Proximal holes to stabilize the
implant with an artificial ligament.
• Made Of Titanium with TiNbN antiallergic Coating.
• Anatomically Shaped.
• 4 progressively growing sizes left and right.
• Proximally and distally stabilized.
3
PRESENTATION AND CHARACTERISTICS
The Navicula system is available in 4
progressively growing Scaphoid implant sizes.
It has two stabilisation devices:
• Distally, a stem is moulded, to be inserted in
a hole bored into the trapezium/trapezoid;
• Proximally, two holes are bored, where an
artificial SLIL ligament fixed into the Lunate
bone is passed and then knotted. The Sz. 1 Sz. 2 Sz. 3 Sz. 4
knot is seated into the niche on the lateral
scaphoid surface.
The correct implant size is determined using
the patient scaphoid bone alongside the trial
implants supplied, in order to restore the
patient's normal anatomy.
TIP: if in between sizes, generally select the
smaller size.
INDICATIONS
• Irreparable fracture outcomes, not
suitable for any graft repair.
• Failed reconstructive surgery.
• No SNAC ≥ 2, radio-carpal and midcarpal
joint preserved, no carpal collapse.
CONTRAINDICATIONS
• Carpal collapse.
• SNAC > 2, radio-carpal and/or mid-carpal
joints changes or destruction.
4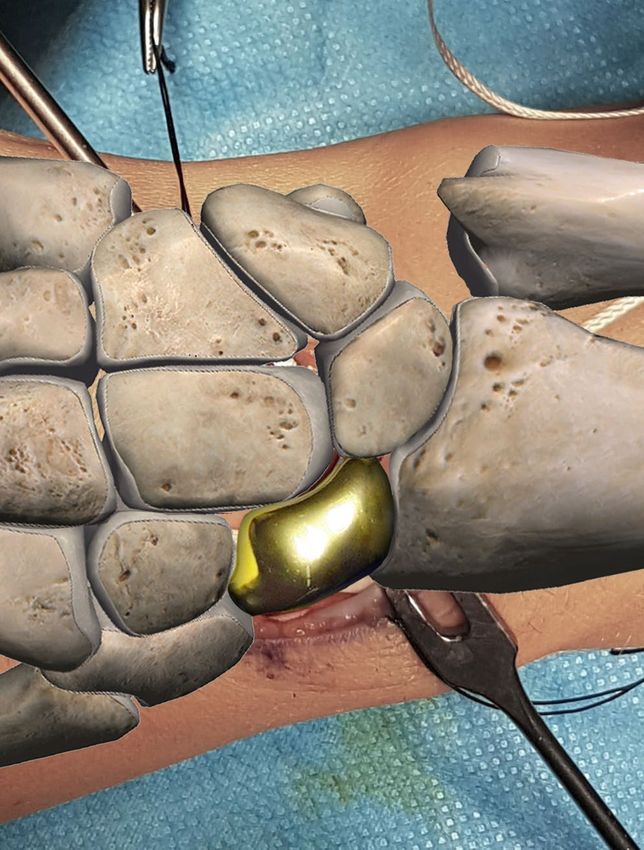
SURGICAL PROCEDURE STEPS
1 • Dorsal sinusoidal incision, Radial nerve branches isolated.
2 • Carpus exposure with a capsular flap radially based, and scaphoid removal.
TIP: The volar ligaments and capsule MUST be
preserved, retaining a volar scaphoid bone chip.
5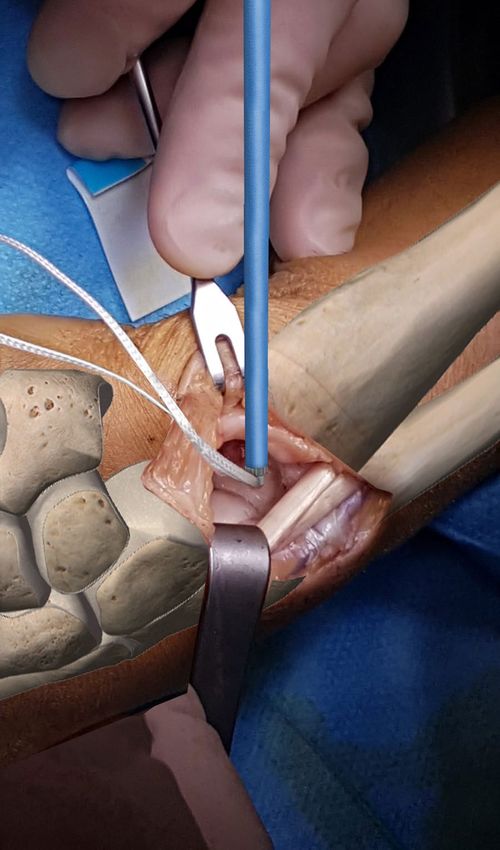
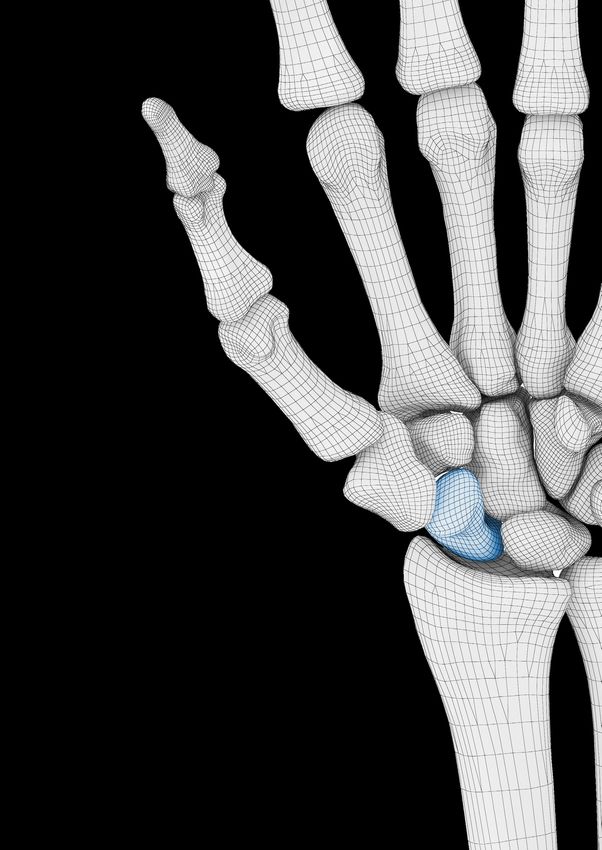
3 • Preparation of the hole to secure the implant distal stem, key for distal stability.
A 2 mm K.wire is drilled into the trapezium-trapezoid midline, considering that the
correct position is the one in line with the 1st metacarpal midshaft.
The Scaphoid implant distal stem location hole is made using a cannulated hand
instrument, perfectly matching the implant distal stem, to be inserted using the K.wire
guide.
6
4 • An anchor is inserted in the lunate bone to hold the artificial ligament
(Arthrex labral tape).
5 • The ligament is then passed through the two distal holes available on the implant.
NOTE: Anchor and synthetic ligament are not included in the Navicula Scaphoid
Surgical Instrument Set.
7
6 • The distal stem is placed in the previously prepared hole in the Trapezium, the implant
is then placed in situ and the ligament is progressively tensioned and finally knotted.
The knot is placed into the niche carved on the lateral scaphoid surface.
8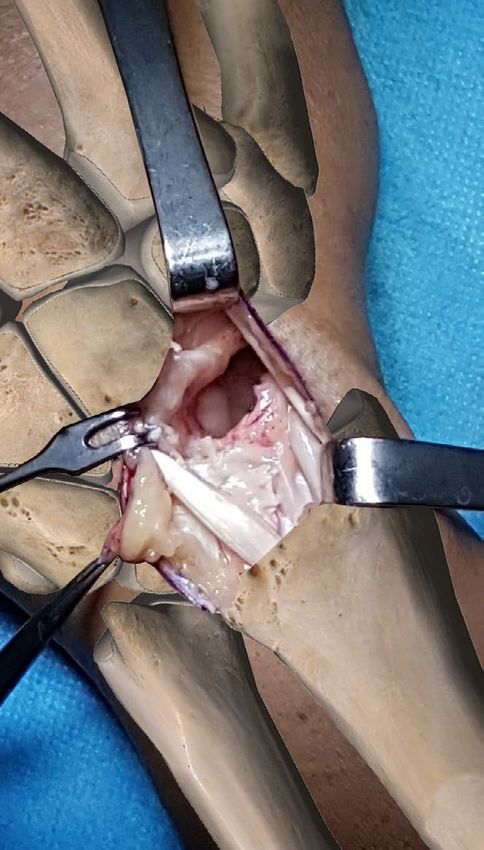
The post-op X-ray control should show the restoration of the Gilula arcs, while the stem
placed in the Trapezium should have a radium-Scaphoid angle < 30°.
15°
7 • The dorsal capsule is then closed with non-absorbable sutures.
TIPS: capsular suture to be performed in a semi-flexed wrist position.
In case of damaged capsule, use a flap of extensor retinaculum to complete or reinforce
the capsular reconstruction.
9
Final X-Ray controls
10IMPLANTS
Code Description
3400001 NAVICULA SCAPHOID SIZE 1 LEFT
3400002 NAVICULA SCAPHOID SIZE 2 LEFT
3400003 NAVICULA SCAPHOID SIZE 3 LEFT
3400004 NAVICULA SCAPHOID SIZE 4 LEFT
3400011 NAVICULA SCAPHOID SIZE 1 RIGHT
3400012 NAVICULA SCAPHOID SIZE 2 RIGHT
3400013 NAVICULA SCAPHOID SIZE 3 RIGHT
3400014 NAVICULA SCAPHOID SIZE 4 RIGHT
A
SIZE A B C C
1 28.5 11.4 14.5
B
2 29.9 12.1 15.4
3 31.3 12.8 16.2
4 32.5 13.5 17.2
11Bibliography
A.B. Swanson et al. "Scaphoid implant resection arthroplasty. Long-term results". The Journal of Arthroplasty;
1(1):47-62. 1986.
A.B. Sattel, A.B. Swanson, G. De Groot Swanson: "Titanium scaphoid implant for scaphoid nonunion".
Operative Techniques in Orthopaedics. Volume 2, Issue 1, pagg. 32-38, 1992.
M.I. Rossello et.al.:"La sostituzione protesica dello scafoide carpale". Riv. Chir: Riab.Arto Sup. XXXI, 1, 1994.
M.I. Rossello, M. Costa, M. Bertolotti: "La susticion protesica del escafoides carpiano". Rev Esp. Cir. mano
N° 48,Vol. 21, 1994.
M.I. Rossello, F. Moretti, G. Priano, G. Novara: "Scaphoid total arthroplasty: our 20 years experience in 71
cases". Abstract book 6th Congress IFSSH, rif. P 083, 1995.
M.I. Rossello, M. Costa, V. Pizzorno: "La sostituzione protesica" Cap. 12 de "Lo scafoide" Monografia della
SICM, Casa Ed. Mattioli, Parma 1997.
M.I. Rossello: "Trattamento degli insuccessi nella patologia dello scafoide: le protesi”. Riv Chir Riab Mano
38 (2), 2001.
O. Spingardi, M.I. Rossello: "The total scaphoid titanium arthroplasty: a 15 year experience". HAND 6;179-
184, 2011.
M.I. Rossello, A. Zoccolan, O. Spingardi: "Protesi totale di scafoide in titanio". Medicina e chirurgia ortopedica
ricerca tecnologia innovazione, Vol. 1 , 2012.
M.I. Rossello, O. Spingardi: "The total scaphoid titanium arthroplasty". Arch,.Ortop. Reum.Vol. 126, 1-3 2015.
M.I. Rossello. "A case of total scaphoid titanium custom-made 3D-printed prostheses with one-year follow-
up". Case Reports in Plastic Surgery and Hand Surgery. VOL. 7, NO. 1, 7–12. 2020.
Manufactured by ADLER ORTHO SpA ADLER ORTHO UK
Manufacturing Unit The Stables
and main office Tarvin Road
Via dell’Innovazione 9 Frodsham - Cheshire -
20032 Cormano (Mi) WA6 6XN
Tel. +39 02 6154371 Tel: +44151 329 3372
01 - 2021
Fax +39 02 615437222
www.adlerortho.com
T-0033-EYou can also read