Multifactor Analysis of Costal Pain in Osteoporotic Fracture of Thoracic Vertebra
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pain Physician 2021; 24:E795-E802 • ISSN 2150-1149
Retrospective Study
Multifactor Analysis of Costal Pain in
Osteoporotic Fracture of Thoracic Vertebra
Jun Xin, MD1, Xiaoyang Liu, PhD2, Xingzhi Jing, PhD2, Cheng Su, MD3, Yi Mao, MD4,
Feifei Chen, PhD2, Wenchao Wang, MD3, and Xingang Cui, PhD1
From: 1Shandong Province Background: The costal pain is common in thoracic osteoporotic fracture patients. It is unclear
Hospital, Shandong University why vertebral fracture patients without any specific nerve impingement on magnetic resonance
School of Medicine: Shandong
University Cheeloo College imaging (MRI) present with costal pain.
of Medicine, Jinan, PR China;
2
Shandong Provincial Hospital, Objectives: The aim of this study was to investigate the potential causes of costal pain in patients
Jinan, PR China; 3Shandong with osteoporotic fracture of thoracic vertebra.
First Medical University,Tai’an
Campus, Jinan, PR China;
4
People’s Hospital of Quzhou, Study Design: A retrospective study.
Jinan, PR China
Setting: Shandong province, China.
Address Correspondence:
Xingang Cui, PhD
Shandong First Medical Methods: In this retrospective study, 100 patients with thoracic osteoporotic fractures were
University as the Shandong collected and assigned into 2 groups on the basis of pain patterns noted during medical history
Provincial Hospital Affiliated and physical examination. Group A was comprised of 50 patients with costal pain. Group B was
to Shandong First Medical comprised of 50 patients without costal pain. The Visual Analog Scale and Oswestry Disability
University, Shandong Provincial
Hospital Affiliated to Shandong Index scores were recorded to assess the pattern and severity of pain. The gender, age, presence or
University, No 9677, Jingshi Road, absence of trauma, time of fracture, fracture segments, and analgesic application were recorded.
Jinan 250013, PR China Computed tomography data including changes in fracture vertebral body shape (height, width,
E-mail: xinhuadegege@163.com and length), intervertebral foramen shape (height and width), wedge shape of fractured vertebral
Disclaimer: There was no external body, and local kyphosis angle were recorded. The fracture edema signal was determined by MRI.
funding in the preparation of this Multivariate analysis was performed for all the above parameters.
manuscript.
Results: There was a statistically significant difference in the vertebral body width between the
Conflict of interest: Each author
certifies that he or she, or a
2 groups.
member of his or her immediate
family, has no commercial Limitations: The number of patients enrolled is not large enough. We also have limitations in
association (i.e., consultancies, interpreting all pains resulting from osteoporotic vertebral compression fractures, because all pain
stock ownership, equity interest,
mechanisms are not fully understood. Further work is needed to improve the accuracy of locating
patent/licensing arrangements,
etc.) that might pose a conflict of pain sources and distinguishing pain patterns which may result from other spinal structures.
interest in connection with the
submitted manuscript. Conclusion: The incidence of costal pain is significantly and positively associated with the width
of the fractured vertebra in patients with osteoporotic thoracic vertebrae fracture.
Manuscript received: 08-01-2020
Revised manuscript received:
12-07-2020 Key words: Osteoporosis fracture, thoracic vertebrae, costal pain, nonmidline pain, intervertebral
Accepted for publication: foramen, sympathetic nerve
01-20-2021
Free full manuscript:
Pain Physician 2021: 24:E795-E802
www.painphysicianjournal.com
O steoporosis is a severe worldwide public
health problem due to its high morbidity
and mortality. As one of the most common
complications of osteoporosis, osteoporotic spine
fractures mainly occur in the thoracolumbar segment,
and patients often complain of severe low back pain in
the corresponding fracture area (1,2). Local tenderness
over the spinous processes of the fractured vertebra
www.painphysicianjournal.com
Pain Physician: September/October 2021 24:E795-E802
and magnetic resonance imaging (MRI) signals of bone pain. The Visual Analog Scale (VAS) score (in the range
marrow edema is common in patients with osteoporotic of 0 = no pain to 10 = worst pain) for pain evaluation
spine fracture (3,4). However, several studies have and the Oswestry Disability Index (ODI) score (sexual
reported that certain vertebral fractures have no focal activity excluded) were conducted for functional assess-
tenderness and local pain over the fractured level, but ment. The fracture types of the vertebral body were
with nonmidline pain in the chest, lower back, near the classified into 3 types: 1) wedge, 2) biconcave, and 3)
iliac crest, the groin, and the trochanteric region (5-8). It crush deformities (8).
is unclear why vertebral fracture patients present with
distal pain without any specific nerve impingement on Considered Parameters
MRI (9). In the previous studies, a variety of causes have The following data were recorded: sex, age, bone
been mentioned, including sympathetic nerve injury, mineral density of the vertebral body, type of fracture,
vertebral body height decline, foramen narrowing, presence or absence of trauma, time of fracture, and
facet changes, disc tearing, and paravertebral muscle the analgesic application. They were obtained from
overload (6,9). However, to our knowledge, the the patients’ medical records and MRI. The level and
relationship between nonmidline pain and fracture type of fractures were divided into 3 categories (less
morphology still remains elusive. The diversity of clinical than 1/3, 1/3-2/3, more than 2/3) according to the sig-
manifestations of nonmidline pain makes it difficult nal scope and intensity of T2-weighted image in the
to analyze its causes. Thoracic vertebra fractures are MRI.
relatively common in osteoporotic fractures. In this Computed tomography (CT) data were collected
study, we chose the costal pain to study the cause of to evaluate the morphology of fractured vertebral
nonmidline pain of thoracic vertebra osteoporotic body and intervertebral foramen. GE Medical Systems’
fractures. We also measured the relevant data of the measurement was conducted to avoid personal error
morphological changes of fractured vertebra and on the film.
intervertebral foramina to elucidate its possible causes
and mechanisms. Measurement of Vertebral Body
Firstly, after locating the center of the injured
Methods vertebral sagittal position, we selected the lower
edge of the injured vertebral pedicle as the baseline
Patient Selection to locate the coronal plane of the injured vertebra
One hundred patients with single-segment tho- and measured the maximum width of the injured
racic osteoporotic fractures, admitted to Shandong vertebra. If the fracture involved only the upper or
Provincial Hospital from 2017 to 2020, were enrolled lower part of the vertebral body, the 3 physicians
and retrospectively studied, including the youngest jointly discussed and decided to select a more appro-
51 years old and the oldest 95 years old. Institutional priate coronal plane and record the maximum width
review board approval was granted for the study. The of the injured vertebral body. Changes in vertebral
patients were selected according to the following in- body width were calculated by the ratio of fractured
clusion criteria: 1) Thoracic osteoporotic fracture was vertebral body width to [(upper adjacent body width
confirmed by thoracic x-ray and MRI, and the fracture + lower adjacent body width)/ 2]. Locating the sagit-
time was less than 3 weeks. 2) All patients had osteo- tal center of the injured vertebra, and measuring the
porosis (vertebra or femoral neck T-scoreMultifactor Analysis of Costal Pain
of the adjacent normal vertebrae was measured at
the same position as the injured vertebrae. Changes
in vertebral length were described by corresponding
ratios: fractured vertebral length / [(upper adjacent
vertebral length + lower adjacent vertebral length)/
2] (Fig. 1).
Measurement of Intervertebral Foramen Size
Because the changes of the morphology of the
injured vertebra will affect the upper and lower
intervertebral foramen of the injured pedicle, the 2
intervertebral foramens were analyzed separately.
The length of the intervertebral foramen refers
to the distance between the upper and lower 2
pedicles. The width is the distance from the lower
angle of the posterior margin of the upper vertebral
body to the apex of the superior articular process
of the lower vertebral body. The change in foramen
was described by the corresponding ratio: foramen
length above the vertebral pedicle of the fractured
vertebra / [(foramen length above the pedicle of up-
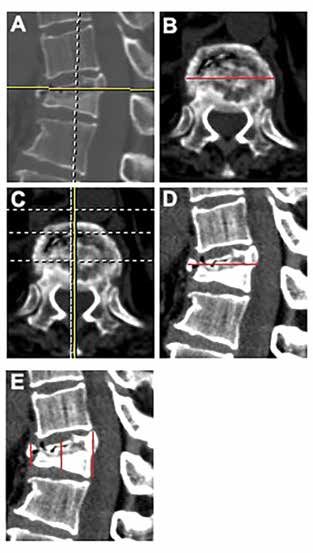
per adjacent vertebra + foramen length below the Fig 1. (A) The center of
pedicle of the lower adjacent vertebra)/ 2]. Foramen the injured vertebral body
length of lower pedicle of fractured vertebra / [(fo- in sagittal position on CT
(B,C). The coronal image of
ramen length above the pedicle of upper adjacent the yellow line of the vertebral
vertebra + foramen length below the pedicle of the body in A. The red line
lower adjacent vertebra)/ 2]. The change in the width represents the width of the
vertebral body (D,E). The
of the intervertebral foramen was calculated in the sagittal images of the injured
same way (Fig. 2). vertebra at the yellow line in
C, the red line represents the
length of the injured vertebra
Measurement of Kyphosis and Vertebral Wedge and the height of the anterior,
Formation middle and posterior.
Local kyphosis was evaluated by the Cobb angle
between the superior endplate of the upper vertebra
and the inferior endplate of the lower vertebra ad- Statistical Analysis
jacent to the fracture. The Cobb angle between up- Statistical analysis was performed using SPSS 25.0
per and lower endplates of the injured vertebra was (SPSS Inc, Chicago, IL, USA). The data of patients with
measured to evaluate the wedge shape of the injured and without costal pain in osteoporotic fracture of
vertebra. Changes in the vertebral body were described thoracic vertebra were compared using t test or Chi
by the corresponding ratio: fracture vertebral wedge square test. Any significant difference (P < 0.05) was
/ [(upper adjacent vertebral wedge + lower adjacent also analyzed using binary logistic regression analysis,
vertebral wedge)/ 2] (Fig. 3). and then P value < 0.05 was considered to be statisti-
The measurements were performed twice to the cally significant.
nearest 0.1 mm. If the 2 measurements showed a dif-
ference of more than 1 mm, a third measurement was
Results
taken and the average of all was used.
We collected as much data as possible to reflect Demographic Data
the morphological changes of the vertebral body, and The clinical characteristics of patients are shown in
analyzed them separately, trying to find the relation- Table 1. The average ages in the costal and noncostal
ship between costal pain and fracture morphology. groups were 68.8 ± 6.9 and 69.8 ± 9.0 years, respectively.
www.painphysicianjournal.com E797Pain Physician: September/October 2021 24:E795-E802
In both groups, the lower thoracic segment (T10-T12)
was the most common level of fracture site (Table 1).
There was significant difference in trauma or not,
analgesic or not, and the VAS between the 2 groups
(P < 0.05).
No statistical significance in the fracture level,
magnetic resonance edema signal size, classification
of fracture types, symptom duration or ODI (P > 0.05)
were observed between the 2 groups.
Comparison of Parameters
There was significant difference in vertebral frac-
ture width, anterior, and middle height between the 2
groups (P < 0.05). While there was no significant differ-
ence in vertebral length or posterior height (P > 0.05)
(Table 2).
There was significant difference in width of left
upper intervertebral foramen or width of right up-
per intervertebral foramen between the 2 groups (P <
0.05). There was no significant difference in the other
parameters of the intervertebral foramen between the
2 groups (P > 0.05) (Table 3).
No significant difference in the wedge angle and
local kyphosis angle was observed between the 2
groups (P > 0.05) (Table 4).
Our t test or Chi square test results showed signifi-
cant differences in the changes of the vertebral fracture
Fig 2. (A) The coronal image of the vertebral pedicle
plane of the fractured vertebra (B,C). The sagittal image width, anterior, and middle height, the width of left
of the yellow line in A. (B) The red line represents the and right upper intervertebral foramen, trauma or not,
height and width of the intervertebral foramen. (C) The analgesic or not, and the VAS between the 2 groups.
red line shows the height and width of the intervertebral To further analyze the correlation of the 8 factors, bi-
foramen below the pedicle. (D) Yellow arrows show the
nary logistic regression analysis was conducted. Binary
middle 2 intervertebral foramina affected by the fracture,
and the mean height and width of the 2 foramina at both logistic regression analysis showed that the change of
ends. the vertebral body width was a constant significant
predictor of costal pain for all patients (P = 0.00, Exp
(B) = 4.531E + 50). Following
binary logistic regression
analysis, the other 7 factors
were no longer predictors
of costal pain (P > 0.05).
The incidence of costal pain
was higher in patients with
increased fracture vertebral
width after adjusting for
the other 7 factors in binary
logistic regression model
(Table 5).
Fig 3. (A) The coronal image of the injured vertebral body. (B,C) The sagittal image of The vertebral width in
the vertebral body at the yellow line of A. The wedge shape and local kyphosis angle of the patients with costal pain
vertebral body were measured, respectively. was significantly higher
E798 www.painphysicianjournal.comMultifactor Analysis of Costal Pain
Table 1. Characteristics of osteoporotic thoracolumbar vertebral Table 2. Results of the relationship between fracture intercostal
fracture patients. neuralgia and vertebral height and width.
Total Group A Group B P Group A Group B
P value
(n = 100) (n = 50) (n = 50) value (n = 50) (n = 50)
Age (years) 69.3 ± 8.0 68.8 ± 6.9 69.8 ± 9.0 0.51 VFW (%) 1.18 ± 0.11 1.01 ± 0.02 0.00
Female gender 16/84 9/41 7/43 0.59 VFL (%) 1.05 ± 0.08 1.03 ± 0.05 0.14
Fracture level 100 50 50 0.33 AVH (%) 0.73 ± 0.19 0.82 ± 0.18 0.02
T6 1 1 0 MVH (%) 0.64 ± 0.19 0.73 ± 0.20 0.03
T7 6 3 3 PVH (%) 0.91 ± 0.10 0.92 ± 0.09 0.50
T8 8 3 5 The results are expressed as mean ± SD.
T9 7 3 4 Abbreviations: VFW, vertebral fracture width; VFL, vertebral fracture
length; AVH, anterior vertebral height; MVH, middle vertebral height;
T10 18 5 13
PVH, Posterior vertebral height.
T11 17 10 7
T12 43 25 18 Table 3. Results of the relationship between fracture intercostal
neuralgia and bilateral intervertebral foramen.
Magnetic
resonance 100 50 27 0.90 Group A Group B
P value
edema signal (n = 50) (n = 50)
< 1/3 15 8 7 ULFH (%) 0.91 ± 0.13 0.88 ± 0.14 0.30
1/3-2/3 32 15 17 ULFW (%) 1.04 ± 0.18 0.94 ± 0.19 0.01
> 2/3 53 27 26 URFH (%) 0.90 ± 0.11 0.89 ± 0.12 0.70
Fracture URFW (%) 1.03 ± 0.18 0.96 ± 0.18 0.04
100 50 50 0.44
classification
LLFH (%) 0.99 ± 0.16 0.96 ± 0.14 0.26
Wedge 46 20 26
LLFW (%) 1.01 ± 0.23 1.05 ± 0.24 0.45
Biconcave 42 24 18
LRFH (%) 0.94 ± 0.13 0.92 ± 0.12 0.40
Crush 12 6 6
LRFW (%) 1.03 ± 0.21 0.98 ± 0.22 0.28
Symptom
11.8 ± 5.7 13.5 ± 5.1 10.1 ± 5.8 0.48 The results are expressed as mean ± SD.
duration (days)
Abbreviations: ULFH, left of upper intervertebral foramen height;
Trauma or not 45/55 29/21 16/34 0.01 ULFW, width of left upper intervertebral foramen; URFH, right upper
Analgesic or not 42/58 28/22 14/36 0.01 intervertebral foramen height; URFW, width of right upper interver-
tebral foramen; LLFH, left of lower intervertebral foramen height;
VAS 6.4 ± 1.3 5.8 ± 1.2 6.9 ± 1.1 0.00 LLFW, width of left lower intervertebral foramen; LRFH, right lower
64.3 ± intervertebral foramen height; LRFW, width of right lower interverte-
ODI 67.4 ± 12.8 70.6 ± 12.3 0.13
12.6 bral foramen.
The continuous variables are expressed as mean ± SD; the categorical Table 4. Results of the relationship between fracture intercostal
variables are expressed as frequency. neuralgia and local kyphotic angle and wedge-shaped vertebral
Abbreviations: VAS, visual analog scale; ODI, Oswestry disability body.
index.
Group A Group B
than that without costal pain (P < 0.05). The incidence P value
(n = 50) (n = 50)
of costal pain is significantly and positively associated LKA (°) 16.33 ± 9.64 13.5 ± 9.57 0.15
with the width of the fractured vertebra in patients WVB (%) 3.60 ± 3.97 3.10 ± 3.96 0.53
with osteoporotic thoracic vertebrae fracture (Fig. 4).
The results are expressed as mean ± SD.
Discussion Abbreviations: LKA, local kyphotic angle; WVB, wedge-shaped verte-
bral body.
Several studies have reported that patients with
certain vertebral fractures have no focal tenderness nerve impingement on MRI present with nonmidline
and local pain over the fractured level (5-8). Patients pain (9). In the previous studies, a variety of causes have
with vertebral fractures may present with nonmidline been mentioned, including sympathetic nerve injury,
pain in the chest, lower back, near the iliac crest, the vertebral body height decline, foramen narrowing,
groin, and the trochanteric region (6,7). It is unclear facet changes, disc tearing, and paravertebral muscle
why vertebral fracture patients without any specific overload (6,9).
www.painphysicianjournal.com E799Pain Physician: September/October 2021 24:E795-E802
Table 5. Associations between the occurrence of intercostal
neuralgia in the intercostal neuralgia and clinical factors, deter- Doo et al (8) reported that the decreased vertebral
mined by binary logistic regression analysis. body height could damage the surrounding zygapoph-
(95%CI) yseal joint and narrow the intervertebral foramen, thus
Sig irritate the posterior branches of the spinal nerve at
Parameters B Exp (B) for Exp
(B) T12, L1, and L2. Remarkably, their study showed a sig-
nificant association between the nonmidline pain and
4.693E+17-
MVW (%) 116.6 4.531E+50 0.00 deformity index (height of vertebral bodies). Moreover,
4.374E+83
they found that pain was extended from the anterior
Trauma or not - - - 0.93
chest to the lowest height of the vertebral body as the
Analgesic or not - - - 0.72
height of vertebral bodies decreased (8). However, our
VAS - - - 0.56 study showed that the occurrence of costal pain was
AVH (%) - - - 0.67 not significantly associated with changes in vertebral
MVH (%) - - - 0.15 body height (P > 0.05). Wilson et al (13) found that the
ULFW (%) - - - 0.40 facet joints may play important roles in the generation
URFW (%) - - - 0.25 of pain in most vertebral fracture patients. Biomechani-
Abbreviations: MVW, middle vertebral width; VAS, visual analog cal instability caused by an adjacent wedge fracture,
scale; AVH, anterior vertebral height; MVH, middle vertebral height; and subsequent sagittal imbalance as well as overload
ULFW, width of left upper intervertebral foramen; URFW, width of of facet joints and paraspinal muscles, were the rea-
right upper intervertebral foramen. sons for which patients felt pain at several vertebral
segments away from the fractures identified on imag-
ing (13). Choi et al (14) believed that the costal pain
developed more frequently in nonwedge deformities
compared to wedge-type fractures, which indicated
that middle column injuries could be an important
contributor to costal neuralgia following costal nerve
injury, the intervertebral foramen could also affect the
costal nerve and induce costal pain at the concordant
vertebral fracture level (14). In our study, however,
there was no significant correlation between costal
pain and foramina changes. Niu J et al (9) found that
kyphoplasty had a superior effect in relieving the
nonmidline pain caused by thoracolumbar vertebral
Fig 4. Scatter plots for the changes of the vertebral fractures. In their opinion, by means of the expansion
body width between the 2 groups. of the balloon and injection of cement, kyphoplasty
could restore the vertebral height, correct local kypho-
sis, eliminate micromotion within fractured vertebrae,
In 1991, Patel et al (10) found that “radiation to the and decrease the mechanical load pressed on the facet
flanks and anteriorly was common” by investigating 30 joints, which all decrease the irritation or compression
patients with acute vertebral compression fractures. In of the sympathetic ganglion or dorsal ramus (9). But
a 2006 study, they found that pain caused by the verte- the authors did not analyze the pain pattern and its
bral fracture in the thoracolumbar region was mainly in relation with the fracture region.
the lumbosacral gluteal area which could confuse the The results of our study indicated that nonmidline
surgeon in choosing treatment strategy (11). O’Connor pain is common in patients without imaging findings
et al (12) commented on thoracic radiculopathy in a of specific nerve impingement. The number of patients
bandlike distribution to the anterior thorax, chest, or with nonmidline symptoms may be understated, as
abdomen. The pain pattern might result from the ven- some patients who answered “no” to the question
tral rami of the thoracic. The explanation given for the regarding nonmidline symptoms lacked a pain loca-
referred pain is that the ventral rami of the thoracic tion diagram. Because patients often answered “no”
spine run anterolaterally between the ribs to innervate when asked if they had pain in other areas, but they
the chest and abdominal wall (12). would answer “yes” when asked if they have pain in
E800 www.painphysicianjournal.comMultifactor Analysis of Costal Pain
the anterior chest or the lateral ribs, these symptoms fractures (OVCFs). For patients with OVCFs, pain loca-
were often ignored. Some of these patients may have tion may not accurately reflect the fracture site. Both
nonmidline pain to the side or elsewhere which was physical examination and radiological image analysis
not addressed in the questionnaire (7). are required for correct diagnosis. Thus, for aged pa-
Our study showed that the occurrence of costal tients with the pain radiating to both or one side along
pain in osteoporotic thoracic vertebrae is related to the intercostal space or to the chest, their thoracic ver-
the change in the width of the vertebral body, the tebra should be examined, regardless of their trauma
incidence of costal pain in patients with the vertebral history in this region.
body bulging to both sides of the fractured vertebra A major limitation of this study is that the number
is relatively high. Anatomically, sympathetic nerve of patients enrolled is not large enough. Significant
chain is distributed on the side of the vertebral body, limitation being the need for prospective studies in
consisting of thoracic sympathetic ganglion and the patients with vertebral fractures with multiple vari-
sympathetic trunk. There are communication branch- ables. We also have limitations in interpreting all pains
es between the sympathetic chain and the intercostal resulting from OVCFs, because all pain mechanisms are
nerve. The range of costal pain was roughly the same not fully understood (9,16). In addition, nonmidline
as that of sympathetic nerve innervation. Therefore, pain has many locations and manifestations, which are
we speculated that the cause of costal pain was the relatively complex and need further clarification.
expansion of the fractured vertebra to both sides,
and the compression of the sympathetic nerve by
Conclusion
fracture block. Jinkins et al (15) described in detail The relationship between costal pain and fracture
the mechanism of vertebra-induced referred pain. morphology has not been previously reported. We
They explained that the referred pain was elicited believe that our classification of pain pattern may be
through the sympathetic nerve pathways and the pain useful in finding the pain sources from OVCFs, and
was radiated to the regions corresponding roughly hence facilitate in the pain management of these pa-
to the somatic distribution of the afferent fibers of tients. We are conducting a study of nonmidline pain in
the spinal nerve with which the afferent sympathetic lumbar osteoporotic fractures. They have similar pain
fibers entered the spinal canal. However, they did not characteristics. We are also conducting a prospective
explain the mechanism of costal pain in osteoporotic study to further confirm the reliability of this conclu-
thoracic vertebrae. sion. We believe that this study may further elucidate
Our results also indicate that costal pain is common the mechanism of nonmidline pain in osteoporotic
in patients with osteoporotic vertebral compression fractures of the spine.
References
1. Edidin AA, Ong KL, Lau E, Kurtz 5. Rad A, Kallmes D. Pain relief following 9. Niu J, Song D, Gan M, et al.
SM. Mortality risk for operated and vertebroplasty in patients with and Percutaneous kyphoplasty for the
nonoperated vertebral fracture patients without localizing tenderness on treatment of distal lumbosacral pain
in the medicare population. J Bone palpation. Am J Neuroradiol 2008; caused by osteoporotic thoracolumbar
Miner Res 2011; 26:1617-1626. 29:1622-1626. vertebral fracture. Acta Radiol 2018;
2. Itshayek E, Miller P, Barzilay Y, et 6. Yang YM, Ren ZW, Ma W, Jha RK. 59:1351-1357.
al. Vertebral augmentation in the Kyphoplasty for the treatment of pain 10. Patel U, Skingle S, Campbell GA,
treatment of vertebral compression distant to osteoporotic thoracolumbar Crisp AJ, Boyle IT. Clinical profile of
fractures: Review and new insights from compressive fractures. Cell Biochem acute vertebral compression fractures
recent studies. J Clin Neurosci 2012; Biophys 2014; 68:523-527. in osteoporosis. Br J Rheumatol 1991;
19:786-791. 7. Gibson J, Pilgram T, Gilula L. Response 30:418-421.
3. Syed MI, Shaikh A. Vertebroplasty: A of non-midline pain to percutaneous 11. Friedrich M, Gittler G, Pieler-Bruha E.
systematic approach. Pain Physician vertebroplasty. Am J Roentgenol 2006; Misleading history of pain location in
2007; 10:367-380. 187:869-872. 51 patients with osteoporotic vertebral
4. Gangi A, Guth S, Imbert JP, Marin 8. Doo T, Shin D, Kim H, et al. Clinical fractures. Eur Spine J 2006; 15:1797-1800.
H, Dietemann JL. Percutaneous relevance of pain patterns in 12. O’Connor RC, Andary MT, Russo RB,
vertebroplasty: Indications, technique, osteoporotic vertebral compression DeLano M. Thoracic radiculopathy. Phys
and results. Radiographics 2003; fractures. J Korean Med Sci 2008; Med Rehabil Clin N Am 2002; 13:623-644.
23:579-588. 23:1005-1010. 13. Wilson D, Owen S, Corkill R. Facet joint
www.painphysicianjournal.com E801Pain Physician: September/October 2021 24:E795-E802
injections as a means of reducing the patients. Korean J Spine 2012; 9:98-101. vertebroplasty, percutaneous
need for vertebroplasty in insufficiency 15. Jinkins JR, Whittemore AR, Bradley WG. kyphoplasty, nerve block, and
fractures of the spine. Eur Radiol 2011; The anatomic basis of vertebrogenic conservative treatment for nonsurgery
21:1772-1778. pain and the autonomic syndrome options of acute/subacute and chronic
14. Choi HJ, Yang HJ, Lee SH, Park SB. associated with lumbar disc extrusion. osteoporotic vertebral compression
The effect of vertebroplasty on costal AJR Am J Roentgenol 1989; 152:1277-1289. fractures (OVCFs) in short-term and
pain related to osteoporotic thoracic long-term effects. Medicine (Baltimore)
16. Zuo XH, Zhu XP, Bao HG, et al.
compression fractures in elderly 2018; 97:e11544.
Network meta-analysis of percutaneous
E802 www.painphysicianjournal.comYou can also read

















































