More Than Ticking A Box: LGBTIQA+ People With Disability Talking About Their Lives - Institute for Health Transformation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

More Than Ticking A Box:
LGBTIQA+ People With
Disability Talking About
Their Lives
Understanding experiences in Healthcare and
Community to Improve Services For All
Findings and Recommendations from a
Victorian Research Project
More than ticking a Box.indd 1 4/3/21 3:36 pm
More than ticking a Box.indd 2 4/3/21 3:36 pm

More Than Ticking A Box:
LGBTIQA+ People With Disability
Talking About Their Lives
Understanding Experiences in Healthcare and
Community to Improve Services For All
Findings and Recommendations from a Victorian Research Project
Project completed by:
Amie O’Shea, J. R. Latham, Sherrie Beaver, Jake Lewis,
Ruby Mountford, Mellem Rose, Anita Trezona, Patsie Frawley
More than ticking a Box.indd 1 4/3/21 3:36 pm
2 Foreword
This project came about at the initiative of Pride This project developed from a shared recognition
Foundation Australia whose philanthropic work of the limited research or policy knowledge that is
supports charitable activities that benefit LGBTIQA+ grounded in the everyday lives of LGBTIQA+ people
people and allied communities in Australia. As part with disability in Australia. As a small project, its
of their priority focus on LGBTIQA+ people with scope was limited to the state of Victoria as an
disability, Pride Foundation Australia formed an Australian case study. The Deakin University team
advisory committee of people with lived experience committed to an additional goal for the project –
and/or professional experience in the field to to include LGBTIQA+ people in meaningful ways
advise it on priority areas of need. Pride Foundation and, from this, to grow their capacity to engage
Australia accepted the advice that policy and with, and produce, research about the health and
practice needed to be informed by a better wellbeing of LGBTIQ+ people and people with
understanding of barriers for LGBTIQ+ people disability. This feature of the project reflects the
with disability in fully participating in Australian values of Pride Foundation Australia, and was
society. Informed by Inclusion Melbourne’s enthusiastically embraced and supported.
collaborations with Pride Foundation Australia and
Deakin University, the Disability & Inclusion team Suggested citation
at Deakin University was approached to co-create a
qualitative research project to explore these issues. O’Shea, A., Latham, J., Beaver, S., Lewis, J., Mountford,
R., Rose, M, Trezona, A., Frawley, P. (2020). More than
Ticking a Box: LGBTIQA+ People With Disability Talking
About Their Lives. Geelong: Deakin University.
More than ticking a Box.indd 2 4/3/21 3:36 pm
Table of Contents 3
Foreword 2
Acknowledgements 4
A note on terminology and our approach 4
LGBTIQA+ sexuality and gender identity 4
Disability 4
An intersectional approach 5
1. Background 6
1.1 Health status and inequities 6
1.2 Experiences of discrimination, violence and abuse 7
1.3 Inclusion and exclusion within communities 8
1.4 Access and engagementwith services 9
1.5 National disability service system 10
1.6 National policy context and implications 11
RECOMMENDATIONS 13
2. Methodology 15
2.1 The research team 15
2.2 Study participants 17
2.3 Data collection 17
2.4 Data analysis 18
RECOMMENDATIONS 20
3. Findings 22
3.1 Managing multiple identities 22
3.1 Community 25
3.1 Accessing Services 28
3.1 The National Disability Insurance Scheme (NDIS) 33
4. Discussion 36
4.1 Visibility 36
4.2 Multiple identities 36
4.3 Understanding access and accessibility 37
RECOMMENDATIONS 39
4.4 Summary 40
4.5 Limitations 40
RECOMMENDATIONS 41
4.6 Peer Researcher reflections 42
5. Recommendations 44
References 48
More than ticking a Box.indd 3 4/3/21 3:36 pm
4 Acknowledgements LGBTIQA+ sexuality
We acknowledge the collaboration and expertise and gender identity
provided by all those involved with the project,
The acronym LGBTIQA+ stands for lesbian, gay,
including the Research Advisory Group of Cameron
bisexual, transgender (or trans), intersex, queer/
Bloom, Nathan Despott, Ian Gould, Ki Hayward,
questioning, asexual, HIV positive and other terms
Ruth McNair, Amielle Penny and Alastair Stewart.
(such as non-binary and pansexual) that people use
We would especially like to thank the LGBTIQA+
to describe or express their sex, gender, sexuality,
people with disability who shared their experiences
and relationships. Intersex people are born with
with us by participating in focus groups for this
physical sex characteristics that don’t fit medical
project.
norms for female or male bodies (Intersex Human
Rights Australia, 2020). The term ‘queer’ is often
The project was funded by a consortium of
used as an umbrella term to refer to sexually and
interested parties led by Pride Foundation Australia,
gender diverse people and communities. Although
which also includes Snow Foundation, Broadtree
historically used as a pejorative, LGBTIQA+ people
Foundation and the Victorian Government.
have reclaimed the term as an expression of
resistance, solidarity and sense of belonging to
We recognise the Traditional Owners of the
a broad community (Drummond & Brotman,
Aboriginal lands on which this research took place:
2014). As with many terms used to describe
the Wurundjeri, Boon Wurrung, Wadawurrung,
identity, the language used to describe sexual and
Taungurong, and Dja Dja Wurrung people of the
gender diversity is constantly changing. Sexual
Kulin Nation. We pay our respects to the past,
and gender identities are complex, dynamic and
present and future Elders and acknowledge that
constantly evolving and, as we address in this
Indigenous sovereignty has never been ceded.
report, situationally particular in response to
external factors (e.g., see Latham, 2017b). There
is no one preferred term used by all sexually and
A note on terminology gender diverse people; people often have multiple,
overlapping identities, and many people and
and our approach communities also have unique ways of describing
their identities, histories and experiences (National
All research is underpinned by a set of beliefs about LGBTI Health Alliance, 2016). We did not ask
its topic. In the sometimes contested and culturally participants which identity category or categories
specific case of sexuality, gender identity and best describes their experience of sexual and
disability, it is particularly important to clarify how gender identity.
we have understood and used these concepts.
Disability
Definitions of disability vary across contexts and
are influenced by various cultural and political
perspectives. A medical model of disability
frames disability in relation to the individual
and focuses primarily on bodily impairment
and medical conditions (Mckenzie & Macleod,
2012), an approach that also informs how people
with intersex variations are understood. We
More than ticking a Box.indd 4 4/3/21 3:36 pm
acknowledge the work of both disability and An intersectional approach 5
intersex advocates in challenging the pathologising
effects of the medical model (see for example To understand the lives and experiences of
Carpenter, 2018; Oliver, 1995), which tends to see LGBTIQA+ people with disability we were informed
disability as a problem to be fixed. In comparison, by the work of American legal scholar Kimberlé
a social model of disability recognises that a Crenshaw’s theory of intersectionality (Crenshaw,
range of social factors impact on how disability is 1990). An intersectional approach means examining
experienced, and focuses instead on how attitudes, the experiences of minority groups as facing
practices and structures within society lead to multiple and overlapping oppression (Crenshaw,
oppression and exclusion of people with disability 1990). Critical disability scholars have found this
(Oliver, 1990). In this sense, the social model of work effective, as Dan Goodley (2017) writes,
disability places responsibility for access, equity because “A body or mind that is disabled is also
and inclusion, not on the individual, but on how defined by race, gender, trans/national location,
broader social structures are set up in ways that age, sexuality, religion and class … Intersectionality
limit access to people with disability. is about not simply bringing together these
markers and the theoretical responses but also
The United Nations Convention on the Rights considering how each supports the constitution of
of Persons with Disabilities (CRPD) provides an one another” (p. 44). An intersectional approach
international human rights framework for the has also been used in LGBTIQA+ research, including
protection of the fundamental rights and freedoms older LGBT people (Westwood, 2019), mental
of people with disability. It is underpinned by a health for LGBT people (Ruth, 2017) and LGBT
bio-psycho-social perspective of disability (World people of colour (Ramirez et al., 2018).
Health Organization, 2002) which recognises
disability as a multidimensional and evolving
concept. In this view, disability occurs resulting
from the interaction between people with
impairments and attitudinal and environmental
contexts that restrict their full and equal
participation in society (United Nations, 2006).
This is similar to sociologist Tom Shakespeare’s
interactional model (Shakespeare, 2006;
Shakespeare, 2013) which understands disability
as a complex and dynamic interaction between the
“they want us to
tick a tick box,
individual and their environment.
Bio-psycho-social and interactional models of
disability are clear that “people with disability”
are not one homogenous group, and experiences
of disability are different for everyone (Goodley,
but we want to
2017). Throughout this report, reference to
disability includes physical, cognitive, psycho- slide a slider”
social, sensory, and/or forms of neurodiversity.
We recognise that disability may be episodic or
consistent, acquired or congenital, single or plural.
We did not ask participants to report the details of
their disability.
More than ticking a Box.indd 5 4/3/21 3:36 pm
6 1. Background There has been increasing recognition of the
The purpose of this project was to explore the importance of including people, particularly
experiences of LGBTIQA+ people with disability in members of marginalised groups, in research. In
Victoria, Australia1, especially in relation to: LGBTIQA+ communities, we recall the work of
Î Accessing health and social services queer people in community-based HIV/AIDS and
other health promotion work (Dowsett et al., 2001).
Î Connecting with LGBTIQA+ and disability
The practices of inclusive research led by academics
identities and communities
working with people with intellectual disability
In doing so the project aimed to also identify and form another backdrop to this project (Johnson
propose recommendations for improvements to & Walmsley, 2003). In this research, we draw on
ensure services are more inclusive and responsive both histories and a cumulative and deepening
to the contemporary needs of LGBTIQA+ people understanding of meaningful and authentic
with disability. research participation in sexuality research with
LGBTIQA+ people and people with disability
Historical oppression and social inequalities are key (Frawley & O’Shea, 2020; O’Shea & Frawley, 2020).
factors influencing the experiences and lowered
health outcomes of both LGBTIQA+ people and
people with disability. For LGBTIQA+ people 1.1 Health status and inequities
with disability, experiences of discrimination
and oppression are compounded by multiple People with disability are more likely to have
social identities, leading to multiple minority poorer overall physical and mental health than
stress (McConnell et al., 2018). ‘Minority stress’ people without disability (Dispenza et al., 2016),
refers to how marginalised groups experience while people with intellectual disability have
stress that arises from experiences of stigma and lower life expectancy
discrimination, which leads to increased negative and higher rates of
People with intellectual disability have
physical and mental health and social wellbeing avoidable deaths
2x
outcomes (Correro & Nielson, 2020). at over twice
the rate of the
An intersectional perspective is therefore critical general population
to understanding the way multiple social identities
the rate
(Reppermund et
and discriminatory processes and systems interact al., 2020; Trollor et of avoidable deaths than
to shape the lived experiences of LGBTIQA+ al., 2017). Research the general popula on
people with disability, their health and wellbeing, has also shown that
and access to services, community and support. lesbian, gay and bisexual people have increased
The project approached this intersection at the likelihood of disability, poor mental health, and
collective levels of disability and LGBTIQA+ because substance use than their counterparts (Fredriksen-
this is where most policy and service provision is Goldsen et al., 2013). Further research on LGBTI
positioned. However we also acknowledge, and ageing demonstrates the cumulative effects of
within the scope available have made attempts this marginalisation over the life course, as older
to avoid, assumptions of homogeneity or LGBTI people have higher rates of disability,
generalisation, while also leaving space for more depression, anxiety and loneliness than the general
intersecting experiences of marginalisation. community, as well as less social support (Crameri
1 We have prioritised Australian literature and service contexts wherever possible, although there is by necessity some
extrapolation of comparable international data.
More than ticking a Box.indd 6 4/3/21 3:36 pm
22.7% LGBT people WITH DISABILITY have
TWICE the rates of ANXIETY
of LGBT respondents reported
and PSYCHOLOGICAL DISTRESS
a DISABILITY or long-term
than LGBT people without
HEALTH CONDITION
et al., 2015). People with intersex variations 7
may be coerced into medical interventions to
normalise sex characteristics in ways that do
harm, especially in regards to sexuality and sexual
health (Latham & Holmes, 2018). The effects of
iatrogenic trauma and ongoing stigma related to
Î 22.7% of LGBT respondents reported a
intersex sex characteristics also produce poorer
disability or long-term health condition
health outcomes for people with intersex variations
(Carpenter, 2018). For trans and gender diverse Î Females were more likely than males to report
people, the classification of their experiences as having a disability or long-term illness
a mental disorder (‘Gender Dysphoria’) can also Î LGBT people with disability were more likely
produce an antagonistic relationship with medical to have poor self-rated health
professionals, and a reluctance to access health and Î LGBT people with disability reported higher
other social services (Latham, 2017a). levels of psychological distress than those
without
Mental health is an important element of overall Î LGBT people with disability have twice the
health and wellbeing. A recent report by the more likely to
rates ofexperience
anxiety andviolence
psychological distress
National LGBTI Health Alliance (2020) on the mental than LGBT people without
health of LGBTIQA+ people showed that compared
Î Rates ofLGBTIQ+
anxiety and psychological distress
to the general population, LGBTIQA+ people are people with
were considerably
disability higher for trans people
more likely to:
(Leonard et al., 2012)
Î Have thoughts of suicide people
with disability
Î Attempt suicide in their lifetime
1.2 Experiences of discrimination,
Î Have engaged in self-harm in their lifetime general
violence
populaand
on abuse
Î Experience and be diagnosed with depression
ve
22.7%
and anxiety Experiences of discrimination, violence and
LGBT people WITH DISABILITY have
Î Experience psychological distress abuse have a significant impact
TWICE onthe
therates
health and
of ANXIETY
27%
As most national datasets
of LGBT respondents reported
a DISABILITY or long-term
ofdotrans
HEALTH and
notCONDITION
collect
wellbeing of LGBTIQA+ peopleand and
disability. People with disability
people with DISTRESS
PSYCHOLOGICAL
than LGBT people
are more without
likely to
gender diverse experience violence and discrimination than people
in information on diverse sexual and gender identities,
respondents without disabilities (Frawley et al., 2015), and the
ed the available data on the health status of LGBTIQA+
stated that they incidence among LGBTIQ+ people with disability
LLY people with disability is severely limited. The
AVOID RELIGIOUS is recognised to be even higher, despite issues of
Y influential Private Lives 2:INSTITUTIONS
The second national
under-reporting (Leonard & Mann, 2018).
survey of the health and wellbeing of gay, lesbian,
bisexual and transgender (GLBT) Australians
The risks of violence, including family/domestic
dueincludes
(Leonard et al., 2012) to actualsome information
violence and sexual violence are higher for women
and/or poten
on people with disability. The most al recent report
EXPERIENCES OF with disability (Disabled People’s Organisations
details that:
DISCRIMINATION Australia, 2017). LGBTIQA+ people with disability
may also be at increased risk of abuse from carers
22.7% and support workers. LGBT
For people WITH
example, oneDISABILITY
third of have
TWICE the rates of ANXIETY
participants in a UK study reported experiences of
of LGBT respondents reported
and PSYCHOLOGICAL DISTRESS
a DISABILITY or long-term discrimination or poor treatment by their personal
than LGBT people without
HEALTH CONDITION assistant or care workers because of their sexual
more likely to
experience violence
LGBTIQ+
people with
disability
More than ticking a Box.indd 7 4/3/21 3:36 pm
than LGBT people without
8 orientation or gender identity(Abbott, 2017). Convention are weakened. It was not until General
Some participants also reported experiences of Comments 6 and 7 that sexual orientation, gender
verbal, physical and sexual abuse by their personal identity and sex characteristics were specifically
assistants or care workers (Abbott, 2017). written into the interpretive architecture around
the Convention (United Nations, 2020).
more likely to
experience violence
1.3 Inclusion and exclusion within
LGBTIQ+
people with communities
disability
LGBTIQA+ people and people with disabilities
people
with disability experience higher levels of social exclusion across
a range of settings, including schools, workplaces,
general social events, general community settings, and
popula on healthcare (Frawley et al., 2015; Social Inclusion
Unit Department of the Prime Minister and
Cabinet, 2009; United Nations, 2016; Waling et al.,
In addition to broad societal discrimination, 2019).
LGBTIQA+ people with disability may also
experience discrimination from within Social support and networks have been shown to
the LGBTIQA+ and disability communities, be protective factors against poor general health,
compounding their sense of social marginality and disability and depression among lesbian, gay
isolation (Abbott, 2017; Leonard & Mann, 2018). and bisexual people (Fredriksen-Goldsen et al.,
Discrimination also leads to internalized stigma 2012) However, LGBTIQA+ people with disability
and victimisation, which have been shown to be experience marginalisation and exclusion within
predictors of disability and depression among both queer and disability communities (Dispenza
queer people (Fredriksen-Goldsen et al., 2012). et al., 2016; Leonard & Mann, 2018; Vaughn et
al., 2015) and therefore report experiencing lower
The rights of people with disability were elucidated social support from, and connection with both
in the United Nations Convention on the Rights of communities (Leonard & Mann, 2018).
Persons with Disabilities (United Nations, 2006)
which was ratified by Australia on 3 May 2008. People with intellectual disability are a group often
However, while it codifies the right to form a left out of wider disability advocacy and research.
family (Article 23), rights for women with disability, We draw on the early results of a consultation
and refers to the right to sexual health education with members of Rainbow Rights, the self-
and reproductive health care (Article 25), the advocacy organization of LGBTIQA+ people with
Convention fails to explicitly refer to sexuality, intellectual disability in Victoria (Rainbow Rights,
gender identity or intersex status (Jaramillo Ruiz, 2020). LGBTIQA+ people with intellectual disability
2017; Schaaf, 2011; Shah, 2017). This is an omission described a number of barriers to inclusion
which itself tells of the contentious nature of including lack of access to health services, negative
sexuality in people’s lives and which leaves holes in (ableist, homophobic or heterosexist) attitudes of
the opportunities for people with disability to have health professionals, income inequality and under
their sexual rights acknowledged and supported diagnosis of mental illness. They call for social,
(Frawley & O’Shea, 2019). Without support for economic, political and civic inclusion for LGBTIQA+
the right to be sexual, other rights codified in the people with intellectual disability, describing it as:
More than ticking a Box.indd 8 4/3/21 3:36 pm“everyone being able to
le with intellectual disability have
participate fully in social,
34.6% 9
22.7% of LGBTIQA+ par cipants in
2x
LGBT people WITH D
economic, political and civic life; a Victorian survey reported TWICE the rates of A
of LGBT respondents reported
OCCASIONALLY OR USUALLY
by getting a good education, a DISABILITY or long-termHIDING THEIR SEXUALITY
and PSYCHOLOGICA
receiving an adequate income, than LGBT people w
the rate HEALTH CONDITION OR GENDER IDENTITY
having a job, being politically when accessing services
of avoidable deaths than
the general popula on aware and being connected to
family, friends, the LGBTIQ+ and One study showed that 34.6 per cent of LGBTIQA+
mainstream community” participants in a Victorian survey reported
occasionally or usually hiding their sexuality or
(Rainbow Rights, 2020 p.3) gender identity when accessing services (Leonard
et al., 2008). For example current religious
In the recent consultation conducted by The Social exemptions give some religious private schools
Deck to inform the next national disability plan, in Australia “permission to discriminate against
LGBTIQA+ participants reported that being LGBTIQ+ transgender and gender diverse students” (Smith
and having a disability increases experiences of et al., 2014 p.49). In the same study, 27% of trans
discrimination, and that people were not always and gender diverse respondents stated that they
accepted in one group or the other. They also avoid religious institutions due to actual and/or
highlighted the cross impacts for people who potential experiences of discrimination. The current
identify as LGBTIQA+ with disability, and additional Religious Freedom Bills2 propose unprecedented
barriers to being included and feeling a sense of protection of the religious beliefs of some, over
more likely to
belonging (The Social Deck, 2019). those of others including those of no faith. This is of experience v
significant concern to both LGBTIQA+ and disability
communities, for example section 41 of the LGBTIQ+
people with
1.4 Access and engagement Religious Discrimination Bill, which would “allow
disability
with services people who wish to express prejudiced, harmful
or dangerous views about women, people with people
A number of systemic barriers impact on access disabilities, LGBTQI+ people and others” (Equality with disabilit
to and utilisation of services by LGBTIQA+ people Australia, 2019 p.2). general
with disability, including the discriminatory popula on
and stigmatising attitudes held by professionals
working in the health, social and disability sectors
(Leonard et al., 2012; Mulé et al., 2009) Similarly,
professionals often lack the knowledge, skills and
34.6%
confidence to deliver inclusive and responsive
27% of trans and
services of
to LGBTIQA+
LGBTIQA+ parpeople with in
disability, and are gender diverse
cipants
not provided with adequate training, resources and respondents
a Victorian survey reported
stated that they
other supports to improve
OCCASIONALLY ORtheir practice (Leonard &
USUALLY
AVOID RELIGIOUS
HIDING
Mann, 2018). THEIR SEXUALITY
INSTITUTIONS
OR GENDER IDENTITY
when accessing services
due to actual
2 Religious Discrimination Bill 2019, Religious Discrimina- and/or poten al
tion (Consequential Amendments) Bill 2019, Human Rights EXPERIENCES OF
Legislation Amendment (Freedom of Religion) Bill 2019
DISCRIMINATION
More than ticking a Box.indd 9 4/3/21 3:36 pm10 There is a lack of understanding among health 1.5 National disability service
professionals and disability services regarding system
the LGBTIQA+ community, which appears to be
a particular issue in regional and rural areas, and Issues of sexuality and relationships are largely
some faith based institutions (Barrett et al., 2015; medicalised and otherwise overlooked in health-
Leonard et al., 2012). The consultation report based disability services such as acquired brain
also noted the need to better understand the injury or rehabilitation (O’Shea et al., 2020). We
experiences LGBTIQ+ people with disability and the focus here on the National Disability Insurance
way policy decisions impact on them (The Social Scheme (NDIS) as the primary locus for disability
Deck, 2019). services and supports.
The most recent Private Lives Survey (Leonard et In 2011 the Productivity Commission conducted a
al., 2012) found that compared to LGBTIQA+ people national enquiry into the National Disability Long-
without disability, LGBTIQA+ people with disability term Care and Support Scheme, which found that
were: the disability support system was under funded,
Î Less likely to have private health insurance fragmented and inefficient, that services were not
Î More likely to have a regular GP, and to see being provided equitably, and that it was failing to
them more often meet the needs of many people with disabilities and
their families (Productivity Commission, 2011). A key
Î More likely to see a counsellor, psychologist or
recommendation of the report was the introduction
social worker
of a national insurance scheme that provides funding
Î More likely to access psychiatric services for long-term high quality care and support for all
Î Slightly less likely to have pap or mammogram people with significant disabilities.
screening
Î Less likely to have ever had a HIV test The NDIS was first introduced in Australia with the
passing of the National Disability Insurance Scheme
An earlier report on the service access experiences
Act (2013) and the subsequent establishment of
of LGBTIQA+ people with disability described how:
the National Disability Insurance Agency (NDIA)
Î LGBTIQA+ people with disability experience (National Disability Insurance Agency, 2020b). The
exclusion from mainstream disability services purpose of the NDIS is to support the independence
Î Trans and gender diverse people with and social and economic participation of people
disability experience greater discrimination with disability, and empower them to exercise
when accessing services than other LGBQ choice and control over their support needs and
people with disability goals (Department of Health and Human Services,
Î LGBTIQA+ people with disabilities from 2018).
culturally diverse backgrounds experience
multiple and intersecting forms of Rollout of the NDIS commenced in 2016, with
discrimination and barriers to accessing nearly 380,000 people currently accessing the
services (Mann et al., 2006). This is NDIS, including nearly 84,000 people living in
particularly significant given that the 2016 Victoria (National Disability Insurance Agency,
Census identifies that 49.1% of Victorians, 2020a). Within the next five years it is expected
or one of their parents, were born outside the NDIS will provide $22 billion per year to an
Australia (Australian Bureau of Statistics, estimated half a million people with ‘permanent
2017). and significant’ disabilities (Department of Health
and Human Services, 2018).
More than ticking a Box.indd 10 4/3/21 3:36 pmPeople with
Theintellectual
NDIA doesdisability havecollect data that
not currently together’ project that developed a peer support 11
22.7%
2x
supports monitoring of LGBTIQA+ demographics. approach, training and a toolkit resource to develop LGBT
While data is collected on participants’ “sex”, capacity in the NDIS respondents
workforce. Further current TWIC
of LGBT reported
and P
information is not collected regarding gender NDIS research grants identify
a DISABILITY LGBTIQA+ people
or long-term
than L
theidentity
rate or sexuality, meaning that the number of HEALTH
with a disability as a CONDITION
core cohort for funding for
LGBTIQA+ people accessing the NDIS is not known. community capacity building. The absence of an
of avoidable deaths than
overall plan to guide work and to clearly articulate
the general popula on
Î In late 2019 a review of the NDIS legislation a commitment to addressing the specific needs of
examined participants’ experiences of the LGBTIQA+ people with disability is a current issue
NDIS and opportunities to improve systems for the sector.
and processes. Specifically, it focused on
the legislative changes required to improve
participants’ experiences with the NDIS,
rather than the broader range of operational
and implementation issues (Tune, 2019).
In relation to LGBTIQA+ people with disabilities,
the review recommended that any amendment
to the legislation should include amendments to
the principles of the NDIS Act to acknowledge
1.6 National policy context and
the unique experiences of women and LGBTIQA+
implications
people with disability, as agreed previously by
Current policy and practice guidelines on disability
Council of Australian Governments (COAG) in 2016.
care and support in Australia do not adequately
The review also set out the proposed elements
acknowledge the unique experiences of LGBTIQA+
of a Participant Service Guarantee, which is to be
people with disabilities, or outline actions and
legislated through NDIS rules in July 2020. ‘Respect’
strategies to address specific support and care
was identified as one of six key engagement
needs.
principles of the Guarantee, which includes a
commitment to ensuring staff have a high level
The National Disability Strategy (“the Strategy”)
of training in diversity, including on practices for
was developed in partnership between the
working with LGBTIQA+ people (Tune, 2019).
Commonwealth, State and Territory Governments
through the Council of Australian Governments.
Despite acknowledging that experiences of
The Strategy set out a ten-year plan for improving
discrimination and social exclusion are significant
34.6%
barriers to people accessing and navigating the
NDIS, LGBTIQA+ people have not been identified
27%
the lives of people with disability, their families
and carers, by guiding activities across mainstream
of trans and
gender
and disability specific areas of public diverse
policy,
as a priority community of for
LGBTIQA+ par
assertive cipants in
outreach respondents
and driving improvements in performance
or enhanced access support (Tune, 2019).reported
a Victorian survey Other stated that they
OCCASIONALLY OR USUALLY and outcomes for people with disability
marginalised communities are represented in such AVOID RELIGIOUS
HIDING THEIR SEXUALITY (Commonwealth of Australia, 2011).
strategies, including Cultural and Linguistically INSTITUTIONS
OR GENDER IDENTITY
Diverse people, and inwhen
the Rural and Remote,
accessing servicesand Although the Strategy acknowledges that a range
Aboriginal and Torres Strait Islander Strategies
of personal characteristics,due
including gender and
to actual
(National Disability Insurance Agency, 2020c).
sexuality, intersect with disability
and/or poten alpeople’s
to shape
Some research has been undertaken to inform
EXPERIENCES
needs, priorities and perspectives, OFsensitive
it is not
approaches to workforce needs including the ‘Out DISCRIMINATION
to these factors. Instead, the Strategy adopts a
More than ticking a Box.indd 11 4/3/21 3:36 pm12 universal approach to its policy directions, goals Furthermore, despite references to LGBTIQA+
and intended outcomes. In a recent review of and the sexual/gender rights of people with
the implementation of the Strategy, meeting the disability across a range of regulatory frameworks
specific needs of diverse groups was identified as a and laws (including equal opportunity and anti-
key gap and priority for future policy development discrimination legislation, NDIS Practice Standards,
and implementation (Davy et al., 2018). The review Disability services legislation, and the Victorian
also emphasised the importance of ensuring that Charter of Human Rights and Responsibilities),
representatives from diverse groups are involved in there are no intersectional statements that
all aspects of policy design and implementation. combine LGBTIQA+ and disability in any of these
frameworks or laws. In particular, there are no
While policy statements acknowledging the clauses that specifically require the application of
unique experiences of LGBTIQA+ people with such rights and practice to people with intellectual
disability have symbolic importance and may disability, a population often quietly excused from
increase their visibility among service providers domains such as the expression of sexuality and
and the broader community, clear policy actions gender due to underlying assumptions about
and practice guidelines are required to ensure capacity.
services are inclusive of and responsive to the
needs of LGBTIQA+ people with disability. The NDIS The Victorian State Disability Plan (2017) included
Quality and Safeguards Commission is responsible detailed action points specific to LGBTIQ people.
for registration and regulation of NDIS service Although such Plans are not formal regulatory
providers. Independent third party auditing and frameworks, this resulted in specific grant funding
certification are conducted using the new NDIS targeting LGBTI projects, and encouraged LGBTI
Practice Standards, representing an important inclusive practice in services. The Plan is currently
element in monitoring and assuring LGBTIQA+ under review, the consultation paper for which
inclusive practice. While a number of the standards acknowledges that people with disability may often
are relevant and applicable to LGBTIQA+ people experience less control over their intimate lives
with disability there is a lack of meaningful (Department of Health and Human Services, 2017).
reference to their rights. However, in light of Clearly, persistent advocacy has been effective
repeated references to diverse characteristics such but is required to retain this focus and to develop
as age, cultural background, religious background, specific guidelines, indicators and directives.
and abilities in the Practice Standards, there
is a conspicuous lack of specific reference to The development of the next National Disability
‘LGBTIQA+’, ‘queer’, ‘sexual orientation’, ‘gender Strategy, and ongoing reforms under the NDIS
identity’ or ‘intersex status’ in any of the NDIS present significant opportunities to prioritise the
Practice Standards and supportive guidelines. needs of LGBTIQA+ people with disabilities in public
Requiring Approved Quality Auditors (AQA) to policy. Policy responses should be co-designed
infer or elucidate such considerations rather with LGBTIQA+ people with disabilities, and should
than providing explicit reference and indicators specify actions that address service delivery needs/
means that the capacity of the scheme to effect priorities, effective communication and information
and drive change is limited (N.Despott, personal provision, increasing the competence/capability
communication, June 22, 2020). As of early 2020, of the workforce, and improving data collection,
the mandated training course for AQAs includes no monitoring and evaluation.
references to LGBTIQA+ people.
More than ticking a Box.indd 12 4/3/21 3:36 pm13
RECOMMENDATIONS
The following recommendations are suggested in order to address gaps in the inclusion of
LGBTIQA+ people with disability in a range of community settings.
1. Publicly funded services should be required to create and make public their statements and
plans for equal access for LGBTIQA+ people with disability, supported with relevant academic
research
2. LGBTIQA+ people with disability should be acknowledged as a priority community for
focussed outreach or enhanced access support within the NDIS. This may occur within the
NDIS and through funding advocacy services.
3. An opportunity to discuss and review the NDIS LGBTIQA+ Strategy should be arranged at
local or state government levels as a matter of priority. This could be trialled within one
region to determine how to best ensure access and cultural safety
4. Create state-based working groups with the assistance of experienced practitioners on
LGBTIQA+ people with disability, to bring together health service providers, LGBTIQA+
organisations, disability services and LGBTIQA+ people with disability to learn from each and
share ideas on inclusive practice. The work of LGBTIQA+ people with disability within these
groups should be appropriately recognised and remunerated. These groups will:
4.1 Establish clear channels for policy reform across all levels of government
4.2 Create connection and peer development for LGBTIQA+ people with disability
4.3 Advise services and departments on inclusive practices for LGBTIQA+ people with
disability
4.4 Promote opportunities in collaborative research development, including grant funding
support
4.5 Organise workshops, seminars and other events to develop ideas and share resources
more broadly
5. Further research by tertiary institutions and independent research bodies into the
experiences of people with disability and LGBTIQA+ people committed to developing the
research capacity of LGBTIQA+ people with disability as an integral part of these research
projects
6. Any funded project connected to disability or LGBTIQA+ topics should expressly aim to
include LGBTIQA+ participants, and report against this outcome
More than ticking a Box.indd 13 4/3/21 3:36 pmMore than ticking a Box.indd 14 4/3/21 3:36 pm
2. Methodology of social structures and subverts power dynamics
within traditional research (Carmack, 2018; Owen &
15
An overarching commitment to developing and Friedman, 2017).
using an inclusive research approach guided the
methods of this project. Inclusive research is guided Strong feedback loops to the research environment
by an evolving set of practices which encompass were built into the project ensuring findings were
a range of approaches and methods (Nind, 2014). being co-developed and used to inform subsequent
The significant element of inclusive research is action research cycles of the overall project. Deakin
that people who were traditionally considered University Human Research Ethics Committee
the objects of research are instead active in roles provided approval for the project (2019-207).
including the instigation of ideas, and the collection
and analysis of data. From the outset, this
project centred LGBTIQA+ people with disabilities 2.1 The research team
in a number of roles, not simply as research
participants, but as members of the Research This research project was conducted by a team
Advisory Group, as peer researchers,3 and through comprised of academic researchers and peer
attempts toward meaningful opportunities for researchers employed by Deakin University. The
participants to access and engage in data collection, academic research team was led by Dr Amie O’Shea
analysis and the project’s outputs. with Dr J. R. Latham and Associate Professor
Patsie Frawley, and additional research assistance
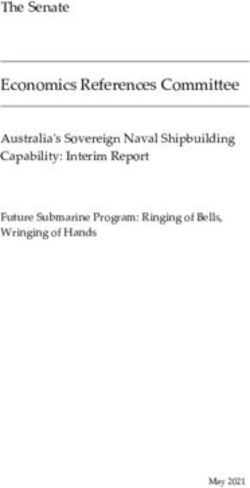
Academic work reflecting on the development of from Dr Anita Trezona. The peer researchers on
inclusive research has recognised the importance the team were Sherrie Beaver, Jake Lewis, Ruby
of making its practices available for critical scrutiny Mountford and Mellem Rose. The team was formed
(Johnson & Walmsley, 2003; O’Shea, 2016), hence to reach across a breadth of lived and professional
we present these in detail within this report. experiences, genders, sexualities and research
knowledges.
Drawing on Participatory Action Research (PAR)
methodologies, the research aimed to take an Peer researchers brought their leadership,
iterative and action-focussed approach across the creativity, experiences and connections with
project planning, research (data collection, analysis) diverse communities across gender, sexual identity,
and outcomes being undertaken iteratively. advocacy,4 and various experiences of disability.
Like inclusive research, PAR represents a range Academic researchers brought their knowledge
of theoretical orientations and methods that and experience of university bureaucracies,
“promote pluralism and creativity in the art of research methods, human research ethics, and
discovering the world and making it better at the a commitment to building the capacity of peer
same time” (Chevalier & Buckles, 2019 p. 3). PAR researchers to ensure the ‘nothing about us
aims to effect change within queer and disability without us’ dictum of inclusive disability research
research, as it promotes self-advocacy, facilitates a was practiced in this project. This report was led
critical-consciousness raising, encourages analysis by the academic researchers with input from the
3 We use the term ‘peer researchers’ to describe LGBTIQA+ people with disability to capture the significance of shared
experience. Other commonly used terms include ‘community researcher’ or ‘co-researcher’.
4 We acknowledge advocacy work comes from funded disability advocacy organisations, self-advocacy (a term in the ac-
ademic literature often referring to advocacy when performed by people with intellectual disability in particular), and the indi-
vidual advocacy that people engage in which is often not funded, but comes as part of engaging with services and systems
which construct them
More than ticking a Box.indd 15 4/3/21 3:36 pm16
Research Paper
Creavity
Experiences in
community Knowledge of
Connecons with university systems
community
Human
Gender research ethics
Sexual identy
Research methods
Advocacy
Experience of disability
Leadership Building capacity to work
further in research
Peer Researchers Academic Researchers
whole research team and Research Advisory Group. participant recruitment, which involved the
Reflections by the peer researchers on this project design of written information and the creation of
can be found at 4.6 of this report. information in Auslan as well as its subsequent
circulation online and through established
The academic researchers were committed to the networks. The peer researchers worked in pairs
peer researcher project, in part with the knowledge to plan focus groups: identifying the location,
that inclusion and opportunities created during this venue, date and time, catering and in deciding if/
project have the potential to feed directly back into when they would like support from the academic
communities. In order to recognise the strengths researchers during the focus group. In order
and contributions of each team member, we spent to ensure the research complied with Human
time getting to know each other and hearing about Research Ethics, the academic researchers
our work in the shared spaces of LGBTIQA+ and managed the consent process and operating digital
disability advocacy, community organising, activism voice recorders used for producing transcripts of
and research. We became familiar with the way that the focus groups. Peer researchers also advised on
professional-personal boundaries are dismantled by access needs including the provision of suitable
holding multiple forms of knowledge as valued, and Auslan-English interpreters, accessible venues,
asked questions of each other to understand our establishing focus group guidelines, making
different perspectives and areas of expertise. available a ‘quiet room’ for if/when participants
In practice this meant that elements of the research needed a break, and the use of a ‘talking stick’ to
method were led by different members of the ensure all participants were able to contribute.
research team. The focus groups were run by peer
researchers with academic researchers present for During data collection, peer researchers facilitated
support if needed. Writing this report was led by the focus groups in pairs, with the exception of one
the academic team with consultation and feedback Deaf5 focus group, which was facilitated in Auslan
from the peer researchers and the Project Advisory by one peer researcher. In all cases, members of
Group. the academic research team attended the focus
Key tasks of the peer researchers included group to provide support as needed. In recognition
5 We follow the convention of capitalised Deaf when referring to people who identify as members of a cultural and linguistic
minority, who use Auslan Ladd, P. (2003). Understanding deaf culture: In search of deafhood. Multilingual Matters.
More than ticking a Box.indd 16 4/3/21 3:36 pmof peer researchers’ dual role within the research Group of focus areas and possible recruitment 17
team and their identification with the participant opportunities.
group, opportunities to debrief were prioritised.
Peer researchers participated in a short debrief 2.3 Data collection
with academic researchers immediately after the
evah ytilibasid lautcelletni htiw elpoeP
%7.22
focus group, and a more detailed debrief 2-4 days Data collection was conducted through four focus
x2
after each focus group, to reflect on the issues groups conducted by the peer researchers. Two
detropconcerns
raised, share er stnednasopthey
ser Tarose,
BGL foand access
focus groups were held in the Melbourne and
mret-gnol ro YTILIBASID a
support in solidarity. one in Bendigo, which were conducted in spoken
NOITIDNOC HTLAEH etar eht
English. Peer researchers identified the location for
Peer researchers also attended the Research focus groups with an eye to cultural
naht shand
taecommunity
d elbadiova fo
Advisory Group meetings, to present their work n o a l u p
familiarity, using venues provided by the Cityo p larof
eneg eht
and to hear reflections and feedback from the Melbourne’s Multicultural Hub, Thorne Harbour
group. Several significant elements of the project Health and Expression Australia.6
came from these discussions, including the
idea of a Deaf focus group in Auslan, and the One focus group was conducted in Auslan by
production of the final report in easy language. Sherrie Beaver and Amie O’Shea in recognition of
Below we detail the peer researchers’ roles in the recruitment connection to the Deaf community
data collection and analysis. In particular, the made possible by peer researcher Sherrie Beaver
development of guidelines for the focus groups by and academic researcher Amie O’Shea (a fluent
the peer researchers was critical to this project’s Auslan user and interpreter). Drawing on the
methodology, as well as its success in recruitment. creativity and flexibility afforded within an inclusive
PAR methodology, Sherrie and Amie worked
together to plan this focus group. All other focus
groups invited people with any experience of
disability, and while we do not differentiate the
data analysis on disability type, we note here that
this included people who identified with various
sensory, physical, intellectual disability as well as
neurodiversity, acquired brain injury and complex
communication needs. We actively resisted any
perceived hierarchy of disability, or privileging of
2.2 Study participants cognition and sought to consider all perspectives
and contributions as equally valued. We did not ask
Research participants were people aged 18 years or participants to outline their experience of disability,
over who self-identified as LGBTIQA+ people with or their identification within LGBTIQA+. The main
disability. In line with the definitions given earlier reason we made this decision was political: we
%72
in the report, there were no additional or more
specific eligibility criteria. There were 29 people
dna snart fo
who participated in focus groups for this project,
know that people with disability are often required
%6.43
to explain their disability and its effects, to their
own detriment, and that people who identify
esrevid redneg
recruited online and through personal networks of ni stnathe
within pic acronym
rap +AQILGBTIQA+
TBGL fo can feel pressured
stnednopser
d et r o p er ye vrus nair otciwithin
V a a particular
ythe
ehtresearch
taht detateam.
ts Recruitment was iterative, with to justify their inclusion
YLLAUSU RO YLLANOISACCO
SUadditional
OIGILER Dguidance
IOVA from the Research Advisory category. We sought to avoid these pressures, and
YTILAUXES RIEHT GNIDIH
SNOITUTITSNI
YTITNEDI REDNEG RO
s e c ivres gnissecca nehw
6 Formerly the Victorian AIDS Council and Victorian Deaf Society respectively
lautca ot eud
la netop ro/dna
FO SECNEIREPXE
NOITANIMIRCSID
More than ticking a Box.indd 17 4/3/21 3:36 pm18 instead focussed our limited time together around 2.4 Data analysis
experiences of health and community services.
Lastly, we recognise the vast differences which can Qualitative data analysis of focus group transcripts
come within disability and LGBTIQA+ identities and follow up contributions was conducted using
such as family support, congenital or acquired thematic analysis and iterative categorisation
disability, and level of engagement with services. across three rounds described below. The
Factors outside these identities which also inform process was designed to facilitate a collaborative
their experiences include cultural background, age, development of meaning and the analytic process
location and so on. of progressive focusing (Srivastava & Hopwood,
2009). Thematic analysis provides a flexibility which
The focus groups were supported by guidelines accommodates the needs of the research project,
developed in response to requests from the peer to capture a complex range of sexual, gender
researchers. The guidelines provided a rundown and disability identities. By embracing researcher
of events (Acknowledgement of Country, consent subjectivity, it recognises the researchers’ active
forms, introductions, and a list of potential interview role within the research (Braun & Clarke, 2013)
questions and topics). The guidelines also included which recognised our position on valuing the voices
notes for various scenarios, such as what to do of peer researchers within the study. Iterative
if group discussion went ‘off track’, if someone categorisation is a technique emerging from
arrived late to the group, or if discussion stalled. The addiction studies (Neale, 2016) which was adapted
guidelines included a suggested list of themes for here to allow for its collaborative approach and the
discussion, such as employment, housing, finances, dual expertise of peer researchers.
relationships, services, and disability/LGBTIQ
communities. Ethical and safety considerations This use of iterative categorisation meant that
were also addressed in line with discussion from analysis of the transcripts freely involved reflections
the Research Advisory Group, and included how of the peer researchers, who could identify
to support a participant who became distressed, their own connections with the source material
and how to maintain confidentiality. The question to expand our understanding. Informed by the
style was open, allowing participants to guide the work of Voronka (2019) it also meant that peer
discussion and share the issues of most significance researcher engagement was not limited to a pseudo
to them. The first question was ‘what brought you ‘professional’ self, which required elimination of
here today?’, which was followed by open ended other equally valued selves or to further question
questions such as ‘what do you think is the most the ‘authenticity’ of peer identities. Instead, it
important thing we need to know?’ and ending with reflected the concept of praxis put forward by
‘is there anything else you’d like to tell us?’ Friere (1986) in his work on liberation for the
oppressed as ‘reflection and action upon the world
Focus groups were digitally recorded for the in order to transform it’ (p. 33).
production of typed transcripts. Participants were
provided with a pen and paper if they wanted to The approach taken to iterative categorisation can
make notes, or write any extra reflections to share be seen in this section.
with the research team. Some participants and Unstructured qualitative data such as focus group
some peer researchers chose to follow up their transcripts often requires some organisation
contribution in writing, which was included in the or order before deeper work can commence
analysis process described below. (Neale, 2016). Accordingly, round 1 was led by
the academic research team and led to the broad
identification of overarching topics. An accessible
More than ticking a Box.indd 18 4/3/21 3:36 pmsummary of each theme was then sent to peer a whole. In this they were supported by each 19
researchers for their review and comment. others’ knowledges and experience, also drawing
Although full transcripts were available, peer on the expertise in lived experience, policy and
researchers preferred to work with the summary, professional experience held by members of
leaving it to function as both an access modification the Research Advisory Group. Our processes
and in scaffolding the upcoming process of analysis. at this point were affected by the situation
surrounding the COVID-19 pandemic and social
Round 2 involved a half-day workshop with the isolation regulations introduced by the Victorian
whole research team. The four peer researchers Government on the 21st of March 2020, which
had each worked with one of the early overarching precluded in-person project meetings. Instead, we
topics, and prepared their comments to some completed this part of the report via email or video
prompt questions to share with the group. This call, rather than in a group face-to-face meeting as
approach was requested as having time to develop planned.
ideas and present their thoughts was experienced
as more accessible by members of the peer This reflexive approach to analysis was designed to
research team. The prompt questions asked them incorporate the multiple experiences held by peer
to: explain the theme to the others, giving some researchers as they related across axes of disability,
examples from the focus group; reflect on how this gender and sexuality. We sought to encourage
theme came out in the focus groups they attended; engagement with and reflection on the data in
share any other thoughts on the theme. The notes a way which would maximise involvement and
from this workshop were presented as issues listed recognise these layers of expertise.
in bullet points, which were then circulated to the
team in advance of round 3 of analysis. Many things were discussed, including visible
versus invisible disabilities, experiences of recent
For round 3, peer researchers reviewed the notes diagnosis, and what can happen when access needs
from round 2 on their own identified theme and for one group may make things more difficult for
one chosen other. At another half day workshop another. The peer researchers talked about their
with the whole research team, peer researchers need for a space in which it was safe for them
again summarised the bullet points and were to express anger, grief and pride as we worked
asked to identify the most pressing or highest through the analysis of the focus group transcripts.
priority issues. This led to a further distilling of the At these times it was the role of the academic
topics, identified emergent cross-topic themes and researchers to hold that space open and reflect on
provided more direction for the research findings. what could be learned not only about the topic at
hand, but about facilitating meaningful inclusion.
The entirety of this report reflects and expands
insights from these analysis workshops. The
recommendations were developed after the
rest of this report had been drafted; when the
research team was able to view the project as
More than ticking a Box.indd 19 4/3/21 3:36 pmYou can also read