MINDFULNESS BASED ELDER CARE - LUCIA MCBEE, LCSW, MPH, CYI WWW.LUCIAMCBEE.COM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MINDFULNESS BASED ELDER CARE
Lucia McBee, LCSW, MPH, CYI
www.luciamcbee.com
MINDFULNESS FOR ELDERS
AND CAREGIVERS
• What is mindfulness?
• Definitions
• Evidence
• Why is mindfulness appropriate for
frail elders and caregivers?
• Applications and adaptations of
mindfulness for elders and caregivers
Mindfulness is paying attention
to our lives,
moment by moment,
on purpose,
in a certain way,
and without
judgment.
-Jon Kabat-Zinn
AWARENESS AND COMPASSION
STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing

MINDFULNESS: THE EVIDENCE HISTORICAL EMPIRICAL PERSONAL

HISTORICAL EVIDENCE • Based on Buddhist and yogic practices • Origins pre AD, approximately 2500 years • Continuously practiced and refined since origins • All major spiritual traditions include contemplative practice

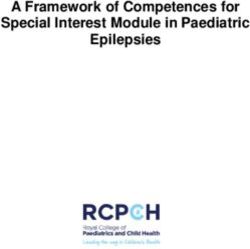
MINDFULNESS: EMPIRICAL EVIDENCE An example of growth in the mindfulness research literature across 32 years, 1980 – 2012. (Results obtained from a search of the term "mindfulness" in the abstract and keywords -limited to publications with English language abstracts.) http://www.mindfulexperience.org/publications.php

THE MODEL:
MINDFULNESS-BASED STRESS REDUCTION (MBSR)
• The most utilized and studied mindfulness
intervention
• Developed in 1979 by Jon Kabat-Zinn
• Psychoeducational group that teaches
meditation, mindfulness and yoga
experientially
• “We are the experts on our health and
healing.”
• Participants encouraged to discover their
own inner resources and strengths
• “There is more right with you than wrong
with you.”
HOW MINDFULNESS HELPS
• IMMEDIATE: TOOLS FOR INSTANT RELIEF
• Interventions can be calming, reducing
stress and anxiety
• PREVENTATIVE: REGULAR FORMAL PRACTICE
• If practiced regularly, will increase an
ability to respond to challenges and
change rather than react
• Potential to increase resiliency
• Physical, emotional and mental changes
may result
MINDFULNESS: KEY STUDIES • Improvements in immune system and brain post MBSR group (Davidson et al, 2003) • Increase in brain’s “grey matter” following 8 week MBSR class (Holzel et al, 2011) • Decrease in cellular aging and disease protection: Increase in telomeres (Epel et al, 2009) • For all studies on mindfulness, visit: www.mindfulexperience.org
STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
PERSONAL EVIDENCE:THE MIND
BODY CONNECTIONTHREE MINUTE BREATHING SPACE
1. Awareness: what is my
experience right now?
2. Gathering: focus on the breath.
3. Expanding: including the entire
body in awareness.
Segal, Williams, and Teasdale Mindfulness-Based
Cognitive Therapy for Depression (2002)MECHANISMS OF MINDFULNESS • Attention regulation • Sustaining attention, and returning • Body awareness • Physical sensations • Emotion regulation • Reappraisal (non-judging awareness) • Exposure, extinction, reconsolidation • Sense of self • Dis-identification with static sense of self • Compassion • (Holzel et al. 2011)
WE ARE NOT HARD-WIRED!
• Neuroplasticity
• Default reactions and the ability for our
brains to physically change in response
to our thoughts, actions, and
environment
• Affective neuroscience
• The possibility of changing emotional
disposition and improving resiliency in
response to thoughts, actions and
environment
• OR, what fires together, wires
togetherTHE SILVER TSUNAMI
NEED FOR NEW MODELS OF MEDICINE • Improvements in acute care à decrease in death from acute illness = population living longer with 1+ chronic conditions • Treatment of chronic conditions is symptom management not cure • New models of care: palliative and CAM/integrative
CARE FOR FRAIL ELDERS • Pharmacological/medical treatment alone often does resolve pain and distress • Mindfulness demonstrated to improve quality of life in multiple populations • Teaching skills that empower • Addresses mind, body and spirit • Multiple chronic conditions require multifaceted approach • Low risk and low cost
MINDFULNESS
AND ELDERS:
EMPIRICAL
EVIDENCE
20COGNITIVE BENEFITS
• Meta analysis of 7 studies suggest a positive effect of
meditation techniques on cognitive functions in the
context of aging and neurodegenerative diseases
(Marciniak, et al. 2014)
• Other studies with older adults show mindfulness and
meditation improve:
• Short term memory, perceptual speed, attention
and executive function (Pakash et al, 2012)
• Mental and emotional health (Moss et al, 2012)
• Memory loss (Hyer et al, 2013)
• Executive function (Moynihan et al., 2013)
• Improvement in cognition and wellbeing for elders
with Mild Cognitive Loss (Wells et al., 2013)
• Cognition and memory improved in
neurodegenerative disease (Newberg et al, 2014)PHYSICAL AND EMOTIONAL BENEFITS
• MBSR decreases
• Psychological distress (Young et al, 2010)
• Sense of loneliness and pro-inflammatory gene
expression in elders (Creswell et al., 2012)
• Lower back pain and improves quality of life (Morone, et
al., 2008)
• MBSR improves health-related quality of life
(Moss et al., 2013)
• Mindfulness-Based Cognitive Therapy (MBCT)
• Helpful for depression (Smith et al., 2007)
• Improves sleep, rumination, anxiety and
depression (Foulk et al 2013)
• MBI decreases blood pressure (Palta et al., 2012)TRADITIONAL MBSR CLASS
• Teaches and practices
• Meditation
• Walking meditation
• Yoga (meditation in movement)
• Informal mindfulness practice- paying
attention
• Group format
• Eight weeks, 2 ½ hour classes
• One all day retreat
• Daily homework using CDs or MP3s
• DiscussionTRADITIONAL MBSR CRITERIA-
Participants need to be able to:
• Contain affect
• Listen and respond in the present
• Utilize instructional audio CDs and
follow classroom instructions
• Remain in the classroom and cope
with group format
• Practice yoga or equivalent
• Organize thoughts, manage logistics
and time commitment
-Dobkin et al 2011STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
MINDFULNESS-
BASED ELDER
CARE (MBEC):
ADAPTING THE
MODEL FOR
FRAIL ELDERS
AND
CAREGIVERSMBEC: OVERVIEW • Modifying the practices • Programs for elders with physical and cognitive frailties • Adaptations for the institutional environment • Working with caregivers
•!Presence and compassion: the essence of
the practice
•!Teaching adaptations
•!Shorter groups
•!Simplified language
•!Increased repetitionVERBAL, VISUAL, PHYSICAL AND NON-VERBAL CUING
STRETCHES, MEDITATIONS AND OTHER EXERCISES MODIFIED FOR ELDERS
MBEC PRACTICES
MINDFULNESS
MEDITATIONGUIDED IMAGERY
MINDFUL MOVEMENT
DIAPRAGMATIC BREATHING
STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
ENVIRONMENTAL ADAPTATIONS •! Creating a calming milieu •! Aromatherapy •! Music
The most important factor is the teacher • A calm demeanor • Flexibility • Acceptance
STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
MBEC APPLICATIONS FOR ELDERS • Groups for nursing home residents with physical and cognitive disabilities • Groups for elders with moderate- severe dementia and behavioral problems • 1:1 with isolated elders • MBEC by telephone •
MINDFULNESS GROUPS FOR
INSTITUTIONALIZED ELDERS
• Elders who completed MBSR showed
improvements in mood and health related
quality of life (60% drop out, homework not
feasible) (Ernst et al, 2008)
• MBEC participants show improved quality of
life and trends towards improved pain
• CDs and homework not feasible
• Attendance irregular
• Ongoing group more successful than time limited
group (McBee et al, 2004)QUOTES • “Makes me feel at peace with the world. It helps my whole body and spirit. I forgot all my troubles.” • “I’ve always liked this [group] since I started.. being quiet, relaxed.. a special feeling.” • “I feel more alive in spite of the pain” • “I feel uplifted. I realize we all have pain. We talk about how we are getting along. It is important to be with other people.”
MBEC ON A DEMENTIA UNIT
• Structured format
• Deep breathing, Gentle stretches, Guided
imagery, Aromatherapy
• Flexibility and presence of teacher
• Results
• Agitated residents benefit from ongoing
group
• Staff also benefit
• Improvements in mood and decrease in
agitation (Cohen-Mansfield scale) (Lantz et
al, 1997)MBEC FOR ISOLATED ELDERS
• By telephone
• Taught via phone and premailed handouts
• Time for discussion, feedback and sharing
• Positive anecdotal feedback
• 1:1 in nursing home
• Identifying problems and current coping
• Individualized interventions
• Isolated elders and caregivers
• Can be used by caregiver and care receiver
• CDs or tapes in other languages can
overcome language barriers
• McBee, 2008STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
CARE FOR THE CAREGIVERS
MBSR FOR FAMILY/FRIEND
CAREGIVERS: THE RESEARCH
• Decreases in caregiver burden, depression
and caregiver self assessment post MBSR
group (Epstein et al, 2009)
• Meta analysis find meditation-based
interventions improve psychological
distress of family caregivers (Hurley et al, 2013)
• Adapted MBCT for caregivers shows
significant improvement in caregiver
distress (Oken et al, 2010)
• MBSR effective for improving mental health,
reducing stress and decreasing depression
in caregivers (Whitebird et al, 2012)STRESS AND MBSR CLASS FOR HEALTH CARE
PROFESSIONALS AND PARAPROFESSIONALS
• 1 in 3 MDs experiencing burn out: :
• Loss of empathy and compassion
• Likelihood of making medical errors
• Influencing trust and confidence of patients
• Emotional exhaustion (Shanafelt 2009)
• MBSR benefits physical and mental health of
health care providers ( Irving et al., 2009)
• Improvements in well-being and attitudes
for MDs post MBSR (Krasner et al., 2009)
• MBSR and mindfulness intervention improve
relaxation and life satisfaction in nurses (Poulin
et al., 2009)MBEC FOR STAFF AND !
FAMILY/FRIEND CAREGIVERS
•! Staff stress reduction offerings
•! One, one hour in-service for entire staff
•! Seven session class for interdisciplinary staff
on two units
•! Wellness coordinator offering
stress reduction
•!Mini on unit classes
•! Family and friend caregivers
•! MBSR classes
•! Nursing home residents and
caregivers togetherTEACHING MINDFULNESS
TO CAREGIVERS
• Emphasize importance of stress
reduction
• Consider short meditations and those
that can be integrated into a busy life
• Integrate meditation that can be used
while caregiving
• Invite caregivers to participate in groups
with eldersThe most important intervention we can bring to our elders is our selves- who we are in each moment. - McBee
Put on your own oxygen mask first!
THREE MINUTE BREATHING SPACE
1. Awareness: what is my
experience right now?
2. Gathering: focus on the breath.
3. Expanding: including the entire
body in awareness.
Segal, Williams, and Teasdale Mindfulness-Based
Cognitive Therapy for Depression (2002)FORMAL AND INFORMAL PRACTICE FORMAL PRACTICE • Set aside a time each day when you know you will not be disturbed • Take a community class • Organize your friends or co-workers for regular practice INFORMAL PRACTICE • Pay mindful attention to everyday activities either yours or with the one(s) you care for • Use transitional time or waiting time as an opportunity • Observe nature • Set your watch or smart phone for an hourly stretch minute
12 FREE AND SIMPLE SELF CARE SKILLS 1. Pay attention 2. Listen to your body 3. Put things in perspective 4.Take a deep breath 5. Drink a glass of water 6. Take a walk 7. Do a good deed 6. Talk to a friend 9. Smile and Laugh 10. Do something creative 11. Practice gratitude 12. Visualize someone or something you love
OR, JUST STOP • S- Stop what you are doing • T- Take a breath • O- Observe how you are feeling • P- Proceed with what you were doing
If you think you're too small to have an
impact, try going to bed with a mosquito
in the room.
- Anita KoddickTHANK YOU!
You can also read