Methylprednisolone-Induced Hypertension - Role for the Autonomic and Renin Angiotensin Systems
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Methylprednisolone-Induced Hypertension
Role for the Autonomic and Renin Angiotensin Systems
OSVALDO KOHLMANN JR., M.D., ARTUR B. RIBEIRO, M.D., ODAIR MARSON, M.D.,
MANOEL A. SARAGO£A, M.D., AND OSWALDO L. RAMOS, M.D.
SUMMARY The role of the autonomic nervous system (ANS) in the pathogenesis of hypertension induced
by methylprednisolone (20 mg/kg/week subcutaneously) was studied in rats before and during chronic renin
angiotensin system (RAS) blockade with captopril (20 mg/kg/erery 8 hrs by mouth). Sympathetic nervous
system (SNS) blockade was accomplished by the intravenous (i.v.) administration of propranolol (0.20
mg/lOOg) plus phentolamine (1.25 mg/lOOg/i.r.) and ganglionlc (G) blockade by the use of pentollnium tar-
tarate (0.5 mg/100g/i.v.). After 4 weeks, methylprednlsolone-treated animals'showed significant decreases in
mean arterial pressure (MAP) with both SNS (-34 ± 2 ram Hg) and G (-56 ± 3 mm Hg) blockades; during
chronic RAS blockade, even greater falls in MAP were observed (SNS = -43 ± 2 mm Hg and G = -75 ± 3
mm Hg). Nevertheless, for both groups the levels of MAP obtained during SNS and G blockades were higher
than those observed in their control groups. At the end of second week, however, in captopril-treated hyper-
tensive rats the values of MAP obtained during ANS blockade were lower than those observed in the control
group. An increased responsiveness to exogenous administration of norepinephrine (NE) was observed in
animals receiving methylprednisolone and captopril. It is concluded that methylprendisolone hypertension in
the rat may be initially explained by activation of RAS and ANS. At later phases, a third mechanism has to be
postulated to explain the hypertensive state. (Hypertension 3 (suppl II): II-107—11-111, 1981)
KEY WORDS * glucocorticoid-hypertension • autonomic nervous system •
renin angiotensin system • norepinephrine responsiveness • captopril • saralasin
S EVERAL mechanisms have been proposed to
explain the pathogenesis of excess glucocorti-
coid hypertension. They include: salt reten-
tion,1 activation of the renin angiotensin system, 1 ''
increased plasma and extracellular volumes,4 and al-
Methods
Induction of the Hypertensive State
Male Wistar rats receiving regular rat chow and tap
water were used. Four groups of rats were prepared: 1)
terations in various components of the autonomic ner- Group M (n = 20), receiving a long-acting prepara-
vous system (ANS).6"7 tion of soluble methylprednisolone (Depo-Medrol,
We have recently confirmed that hypertension in- Upjohn) at a dose of 20 mg/kg/week subcutaneously;
duced by methylprednisolone in the rat is accom- 2) Group M + C (n = 20), receiving methyl-
panied by activation of the renin-angiotensin system.' prednisolone as in Group M plus concomitant cap-
However, this hypertension may occur even during topril (Squibb and Sons') at a dose of 20 mg/kg/every
chronic renin angiotensin system blockade with cap- 8 hours by gavage; 3) Group N (n = 20), receiving dis-
topril," leading to the conclusion that other mech- tilled water by the same route and same frequency as
anism^) may participate in the pathogenesis of this Group M; 4) Group N + C (n = 20), receiving dis-
hypertension. In this study we tested the role of the tilled water as Group N plus concomitant daily cap-
ANS in hypertension induced by methylprednisolone topril given as in Group M + C. All groups were
in the rat. Special emphasis is placed upon the interac- followed for 4 weeks, and tail arterial pressure was
tion of the autonomic and renin angiotensin systems in registered every week using a tail microphonic
this type of experimental hypertension. method' in unanesthetized animals.
From the Department of Medicine, Division of Nephrology, Pharmacological Blockade of the Sympathetic Nervous
Escola Paulista de Mcdicina, SSo Paulo, Brazil
Dr Ribeiro is an Established Investigator from the Brazilian System (SNS)
Council for the Development of Science and Technology (CNPq) At the end of the fourth week, 10 animals of each
Address for reprints Artur B. Ribeiro, M D, Associate
Professor of Medicine, Division of Nephrology, Escola Paulista de experimental group (M; M + C; N, and N + C) had
Medicina, Rua Botucatu, 720-04023 S3o Paulo, Brazil catheters placed into the carotid artery and jugular
11-107
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 201511-108 PROCEEDINGS/INTERAMERICAN SOCIETY S U P P II, HYPERTENSION, VOL 3, N o 6, N O V / D E C , 1981
vein under ether anesthesia. On awakening, the rats' TABLE 1. Tail Arterial Pressure (in mm Hg) in groups M,
mean arterial pressure (MAP) was continuously M+C,NandN+C
recorded with a Beckman physiograph, and the ani- Weeks
mals were kept unrestrained with free access to water Groups Control 1 2 3 4
and food. After a 2-hour control period, blockade of M 114 ± 1 126 ±1* 138 ± 1 * 147 ± 1* 155 ± 1*
sympathetic nervous system (SNS) was induced by in- M + C 116 ± 1 119 ± 1 122 ±1** 134 ± 1** 140 ±1**
travenous administration of propranolol (Inderal,
N 114 ± 1 116 ± 1 117 ± 1 117 ± 1 116 ± 1
Ayerst Laboratories) at a dose of 0.20 mg/100 g body
weight, followed by phentolamine (Regitine, Ciba N + C 116± 1 114 ± 1 110 ± If 108 ± IT 107 ± IT
Geigy Corporation) at a dose of 1.25 mg/100 g body •p < 0.01 compared to groups M + C, N and N + C.
weight/i.v. The MAP was recorded for 60 minutes **p < 0.01 compared to group N and N + C.
after the initial injection. Results are expressed by tp < 0.01 compared to group N.
differences in MAP values before propranolol and 30
minutes after phentolamine administration. Identical
procedures as described above were used in animals of
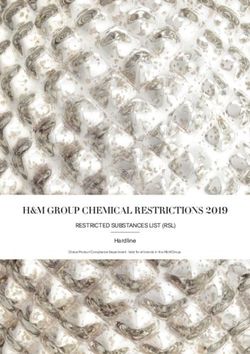
Absolute values of direct MAP, as well as changes
Groups M + C (n = 12) and N + C (n = 12) studied in MAP induced by SNS and ganglionic blockade, are
at the second week. summarized in table 2 and figure 1 respectively. It is
apparent that both SNS and ganglionic blockade
Ganglionic Blockade and Vascular Responsiveness to evoked significant drops in MAP in all groups. During
Norepinephrine (NE) SNS blockade, reductions in MAP of methyl-
Four weeks after the initiation of methylpred- prednisolone-treated groups (M = — 34 ± 2 mm Hg
nisolone administration, 10 animals of each group (M, and M + C = —43 ± 2 mm Hg) were significantly
M + C, N, and N + C) were prepared, as described greater (p < 0.01) than those observed in the control
above. After a 30-minute control period, norepineph- groups (N = - 1 5 ± 2 mm Hg and N + C = - 2 4 ± 1
rine (NE) (Noradrenaline, ByK Laboratories) was ad- mm Hg). Similar but greater decreases in MAP were
ministered at increasing doses of 50, 100, and 200 observed during ganglionic blockade: M = —56 ± 3
ng/100 g body weight, i.v. Each injection was given mm Hg; M + C = - 7 5 ± 3 mm Hg; N = - 3 4 ± 2
after the MAP had stabilized following the previous mm Hg; and N + C = - 4 8 ± 2 mm Hg. It is also
injection, and each dose was given twice. The effect of noteworthy that in the captopril-treated groups (M +
NE upon MAP is represented by the mean of the two C and N + C) changes in MAP induced by both
maximal elevations observed for each dose used. blockades were significantly greater than those ob-
Following a recovery period from the last dose of NE, served in the groups that did not receive that drug (see
all animals underwent ganglionic blockade by the ad- figure 1). Furthermore, during autonomic nervous
ministration of pentolinium tartarate (Ansolysen, system blockade MAP values in the M + C group
Wyeth Laboratories) given as a single intravenous
dose of 0.5 mg/100 g body weight. The MAP was
registered continuously, and after stabilization, TABLE 2. Mean Arterial Pressure (MAP) m mm Hg Before
responses to NE were evaluated as before pento- and During Sympathetic Nervous System (SNS, Proprano-
linium. Vascular responsiveness to NE was also tested lol + Phentolamine) and Ganglionic (Pentolinium Tartar-
ate) Blockade m Groups M, M + C, N and N + C Studied at
in eight animals of Group M + C and N + C studied the 4th week (X ± SEM)
at the second week.
Groups Before SNS Ganglionic
Results are expressed as mean ± standard error of
the mean. Statistical analysis were obtained by Stu- M 154 ±2* 118 ±2* 100 ±4*
dent / test or analysis of variance when appropriate. M+C 136 ± IT 93±2t 60±3T
N 115 ±3TT 100±3TT 81 ±2TT
Results N+C 98 ± 1 73 ± 2 50±l
Table 1 shows the values of tail arterial pressure *p < 0.01 — compared to groups M + C, N and N + C.
(TAP) observed in the four groups studied. As can tp < 0.01 — compared to group N + C.
be seen, in animals receiving only methylpredniso- ftp < 0.01 — compared to group N + C.
lone TAP was significantly elevated by 1 week, and
reached a maximal elevation of 41 ± 1 mm Hg at 4
weeks. In the group receiving captopril methyl-
prednisolone (M + C), a progressive rise in TAP was TABLE 3. Mean Arterial Pressure (MAP) m mm Hg Before
and During Sympathetic Nervous System (SNS, Proprano-
observed only after the first week, and a maximal lol + Phentolamine) and Ganglionic (Pentolinium Tartar-
change of 24 ± 1 mm Hg was observed at the fourth ate) Blockade in Groups M+C, and N+C Studied at the
week. These values were significantly lower than those 2nd Week (X ± SEM)
observed in Group M (p < 0.01). No significant Before SNS Ganglionic
Groups
changes in TAP were noted in Group N, whereas a
small but statistically significant decrease (ATAP = M+C 112 ± 1 * 76 ±2* 50 ±3*
- 9 ± 1 mm Hg, p < 0.01) was observed in Group N N+C 98 ± 2 85±3 61 ± 2
+ C at the fourth week. *p < 0.01 compared to group N + C.
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 2015METHYLPREDNISOLONE-INDUCED HYPERTENSION/Kohlmann et al. 11-109
fiMAP 0 AMAP
(mriHg}
(mmHg)
-10 -
-10 -
-20 -
N+C
N+C -20 -
-30 -
-40 - -30 -
M+C
-50 - M+C
-40 -
SNS
-60 -
D
0 GANGLIONIC -50 •
-70 -
Q SNS
-80 - GANGLIONIC
-60 -
J
FIGURE 1. Decreases in mean arterial pressure (AMAP), -70
in mm Hg, during sympathetic nervous system (propranolol FIGURE 2. Decreases in mean arterial pressure (AMAP),
+ phentolamine) and ganglionic (pentolinium tartarate) in mm Hg, during sympathetic nervous system (propranolol
blockades in Groups M, M + C, N and N + C studied at + phentolamine) and ganglionic (pentolinium tartarate)
fourth week. *p < 0.01 compared to Group M, **p < 0 01 blockades in Groups M + C and N+C studied at second
compared to Group N week *p < 0 01 compared to Group N + C.
reached levels that were significantly lower than those
observed in the M group, and similar to those of the
N group. However, MAP in the M + C group re-
mained significantly higher than in the N + C group
(see table 2). AMAP
Values of MAP in the groups studied at the second (mmHg)
week (M + C and N + C) before and during SNS and 120 -
BEFORE
ganglionic blockade are shown in table 3 and figure 2. DURING GANGLIONIC * •
Basal MAP values in M + C group were significantly BLOCKADE
higher than those of N + C. Also, both blockade 100 -
procedures resulted in evident decreases in MAP *T*
values for both groups. However, drops in MAP were
of greater magnitude in M + C animals ( - 3 2 ± 2 and
—59 ± 2 mm Hg, figure 2) as compared to those ob-
80 -
]lc
tained in Group N + C ( - 1 3 ± 1 mm Hg and - 3 6 ±
** ...-'"' . ', •
2 mm Hg) {p < 0.01 for both procedures). Thus, dur- 60 -
ing both blockades, MAP was lower in Group M + C I . - - ' ' . - - ' • ' ^ , - ' '
as compared to Group N + C. 1' ___J^ + C
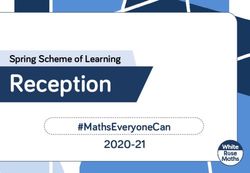
Figure 3 shows the increments in MAP obtained TM
40 • =S3 N
with NE injections before and during ganglionic - ^ ^ N+C
blockade. It is evident that the NE-induced incre-
ments in MAP were greatly enhanced by ganglionic 20 •
?
blockade. Both before and during ganglionic block-
ade, elevations in MAP induced by NE were greater in
Group M + C as compared to the other groups (p <
0.05, M + C vs M or N or N + C).
50 100 200 NE(ng/IOOg)
Figure 4 shows elevations of MAP induced by NE
before and during ganglionic blockade in Groups M +
C and N + C studied at the end of second week. For FIGURE 3. Mean arterial pressure elevations (AMAP)
all but the first NE dose tested, elevations in MAP for with increasing doses of norepinephrtne (NE) before and
both groups were significantly greater during gan- during ganglionic blockade at the fourth week. *p < 0 05
glionic blockade. Again, greater elevations in Group compared to Groups M, N, and N+C before ganglionic
M + C were observed before and during ganglionic blockade **p < 0 05 compared to Groups M, N, and N +
blockade for all three NE doses tested. C during ganglionic blockade.
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 201511-110 PROCEEDINGS/INTERAMERICAN SOCIETY SUPP II, HYPERTENSION, VOL 3, N o 6, N O V / D E C , 1981
A MAP Thus, methylprednisolone hypertension cannot be ex-
mmHg)
plained only by hyperactivity of the ANS. These
eo - results agree with a previous report from our labora-
tory which documented a role for the RAS in the
BEFORE maintenance of this type of hypertension.' In the
DURING GANGLIONIC group receiving captopril and methylprednisolone (M
100 - BLOCKADE + C), ANS blockade caused decreases in MAP that
V M+C were greater than those of Group M. Also, the levels
of M A P attained during ganglionic and SNS
60 - y blockades were lower in M + C as compared to M.
This fact helps to corroborate the hypothesis of a
N+C simultaneous activation of the RAS and SNS in the
•• methylprednisolone-induced hypertension. However,
60 - the fact that, during ANS blockade, the blood pres-
^y M+C sure levels of the captopril-treated group (M + C)
were still higher than those of its appropriate control
(N + C) suggests that a third factor, in addition to
40 - N+C
ANS and RAS, must be involved to explain the hy-
•P pertension following methylprednisolone adminis-
tration.
20 -
r"
^-^^^ In contrast, at the second week of glucocorticoid
administration, both SNS and ganglionic blockades
completely reversed elevations of MAP observed in
Group M + C. Actually, during these blockades,
50 100 200 NE
MAP levels were even lower in Group M + C com-
(ng/IOOg) pared to those of Group N + C. Thus, it is apparent
that in the earlier phases of methylprednisolone ad-
ministration the elevations in blood pressure may be
FIGURE 4. Mean arterial pressure elevations (LMAP)
explained by simultaneous activation of the RAS and
with increasing doses of norepinephnne (NE) before and
ANS only.
during ganglionic blockade at the second week *p < 0 05
compared to Group N + C before ganglionic blockade. **p Whereas the role of the renin-angiotensin system in
< 0 05 compared to Group N + C during ganglionic this type of hypertension is well established,2' ' • ' the
blockade. effect of glucocorticoid administration on SNS func-
tion remains controversial. 1 ' 6 ' '• '• 10 Some others have
suggested alterations in tissue metabolism of cate-
cholamines" and others, an increase in vascular sensi-
tivity to exogenous NE.' 1 7 In our work we observed
that methylprednisolone alone did not significantly
alter vascular responsiveness to the three doses of ex-
Discussion ogenous norepinephrine used, since MAP elevations
A role for the renin angiotensin system (RAS) in were similar in Group M and N both before and dur-
the pathogenesis of methylprednisolone hypertension ing ganglionic blockade. Comparable results were pre-
in the rat has been previously demonstrated.*• *• * viously reported in the same species studied at 2
However, we have reported previously that RAS weeks.2 However, when methylprednisolone was asso-
blockade with captopril does not prevent the develop- ciated with captopril (Group M + C), a significant in-
ment of this type of hypertension." This observation is crease in responsiveness to these doses of NE was ob-
confirmed in the present work, since elevations in arte- served before and particularly during ganglionic
rial pressure were evident at the fourth week in the blockade. This was observed already at the second and
group treated with methylprednisolone and captopril was still present at the fourth week. This increased
(M + C). Thus, other mechanism(s) must have come responsiveness to NE cannot be attributed to captopril
into play to explain the elevations of MAP during alone since the increments in blood pressure observed
chronic RAS blockade. in Group N + C are not different from those of Group
Our results clearly show that administration of N (fig. 3). Thus, we could observe an increased respon-
methylprednisolone for 4 weeks causes hypertension siveness to three exogenously administered doses of
accompanied by an increase in SNS activity. Accord- NE only with the association of methylprednisolone
ingly with both pharmacological blockade procedures and captopril. Although interpretation of these results
used, significantly greater drops were observed in is difficult, one might speculate that a diminished
methylprednisolone-treated rats. In the group of endogenous liberation of catecholamines induced by
animals receiving only methylprednisolone (M), both the diminution of angiotensin II caused by captopril11
blockades elicited significant drops in MAP; however, could unmask the reported hypersensitivity of
the levels of MAP attained were still greater than adrenergic receptors caused by corticosteroid.7 The
those observed in the appropriate control (Group N). enhanced responsiveness observed in the Group
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 2015METHYLPREDNISOLONE-INDUCED HYPERTENSION/Kohlmann el al. 11-11
M + C after ganglionic blockade could help to sup- 3 Elijovich F, Krakoff LR Effect of converting enzyme inhibition
on glucocorticoid hypertension in the rat. Am J Physiol 238:
port this hypothesis. H844, 1980
In conclusion, it is possible to detect the participa- 4 Haack D, MBhnng J, M5hnng B, Petnm M, Hackental E
tion of both the renin-angiotensin system and the Comparative study on development of corticostcrone and
autonomic nervous system in the pathogenesis of glu- DOCA hypertension in rats Am J Physiol 233: F403, 1977
5 Kalsner S Mechanism of hydrocortisone potentiation of re-
cocorticoid hypertension. In the early stages (second sponse to cpinephnne and norepinephnne in rabbit aorta Circ
week) of hypertension, these two factors seem to be Res 24: 383, 1969
responsible for the elevated blood pressure. Subse- 6 Mendlowitz M, Naftchi N, Weinreb HL, Gitlow SE' Effects of
quently (fourth week) a third factor must be predmsolone on digital vascular reactivity in normotensive and
postulated to explain the raised arterial pressure. The hypertensive subjects J Appl Physiol 16: 89, 1961
7 SchCmig A, Lflth B, Dietz R, Gross F Changes in vascular
apparent role of the ANS hyperactivity in this type of smooth muscle sensitivity to vasoconstrictor agents, induced by
hypertension may be, at least in part, explained by an corticosterone, adrenalectomy and differing salt intake in rats.
increased responsiveness to catecholamines. Clin Sci Mol Med 51: 61s, 1976
8 Kohlmann O Jr, Marson O, Ramos OL, Ribeiro AB Effect of
captopril on glucocorticoid excess hypertension. Clin Res 28:
333A, 1980
9 Friedman M, Freed C Microphone manometer for indirect
determination of systolic blood pressure in the rat Proc Soc
References Exp Biol Mcd 70: 670, 1949
10 Sambhi MP, Weill MH, Udhoji VN Pressor responses to
1. David SD, Gneco MH, Cushman P Adrenal glucocorticoids norepinephrine in humans before and after corticosteroid Am J
after twenty years' a review of their clinically relevant conse- Physiol 203: 961, 1962
quences. J Chron Dis 22: 637, 1970 11 Antonaccio ML, Kerwin L' Pre and Post junctional inhibition
2 Krakoff LR, Selvadurai R, Sutter E Effect of methyl- of vascular sympathetic function by captopnl in SHR Implica-
prednisolone upon arterial pressure and the renin angiotensin tion of vascular angiotensin II in hypertension and anti-
system in the rat Am J Physiol 228: 613, 1975 hypertensive actions of captopnl Hypertension 3: 54, 1981
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 2015Methylprednisolone-induced hypertension. Role for the autonomic and renin angiotensin
systems.
O Kohlmann, Jr, A B Ribeiro, O Marson, M A Saragoça and O L Ramos
Hypertension. 1981;3:II-107
doi: 10.1161/01.HYP.3.6_Pt_2.II-107
Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1981 American Heart Association, Inc. All rights reserved.
Print ISSN: 0194-911X. Online ISSN: 1524-4563
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://hyper.ahajournals.org/content/3/6_Pt_2/II-107
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Hypertension is online at:
http://hyper.ahajournals.org//subscriptions/
Downloaded from http://hyper.ahajournals.org/ by guest on May 20, 2015You can also read