Mental Health and Addictions Transformation Phase II Report - Te Pare ō Toi Bay of Plenty District Health Board
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Te Pare ō Toi
Bay of Plenty District Health Board
Mental Health and
Addictions
Transformation Phase II
Report
Date: 7 July 2021
Author: Louise Ihimaera (Project Lead)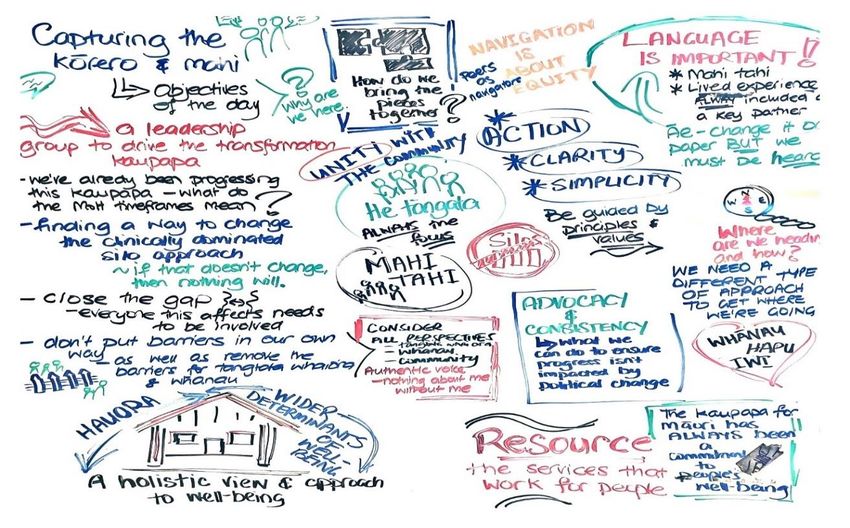
Takina atu rā te kawa tapu o ngā atua, I tiritiria, i poupoua i Papatūānuku Ki te ira tangata, Ki te whai ao, ki te ao mārama, Hei oranga mō te iwi, Mai i ngā kurī a Whārei ki Tihirau, Mai Maketū ki Tongariro, Toi Ora ē! Kei te mutunga kore āku mihi ki tōku Matua i te rangi, nānā nei tōku wānanga Ka nui tonu te reo maioha ki ngā tupuna, nā rātou anō te whāriki mō āku rekereke, te korowai mō āku pokohiwi. Ka huri tōku whakaaro ki ngā whānau, ki ngā tangata whaiora me ngā tangata katoa nā rātou ake ngā kōrero ki roto i tēnei rīpoata, tēnā koutou tēnā koutou tēnā koutou katoa Mai tē kore ki te pō, mai te pō ki te wheiao ki te ao mārama Kei te mutunga kore āku mihi ki tōku Matua i te rangi, nānā nei tōku wānanga Ka nui tonu te reo maioha ki ngā tupuna, nā rātou anō te whāriki mō āku rekereke, te korowai mō āku pokohiwi. Ka huri tōku whakaaro ki ngā whānau, ki ngā tangata whaiora me ngā tangata katoa nā rātou ake ngā kōrero ki roto i tēnei rīpoata, tēnā koutou tēnā koutou tēnā koutou katoa. We appreciate all those, past and present who have been a part of the MHA Transformation Programme activities over the past 2 to 3 years and more specifically during the past 6 months. The wide stakeholder engagement across Te Moana a Toi, West and East Bay of Plenty has involved Te Kāhui Kaumātua, Te Rūnanga Hauora ō Te Moana a Toi, ngā Iwi katoa. Kaupapa and Māori providers, mainstream NGO providers and DHB primary, planning and funding, and secondary mental health services, Primary Health Organisations and Alliances. To the Whānau, Lived Experience, Consumer Consultants, Peer Support Workers, and individuals who shared selflessly with your time, expertise and resource – we acknowledge you for your courage in standing up and out, fearlessly reminding us why and who it is that we are here for. Your voices like so many others have been a catalyst for enabling positive change. You have all contributed in numerous ways in the various roles you walk and work in the services. Kei te mihi kei te mihi kei te mihi ki a koutou katoa.
Ngā Rārangi: Table of Contents FOREWORD ................................................................................................................................. 3 1.0 EXECUTIVE SUMMARY ........................................................................................................ 4 2.0 PRELUDE: TE MOANA A TOI: BAY OF PLENTY REGION .......................................................... 6 TRANSFORMING MENTAL HEALTH & ADDICTION SERVICES ........................................................... 6 3.0 PHASE II COMMUNITY CONSULTATION ................................................................................ 8 4.0 CONCLUSION ..................................................................................................................... 26 5.0 REFERENCES ..................................................................................................................... 30
FOREWORD
Contributors in the Mental Health & Addiction Transformation phases I and II open their
journey of ‘preparing for collaborative design’ with acknowledgement of Te Toi Ahorangi and
to the greatness of Te Moana a Toi tūpuna who looked to te pō where they were nourished
with knowledge and wisdom in searching and reading ngā whetū, the stars.
“Like our great ancestors, we look to te pō, the space that blankets our sky each night to reveal
the tapestry of stars that connect us to our past and future generations. It is in the darkness
that we see the light of our tomorrow”1
The constellation of Matariki has appeared and features as the first star of the Māori New
Year. Matariki is seen as a time of reflection, a time to let go, a time to celebrate and a time
for new beginnings.
“Most of the time, the right time to find Matariki is at the end of June, or the beginning or
middle of July. That’s Pipiri on the Māori calendar ... using the lunar year”
(Dr. Rangi Matamua in interview 22 May 20172)
Significant to this time of transformation of Mental Health and Addiction services,
communities and their members in the Bay of Plenty, are also looking to the stars.
“This is divine timing Whaea. Hiwa-i-te-Rangi, the 9th star of Matariki signals it is time for all
Māori aspirations, dreams and innovations to be grounded into the Health sector systems …
I feel all our tupuna are celebrating … and wow it’s overwhelming in knowing that”3.
Matariki is a time for reflection and for celebration and on Friday June 24th of 2022,
“Matariki will be a distinctly New Zealand holiday … our first public holiday that recognises Te
Ao Māori” (Honourable Jacinda Ardern, Prime Minister, New Zealand, 5th February 2021)4.
1Te Rūnanga Hauora Māori ō Te Moana a Toi. 2019.
2
Te Kuru Marama Dewes. Monday May 22nd 2017. Dr. Rangi Mātāmua Hopes to Revive Māori Astronomy. Retrieved
https://www.teaoMāori.news/dr-rangi-matamua-hopes-revive-Maori-astronomy
3
Te Rereorangi Tutua, Lived Experience & Peer Support Advocate, 25th May 2021 shared in personal communication.
4
Elle Hunt in Wellington. Thursday February 4th 2021. New Zealand Creates Public Holiday to Celebrate Māori New Year.
Retrieved: https://www.theguardian.com/world/2021/feb/04/new-zealand-matariki-creates-public-holiday-to-
celebrate-Maori-new-year-waitangi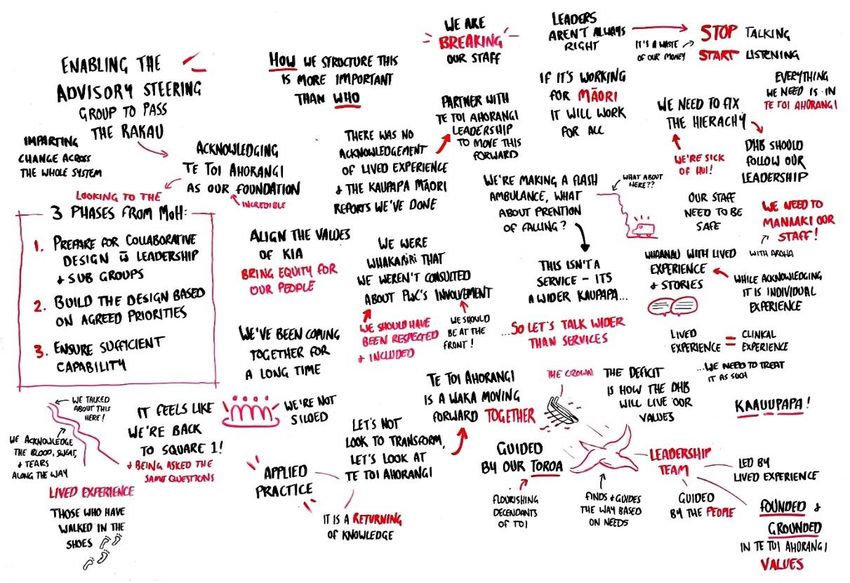
1.0 Executive Summary
Transformational change has many meanings to many groups of people and individuals in Aotearoa.
For the people of Bay of Plenty the significant events of the partnership between Te Rūnanga Hauora
Māori o Te Moana a Toi representing 17 Iwi; and the Bay of Plenty District Health Board (BOPDHB)
have been a key catalyst of change for the transformation of Mental Health and Addiction (MHA)
Services. In 2019 the people witnessed the launch of Te Toi Ahorangi as the foundational commitment
of both parties to work together by honouring te Tiriti o Waitangi to reduce health disparities and
inequity for Māori. In doing so, this partnership is supporting the goal to achieve overall improvement
of the population’s health and wellbeing.
This report acknowledges related activities undertaken during MHA transformation phase I and
illustrates the activities during Phase II. It can be hoped that the partnerships that have been created
and strengthened during the Phase II period of 6 months will also be a catalyst for change. Important
to note are some of the challenges that came up for Kaupapa Māori providers and others in what they
regarded as a lack of appropriate action, ineffective communication, and perceptions of not being
heard since their consultation hui of over a year ago. Opportunities, considerations, and a way forward
in how to address these concerns are presented in this report.
Overall, the various groups and individuals who participated in consultation hui and sector
representatives who came together, helped establish an Advisory Steering Group and produced
important outcomes. These outcomes are highlighted throughout this report and in section six,
individuals and groups share how relationships strengthened during that six-month period and
collaborative initiatives are progressing towards achieving the goals of equity for Māori and
improvements for overall population health.
The Wai 2575 Hauora claims provided catalysts for efficient transformative change for national groups
and particularly for He Ara Oranga panel and their 40 recommendations. Moreover, the panel of
inquiry members considered their process itself was a catalyst for remarkable change in that:
the breadth of its Terms of Reference took a whole of community and cross sector approach.
there was a striking degree of consensus from most parts of New Zealand society about the need
for change and a new direction.
the panel deliberately took a ‘people first methodology’, and
remained guided by the needs of the people and the community rather than the preferences of
various groups as has been done in the past from the many other Mental Health reviews that have
happened5.
Prominent Māori Leader Tā Mason Durie6 also asserts a transformational mindset change is essential
as he submits Te Kawenata o Waitangi, is ‘the covenant’ that declares Te Tiriti is more than a founding
document. Highlighting that central to the functioning of the New Zealand Health system, whether
there are health inequities or not Te Kawenata o Waitangi reinforces the relationships that support
and enable Māori to experience equivalent health outcomes to non-Māori.
Lived Experience Leader Mary O’Hagan (2018) is another example promoting transformation in the
Wellbeing Manifesto to change current terminology with new language to replace mental illness and
mental health. Wellbeing to replace mental health and distress or, mental distress replaces mental
illness (O’Hagan, 2018). Seven wellbeing priorities7 expect a government commitment to prevent,
respond to, and to lessen the impact of mental health distress and addiction (ibid). These wellbeing
priorities and ‘new’ language terms sit well with Māori who have for a long time advocated a wellness
approach in oranga hinengaro treatment and healing.
All these key events for change have influenced the discussions and views throughout this document.
We also take heed of and leadership from the tūpuna that by looking back we will move forward
learning valuable lessons from the past.
5 The Crown. 2018. He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction Inquiry (p 10).
Office of the Minister of Health: Wellington.
6 A Window on the Quality of Aotearoa New Zealand’s Health Care [HQSC]. 2019: Professor Tā (Sir) Mason Durie. Window
of Quality HQSC, 2019, p6)
7 See appendix two.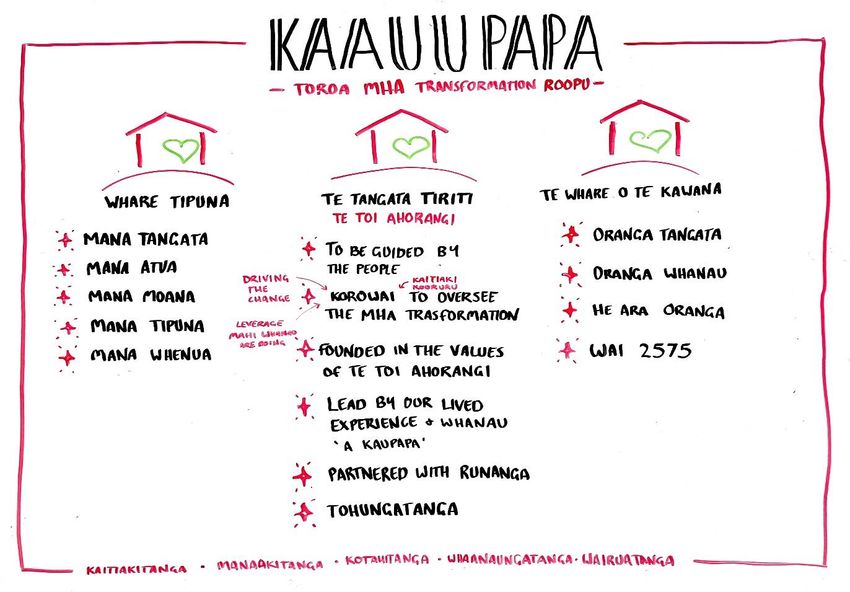
2.0 Prelude: Te Moana a Toi: Bay of Plenty Region
Transforming Mental Health & Addiction Services
“Te Toi Ahorangi describes the journey to achieving an authentic Tiriti partnership
and aspires for all accessing Mental Health & Addiction services,
becoming flourishing individuals and families”8.
In October 2019, Te Toi Ahorangi: Te Rautaki o Toi Ora 20309 was launched. Te Toi Ahorangi (TTA)
reflects the wellbeing aspirations for the descendants of Te Moana a Toi, of the 1810 Bay of Plenty iwi.
Its strategies when implemented well will benefit all communities and their members who reside
within Bay of Plenty rohe. With the intention of being the first Tiriti-led DHB, Bay of Plenty DHB Board
endorsed and adopted Te Toi Ahorangi. A key focus being a joint commitment to accelerate health
equity for Māori.
Bay of Plenty Mental Health and Addiction (MHA) Transformation Phase One
Communities need the opportunity to shape models of care so that they fit the (cultural and social)
needs of the communities they serve11.
Te Pare o Toi along with DHB Planning & Funding held consultation and information sharing meetings
with DHB and NGO MHA providers; Lived Experience and Whānau groups. This involved orientation
to Te Toi Ahorangi principles while hui participants confirm their priorities for MHA transformation
leadership group ideas12 Māori providers across Eastern and Western Bay of Plenty held their own
consultation meetings in August 2019 and September 2020, respectively.
Māori Lived Experience and Whānau Mentoring providers13 held their hui during December 2019 to
January 2020.
Orientation to Te Toi Ahorangi was highlighted in the Eastern Bay hui with one of their principles being
“action to drive change towards Te Toi Ahorangi, and recommendation 24, to establish a Te Toi
Ahorangi Cross Sector Governance Group led by Māori” (Eastern Bay [EB] Report, 2020, ps 7 & 10).
The substantial contributions made over the 2019 to 2020 years, signalled that Lived Experience,
whānau, hapū, iwi and communities were ready for further transformational re-design activities to
8 Te Rūnanga Hauora Māori o Te Moana a Toi leader, Whaea Rutu Swinton, September 2020).
9
Te Rūnanga Hauora Māori o Te Moana a Toi. 2019. Te Toi Ahorangi Te Rautaki a Toi Ora 2030
10 17 of the 18 Iwi in the Bay of Plenty are part of Te Runanga. Tuhoe is not, however Te Toi Ahorangi is for all 18 Iwi
11 Community Advocate in He Ara Oranga (HAO), 2018, p48.
12 DHB Planning & Funding Manager, Caleb Putt. July 2020. Minutes of DHB & NGO Provider Hui & Minutes of Lived
Experience Hui held in July 2020.
13 Te Pare Ō Toi. 2020. Lived Experience Report. BOPDHB. Tauranga. Rau o Te Huia Trust; Ngā Kākano Foundation &
Waiariki Whānau Mentoring views of ‘what transformation means to them’ are represented in this report.
commence and with expectations that whānau, lived experience and primary, secondary and community partners are to be leaders of transformation14. 14 See footnote 8
3.0 Phase II Community Consultation
He Ara Oranga: The Government Inquiry into Mental Health and Addiction Report15and
recommendations from the Wai 2575 Hauora claim are foundational to understanding the aspirations
for mental wellbeing of the communities and their peoples; whānau, hapū and iwi. He Ara Oranga
findings and Oranga Tāngata, Oranga Whānau; kaupapa Māori analysis of the Māori consultations16
prepared the ground for transformation of mental health and addiction services (MHAS) across the
nation.
Phase 2 consisted of a 6-months with the following events being undertaken:
1. Leadership and management of the MHA transformation programme shifted to Te Pare ō Toi
2. A Project lead was appointed in November 2020.
3. MHA transformation phase II project plan was developed, and key activities, that included:
a. setting up an Advisory / Steering group to advise the Project Lead on:
i. establishing & realising an Oversight Leadership Group, seminal to overseeing the progress
of all MHA transformational phases, and
ii. developing an agreed mahitahi approach for the Bay of Plenty.
Stage One
From December 2020 to March 2021 the Project Lead was introduced to and met with DHB, NGO and
PHO providers; Lived Experience & Peer Support Groups and Individuals; and Whānau groups. Two
main outcomes of these hui were to:
hear and receive the peoples’ kōrero on what transformation meant to them and,
invite and obtain participation in an Advisory Steering Group.
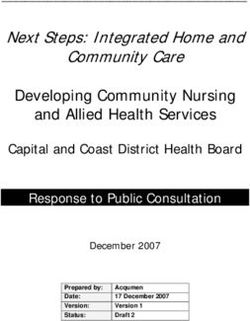
The conversations and discussions with the various groups and individuals were valuable. The
following visuals and summaries in this section provide an overview of some of the views shared. This
consultation journey began in Whakatāne at the Te Kāhui Kaumātua17 hui.
15 The Crown. 2018. He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction Inquiry. Office of
the Minister of Health: Wellington.
16 See Inquiry into Mental Health and Addiction. 2019. Oranga Tāngata, Oranga Whānau: A Kaupapa Māori Analysis of
Consultation with Māori for the Government Inquiry into Mental Health and Addiction. Department of Internal Affairs:
Wellington.
17 Project Lead notes of the information written during this hui held 16 December 2020.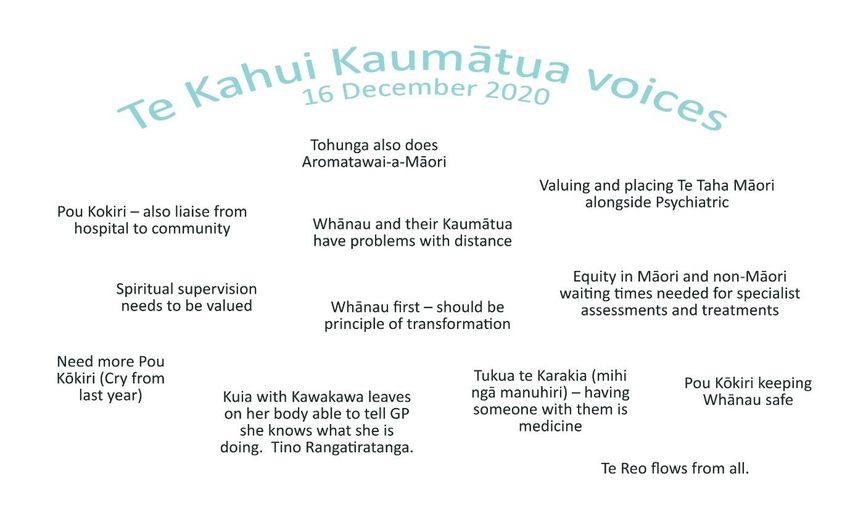
Main themes that came from Te Kāhui Kaumātua kōrero focused on what and how transformation could promote and provide cultural education and valuing of cultural safety for Whānau and cultural workers; appreciate Māori healing practices are vital to Māori wellbeing; reduce inequity in waiting times for Māori accessing specialist services and, Whānau first should be a principle of transformation. There was also a karanga (call) that more cultural workers are needed as their current workload is demanding and they cannot meet the need and the demand of whānau accessing services.
Lived experience voices came from two main sources – the BOPDHB Consumer Consultant Hui on February 1618, and from individual Lived Experience voices – participants from the Consumer Consultant hui came from across the BOP region and were employed by the DHB or NGO services such as Turning Point. They held roles in different areas, that is, general hospital services, quality and health team including mental health and addiction. They all had in common lived experience of experiencing mental distress and accessing and receiving mental health and addiction services. Key themes centered on their participation in transformation activities to build resilience as effective contributors, equitable services with a shift in distribution of power and an awareness of inclusion and connection as a network. There was strong support for Lived Experience as Leaders, for Te Toi Ahorangi and te Tiriti o Waitangi and for Rongoā Māori to be an accessible choice of care and treatment. Some individuals advocated training leading to learning a trade rather than periodic detention which they saw as futile. Kaupapa Lived Experience also are lobbying for their own regional leadership network to be set up and supported. 18 Information taken from Project Lead notes from the meeting.
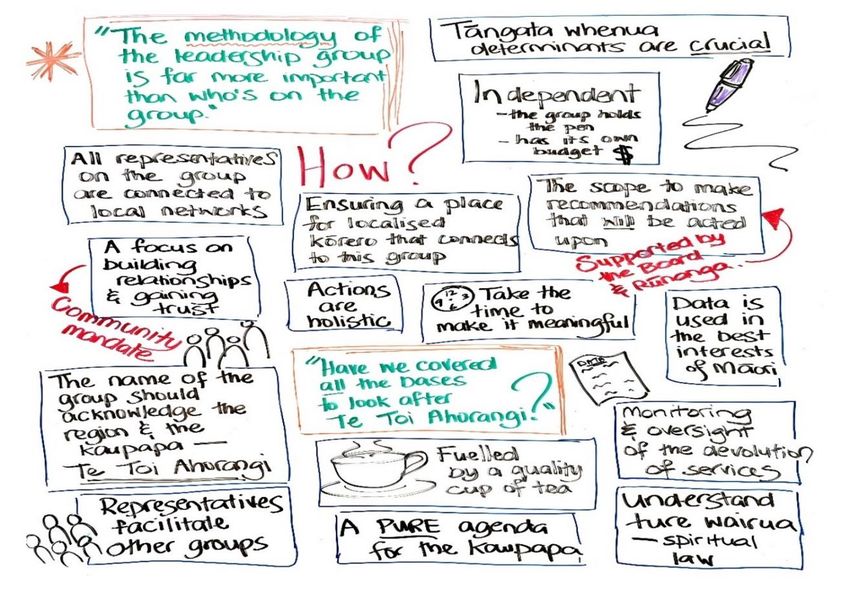
The views above were collated from separate hui held with Eastern Bay Primary Health Alliance and Ko Kollective of Opotiki and three other Whānau Support Services19, that is, Brave Hearts, Tauranga; Family Link, Tauranga; and Pou Whakaaro, Whakatane. Barriers identified included – current contracting arrangements hinder effective planning and job security; Whānau are excluded in their members’ continuum of care; lack of understanding addiction and, the ‘relationship’ recovery response needed by all; issues for Whānau getting access to necessary social services. 19Project Lead notes: Ko Kollective with EBPHA Hui 22.01.2021; Family Link Hui 18.02.2021; Pou Whakaaro Hui 19.02.21 Brave Hearts Hui 25.02.2021.
Transformation is rewiring of thinking, setting up a Whānau Support services network for integration
of services, increasing access to education; improving advocacy for Whānau and having their voices
heard too; strengthening relationships and connections; and more access to Māori and Pacific workers
to better cater for Whānau who access their services.
Peer Support workers came together in March20 at the Orchard Church venue in Te Puke to explore
opportunities on how to strengthen their networking. They shared concerns that as a group spread
across the region there was a lack of consistency in process, roles and responsibilities from
organisation to organisation who all employed peer support workers. They also spoke about being
conflicted in their roles at times, how hard it has been working for whānau with access to limited
resources and their own selves needing to attend to their workforce development needs. Yet they saw
the value of having their peer support roles.
“We see ourselves as a gateway to the community as we are able to access necessary resources like
accomodation for whānau and clients much more efficiently than other workforce groups”.
Forming a regional Peer Support network is ongoing and they are being assisted in this by the BOPDHB.
Community Consultation Prevailing Themes
Transformation is:
- To promote cultural education and cultural safety
- Appreciate Māori healing practises are vital to Māori wellbeing
- Waiting times for Māori to access specialists increases health inequity for Māori
- More cultural and peer support workers are needed
- Regional network forums need to be set up for Lived Experience, Peer Support Workers and
Whānau providers for better integration of services, to have each group’s voices heard and for
more inclusion in MHA planning, delivery, and monitoring.
- Outcome based contracts are preferred with 2 5 years duration.
20This information and the quote are taken from the Writer’s notes of the March 16 hui and minutes distributed after the
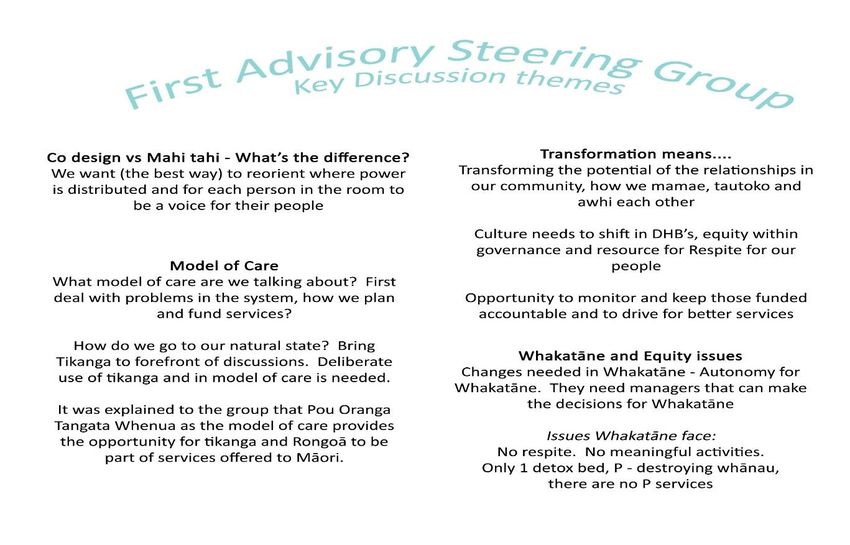
hui.Stage Two Hui One - Forming Advisory Steering Group The Meet & Greet consultation and information sharing hui were rewarding. Invitations were widely distributed across individuals, services and organisations requesting nomination for the membership of the Advisory Steering Group (ASG). Some provider representatives were put forward by their network groups to represent either the Eastern or Western Bay of Plenty. The first of four monthly meetings were held March 25th. Membership included a wide range of stakeholders who represented Lived Experience, Whānau/ Family, Primary Care, NGOs comprised of mainstream, Māori and Kaupapa Māori providers, DHB Secondary Service Leadership and Planning & Funding. The initial ASG membership size was to be 16. The first hui saw 11 of the 26 who attended were Lived Experience and Whānau / Family representatives; each representative had the option to share the responsibility with a nominated ‘other’ at alternative meetings. The ASG member’s comments have been listed below.
Hui Two – Reset - the Ministry of Health Draft Collaborative System Design Directive
The hui on April 30th respectively came to the ASG when the MOH draft Collaborative System Design
service specifications21 were introduced to the sector. As further commitment to support the BOP
MHA Transformation phase II, external facilitators were engaged to help assist ASG members to
understand why the increased pace of change was required.
The purposes of the two hui:
reflected on and acknowledged ASG members contributions to MHA transformation activities.
21 Ministry of Health. March 2021. Draft: Collaborative System Design. Ministry of Health: Wellingtonexplained the next steps motivating the transformation activities as per the MOH’s service
specifications and directive.
support embedding a collective understanding of leadership.
enabled ASG members to confidently hand the rākau over to the Cross-Sector leadership group to
be established in July, and
reinforced going forward, Te Toi Ahorangi principles continues to provide a sound foundation for
the mental health and addiction transformation activities22
Hui Two – Advisory Group Affirmed Key Cultural Themes23
“Te Toi Ahorangi affirms the different identities of all the iwi who have participated……Relationships
come first, second, last, always. It’s not negotiable.
22 April 30th Playback document written up by Price Waterhouse Cooper [PWC].
23 ASG members whakaaro whiteboard visual April 30th HuiMAPPING OUT THE ‘WHO’ FOR A CROSS-SECTOR LEADERSHIP GROUP24
To breathe life into Te Toi Ahorangi and establish a leadership group capable of that task, requires
thoughtful consideration of ‘who’ needs to be part of the membership of the group and ‘how’ the
group will function. Regarding the ‘who’25, the kōrero of the ASG reflected on the breadth of
representation that needs to be at the table - or connected to those at the table. To be effective,
the group’s membership needs to include iwi, lived experience (youth and adult, Māori and
Pākehā), community and whānau, non-clinical and clinical service delivery, cross-sector
representation, and a strong knowledge and understanding of te ao Māori, including mate Māori.
In addition to that breadth of representation, the group should also be enabled with the necessary
expertise in terms of system design, data insight, change management and communications. The
group should be flexible in its membership, co-opting specific expertise as and when required.
24 April 30 ASG members in discussion about “who” should participate on Oversight Cross Sector Leadership Group.
25 Price Waterhouse Cooper. 2021(a).Playback Document 30th April 2021, p10.Charting out the ‘how’ of the leadership group
“Have we considered all the bases to look after Te Toi Ahorangi?”26
The kōrero of the Advisory Group reflected on two key points in terms of the ‘how’27 of the leadership
group:
its methodology and level of influence; and
whether it was designed and enabled to deliver Te Toi Ahorangi.
Important aspects of how the group would function included:
● its mandate and autonomy;
● its connections and relationships; and
● a comprehensive and holistic scope; and substance over speed.
These characteristics will be key in determining the terms of reference of the group.
26Quote from April 30th hui by one of the participants
27
Price Waterhouse Cooper. 2021(a).Playback Document 30th April 2021, p11.Mā te Rongo Ake28 reported despite some positive changes occurring there remained in the sector
frustration as:
the disconnect between system-level change and the ongoing issues for people in the community
can be adding to a strong sense of frustration.
biomedical service models continue to dominate MHA systems while other service delivery
models such as Peer Support or Kaupapa Māori exist on the fringes.
Change the Clinically Dominated Silo Approach if that doesn’t change …
then nothing will.
While generally ASG members in Hui two achieved some very positive outcomes, the current systems
approach continued to produce barriers and not close gaps and they all agreed a different approach
is needed to make meaningful and helpful change. They had been on this journey of change for the
past 2 years since the new Health Reforms had been announced. They emphasized that language is
important and that voices must be heard. The disconnect between the system – level change was
28 See Mental Health and Wellbeing Initial Report, 2021, p21.evident from the kōrero that there is a disconnect on the language – level change. This prevailing
theme of the disconnect between the language level change raised itself in Hui Three.
Hui Three – With Hope Also Comes Frustration
The third ASG hui (May) was arranged following the expression from the ASG members that they
needed more time to articulate what the future Leadership team should look like. In the third hui
there was a strong contingent of Māori who attended, made up of Kaupapa providers, Lived
Experience and Whānau - some came as part of the original ASG membership and others came for the
first time on the day and many of them expressed deep frustration. They were initially open to kōrero
about the form and function of a leadership group but as the discussion evolved, frustration with what
was being asked of them became increasingly evident. The Group was clear that several significant
pieces of work by Māori stakeholders in the Bay of Plenty have been achieved through collaborative
design and set out the changes that are required to transform the system. Their core concerns were
‘Not being listened to, not being responded to effectively and not being adequately communicated to,
all sat at the core of their frustration’.
… Leaders aren’t always right
STOP Talking START Listening… It feels like we’re back at square 1!Just as there are different changes in currents to navigate while rowing a waka where some currents
are stronger than others and present more of a challenge than a smooth sail, it seems this too reflects
the six-month journey of Phase II. Also importantly change of currents provides rationale on why
change is necessary and acknowledgement of the frustration in this meeting needed to be made.
As expressed by ASG members:
Some of the local providers and individuals who have been on the journey for change for several
years felt they are still not being heard or responded to well, and
Communication of certain aspects of Phase II activities and response to matters that arose for
Kaupapa and Māori providers has not happened in timely and effective ways.
With Frustration Also Comes Hope
Language the Change is a key theme of the Western Bay Māori Provider Report of September 2020
and in this third hui, how and when language is used or not used could be considered as the core of
the providers’ frustration. By extracting from the words of the Kaupapa providers as expressed on thepage before, as not being listened to or not being adequately communicated to, and linking them to
‘are we as Māori and non-Māori still talking past each other after almost 200 years?’ If that is so, then
are we still looking at transformation from different lenses? Both examples are currently ongoing
barriers to achieving the change needed to achieve the goals of equity for Māori and improvements
for overall population health. If the disconnect between the language – level change is not corrected,
then genuine connections cannot be made and sustained.
During this exchange of views, the facilitators captured and noted that following the release of
frustrated opinions: “There was a rich and powerful kōrero about the role and function of a leadership
group …”29, which came from the kaupapa providers and Māori Lived Experience members.
The Mahi Tahi cultural concepts of whakapapa, whakamana, wānanga me haututū30 were actualised
with the issues raised. Acknowledgement was made that they were being heard and their kōrero
validated that their reports and respective recommendations held true for them in the present day as
they did 18 months ago. Tikanga Māori provided opportunity for Māori at this hui to present to the
group their view of what a Cross Sector Leadership Group within a Māori Framework could look like
and how it could function.
Te Toroa Cross Sectoral Leadership Group
“The Toroa and the 4 winds is the returning of the old knowledge,
systems, and bases”31.
29 PWC: Draft May 28 Hui Playback Document, ps 7 & 8.
30 See section 5 for a summary of Mahi Tahi (2021) as described by Graham Cameron, Pou Tikanga Te Pare Ō Toi, BOPDHB.
31 Name for proposed Kaauupapa Oversight Cross Sector Leadership Group, May 28 2021.Collectively the Kaupapa providers and Māori Lived Experience presented the following32:
● it will be named the “Toroa Mental Health and Addiction Transformation Leadership Group”
● it will ensure the kaupapa Māori Toi Oranga Ngākau MHA recommendations are implemented
● it will be guided by the people
● it will be a watchdog to oversee the mental health and addiction transformation activities are in
line with Oranga Tāngata, Oranga Whānau and He Ara Oranga
● it will be founded in the values of Te Toi Ahorangi
● it will be led by our lived experience and whānau a kaupapa
● it will be partnered with the Rūnanga
● its principles will be: Kaitiakitanga, Manaakitanga, Wairuatanga, kotahitanga, whanaungatanga
● it will uphold: mana tangata, mana atua, mana moana, mana tupuna, mana whenua
Matrix one below presents a collective view of a Leadership Group by those ASG members who
attended Hui two (April). By comparison both Leadership models have aspects to offer to each other
– both acknowledge te ao Māori and Te Toi Ahorangi and the importance of relationships,
32
PWC: Draft May 28 Hui Playback Document, p 13.connections, mandate, and autonomy. Both models claim holism in their scope. The Kaupapa model
though is grounded in Te Toi Ahorangi, and tikanga values, principles and te ao Māori worldviews and
expertise, while western concepts and expertise feature in the Hui 2 discussions. What is as important
as these views presented on these two pages is which suggested model will be able to achieve the
Ministry of Health’s main aims more readily to collaboratively progress towards achieving the goals of
equity for Māori and improvements for overall population health?
Matrix 1: Hui Two – A Collective View of Key Points for a Cross Sectoral Leadership Group33
The ‘Who The ‘How’
The group’s membership needs to include iwi, The kōrero of the Advisory Group reflected
lived experience (youth and adult, Māori and on two key points in terms of the ‘how’34 of
Pākehā), community and whānau, non-clinical and the leadership group:
clinical service delivery, cross-sector its methodology and level of influence;
representation, and a strong knowledge and and
understanding of te ao Māori, including mate whether it was designed and enabled to
Māori deliver Te Toi Ahorangi.
The group should also be enabled with the Important aspects of how the group would
necessary expertise in terms of: function included:
- system design ● its mandate and autonomy;
- data insight ● its connections and relationships; and
- change management, and ● a comprehensive and holistic scope; and
- communications. ● substance over speed.
The group should be flexible in its membership, co- The characteristics in the matrix frame above
opting specific expertise as and when required will be key in determining the terms of
reference of the group.
Going forward, all group members engaged well, and shared discussions was animated. There was an
atmosphere of positive inquiry. The proposed Framework for a Te Toroa Cross Sector Leadership
would have three key areas of responsibility – to oversee MHA transformation activities; to monitor
those activities in meeting the goal of health equity for Māori; and to drive the changes the people
want to see.
33 See Price Waterhouse Cooper. 2021(a).Playback Document 30th April 2021, ps 10 & 11 for table contents
34 Price Waterhouse Cooper. 2021(a).Playback Document 30th April 2021, p11.Overall, in this third hui the ASG identified opportunities and challenges for progress35.
Opportunities for the MHA Programme Leadership
- to take the opportunity to review the aforementioned documents and the ideas put forward for
service and system transformation.
- rather than looking to create a new structure for the next phase, consider how existing structures
and networks can be utilised.
The group were clear that there were many effective partnerships that addressed the issue of silos
and there is merit in capitalising on effective relationships. Given that the group agreed on the
function of the leadership group component, the DHB – Te Rūnanga and Whare Waka programme
executive could consider how existing groups form the ‘sub-group’ structure.
Challenges
moving forward without responding to previous mahi highlighted above, could risk alienating
stakeholders, and potentially result in a lack of endorsement of proposals that stem from a
collaborative design process.
Considerations
collaborative design process - the existing consultation reports cited by the Māori Roopū places
the DHB and Rūnanga in a strong position in terms of the required collaborative design process,
with potentially a significant body of work already undertaken.
It would be beneficial to review and map the substance of those proposals. That detail could be used
to develop the framework of a transformation plan, with a collaborative design process used to
(1) attend to any ‘gaps’ and
(2) explore and determine a greater level of detail (if required).
Composition of the leadership group – the April wānanga resulted in several recommendations for
composition of the group. Given that the DHB sees the group as the ‘delivery’ waka to effect the
changes proposed by sub-groups (or in this case, potentially the proposals outlined in the local Māori
consultation documents in section two), the leadership group could be limited in its size with a focus
on a membership comprised of individuals/organisations who have the decision-making ability across
the sector.
35PriceWaterhouseCooper (PWC) Facilitation Team wrote up this summary which has been left in its wholeness. Playback
documents of ASG Hui held April 30 & May 28, 2021.The leadership framework could potentially comprise two parts - (1) design and (2) delivery - with a
different membership structure connected to each.
The ‘design’ aspect could have a clear link to the sub-group structure of existing groups. There was a
strong and repeated message regarding Lived Experience as leaders, which will warrant further
consideration as to how best to enable that in this process.
Communication and next steps - before moving into the next phase, the DHB and Rūnanga should
consider a communication and engagement strategy that sets out the position regarding the
documents highlighted by this group, and if and how that mahi will be incorporated into this next
phase of this kaupapa.
Prevailing themes – Section Four
Three ASG hui held and each hui held its own challenges related to the journey of expectations
since the new Health Reforms have been ushered in and then to a reset by the MOH to increase
the pace for transformational change.
In preparing for a Cross Sectoral Leadership Group, Hui 2 and Hui 3 saw participant collective views
shared and compared – both sets of views have merit and much to offer a Leadership Group to
achieve the MOH equity goals for Māori and the overall population.
Doing things differently and autonomously seem to be underlying factors in the ASG activities.
Language the Change – the disconnect between the language – level change is a barrier and that
is important to acknowledge and to correct to enable genuine relationships and connections are
made and sustained to improve relationships and trust between Māori and non- Māori.
Te Toroa Cross Sector Leadership Group model framed within Te Ao Māori is proposed as the
model to oversee, monitor, and drive MHA transformations in Bay of Plenty. There was a
consensus to support this model.
Recommendations for implementation of Cross Sector Leadership moving forward alert to risks,
opportunities, challenges, and considerations.
Appropriately addressing issues raised by Māori Providers of not being listened to or
communicated to effectively should be included in the plan going forward.4.0 Conclusion
The peoples of Te Moana a Toi, Bay of Plenty journeys to transform mental health and addiction
services has seen a series of ‘resets’ and ‘reframing’ in their ways of thinking, expressing and doing.
Key documents of He Aranga Oranga, Te Toi Ahorangi and the Ministry of Health’s Collaborative
System Design, feature as to who to focus on, what to focus on and how those priorities are to be
rolled out. Te Tiriti o Watangi and key principles of health equity, options, partnership, participation
and active protection underline all key documents. Whakamaua and Kia Kaha hold the responsibility
of keeping Mental Health and Addiction (MHA) services and their leaders and workforce groups to the
kaupapa of the longer term transformation pathway for mental wellbeing in Aotearoa.
It is asserted that Te Toi Ahorangi like ngā whetū (the stars) and the constellation of Matariki, supports
Te Moana a Toi, Bay of Plenty (BOP) peoples to remain on course. Te Kōhao36 o te Waka o Toi is the
strategic platform from which Māori and non-Māori leaders work together to achieve change. It is also
at this forum that the transformation of Mental Health and Addiction services across the Bay of Plenty
is currently governed.
This report has illustrated that the MHA transformation Phase II journey at times has been complex
and comprehensive. Peoples’ willingness to engage and share their views and in many cases continue
to see Phase II complete this part of the MHA transformation activities is commendable. Te Toi
Ahorangi like Matariki ushers in new opportunities, time to reflect, partnerships to be cemented, new
partnerships to be made and or renewed. Importantly in keeping with Matariki, the considerations
and prevailing themes that are in sections 3 and 4 require attention prior to the plan moving forward
into MHA Transformation Phase III.
The experiences gained and shared throughout the transformation have confirmed that for effective
transformation activities to achieve the national goals all must work together – (i) achieving health
equity for Māori and (ii) Improved population wellbeing and Te Toi Ahorangi’s vision of Toi Ora
flourishing descendants of Toi. Māori or non-Māori cannot do these transformational changes alone
– being people and environment centred, developing our leaders, providers and workforce, effective
communication and negotiable and trusting partnerships are key enablers. In moving forward let us
all move together.
“Te ara tawhāiti o Tāwhaki
In the now is the pathway of all time”37
36 See Te Toi Ahorangi Te Rautaki a Toi Ora 2030, ps 15 & 17: www.bopdhb.health.nz/te-toi-ahorangi-2030
37 See Te Toi Ahorangi Te Rautaki a Toi Ora 2030 opening pages.Appendices One: Mental Health & Addictions Transformation Phase II Advisory Steering Group Members
Project Lead: Louise Ihimaera
REPRESENTATION OF AREAS INDIVIDUALS
Tikanga Tautoko Pou Tikanga/ Ruahine/ Pou Kokiri
Interim Chair Dr David Chaplow
BOPDHB Caleb Putt
Stewart Ngatai
Mainstream MHAS Secondary Services Jen Boryer, Fiona, Andrew Neas (Maximum of two attending)
Eastern Bay Primary Health Alliance (EBPHA) Jamie Sullivan
Ngā Mataapuna Oranga Primary Health Cindy Mokomoko (For information purposes)
Organisation (NMO)
Māori providers Ngāti Ranginui – Roy Nathan
Ngā Kākano – Ripeka Armstrong; Rutu Swinton-Maxwell
Ngāti Kahu – Fred Hika; Wirepo Brown
Eastern Bay Iwi Alliance - Peta Ruha
Mainstream service Hamner Clinic – Jill Knowles
Vincent House – Jeff Orr
HealthCare NZ – Vanessa Kirk
Lived experience Margaret Gunderson
Vaughn Cruickshank
Tarnia McCall
Arana Pearson
Patricia Bennet
Whānau Family Link - Brian Thomas
Brave Heart – David Benton
Pou Whakaaro - Claire Pye, Tangi,
Ko Kollective - Shannon HanrahanMental Health & Addictions Transformation Phase II Contributors
Whānau Tautoko Rebecca Chaplow BOPDHB Te Pou Kōkiri Whakatāne Te Reinga Kingi-chase
EBPHA CEO Greig Dean Pou Whakaaro Peer Support James Pilkington
EBPHA/ Poutiri Trust Ray Wihapi Pou Whakaaro Peer Support Dennise Neho
Cultural/ Whānau Ora Advisor
Emerge Aotearoa Manager Pip Lee Te Pou Oranga o Whakatōhea- CEP Anau Apanui
Clinician & Practice Leader
Poutiri Trust Cultural Advisor Karam Hood Te Whānau a Apanui – WO ManagerRichard McDonald
BOPDHB Consumer Advisor MH Patricia Bennett Te Tohu o Te Ora o Ngāti Awa- Rachel Morris
Health Services Manager
Pacifica Lived Experience Ngaoa Marsters Te Tohu o Te Ora o Ngāti Awa Matetu Mihinui
Lived Experience Cultural Advisor Julie Stewart Te Tohu o Te Ora o Ngāti Awa Orini Marr
BOPDHB Toitiaki ki Whakatāne Frances Te Kani Tūwharetoa Ki Kawerau Jarno Savage
BOPDHB Te Pou Kōkiri - Tauranga Hineira Hamiora Tūwharetoa Ki Kawerau Tayna Kanekane
BOPDHB Te Pou Kōkiri Whakatāne Paora Morunga Tūwharetoa Ki Kawerau Bree Soloman
BOPDHB Te Pou Kōkiri Whakatāne Rawiri Keepa
BOPDHB Te Pou Kōkiri Whakatāne Stan RatahiAppendix Two
ME MAHI TĀTOU MŌ TE ORANGA O TE KATOA
WE MUST WORK TOGETHER FOR THE WELLBEING OF ALL
COMMITMENT TO THE SEVEN WELLBEING PRIORITIES38
The government needs to commit to seven wellbeing priorities across the
spectrum – to prevent, respond to, and lessen the impact of mental
distress and addiction. All people:
1. Live in social conditions that enable to them to look after their own and
each other’s wellbeing.
2. Know how to recognise and respond to stress, distress, and addiction.
3. Can easily find services and supports for people with distress and
addiction.
4. Get timely, respectful, and helpful responses from them.
5. Have access to a comprehensive range of community-based services
and supports.
6. Are supported by people who have ‘walked in their shoes’ as well as
professionals.
7. Are enabled to reconnect with themselves, their whānau, and valued
roles in their communities.
38
O’Hagan, Mary. 2018. Wellbeing Manifesto for Aotearoa New Zealand (p3). A submission to the
Government Inquiry into Mental Health and Addiction. Prepared for PeerZone and ActionStation
https://www.wellbeingmanifesto.nz (accessed May 28 2021).5.0 References Cameron, G. October 2020. Decision Paper: Mental Health and Addiction Transformation. Prepared for Bay of Plenty District Health Board Executive Committee. For and behalf of Te Pare Ō Toi and the Mental Health Transformation Programme. Bay of Plenty District Health Board: Tauranga: Bay of Plenty. Department of Internal Affairs. (2019). Inquiry into Mental Health and Addiction. Oranga Tāngata, Oranga Whānau: A Kaupapa Māori Analysis of Consultation with Māori for the Government Inquiry into Mental Health and Addiction. Department of Internal Affairs: Wellington. Dewes, Kuru Marama. Monday May 22nd 2017. Interview: Rangi Mātāmua Hopes to Revive Māori Astronomy. https://www.teaoMāori.news/dr-rangi-matamua-hopes-revive-Māori-astronomy (Accessed: May 28, 2021) Fairman, Steve. Blog: Transformational change – a call to action. Managing Director of NHS Improving Quality. England, United Kingdom. Retrieved: May 28, 2021. https://nhsiq.wordpress.com/2014/07/23/transformational-change-a-call-to-action/ Health Quality & Safety Commission. 2019. Window 2019: A Window on The Quality of Aotearoa New Zealand’s Health Care 2019: Foreword Professor Sir Mason Durie. Wellington: Health Quality & Safety Commission. Keane, Basil. 2012. He Whakaputanga – Declaration of Independence, Te Ara – the Encyclopedia of New Zealand. Retrieved June 2, 2021. https://teara.govt.nz/en/he-whakaputanga-declaration-of- independence (Accessed June 2, 2021) Leakey, Cameron. (2020). Craccum speaks to Dr. Diana Kopua. An indigenous approach to mental health that incorporates mātauranga Māori and Te Ao Māori. Craccum University of Auckland Student Magazine. Auckland: New Zealand. http://craccum.co.nz/features/mahi-a-atua-a-Māori-approach-to- mental-health/ (Accessed May 24, 2021) Mental Health Foundation of New Zealand. (2019a). Emphasise hope and make it happen Response to He Ara Oranga from the Mental Health Foundation of New Zealand. Auckland: Mental Health Foundation of New Zealand.
Mental Health Foundation of New Zealand. (2019b). MHF statement on the Government’s response to He Ara Oranga. Auckland: Mental Health Foundation of New Zealand. Retrieved from: Mental Health Foundation of New Zealand. https://mentalhealth.org.nz/news/post/mhf-statement- on-the-governments-response-to-he-ara-oranga (Accessed September 10, 2020) Mental Health and Wellbeing Commission. 2021. Mā te Rongo Ake: Through Listening and Hearing: Initial Report. Wellington: Mental Health and Wellbeing Commission. Ministry of Health. (2014). The Guide to He Korowai Oranga – Māori Health Strategy. Wellington. Ministry of Health. Ministry of Health. (2018). Mental Health and Addiction Workforce Action Plan 2017–2021 (2nd ed). Wellington: Ministry of Health. Ministry of Health. 2020a. Kia Kaha, Kia Māia, Kia Ora Aotearoa: COVID-19 Psychosocial and Mental Wellbeing Plan. Wellington: Ministry of Health. Ministry of Health. 2020b. Whakamaua: Māori Health Action Plan 2020–2025. Wellington: Ministry of Health. Ministry of Health. 2021. Draft: Collaborative System Design. Wellington: Ministry of Health. Neilson, Michael. 2021.The New Zealand Herald. Māori Health Authority: Sir Mason Durie to head new Government advisory group. Auckland: The New Zealand Herald. Retrieved from The New Zealand Herald: https://www.nzherald.co.nz/nz/Māori-health-authority-sir-mason-durie-to-head- new-government-advisory-group/5OT52SK2B7KMMLOTVM2SUNMF5U/ O’Hagan, Mary. 2018. Wellbeing Manifesto for Aotearoa New Zealand (p3). A submission to the Government Inquiry into Mental Health and Addiction. Prepared for PeerZone and ActionStation https://www.wellbeingmanifesto.nz (accessed May 28 2021). Ruha, Peta. (2019). Toi Oranga Ngākau. Kaupapa Māori Mental Health & Addictions and Re-Design Report. Toi Ora Māori Health Gains & Development Unit, Bay of Plenty District Health Board. Tauranga, New Zealand.
The Crown. (2018). Inquiry Panel. He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction. The Crown. Wellington: New Zealand. Te Pare ō Toi. 2020. Lived Experience Report: Transforming and Moving Bay of Plenty Mental Health and Addiction Services into the 21st Century. Bay of Plenty District Health Board. Tauranga. Te Pare ō Toi. No date (n.d.). Unpublished Document prepared by Graham Cameron: Mahi Tahi Process. Bay of Plenty District Health Board. Tauranga. Te Rūnanga Hauora Māori ō Te Moana a Toi. (2019). Te Toi Ahorangi: Te Rautaki a Toi Ora 2030. Te Moana a Toi: Aotearoa New Zealand. Te Rūnanga Hauora ō Te Moana a Toi. 2007. He Pou Oranga Tangata Whenua: Tangata Whenua Determinants of Health Framework. Te Moana a Toi: Bay of Plenty.
You can also read