What Will Become Of The Medical Mecca? Health Care Spending In Massachusetts
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Te a c h i n g Hospi tals
What Will Become Of The
Medical Mecca? Health Care
Spending In Massachusetts
Do the benefits of a concentrated academic medical infrastructure
justify higher health spending?
by Robert E. Mechanic
ABSTRACT: Massachusetts has been called a “medical mecca.” It has also been called
the world’s most expensive health care market. This paper concludes that claims of excess
costs in Massachusetts are overstated. Massachusetts hospitals have lower inpatient
costs than peer institutions in other states, yet the state’s concentration of academic hos-
pitals tilts the system toward higher spending. In markets like Massachusetts, there is grow-
ing pressure to demonstrate tangible benefits to justify the additional costs of academic
health centers (AHCs). Applying new information technologies to proactively manage pa-
tients with expensive chronic illnesses is a critical area for future collaboration between
payers and AHCs.
M
a s s ac h u s e t ts h a s b e e n c a l l e d a “medical mecca.” It is home to
some of the nation’s most prestigious teaching hospitals and medical
schools and a place where state-of-the-art clinical services and ground-
breaking scientific discoveries are a source of civic pride. Spurred by reports with
titles such as The World’s Most Expensive Hospitals, though, many view the Massachu-
setts health care system as wasteful and inefficient.1 This perception is bolstered
by commonly cited national data sources that show per capita hospital and health
spending in Massachusetts to be far above the national average. But users of these
data typically fail to control for important market characteristics such as high la-
bor costs or the substantial hospital-based medical research costs that are not
borne by patients or health plans. This paper examines a range of health spending
data sources and concludes that differences between Massachusetts and other re-
gions are far less than have been previously asserted. It also finds that Massachu-
setts hospitals actually have lower average costs than peer institutions in other
states.
Health care spending in Massachusetts is influenced by the state’s unique mar-
Rob Mechanic is director of Robert Mechanic and Associates, a health care management consulting firm in
Cambridge, Massachusetts. From 1998 through 2000 he was senior vice-president of the Massachusetts Hospital
Association.
130 November/ December 2003
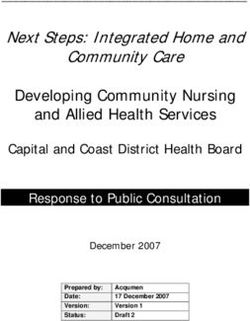
DOI 10.1377/hlthaff.22.6.130 ©2003 Project HOPE–The People-to-People Health Foundation, Inc.Massachusetts Ho spital s ket structure. With four medical schools and six academic health centers (AHCs), in a state with six million residents, Massachusetts has one of the largest concen- trations of academic medicine in the country.2 A decade ago the prevailing theory was that managed care would draw patients away from more costly teaching hos- pitals, but AHCs in Massachusetts have actually gained market share. This creates vexing questions for policymakers: first, whether the potential benefits of a con- centrated academic medical infrastructure—quality of care, economic develop- ment, or academic missions—justify higher health care spending; second, whether market competition will promote appropriate use of community-based health re- sources; and finally, whether academic systems will be able to develop compara- tive advantages in health care informatics and chronic disease management that could slow long-run health care spending growth while improving quality. This paper first examines the assertion that Massachusetts has the world’s most expensive health care system. It reviews changes in the market during the 1990s and examines comparative regional spending measures. Then, because con- tinued double-digit health spending growth is unsustainable, it examines how ac- ademic health systems, health plans, and purchasers might address long-run affordability issues. Competition Comes To Massachusetts In December 1991 the Massachusetts legislature signed a bill into law to dereg- ulate the state’s hospital pricing system, freeing institutions to negotiate with in- surers. Thus began an era of aggressive competition, consolidation, and down- sizing across the hospital sector.3 Between 1991 and 2001 Massachusetts hospitals closed beds and reduced inpatient utilization faster than the rest of the country (Exhibit 1). By 2001 inpatient utilization had declined to the national average, al- though outpatient utilization remained high. Consolidation was not limited to hospitals. A wave of health plan mergers left three dominant health plans. By 2002 Blue Cross and Blue Shield of Massachu- setts, Tufts Associated Health Plan, and Harvard Pilgrim Health Care controlled approximately 75 percent of the private health insurance market.4 While most plan members are in some form of managed care, the three major insurers offer broad provider networks in which enrollees typically exercise free choice of doc- tors and hospitals without financial consequences. Because of this, health plans’ cost containment has focused primarily on controlling medical prices. As health maintenance organization (HMO) enrollment grew, Massachusetts hospitals, anxious not to be left out of provider networks, came to the table ready to bargain. A feeding-frenzy atmosphere was fueled by expectations that capita- tion would become a dominant form of reimbursement. In 1996 the state’s largest insurer, Blue Cross and Blue Shield, lost $90 million and began to pursue substan- tial rate reductions from contracted hospitals.5 At the time, hospitals could offer deep discounts because of earnings on Medicare business.6 By 1999 Massachusetts H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 131
Te a c h i n g Hospi tals
EXHIBIT 1
Change In Utilization And Capacity In Massachusetts And U.S. Community Hospitals,
1991–2001
Massachusetts United States
1991 2001 % Change 1991 2001 % Change
Hospitals 101 80 –20.8 5,342 4,908 –8.1
Beds (thousands) 21 16 –23.8 924 825 –10.6
Admissions (thousands) 821 766 –6.6 31,084 33,813 8.8
Inpatient days (thousands) 5,771 4,382 –24.1 222,964 194,106 –12.9
Outpatient visits (thousands) 10,647 18,778 76.4 322,048 538,480 67.2
Length-of-stay (days) 7.0 5.7 –18.6 7.2 5.7 –20.8
Area population 6,022 6,379 5.9 253,493 284,797 12.3
Beds per 1,000 3.6 2.6 –28.0 3.6 2.9 –20.4
Admissions per 1,000 136.4 120.2 –11.9 122.6 118.7 –3.2
Days per 1,000 958 687 –28.3 880 682 –22.5
Visits per 1,000 1,768 2,944 66.5 1,270 1,891 48.8
SOURCE: American Hospital Association, Hospital Statistics, 1992 and 2003.
NOTE: Massachusetts data include 26,473 net admissions by out-of-state residents after subtracting out-of-state admissions
by Massachusetts residents.
hospital reimbursement from private payers was estimated to be 4 percent below
the cost of services, compared with the U.S. average of 12 percent above cost.7
Excess capacity and the negotiating power of the state’s “big three” insurers
kept payments flat through the late 1990s. The federal Balanced Budget Act of 1997
placed additional pressure on hospital revenues. Both community and teaching
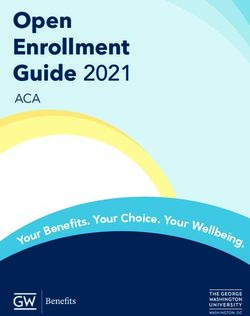
hospitals were forced to become more efficient. By 2000 average Medicare inpa-
tient costs per discharge for the state’s AHCs, major teaching hospitals, and com-
munity hospitals were 8–16 percent lower than peer hospitals nationally (Exhibit
2).8 Prior analyses have also shown Massachusetts hospitals to be more efficient
than their peers, based on multivariate regression models.9
However, 47 percent of Massachusetts hospital inpatient days are in AHCs or
major teaching hospitals, compared with a U.S. average of 21 percent. AHC and
major teaching hospital costs are much higher than those of nonteaching commu-
nity hospitals.10 Despite lower average costs within each peer group, the mix of
hospitals tilts the Massachusetts system toward higher overall spending.
Developing More Accurate Regional Cost Comparisons
Many analysts use per capita health spending as an indicator of the comparative
health system efficiency across geographic areas. This is problematic in Massa-
chusetts. First, the high concentration of academic hospitals and physicians re-
sults in a health care “product” that is distinct from the U.S. norm. Second, Massa-
chusetts hospitals face higher input prices than those in most other regions.
Finally, a variety of “accounting issues” related to hospital-based clinical research
results in national data showing higher costs than those actually borne by Massa-
chusetts patients and payers. Data sources commonly used to evaluate variation in
132 November/ December 2003Massachusetts Ho spital s
EXHIBIT 2
Medicare Inpatient Operating Costs Per Discharge, By Hospital Category (Urban
General Acute Care Hospitals with 100+ Beds), Fiscal Year 2000
Unadjusted costs ($)a
Massachusetts U.S. % Difference
Academic health centerb 9,796 10,307 –5.0
Major teaching hospitalc 7,068 8,322 –15.1
Other teaching hospitald 5,296 7,090 –25.3
Nonteaching hospital 5,198 6,334 –17.9
Case-mix- and wage-adjusted costs ($)e
Academic health center 5,139 5,567 –7.7
Major teaching hospital 4,461 5,007 –10.9
Other teaching hospital 3,870 4,571 –15.3
Nonteaching hospital 4,090 4,519 –9.5
SOURCE: Author’s analysis of Medicare FY 2000 (PPS-17) Medicare Cost Report data from the Centers for Medicare and
Medicaid Services (CMS) Hospital Cost Report Information System (HCRIS).
a
Medicare inpatient operating costs include capital costs but exclude direct graduate medical education. Costs are adjusted to
reflect a common base year (1 October 1999–30 September 2000) using the CMS hospital market basket index.
b
Association of American Medical Colleges–designated integrated academic health centers (AHCs).
c
Hospitals with 25 or more residents per 100 staffed beds (excluding AHC hospitals).
d
Hospitals with 1–24 residents per 100 staffed beds.
e
Wage adjustments were calculated by dividing labor portion of costs by Medicare geographic wage index prior to
reclassifications or application of rural floors. Adjustments assume labor costs account for 51.2 percent of Medicare inpatient
operating costs. Capital costs were adjusted using Medicare’s geographic adjustment factor. Wage-adjusted costs were
divided by hospital-specific case-mix index as reported in the Federal Register.
regional health care costs include (1) hospital expenses; (2) personal health care
spending; (3) Medicare spending; and (4) employer health insurance premiums.
n Hospital expenses. On an unadjusted basis, data from the American Hospital
Association (AHA) annual survey show 2001 Massachusetts per capita hospital ex-
penses to be 40 percent above the U.S. average. This difference falls to 11.6 percent
with several adjustments to improve data comparability (Exhibit 3).
Research grants. In 2001 Massachusetts institutions received nearly five times the
national average in research awards from the National Institutes of Health (NIH)
per state resident. Most NIH grants are awarded to medical schools and universi-
ties and are not reflected in hospital budgets. But Massachusetts hospitals re-
ceived more than $700 million in NIH funding. Private contracts elevated
hospital-based research funding to more than a billion dollars.11 These research-
related revenues and expenses are reported on hospital income statements and on
the AHA annual survey. Yet research costs are not borne by the Massachusetts res-
idents who make up the “denominator” of the per capita spending calculation.
Comparing patient revenue rather than total hospital expense is one way to filter
out research costs.
Out-of-state revenues. In 2001 more than 26,000 net out-of-state patients were
treated in Massachusetts facilities. AHA statistics reflect the location of hospitals
H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 133Te a c h i n g Hospi tals
EXHIBIT 3
2001 Hospital Per Capita Expense Versus Payments For Patient Care Services In
Massachusetts And U.S. Hospitals
Massachusetts ($) U.S. ($) % Difference
Per capita expensea 1,890 1,347 40.3
Difference between total expense and
patient revenueb –271 –46
Per capita patient revenuea 1,619 1,301 24.4
Out-of-state patientsc –50 0
Medicare IME/GMEd –57 –21
Wage and case-mix differencee –98 –12
Adjusted per capita patient revenue 1,414 1,268 11.6
SOURCES: Author's calculations based on American Hospital Association (AHA) annual survey data; and see below.
a
AHA, Hospital Statistics, 2003.
b
Reported nonpatient revenue per capita was $276 for Massachusetts and $106 for U.S. hospitals.
c
Net patient migration factors from A. Martin et al., “Health Care Spending during 1991–1998: A Fifty-State Review,” Health
Affairs (July/Aug 2002): 112–126.
d
1999 Medicare indirect medical education (IME) and graduate medical education (GME) payments from Centers for Medicare
and Medicaid Services (CMS) Hospital Cost Report Information System (HCRIS).
e
Wage adjustment uses 2003 Medicare geographic wage index (1999 data) of 1.1234 to adjust labor-related hospital
expenses. Medicare case-mix index from Federal Register. Weighted average case-mix applied to inpatient cost.
rather than patients’ state of residence. Per capita hospital expenses should be ad-
justed to reflect the net flow of patients across state boundaries. Massachusetts
hospitals also received $360 million in 2001 Medicare graduate medical education
(GME) payments, nearly three times the per capita average nationally.
Labor costs and input prices. Hospital wages in Massachusetts are about 12 percent
above the U.S. average.12 Medicare recognizes that wage levels affect variation in
hospital costs and adjusts payments to reflect these differences. General costs of
doing business are also high—Boston’s cost of living is 37 percent above the U.S.
average.13 These factors must be acknowledged in regional hospital cost compari-
sons.
n Personal health spending. Estimates developed by the Centers for Medicare
and Medicaid Services (CMS) show that 1998 Massachusetts personal health ex-
penditures were 28 percent above the U.S. average.14 The estimates are not intended
to include medical research, but because they incorporate total hospital revenues
from the AHA survey, more than a billion dollars in Massachusetts research-related
funding is included.15 The CMS also does not adjust for wage differences across
states. Exhibit 4 presents personal health expenditures for Massachusetts and the
United States by type of service. It also calculates the impact of removing
nonpatient hospital revenues and adjusting for geographic wage differences. With
these modifications, per capita Massachusetts personal health spending declines to
19.3 percent above the U.S. average, and per capita hospital spending declines to 11.4
percent above average.
n Medicare spending. There is less variation in Medicare spending across
states because Medicare statistics reflect an insured patient population and a uni-
134 November/ December 2003Massachusetts Ho spital s
EXHIBIT 4
Personal Health Care Expenditures In The United States And Massachusetts, By
Spending Component, 1998
Home Nursing
Total Hospital Physician health home Drug Other
United States $3,759 $1,405 $1,095 $108 $325 $451 $374
Massachusetts $4,810 $1,807 $1,316 $167 $573 $469 $479
Difference 28.0% 28.6% 20.2% 54.6% 76.3% 4.0% 28.1%
Adjusted for non-patient-
related hospital spendinga
United States $3,630 $1,277 $1,095 $108 $325 $451 $374
Massachusetts $4,478 $1,470 $1,316 $167 $573 $469 $479
Difference 23.3% 15.1% 20.2% 54.6% 76.3% 4.0% 28.1%
Adjusted for area wage
differencesb
United States $3,630 $1,277 $1,095 $108 $325 $451 $374
Massachusetts $4,330 $1,423 $1,274 $162 $555 $469 $464
Difference 19.3% 11.4% 16.3% 49.6% 70.6% 4.0% 23.9%
SOURCE: A. Martin et al., “Health Care Spending during 1991–1998: A Fifty-State Review,” Health Affairs (July/Aug 2002):
112–126. Data from the Centers for Medicare and Medicaid Services (CMS) are adjusted for patient migration. Other
adjustments are author’s calculations.
a
The national health expenditures (NHE) hospital spending estimate is based on total revenue reported in the American
Hospital Association (AHA) annual survey. The nonpatient spending adjustment subtracts 1998 hospital nonpatient revenue
per capita and Medicare indirect medical education (IME)/graduate medical education (GME) payments.
b
Wage adjustments based on Medicare hospital wage index weighted across all Massachusetts regions (1.1234). Adjustment
assumes labor-related share of 51.2 percent based on 2001 AHA annual survey data.
form national payment structure. Medicare data are adjusted for state border cross-
ing and do not include research grants. Precise comparisons of Medicare spending
per beneficiary can be made with data published in the Dartmouth Atlas of Health Care,
which adjusts fee-for-service Medicare reimbursements for age, sex, race, illness,
and local price factors. It analyzes data from hospital referral regions—geographic
units that reflect where patients actually receive care—which are more appropriate
for regional comparisons than political boundaries. Exhibit 5 shows 1996 Medicare
spending per beneficiary in twelve hospital markets that are top recipients of NIH
research funding. Compared with the twelve-region average, total Medicare spend-
ing for Boston is 7 percent higher, inpatient spending is 4 percent lower, hospital
outpatient spending is 24 percent higher, and professional and laboratory spending
is 9 percent lower. Taken together, the combination of outpatient and professional
spending in Boston is nearly identical to the twelve-region average. Therefore, high
hospital outpatient use may reflect a “substitution” for services delivered in physi-
cians’ offices or clinics in other regions.
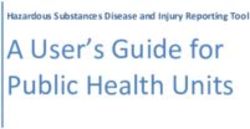
n Insurance premiums. Insurance premiums are the most direct health care
outlay for businesses and consumers. The Agency for Healthcare Research and
Quality’s (AHRQ’s) Medical Expenditure Panel Survey (MEPS) publishes data on
health insurance premiums from more than 29,000 establishments. In 2000, family
premiums in Massachusetts firms with fifty or more workers were 5 percent above
the U.S. average, while single-coverage premiums were 1 percent below the average
H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 135Te a c h i n g Hospi tals EXHIBIT 5 Age-, Sex-, Race-, Illness-, And Price-Adjusted Medicare Reimbursements Per Enrollee, In Top 12 Recipient Cities For National Institutes Of Health (NIH) Research Awards, 1996 Hospital Professional referral Inpatient Professional Outpatient plus All region Total ($) hospital ($) and lab ($) hospital ($) outpatient ($) other ($) Houston 6,617 3,149 1,118 545 1,664 1,804 Los Angeles 6,200 3,024 1,534 416 1,950 1,226 New York 6,055 3,612 1,396 391 1,786 657 Boston 5,949 2,766 1,008 566 1,575 1,609 Philadelphia 5,792 3,154 1,304 414 1,718 919 Pittsburgh 5,720 2,954 1,081 472 1,552 1,213 San Diego 5,678 2,649 1,199 427 1,625 1,403 Chicago 5,549 3,169 999 396 1,395 984 Baltimore 5,119 2,777 1,096 555 1,650 691 St. Louis 4,943 2,571 867 500 1,366 1,006 San Francisco 4,557 2,478 848 382 1,230 849 Seattle 4,340 2,227 824 402 1,226 887 12-area average 5,543 2,877 1,106 455 1,562 1,104 Ratio of Boston to 12-area average 1.07 0.96 0.91 1.24 1.01 1.46 SOURCE: Dartmouth Atlas of Health Care, 1999, www.dartmouthatlas.org/tables/99table1.php (25 April 2003). (Exhibit 6). These results are consistent with 2002 surveys by private employee benefit firms.16 Controlling for wage levels would lower Massachusetts premiums relative to those of other areas, while adjusting providers’ operating margins up to national averages would increase them. n The bottom line. A decade of price competition has yielded large reductions in hospital inpatient capacity, provider and health plan consolidation, and improved cost-efficiency. This has led to average Massachusetts inpatient costs that are below those of peer institutions in other states. Health spending is similar to spending in other large urban areas once wage levels and external funding sources are consid- ered, and employer health insurance premiums are consistent with those in other large states. But competition has also created a system that has become increasingly concentrated around academic health systems with fewer low-cost community care options.17 The Rationale For Supporting The Medical Mecca Purchasers will keep trying to reduce health care spending unless they can be convinced that the system generates benefits that justify additional costs. Sources of value commonly attributed to teaching hospitals include quality of care, eco- nomic development, and academic missions such as physician training, research, and indigent care. n Quality of care. Teaching hospitals are recognized for their advanced technol- 136 November/ December 2003
Massachusetts Ho spital s
EXHIBIT 6
Premiums For Single And Family Health Insurance In Private-Sector Establishments
With 50 Workers Or More, By Most Costly State, Fourteen States And U.S. Average,
2000
Family Difference Single Difference
coverage from U.S. coverage from U.S.
State premium ($) average (%) State premium ($) average (%)
New Jersey 7,458 10.5 Illinois 2,898 11.7
Illinois 7,286 7.9 New Jersey 2,784 7.3
Maryland 7,260 7.5 New York 2,716 4.7
Massachusetts 7,089 5.0 Michigan 2,705 4.2
New York 6,836 1.2 Georgia 2,674 3.0
Florida 6,831 1.2 Maryland 2,621 1.0
Texas 6,818 1.0 Virginia 2,599 0.2
Michigan 6,800 0.7 North Carolina 2,587 –0.3
Virginia 6,712 –0.6 Massachusetts 2,572 –0.9
Georgia 6,666 –1.3 Florida 2,558 –1.4
Pennsylvania 6,628 –1.8 Ohio 2,550 –1.7
Ohio 6,622 –1.9 Texas 2,538 –2.2
North Carolina 6,606 –2.2 Pennsylvania 2,397 –7.6
California 6,235 –7.7 California 2,389 –7.9
U.S. 6,752 U.S. 2,595
SOURCE: Agency for Healthcare Research and Quality, 2000 Medical Expenditure Panel Survey.
ogy, specialized services, medical research, and treatment of patients with complex
conditions. But the majority of patients treated at teaching hospitals receive routine
services that are also available at many nonteaching institutions. A recent review of
the literature concluded that for common conditions, major teaching hospitals gen-
erally offer better care than nonteaching hospitals do.18 Purchasers support the no-
tion of paying for higher quality since they generally believe it will result in lower
long-run health care costs.19 But publicly available data that allow payers and pa-
tients to compare the quality of specific services across specific institutions are
scarce. Furthermore, there is little evidence that patients use the quality informa-
tion that is available now.20 Development and dissemination of quality data that pa-
tients can actually use should be a priority for providers, payers, and government
agencies. Without data, reputation holds sway and patients’ demand for teaching
hospitals will remain strong.
n Economic development. AHCs are large employers, and AHC research pro-
grams are often said to stimulate spinoff life science businesses. In Massachusetts,
health care and closely related sectors employ 420,000 people and represent 13 per-
cent of total state employment.21 This provides a stabilizing influence during vola-
tile economic times. The health sector gained more than 10,000 jobs between Octo-
ber 2000 and October 2002, while the nonhealth sector lost nearly 86,000 jobs.22
Economic forecasters estimate that every ten new Massachusetts health care jobs
stimulate eight jobs in other economic sectors.23
Research programs in Massachusetts AHCs and universities help to create a
H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 137Te a c h i n g Hospi tals “Massachusetts hospitals are ahead of their peers in implementing systems that can accelerate performance improvements.” beneficial climate for the state’s biotechnology industry, which added 12,000 new jobs between 1996 and 2001.24 Approximately 8 percent of the world’s pipeline of new drugs now comes from Massachusetts-based companies, and many large pharmaceutical companies have established local research operations there. Most recently, global giant Novartis relocated its research headquarters to Cambridge. Economists have identified life sciences as one of Massachusetts’s most promising sectors, and state officials are actively discussing ways to attract more life sciences investment to the state.25 While the health care sector’s economic benefits are compelling to many, it remains difficult to quantify the trade-offs between health spending levels and economic development. n Academic missions. AHC missions—education, clinical research, specialty services, and care for low-income patients—have been documented extensively.26 These missions are partially supported by government funding, including Medicare direct and indirect GME payments, Medicaid disproportionate-share hospital (DSH) payments, and federal research grants. AHCs also finance mission-related activities with clinical revenues, although recent reimbursement cuts erode these cross-subsidies. While businesses may see value in AHCs’ social missions, most be- lieve that support should come from broad-based tax revenues instead of higher premiums. Little Consensus On Addressing Rising Costs In spring 2003 Massachusetts health plans announced rate increases of 15–20 percent for July 2003 contract renewals.27 A task force made up of Massachusetts’s most senior political and health system leaders recently debated how to control health spending while maintaining access to care and a financially viable delivery system. In its final report, the task force supported the concept of delivering more care at lower-cost, clinically appropriate sites. But aside from expanded state monitoring, the task force did not endorse a formal government role.28 In the absence of government intervention, responsibility falls to the private sector. The three largest plans in Massachusetts finance a much larger volume of health care services than state government does. Massachusetts payers have his- torically been reluctant to limit provider networks, and the national consumer backlash against managed care controls makes it unlikely that they will soon move in this direction. In the past year, however, both Blue Cross and Blue Shield and Tufts Health Plan announced products that will charge higher copayments to patients who select more expensive hospitals.29 Although a logical way to enhance the public’s price-consciousness, the move has stirred concern that patients with valid geographic or clinical reasons to use these hospitals will be penalized. It is 138 November/ December 2003
Massachusetts Ho spital s
still unclear whether these types of products will gain sizable market share.
Cynics might conclude that in the absence of viable options, public and private
Massachusetts payers will fall back on their most effective tool: unit price con-
trols. Rate negotiations have become increasingly acrimonious.30 Yet the predomi-
nant driver of hospital spending growth in 2001 and 2002 was utilization rather
than prices.31 Instead of simply fighting over rates, payers and providers should
collaborate to reduce unnecessary service volume.
Future Directions For The Medical Mecca
A growing body of research documents the need for dramatically better health
care system performance.32 In response, organizations are developing a range of
tools to identify high-risk patients early, transmit information to clinicians at the
point of care, and help people manage their chronic conditions outside of formal
care settings.33 AHCs could lead the movement to refocus medical science and in-
formation technology toward managing the small population of high-cost people
that constitute the majority of health care expenditures each year. But changes in
organizational culture and behavior necessary to support such improvements will
come slowly under current health care financing structures. Sanders Williams
and colleagues make this point eloquently in a recent Science magazine editorial:
Personalized health planning to anticipate and minimize each individual’s risk for the onset and progression
of disease is what our health care future will require…These capabilities are at hand, yet nothing at all like
this happens today in U.S. clinics and hospitals. Worse, current payment systems punish providers who try
to practice in a manner consistent with the best science. For example, a recent pilot program launched by our
institution improved outcomes and reduced annual expenses for the care of patients with congestive heart
failure from approximately $23,000 to $14,000 per patient. The financial consequences for our health care
system under current payment principles however, were strongly negative because patients stayed out of the
hospital and avoided procedures that are relatively well reimbursed, while incurring somewhat greater ex-
penses for ambulatory visits and patient education, for which payments do not meet costs.34
Massachusetts hospitals are ahead of their peers in implementing systems that
can accelerate performance improvements. Brigham and Women’s Hospital is a
national leader in using computerized physician order entry (CPOE) systems to
reduce medical errors.35 Both the Partners and CareGroup health systems have im-
plemented electronic patient records that are broadly accessible across system
hospitals and affiliated medical groups. While electronic health care information
is now shared only within systems, mechanisms such as the New England
Healthcare EDI Network (NEHEN), now used to transmit administrative data,
could eventually facilitate much broader clinical data integration. While still
years away, statewide clinical data linkages could facilitate greater use of commu-
nity care settings supported by electronic connections to downtown specialists.
Electronic clinical information can also support more robust quality analysis,
reporting, and feedback than now exists. As these systems develop, Massachu-
setts AHCs will have a chance to document the “value added” from care in the
Medical Mecca. This is both an opportunity and a risk, since market advantages
H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 139Te a c h i n g Hospi tals
built on reputation could diminish in the face of potentially ambiguous quality
metrics.
M
a s s ac h u s e t ts h o s p i ta l s have made efficiency gains under the cur-
rent model of care. Whether this can continue is unclear. The largest
source of untapped value in the Medical Mecca is the potential to lead
“proactive” health care initiatives that improve clinical outcomes and patients’ ex-
periences. Yet current reimbursement structures make it difficult for providers to
make a “business case” for programs that would otherwise produce favorable re-
sults for purchasers, patients, and society.36 Progress will require that public and
private payers work with providers to move beyond the current financial gridlock
and develop new health care financing and delivery models. Massachusetts, with
its tradition of innovation, concentration of scientific knowledge, and increasingly
integrated systems of care, would do well to move rapidly in this direction.
NOTES
1. A. Sager et al., The World’s Most Expensive Hospitals (Boston: Access and Affordability Monitoring Project,
1991); and A. Sager and D. Scholar, The World’s Most Expensive Health Care: Massachusetts Health Care Costs,
1980–1998 (Boston: Access and Affordability Monitoring Project, 2000).
2. AHCs are defined as teaching hospitals under common ownership with a medical school and those in
which the majority of the chiefs of service also serve as department chairs at the medical school. Based on
1999 data, Massachusetts has a higher proportion of inpatient hospital days in AHCs than all states ex-
cept the District of Columbia. New York State has a higher proportion of days in AHCs and major teach-
ing hospitals combined.
3. J.H. Grossman, An Economic History of Health Care in Massachusetts, 1990–2000 (Boston: Pioneer Institute for
Public Policy Research, 2000).
4. Tillinghast-Towers Perrin, unpublished analysis, July 2002.
5. A. Pham, “State Seeks Oversight of Ailing Blue Cross,” Boston Globe, 22 May 1997.
6. Medicare hospital margins reached a peak in 1997 prior to enactment of the Balanced Budget Act. See, for
example, MedPAC, Report to the Congress: Medicare Payment Policy (Washington: MedPAC, 2003); and A.
Dobson et al., Financial Performance of Academic Health Center Hospitals, 1994–2000 (New York: Commonwealth
Fund, 2002).
7. Medicare Payment Advisory Commission, Report to the Congress: Medicare Payment Policy (Washington:
MedPAC, 2001).
8. Major teaching hospitals are defined as institutions with twenty-five or more residents per 100 staffed beds.
AHCs are treated as a distinct category.
9. Lewin Group, Analysis of the Reimbursement Rates for Acute Hospitals, Nonacute Hospitals, and Community Health Cen-
ters (Falls Church, Va.: Lewin Group, 2001).
10. R.E. Mechanic et al., “Teaching Hospital Costs: Implications for Academic Missions in a Competitive En-
vironment,” Journal of the American Medical Association 280, no. 11 (1998): 1015–1019; and Commonwealth Fund
Task Force on Academic Health Centers, Envisioning the Future of Academic Health Centers (New York: Com-
monwealth Fund, February 2003).
11. In a review of 2001 audited financial statements of eight Boston hospitals, the author identified research
revenues of approximately $1.1 billion.
12. “Medicare Program: Changes to the Hospital Inpatient Prospective Payment Systems and Fiscal Year 2003
Rates,” Federal Register 67, no. 148 (2002): 50214–50224.
13. ACCRA, “ACCRA Cost of Living Index” for the first quarter of 2003, www.coli.org (15 August 2003).
14. A. Martin et al., “Health Care Spending during 1991–1998: A Fifty-State Review,” Health Affairs (July/Aug
2002): 112–126.
140 November/ December 2003Massachusetts Ho spital s
15. Centers for Medicare and Medicaid Services, National Health Accounts: Definitions, Sources, and Methods Used in
the NHE 2001, cms.hhs.gov/statistics/nhe/definitions-sources-methods (18 September 2003).
16. Hewitt Associates, “Health Care Cost Increases Expected to Continue Double-Digit Pace in 2003,” 14 Oc-
tober 2002, was4.hewitt.com/hewitt/resource/newsroom/pressrel/2002/10-14-02.htm (25 April 2003);
and Mercer Human Resources Consulting, “Rate Hikes Pushed Employers to Drop Health Plans, Cut
Benefits in 2002—but Average Cost Still Rose,” 9 December 2002, www.mercerhr.com/pressrelease/
details.jhtml/dynamic/idContent/1076975 (25 April 2003).
17. Massachusetts Health Care Task Force, Final Report 2002, www.state.ma.us/healthcare/pages/pdf/final.pdf
(18 September 2003), 31.
18. J.Z. Ayanian and J.S. Weissman, “Teaching Hospitals and Quality of Care: A Review of the Literature,”
Milbank Quarterly 80, no. 3 (2002): 569–593.
19. R.S. Galvin, “An Employer’s View of the U.S. Health Care Market,” Health Affairs (Nov/Dec 1999): 166–170.
20. M.N. Marshall et al., “The Public Release of Performance Data: What Do We Expect to Gain? A Review of
the Evidence,” Journal of the American Medical Association 283, no. 14 (2000): 1866–1874.
21. Standard and Poor’s/DRI, The Massachusetts Health-Care Industry: A Stalled Engine of Economic Growth
(Burlington: Massachusetts Hospital Association, 2000).
22. L. Kowalczyk, “Hiring for Health Care Is Surging in Bay State,” Boston Globe, 29 January 2003.
23. Ibid.; and Standard and Poor’s/DRI, The Massachusetts Health-Care Industry.
24. Boston Consulting Group, MassBiotech 2010: Achieving Global Leadership in the Life Sciences Economy (Cambridge:
Massachusetts Biotechnology Council, 2002).
25. R. Kerber, “Economists Say Life Sciences Offer Great Promise for State,” Boston Globe, 13 September 2003.
26. D. Blumenthal et al., Understanding the Social Missions of Academic Health Centers (New York: Commonwealth
Fund, 1997).
27. L. Kowalczyk, “Health Insurance to Jump: Cities, Towns Face Latest Fiscal Blow,” Boston Globe, 12 April
2003.
28. Ibid.; and Massachusetts Health Care Task Force, Final Report.
29. L. Kowalczyk, “HMOs Eyeing Surcharge for High-End Care; Some ’02 Plans Affect Visits to Medical Cen-
ters,” Boston Globe, 28 August 2001.
30. B.C. Strunk et al., Health Plan–Provider Showdowns on the Rise, Issue Brief no. 40 (Washington: Center for
Studying Health System Change, June 2001).
31. B.C. Strunk and P.C. Ginsburg, “Tracking Health Care Costs: Trends Stabilize but Remain High in 2002,”
11 June 2003, www.healthaffairs.org/WebExclusives/Strunk_Web_Excl_061103.htm (15 August 2003). In a
1 June 2003 interview with the Boston Globe, Tufts Health Plan CEO Nancy Leaming said that utilization
drives 60 percent of the increase in medical care cost.
32. Institute of Medicine, Crossing the Quality Chasm: A New Health System for the Twenty-first Century (Washington:
National Academies Press, 2001).
33. R.E. Mechanic et al., Proactive Medical Management (Cambridge: Forrester Research, 2001).
34. R.S. Williams et al., “Personalized Health Planning,” Science 300, no. 5619 (2003): 549.
35. D.W. Bates et al., “Effect of Computerized Physician Order Entry and a Team Intervention on Prevention of
Serious Medication Errors,” Journal of the American Medical Association 280, no. 15 (1998): 1311–1316.
36. S. Leatherman et al., “The Business Case for Quality: Case Studies and an Analysis,” Health Affairs (Mar/Apr
2003): 17–30.
H E A L T H A F F A I R S ~ Vo l u m e 2 2 , N u m b e r 6 141You can also read