LTC COVID-19 Update Lori Davenport, Director of Regulatory & Clinical Affairs Kara Dawson, QSource Indiana Department of Health Team - Indiana ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

June 23, 2022 LTC COVID-19 Update Presented by: Lori Davenport, Director of Regulatory & Clinical Affairs Kara Dawson, QSource Indiana Department of Health Team
Today’s Topics • IDH Updates Vaccines for children and Langham portal and PPE orders – Dr. Vuppalanchi • NAT Waivers, what you need to know – Suzanne Williams • NHSN Update and a snack – Kara Dawson • Q&A DON Workshop for SNF nurses, June 29-30, details HERE IHCA/INCAL Annual Convention & Expo, registration open, details HERE
COVID-19 UPDATE SHIREESHA VUPPALANCHI, M.D. MEDICAL DIRECTOR 06/23/22

OUR MISSION: To promote, protect, and improve the health and safety of all Hoosiers. OUR VISION: Every Hoosier reaches optimal health regardless of where they live, learn, work, or play.
COVID-19 Vaccine updates

COVID-19 vaccine
• COVID-19 vaccination is recommended for everyone ages 6 months and older,
regardless of a history of symptomatic or asymptomatic SARS-CoV-2 infection. This
includes people with prolonged post-COVID-19 symptoms and applies to primary
series and booster doses. This recommendation also applies to people who
experience SARS-CoV-2 infection after receiving any COVID-19 dose.
• Everyone ages 5 years and older should receive at least 1 booster dose of COVID-19
vaccine if eligible (i.e., if a booster dose is FDA-approved or FDA-authorized for use in
a specified population). Recommendations for booster dose(s) vary based on age,
COVID-19 vaccine product, and immunocompetence.
• Janssen COVID-19 Vaccine should only be used in limited situations; Pfizer-BioNTech
or Moderna COVID-19 Vaccines are preferred for primary and booster vaccination.
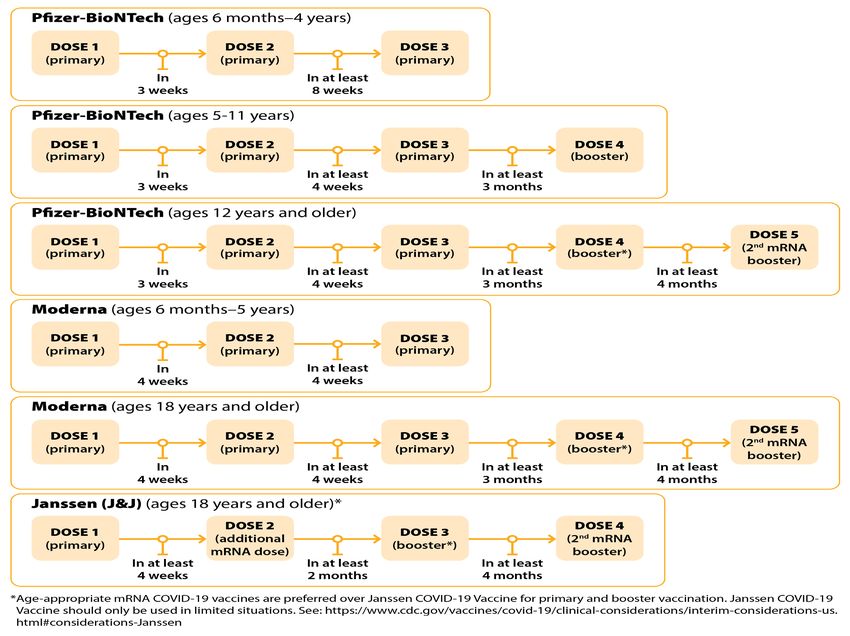
COVID-19 Vaccine Interim COVID-19 Immunization Schedule for 6
6
Clinical Guidance for COVID-19 Vaccination | CDC
Months of Age and Older (cdc.gov)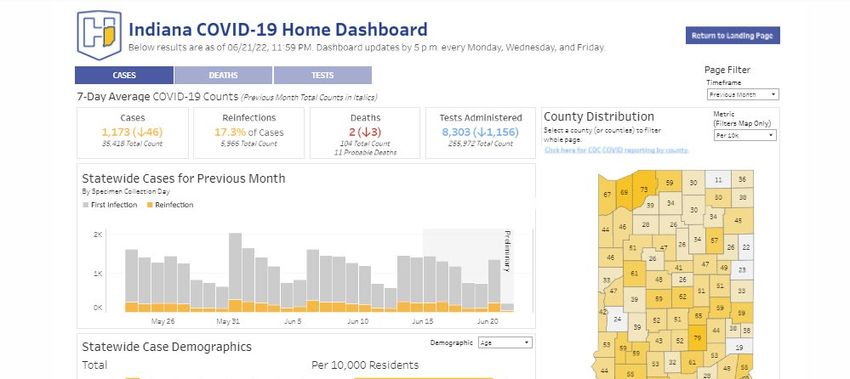
Pfizer
Vaccination
Schedule
7
COVID19-vaccination-schedule-most-people.png (1200×1084) (cdc.gov)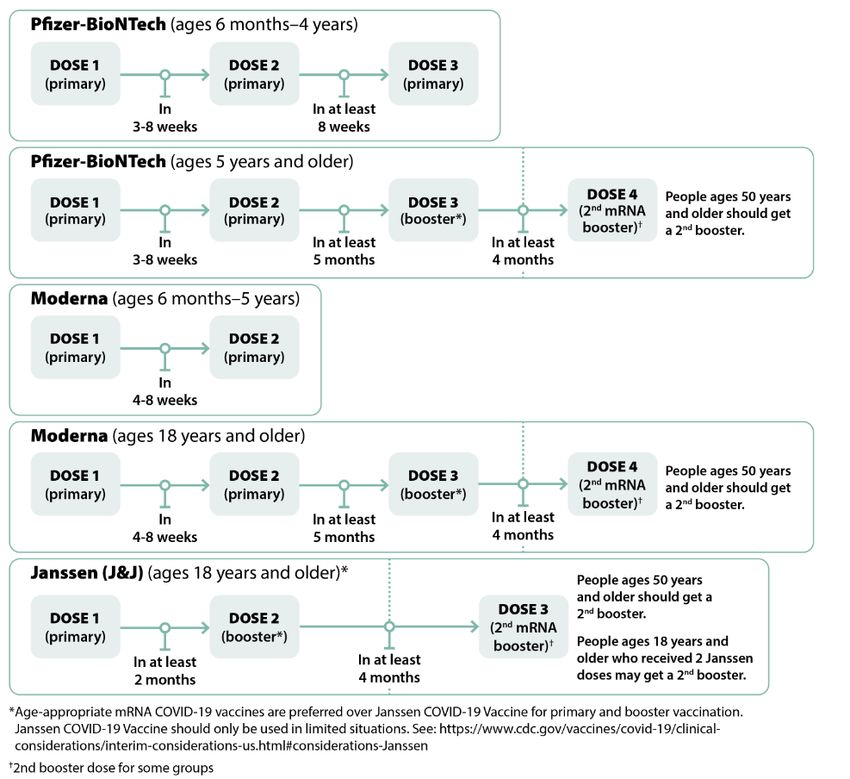
6 months to 11 years
8
Clinical Guidance for COVID-19 Vaccination | CDC
12-17 years
Clinical Guidance for COVID-19 Vaccination | CDC
9
18 years and older
Notes
* mRNA COVID-19 vaccines are preferred over Janssen COVID-19 Vaccine for both primary and
booster doses; an mRNA COVID-19 vaccine must be used for the second booster dose.
†An 8-week interval may be optimal for some people ages 6 months–64 years, especially for
males ages 12–39 years. A shorter interval (3 weeks for Pfizer-BioNTech; 4 weeks for Moderna)
between the first and second doses remains the recommended interval for people who are
moderately or severely immunocompromised; adults ages 65 years and older; and in situations
in which there is increased concern about COVID-19 community levels or an individual’s higher
risk of severe disease.
‡People ages 18–49 who received Janssen COVID-19 Vaccine as both their primary dose and
first booster dose may receive a second booster dose using an mRNA vaccine at least 4 months
after the first booster dose.
11Pfizer vaccine dosing
12Moderna vaccine dosing
Vaccine Label Primary series Booster doses†
Age Dilution
vial cap border Injection Injection
indication required Dose Dose
color color volume volume
6 months–
Dark blue Magenta No 25 µg 0.25 mL NA NA
5 years
18 years
Red Light blue No 100 µg 0.5 mL 50 µg 0.25 mL
and older
18 years
Dark blue Purple No NA NA 50 µg 0.5 mL
and older
13Updated schedule for immunocompromised
Self-attestation of immunocompromised status
People can self-attest to their moderately or severely immunocompromised
status and receive COVID-19 vaccine doses wherever vaccines are offered.
Vaccinators should not deny COVID-19 vaccination to a person due to lack of
documentation.
15For Immunocompromised
Clinical Guidance
for COVID-19
Vaccination | CDC
16Immunocompromised Ages 6-11
Clinical Guidance for COVID-19 Vaccination | CDC
17Immunocompromised Ages 12-17
Clinical Guidance for COVID-19 Vaccination | CDC
18Immunocompromised Ages 18 and older
Clinical Guidance for COVID-19 Vaccination | CDC
19Pearls
Dosage and mAbs
• Doses administered up to 4 days before the minimum interval, known as the 4-day grace
period, are considered valid. This applies to primary series and booster doses. Doses
administered at any time after the recommended interval are valid.
• People should receive the recommended age-appropriate vaccine dosage based on their age
on the day of vaccination. If a person moves from a younger age group to an older age
group during the primary series or between the primary series and receipt of the booster
dose(s), they should receive the vaccine product and dosage for the older age group for all
subsequent doses.
• People who previously received antibody products (anti-SARS-CoV-2 monoclonal antibodies
or convalescent plasma) as part of COVID-19 treatment, post-exposure prophylaxis, or pre-
exposure prophylaxis can be vaccinated at any time; COVID-19 vaccination does not need to
be delayed following receipt of monoclonal antibodies or convalescent plasma.
21Vaccination after close contact
• COVID-19 vaccines are not recommended for post-exposure prophylaxis to prevent SARS-CoV-2
infection. Unvaccinated people who were close contacts of a person with SARS-CoV-2 infection should
typically not seek vaccination until quarantine has ended
• In certain circumstances, to avoid missed opportunities for vaccination, vaccination during quarantine
could be considered during outreach and contact tracing activities or at the time of post-exposure
SARS-CoV-2 testing. Examples might include when people
1) are likely to have repeated SARS-CoV-2 exposures because they are unable to effectively quarantine
(e.g., residing in a congregate or crowded setting or during outbreaks in their community), or, 2) will have
limited access to vaccination after their quarantine period has ended, or, 3) are unlikely to otherwise seek
vaccination after their quarantine period has ended. In such situations, the person recommended for
quarantine can receive vaccination as long as 1) they do not have symptoms consistent with COVID-19 or
current SARS-CoV-2 infection, and, 2) appropriate infection prevention and control procedures are
employed during vaccination.
• If had exposure while not up to date, they cannot come out of quarantine due to getting the booster.
They have to complete the serial testing and TBP time.
22Second Booster timing
23Booster timing with respect to time of admission
• If boosted 24 hours or more before admission, they follow guidance for the
up to date.
• If a new admission/readmission receives a booster dose upon admission to a
facility or within 24 hours prior to admission, they can come out of TBP
provided they had
o No close contact in the 10 days prior to admission and
o Asymptomatic
o Tested negative at admission and 24 hours after admission and
o Not immunocompromised.
o They should still undergo testing at 5-7 days like all new admissions
24Trends
Hospitalization trends
26Hospital census
Novel Coronavirus (COVID-19): Hospital Dashboard (in.gov)
27Miscellaneous
PPE Still Available to Order Through Langham
IDOH still has an abundant supply of PPE available for LTC facilities to order for
residents, staff, or visitors. Facilities may order any items that are available and
as much as they would like. We recommend that facilities order extra PPE to
build up the facility’s on-hand supplies.
All PPE and shipping costs will continue to be FREE to LTC through the end of
July or while supplies last.
Due to a scheduled inventory cycle count, no orders will be shipping out until June 29, 2022
IDOH Order Entry Portal Guide Instructions
Access Langham Portal (Sign In)
29Visitation
While it is safer for visitors not to enter the facility during an outbreak
investigation, visitors must still be allowed in the facility. Visitors should be
made aware of the potential risk of visiting during an outbreak investigation
and adhere to the core principles of infection prevention. If residents or their
representative would like to have a visit during an outbreak investigation, they
should wear face coverings or masks during visits, regardless of vaccination
status, and visits should ideally occur in the resident’s room.
30
https://www.cms.gov/files/document/qso-20-39-nh-revised.pdfMasks
Source control and physical distancing (when physical distancing is feasible and will not
interfere with provision of care) are recommended for everyone in a healthcare setting.
• HCP who are up to date with all recommended COVID-19 vaccine doses:
◦ Could choose not to wear source control or physically distance when they are in well-defined
areas that are restricted from patient access (e.g., staff meeting rooms, kitchen).
◦ They should wear source control when they are in areas of the healthcare facility where they
could encounter patients (e.g., hospital cafeteria, common halls/corridors).
• Residents who are up to date with all recommended COVID-19 vaccine doses in Nursing
Homes in Areas of Low to Moderate Transmission:
o Consideration could be given to allowing residents who are up to date with all recommended
COVID-19 vaccine doses to not use source control when in communal areas of the facility;
however, residents at increased risk for severe disease should still consider continuing to
practice physical distancing and use of source control
31
Infection Control: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) | CDCFans
32
Ventilation in Buildings | CDCQuestions? CONTACT: Shireesha Vuppalanchi, MD Medical Director Indiana Department of Health svuppalanchi@isdh.in.gov
Nurse Aide Training Waivers
What You Need to Know
Suzanne Williams
6/23/202235
Nurse Aide Training Waivers
Ending July 1:
• Personal care attendants (PCAs) and temporary nurse aides (TNAs).
• Facilities have been encouraged to complete the training of their PCAs,
TNAs and others working as nurse aides by that date; however, they may
test after July 1.
• Nurse aide training programs have until July 1 to train nurse aides using
the abbreviated or expedited training – that training is only allowed under
the waivers that expire July 1.
• Any nurse aide training after July 1 must be the usual 105 hours of
training.
36Federal Waiver Ended June 6
• The federal waiver from Centers for Medicare and Medicaid Services (CMS) allowing nurse aides 8
months to work and complete their training and testing, rather than just 4 months, expired June 6.
• Nurse aides still have 4 months after the waiver ended (until October 6) to complete their training,
testing and certification.
• Refer to the CMS press release and QSO-22-15-NH & NLTC & LSC.
37If PCAs, TNAs or other nurse aides do not complete training by July 1, they can continue to work as
nurse aides as long as they enroll in a nurse aide training program (105-hour program) and become
certified by October 6 (if they were hired before June 6).
Any nurse aides hired after June 6 have the usual 4 months to complete their training and testing and
become certified.
38• If nursing facilities or training programs have questions or experience capacity issues in training and
testing that will result in a delay for a nurse aide to meet the full requirements within 4 months after the
federal waiver ended, please notify Suzanne Williams at suwilliams@isdh.in.gov.
• If an individual nurse aide is experiencing a delay in being placed on the Nurse Aide Registry and it has
been more than 30 days since they completed their training hours and successfully passed the CNA
Competency Evaluation Examination, please contact Ivy Tech at CNA_QMA_testing@ivytech.edu.
39Coming Soon
Nurse Aide in Training Registry
• A REDCap Nurse Aide in Training Registry has been created to provide a
record of nurse aides in training in nursing facilities in Indiana.
• This will enable IDOH to monitor capacity related to the training, testing and
certification of nurse aides.
• Beginning July 1, nursing facilities should complete the survey for any nurse
aides hired who are not yet certified. This would include former PCAs and
TNAs who did not complete their nurse aide training prior to July 1 but are
enrolled in a nurse aide training program with the intention of completing the
training, testing and certification.
40F728
A facility must not use any individual working in the facility as a nurse aide for
more than 4 months, on a full-time basis, unless (i) That individual is
competent to provide nursing and nursing-related services; and (ii)(A) That
individual has completed a training and competency evaluation program, or a
competency evaluation program approved by the state as meeting the
requirements of §483.151 through §483.154.
A facility must not use any individual who has worked less than 4 months as a
nurse aide in that facility unless the individual (i) is a full-time employee in a
state-approved training and competency evaluation program; and (ii) has
demonstrated competence through satisfactory participation in a state-
approved nurse aide training and competency evaluation program or
competency evaluation program.
41New Policy for Requesting a Waiver of NATCEP
Loss
Facilities whose CNA training has been banned had the opportunity during the COVID-
19 public health emergency to request a waiver and conduct abbreviated nurse aide
training in their facility by an approved CNA training program.
• These waivers of NATCEP loss allowing training in banned facilities expire on July 1,
2022.
The new IDOH policy and procedure for facilities to request a waiver of disapproval of
nurse aide training has been in effect since June 1.
Facilities may request a waiver by emailing ISDHLTCTrainingPrograms@ISDH.IN.gov with
the required information in the checklist of information to request a waiver of
disapproval of Nurse Aide Training and Competency Evaluation Program (NATCEP).
This information was also in the 5/26/2022 LTC Newsletter.
42Contacts
Ivy Tech Contacts:
If you have general questions about the CNA QMA Testing Office, please email
cna_qma_testing@ivytech.edu.
Also, visit their website for additional information and FAQs:
https://www.ivytech.edu/cna_qma_testing
If you are representing a training facility and you have questions or need
information, please email Lori Urick at lurick@ivytech.edu.
IDOH CNA/QMA Training and Registry webpage:
https://www.in.gov/health/rules/aide-training-certification-and-registry/
43Questions?
CONTACT:
Suzanne Williams
SuWilliams@isdh.in.gov
44Vaccination Tracking
QSO-22-17-ALL
• Survey oversight of the staff vaccination requirement for
Medicare and Medicaid certified providers and suppliers
will continue to be performed during initial and
recertification surveys but will now only be performed in
response to complaints alleging non-compliance with this
requirement, not all surveys. Under prior guidance, all
surveys included oversight of the staff vaccination
requirement.
• CMS will revise QSO 22-11 to ensure deficiency
determinations reflect good faith efforts implemented by
providers and suppliers and incorporate harm or potential
harm to patients and residents resulting from any non-
compliance
46Vaccination Tracking
• Tracking of staff and resident vaccinations is essential to ensuring
compliance with regulations
• Utilizing internal tracking tools to monitor vaccination and/or
exemption status of all healthcare workers and residents
• Developing systems to ensure that residents and/or healthcare
workers that are not up to date and/or eligible for the next step in
their vaccination series receive their vaccinations in a timely
manner to ensure compliance.
47Vaccination Reminders
• Must wait 21days (Pfizer) and 28 days
(Moderna) between primary doses.
• An individual is eligible for 1st booster 5
months after primary series completed
• Individuals over 50 years of age or severely
immunocompromised are recommended to
receive a second booster (Pfizer or Moderna)
at least 4 months after first booster
48Staff Vaccination InternalTracking Tool
Complete this form or Direct facility Age or Date Title/Positio Assigned Vaccinated Not Vaccinated
provide a list containing hire (DH), of Birth n work area
the same information Contracted hire
required in this form. (C), Other (O)
Section I: Complete based
on the Day 1 of the
survey:
Total # of staff:
# partially vaccinated staff
(5):
# completely vaccinated
staff (6):
# pending exemption (8
and 9):
# granted exemption (8 and
9):
# temporary delay/new hire
(10):
# not vaccinated without
exemption/delay
(11):
Note: The sum of the #’s
for columns 5, 6, 8 through
11 should equal the total #
of staff.
Partially Eligible Completely Eligible 1st Booster Eligible for Eligible Date 2nd Booster Pending (P) Pending Temporary Not vaccinated without
vaccinated Date for 2nd vaccinated Date for 1st dose 2nd Booster for 2nd Dose or Granted (PN) or delay per exemption/delay
Booster Dose
Shot Booster Yes/No (G) medical Granted CDC/ new
(Primary exemption (GN) non- hire
Series) medical
exemption
Staff Name
Sally Sunshine DH 52 RN DON X X Yes 6/30/2022 N/A N/A N/A N/A
Patty Cake DH 25 CNA 200 hall X 7/4/2022Resident Internal Tracking Sheet
Complete this form or Date of Discharge Isolation - Assigned Vaccinated Not Vaccinated
provide a list containing the Admission Date Yes/No Room #
same information required in
this form.
Section I: Complete based on
the Day 1 of the survey:
Total # of residents
# partially vaccinated
residents :
# completely vaccinated staff
(6):
# pending exemption (8 and
9):
# granted exemption (8 and
9):
# temporary delay
(10):
# not vaccinated without
exemption/delay (11):
Note: The sum of the #’s for
columns 5, 6, 8 through 11
should equal the total # of
staff.
Partially Eligible Complete Eligible 1st Eligible 2nd Fully Pending Pending Tempora Not vaccinated
vaccinate Date for ly Date for Booster Date for Booster Vaccinate (P) or (PN) or ry delay without
d 2nd Shot vaccinate 1st dose 2nd Dose d Granted Granted per CDC/ exemption/delay
(Primary d Booster Booster (G) (GN) new hire
Series) Dose medical non-
exemptio medical
n exemptio
n
Resident Name
Jack Benimble 6/20/2022 No x 1/1/2022 6/1/2022 X
50Tickler System
• Pending File
• Files numbered 1-31 (days of the month)
• Place notice in corresponding number according to eligible date
• Load files at end of month for the next month (ex : end of June for
July)
• Look a week ahead to notify staff and/or residents of their upcoming
eligible date
• Schedule clinics according to demand each week/month
• Take all notices out of current day to morning meeting – to discuss
with team
• Place the notices in pending file and once proof of vaccination (copy
of card, etc.) is obtained shred notice in pending file and file current
vaccination card and update tracking tool.
51Qsource Assistance
• The QIO is available to assist facilities with tracking
tools and/or implementing the tracking/tickler system.
• Kara Dawson
kdawson@qsource.org
317-628-1145
• Teresa Hostettler
thostettler@qsource.org
812-381-1581
52Q&A
IHCA.ORGContact Information
Lori Davenport – IHCA/INCAL Clinical/Regulatory
• ldavenport@ihca.org Dr. Shireesha Vuppalanchi – Clinical, IDH Deeksha Kapoor – IHCA/INCAL Communications/PR
• 765-516-0148 • svuppalanchi@isdh.in.gov • dkapoor@ihca.org
Amy Kent – Assistant Commissioner, IDH Brenda Buroker – Survey, IDH Rob Jones – IDH Gateway Assistance
• amkent1@isdh.in.gov • rjones@isdh.in.gov
• bburoker@isdh.in.gov
• 317-233-7289 • 317-234-7340 David McCormick
Jennifer Spivey – Infection Control, IDH • DMcCormick@isdh.IN.gov
Jan Kulik
• JSpivey1@isdh.IN.gov • jkulik@isdh.in.gov Dr. Lindsey Weaver
• 317-232-0639 • 317-233-7480 • lweaver@isdh.in.gov
• 317-471-7844 cell
Peter Krombach Suzanne Williams
Paul Krievins • SuWilliams@isdh.in.gov
• pkrombach2@isdh.in.gov
• pkrievins@isdh.in.gov Langham Customer Service
Michelle Donner
Kelly White – Reporting, IDH • 866-926-3420
• midonner@isdh.in.gov • Covidsupport@elangham.com
• kewhite@isdh.in.gov
Pam Pontones – CDC Guidance, IDH
Tammy Alley – Vaccine Questions, IDH • ppontones@isdh.IN.gov
• talley@isdh.in.gov • 317-233-8400
• 317-223-7441
Kara Dawson – NHSN
Randy Synder – Vaccine Questions, IDH • kdawson@qsource.org
• rsnyder1@isdh.in.gov • 317-628-1145 OR contact:
Russell Evans • Angeleta Hendrickson -
ahendrickson@qsource.org
• russ@probarisystems.com
• Teresa Hostettler - thostettler@qsource.org
• outreach@probarisystems.com
• 317-804-4102THANK YOU!
IHCA.ORGYou can also read