Long term alterations of growth after antenatal steroids in preterm twin pregnancies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

J. Perinat. Med. 2021; 49(2): 127–137
Academy’s Paper
Thorsten Braun*, Vivien Filleböck, Boris Metze, Christoph Bührer, Andreas Plagemann
and Wolfgang Henrich
Long term alterations of growth after antenatal
steroids in preterm twin pregnancies
https://doi.org/10.1515/jpm-2020-0204 significantly decreased between infancy and early child-
Received May 11, 2020; accepted September 11, 2020 hood by 18.8%. Birth weight percentiles significantly
published online October 5, 2020
changed in a dose dependent and sex specific manner,
most obviously in female-female and mixed pairs. The
Abstract
ponderal index significantly decreased up to 42.9%, BMI
index increased by up to 33.8%.
Objectives: To compare the long-term effects of antenatal
Conclusions: ANS results in long-term alterations in infant
betamethasone (ANS, ≤16 mg, =24 mg and >24 mg) in twins
and childhood growth. Changes between infancy and early
on infant and childhood growth.
childhood in ponderal mass index and BMI, independent
Methods: A retrospective cohort follow up study among
of dose or twin pair structure, might indicate an ANS
198 twins after ANS including three time points: U1 first
associated increased risk for later life disease.
neonatal examination after birth and in the neonatal
Synopsis: First-time report on long-term ANS administra-
period; U7 examination from the 21st to the 24th month of
tion growth effects in twin pregnancies, showing persisting
life and U9 examination from the 60th to the 64th month of
alterations beyond birth in infant and childhood growth up
life using data from copies of the children’s examination
to 5.3 years as potential indicator of later life disease risk.
booklets. Inclusion criteria are twin pregnancies with
preterm labor, cervical shortening, preterm premature Keywords: antenatal betamethasone; antenatal steroid
rupture of membranes, or vaginal bleeding, and exposure (ANS); dosage; early childhood; follow up; infancy; sex;
to ANS between 23+5 and 33+6 weeks. Outcome measures twin pregnancy.
are dosage-dependent and sex-specific effects of ANS on
growth (body weight, body length, head circumference,
body mass index and ponderal index) up to 5.3 years.
Introduction
Results: Overall, 99 live-born twin pairs were included.
Negative effects of ANS on fetal growth persisted beyond
In pregnancies threatened with preterm birth, antenatal
birth, altered infant and childhood growth, independent of
steroid (ANS) treatment to induce fetal lung maturation
possible confounding factors. Overall weight percentile
and to reduce neonatal morbidity and mortality is common
practice [1] and appropriate alternatives currently do not
exist [2]. We have previously shown that ANS treatment in
*Corresponding author: Thorsten Braun, Clinic of Obstetrics, Division
of Experimental Obstetrics, Charité – Universitätsmedizin Berlin, normally grown singleton and twin pregnancies reduced in
Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, a dose-dependent and sex-specific manner fetal weight
Germany, E-mail: thorsten.braun@charite.de gain, length and head circumference compared with
Vivien Filleböck and Wolfgang Henrich, Clinic of Obstetrics, Charité – gestational age-matched controls [3, 4]. ANS doses esca-
Universitätsmedizin Berlin, Corporate Member of Freie Universität
lation even increased the negative effects on fetal growth,
Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health,
Berlin, Germany
but did not improve neonatal morbidity and mortality at
Boris Metze and Christoph Bührer, Clinic of Neonatology, Charité – birth. Although birth weight is only a rough surrogate
Universitätsmedizin Berlin, Corporate Member of Freie Universität marker for hormonal or nutritional changes in the intra-
Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, uterine environment, impaired fetal growth is associated
Berlin, Germany with a number of long-term developmental and health
Andreas Plagemann, Division of Experimental Obstetrics, Charité –
implications [5, 6]. Exposure to high levels of glucocorti-
Universitätsmedizin Berlin, Corporate Member of Freie Universität
Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, coids in utero is amongst the proposed mechanisms of
Berlin, Germany perinatal programming [5, 7, 8]. The implications for ANS
Open Access. © 2020 Thorsten Braun et al., published by De Gruyter. This work is licensed under the Creative Commons Attribution 4.0
International License.128 Braun et al.: ANS and follow up in twins
are still not fully understood. There are still ongoing trials Material S3). For the documented anthropometric data, percen-
and research projects in singleton pregnancies, investi- tiles were calculated using the Ped (Z) pediatrician calculator
[17]. This web calculator is based on data from Kromeyer-
gating all different kinds of aspects regarding ANS treat-
Hauschild et al. for pediatric percentiles of infants, children and
ment such as which type of glucocorticoid and which adolescents for height, weight and BMI [18]. In addition, per-
formula should be used, which dosages and time intervals centiles for 0–6 year old children were derived for a variety of
between injections are preferable, which gestational age somatic parameters according to Hesse et al. [19–21]. For the
would benefit most and what kind of long term implica- head circumference percentiles, the data of the ‘Zurich Longitu-
dinal Studies’ (1955–2009) were used [22].
tions are associated even with reduced ANS dosages [8].
As reported previously, the protocol for steroid administration
In multiple pregnancies, the different pharmacokinetics
changed over time at our institution according to different local and
of ANS compared to singletons, the increased total fetal international clinical recommendations in effect during the study
mass and increased volume distribution in twins led to the period [4]. The betamethasone treatment regimen ranged from 2×8 mg
discussion that the current glucocorticoid dose applied (≤16 mg) or 2×12 mg (=24 mg) given once during pregnancy, to repeated
might be too low to induce fetal lung maturation [9–13]. The doses of betamethasone (8 mg weekly or 2×12 mg every second week)
when the diagnosis of preterm labor still persisted (collectively
effects of antenatal lung maturation with glucocorticoids in
grouped as ≥24 mg). Betamethasone dosage effects were analyzed
multiple pregnancies still remains unclear as trials in twins among three different dosages: ≤16 mg, 24 mg and >24 mg. Gender
are limited and evidence is lacking [1, 9–15]. Especially specificity was tested for male-male, female-female and mixed-pairs of
follow up studies on long term changes are missing. twins. The Charité Hospital Ethics Review Committee approved the
Therefore, the present study’s objective was to inves- trial (EA2_111_15). All participants gave written informed consent
before the study began.
tigate in twin pregnancies ANS dosage and sex-specific
long-term effects on infant and child growth development
up to 5.3 years of age.
Statistics
Crossed items in the sent copies of the children’s examination booklets
Materials and methods were interpreted as true, unchecked items as inaccurate and thus
transferred to an Excel database. Statistical analyzes were performed
Prospective cohort study of twins born between December 1993 and using the SPSS 25 software (IBM, SPSS Statistics, version 25, IBM
January 2011 in a tertiary referral center at the Clinic of Obstetrics, Corporation, Armonk, NY, USA). Data were tested for normality
Charité University Hospital Berlin, Germany. Details on the original assessing the histogram and using the Shaipiro-Wilks test. To analyze
birth cohort has been described previously [4]. Briefly, cases were the long-term effects of antenatal betamethasone on anthropometrics
defined as twin pregnancies with the diagnosis of preterm labor with (body weight, head circumference, body length, body mass index, tri-
symptomatic contractions and cervical ripening, premature rupture ponderal mass index [23] and body mass index), in terms of steady
of membranes or vaginal bleeding and exposed to antenatal beta- state characteristics, the unifactorial ANOVA with Kruskal-Wallis post
methasone (Celestan®, MSD GmbH, Haar, Germany) between hoc test was performed for two or more independent samples. For
23 weeks plus five days of pregnancy (23+5 weeks) and 33+6 weeks and repeated measures a MANOVA and Friedman post hoc test was used to
delivered between 25+0 and 36+6 weeks. Exclusion criteria were: high identify possible significant effects of different betamethasone dos-
numbered multiple pregnancies, twin-to-twin transfusion syn- ages on growth trajectories (growth percentiles, ponderal index and
drome, intrauterine death, malformations, chromosomal anomalies body mass index) in follow up data between U1 and U9 time points.
or other fetal or maternal diseases and pathological umbilical or Data are reported as median and interquartile range or mean and
uterine doppler findings. Fetuses with sonographically estimated standard deviation, as appropriate. Possible confounders were iden-
fetal weight below the 10th centile at the time of the initial betame- tified (Supplemental Material S4) and significant results were
thasone treatment were defined as small for gestational age and controlled for major confounders by analysis of covariance (ANCOVA).
excluded from the study to rule out possible growth restricting by an Statistical analyses were performed for overall, male-male, female-
already existing placental insufficiency [4]. Estimated date of de- female and mixed-pairs. For all tests, statistical significance was set at
livery was corrected by first trimester ultrasound when the difference pBraun et al.: ANS and follow up in twins 129 and 36+6 weeks of gestation, were included into the study (Figure 1). Seventy one (71.7%) women remained pregnant seven or more days after the initial betame- thasone treatment. Sixty children (30.3%) were born after 34+0 weeks of gestation. Maternal characteristics (Supplemental Material S4) were not associated with the observed changes in anthropometrics after beta- methasone exposure in multivariate analysis. Neither the number and distribution within the twin-pair structure nor its relation to the dosis-group was sig- nificant different (data not shown). Overall effects Overall weight percentile significantly decreased between U1 and U7/9 (U1: 45.5±28.1 centile vs. U9: 37.0±28.2 centile p=0.001; U7: 38.9±27.0 centile vs. U9: 37.0±28.2 centile p=0.027, Figure 2A). The length percentile increased be- tween U7 and U9 (U7: 43.3±31.0 vs U9: 48.0±31.0 p=0.001). The ponderal index as a marker for fat levels, continuously decreased between U1, U7 and U9 (U1: 22.6±2.7 vs. U7: 18.3±1.9 vs. U9: 13.1±1.1 p
130 Braun et al.: ANS and follow up in twins
Table : Betamethasone dosage effects on anthropometrics.
U ≤ mg mg > mg p-Valuea
Weight, g+ .±. .±(.) .±. .
n= n= n=
Weight percentile++ . (.)b . (.) . (.) .
n= n= n=
Length, cm++ . (.) . (.) . (.) .
n= n= n=
Length percentile++ . (.) . (.)d . (.) .
n= n= n=
Head circ., cm++ . (.) . (.) . (.) .
n= n= n=
Head circ. percentile++ . (.) . (.) . (.) .
n= n= n=
Ponderal index++ . (.)f . (.)g . (.)h .
n= n= n=
BMI+ .±.j .±.k .±.l .
n= n= n=
U ≤ mg mg > mg p-Valuea
Weight, g+ .± .±. .±. .
n= n= n=
Weight percentile++ . (.)c . (.) . (.) .
n= n= n=
Length, cm++ . (.) . (.) . (.) .
n= n= n=
Length percentile++ . (.) . (.)e . (.) .
n= n= n=
Head circ., cm+ .±. .±. .±. .
n= n= n=
Head circ. percentile++ . (.) . (.) . (.) .
n= n= n=
Ponderal index+ .±.f .±.g .±.i .
n= n= n=
BMI+ .±.j .±.k .±.l .
n= n= n=
U ≤ mg mg > mg p-Valuea
Weight, g++ () () () .
n= n= n=
Weight percentile++ . (.)b,c . (.) . (.) .
n= n= n=
Length, cm+ .±. .±. .±. .
n= n= n=
Length percentile++ . (.) . (.)d,e . (.) .
n= n= n=
Head circ., cm++ . (.) . (.) . (.) .
n= n= n=
Head circ. percentile++ . (.) . (.) . (.) .
n= n= n=
Ponderal index+ .±.f .±.g .±.h,i .
n= n= n=
BMI++ . (.)j . (.)k . (.)l .
n= n= n=Braun et al.: ANS and follow up in twins 131 Data presented as mean+ (standard deviation [SD]) and median++ (interquartile range [IQR]) for normally and non-normally distributed data, respectively. aKruskal–Wallis test, asymptomatic significance. Growth trajectories – weight percentile: ≤ mg: MANOVA for repeated measures p
132 Braun et al.: ANS and follow up in twins
Table : Antenatal betamethasone and the effects of anthropometry with respect to twin pair structure.
U Male-male Female-female Mixed p-Valuea Mixed p-Valueb
Male Female
++
Weight, g . () . () . () . .±. .±. .
n= n= n= n= n=
Weight percentile++ . (.) . (.)a . (.)a,f,g . . (.)o . (.) .
n= n= n= n= n=
Length, cm++ . (.) . (.) . (.) . . (.) . (.) .
n= n= n= n= n=
Length percentile++ . (.) . (.)d . (.)b,i,j . . (.)p . (.)r .
n= n= n= n= n=
Head circ., cm++ . (.) . (.)k . (.) . . (.) . (.) .
n= n= n= n= n=
Head circ. percentile++ . (.) . (.) . (.) . . (.) . (.) .
n= n= n= n= n=
Ponderal index+ .±.l .±.m .±.n . .±.t .±.u .
n= n= n= n= n=
BMI+ .±.v .±.w .±.x . .±.y .±.z .
n= n= n= n= n=
U Male-male Female-female Mixed p-Valuea Mixed p-Valueb
Male Female
+
Weight, g .±. .±. .±. . .±. .±. .
n= n= n= n= n=
Weight percentile++ . (.) . (.)e . (.)f . . (.) . (.) .
n= n= n= n= n=
Length, cm++ . (.) . (.) . (.) . .±. .±. .
n= n= n= n= n=
Length percentile++ . (.) . (.)h . (.)i . . (.)p,q . (.)r,s .
n= n= n= n= n=
Head circ., cm++ . (.)a . (.)a . (.)Braun et al.: ANS and follow up in twins 133 a Kruskal-Wallis test, cpairwise comparison p=., dpairwise comparison p=.. Data presented as mean+ (standard deviation [SD]) and median++ (interquartile range [IQR]) for normally and non-normally distributed data, respectively. aKruskal–Wallis test, asymptomatic significance. bMann Whitney U-test; Growth trajectories – weight percentile: female-female: MANOVA for repeated measures p=. (friedman’s two-way analysis of variance by ranks): eU vs. U p=.; mixed MANOVA for repeated measures p=. (friedman’s two-way analysis of variance by ranks): fU vs. U p=., gU vs. U p=.; length percentile: female-female: MANOVA for repeated measures p=. (friedman’s two-way analysis of variance by ranks): hU vs. U p=.; mixed MANOVA for repeated measures p
134 Braun et al.: ANS and follow up in twins
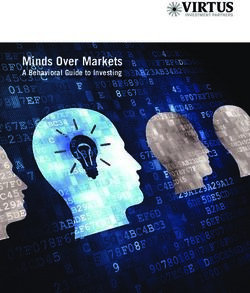
Figure 3: (A–C) Effects of different antenatal
bethamethasone dosages on growth
trajectories with respect to twin-pair
structure.
Data were analyzed by MANOVA for
repeated measures followed by Friedman
post hoc test. Significant differences
between time points are indicated by
stars/crosses. Head circumference
percentiles in >24.
mg and mixed ≤16 mg are not shown due too
low numbers. Data are presented as
mean±95%CI.
betamethasone dose group and not seen in the ≥24 mg pairs between U1 and U7 and let us speculate, that with
betamethasone dose group. Taking the twin pair structure regard to postnatal weight development, the dose of 24 mg
into account, birth weight percentiles did not change in antenatal betamethasone might be favorable to prevent
male-male pairs. In line with our previous observations in growth alterations in preterm twin pregnancies.
singletons [3, 26] and twins [4], sex-specific strategies for Body length percentiles significantly increased overall
adapting to changes in the uterine environment have been between infancy and early childhood by up to 10.9% (U7
described [27] and the present study supports our antenatal vs. U9 p=0.037). Body length percentiles in male-male
findings, that female-female and mixed pairs experience pairs were unaffected by antenatal glucocorticoid treat-
more growth restriction in response to prenatal betame- ment. However, in mixed pairs (U1 vs. U7, all three doses)
thasone than male-male pairs, which persisted beyond antenatal glucocorticoid treatment resulted in a significant
birth and early childhood. Only in female-female pairs decrease in body length percentiles between U1 and U7,
which had received ≤16 mg bethamethasone, birth weight independent of the betamethasone dose.
percentiles significantly decreased. ≥24 mg betamethasone The ponderal index is a relative stable measure of
actually increased weight percentiles in female-female adipose tissue (fat) levels in childhood and adolescenceBraun et al.: ANS and follow up in twins 135
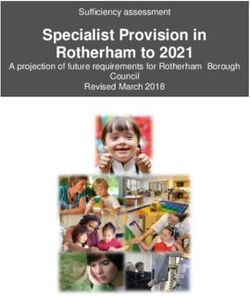
Figure 4: (A–B) Ponderal index (body weight
in kg/height in m³) and BMI (body weight in
kg/height in m2) in relation to
betamethasone dosis group and twin pair
structure.
Data were analyzed by MANOVA for
repeated measures followed by Friedman
post hoc test. Significant differences
between time points are indicated by
stars/crosses, data are mean±95%CI.
[28]. Rapid gain in ponderal index in infancy has been “physiological profile of normalization” of this index.
associated with increased obesity and adverse later Changes in BMI between 2 and 5 years have been reported
outcome such as cardiovascular disease [29, 30]. However, to be strongly associated with later adiposity and Howe
others reported less evidence for the changes in ponderal et al. suggested that BMI changes were also strongly
index in infancy but demonstrated a strong association of associated with increased fat mass, as well as with a range
rapid BMI change between 8.5 and 10 years of age and of cardiovascular risk factors at age 15 [31].
associate risk for cardiovascular disease [31]. We therefore We do acknowledge, that the BMI is associated with
analyzed the ponderal index as well as the changes of BMI both lean and fat mass in young children, however, in in-
after antenatal betamethasone in infancy and early child- fancy and childhood the BMI is an imperfect measure of
hood up to the age of 5.3 years. Interestingly, the ponderal adiposity. We therefore included the data for the ponderal
index significantly decreased between U1 and U9, inde- index and evidence from other cohorts suggests that BMI
pendent of twin pair structure or betamethasone dose. The has similar magnitudes of association to cardiovascular
BMI index, however, increased between U1 and U9 (≤16 and risk factors in childhood as does total fat mass assessed by
24 mg) and between U1 and U7 (≥24 mg), independent of DXA or waist circumference, suggesting that BMI may
twin pair structure, probably indicative of catch up growth adequately assess adiposity in childhood [31].
in length. Between U7 and U9, BMI trajectories signifi- There are limitations to our study. Uncontrolled data
cantly decreased again in male-male and female pairs collection and selection bias may be present in the ana-
with ≤16 mg and mixed pairs with 24 mg. These opposite lyses. However, due our large sample size, these effects are
BMI and ponderal index trajectories between birth and the unlikely to account for the differences observed. Although
age of five in twins after antenatal betamethasone treat- we used regression analysis to control for possible con-
ment were similarly observed earlier in singletons [32] and founding variables, the multiple factors affecting growth
seem to follow within a 2x standard deviation the make comparison of groups difficult and we acknowledge136 Braun et al.: ANS and follow up in twins
that additional factors affecting growth trajectories exist. Research funding: The study was supported by the
Unique strengths of our study are the large sample size; the “Stiftung für das behinderte Kind”, Schirmherrin Frau Dr.
exclusion of fetuses with EFW 24 mg betamethasone is not recommended. Further
Perinatol 1996;13:351–4.
studies are needed to understand the mechanism of 11. Blickstein I, Shinwell ES, Lusky A, Reichman B, Israel Neonatal N.
antenatal glucocorticoid treatment and its impact on Plurality-dependent risk of respiratory distress syndrome among
long-term development and morbidity, considering the very-low-birth-weight infants and antepartum corticosteroid
special needs in twin pregnancies. treatment. Am J Obstet Gynecol 2005;192:360–4.Braun et al.: ANS and follow up in twins 137
12. Crowley P. Prophylactic corticosteroids for preterm birth. antenatal betamethasone treatment and the role of human
Cochrane Database Syst Rev 1996:CD000065. https://doi.org/ placental lactogen. Placenta 2013;34:407–15.
10.1002/14651858.CD000065. 25. Liggins Institute. The University of Auckland New Zealand.
13. Ballabh P, Lo ES, Kumari J, Cooper TB, Zervoudakis I, Auld PA, et Antenatal corticosteroids given to women prior to birth to
al. Pharmacokinetics of betamethasone in twin and singleton improve fetal, infant, child and adult health. N Z Aust Clin Pract
pregnancy. Clin Pharmacol Ther 2002;71:39–45. Guidel 2015.
14. Gyamfi C, Mele L, Wapner RJ, Spong CY, Peaceman A, Sorokin Y, et 26. Braun F, Hardt AK, Ehrlich L, Sloboda DM, Challis JRG, Plagemann
al. The effect of plurality and obesity on betamethasone A, et al. Sex-specific and lasting effects of a single course of
concentrations in women at risk for preterm delivery. Am J Obstet antenatal betamethasone treatment on human placental 11beta-
Gynecol 2010;203:219 e1–5. HSD2. Placenta 2018;69:9–19.
15. Suhag A, Berghella V. What’s new in the multiple gestations 27. Challis J, Newnham J, Petraglia F, Yeganegi M, Bocking A. Fetal sex
literature?. J Perinat Med 2018;46:823–4. and preterm birth. Placenta 2013;34:95–9.
16. Bührer C. Perinatalerhebung 2013. Geburtshilfe Frauenheilkd 28. Peterson CM, Su H, Thomas DM, Heo M, Golnabi AH, Pietrobelli A,
2016;76:A4. et al. Tri-ponderal mass index vs body mass index in estimating
17. Gräfe D. Ped(z) Kinderarzt rechner; 2019. Available from: https:// body fat during adolescence. JAMA Pediatr 2017;171:629–36.
www.pedz.de/de/bmi.html. 29. Ong KK, Loos RJ. Rapid infancy weight gain and subsequent
18. Kromeyer-Hauschild K, Wabitsch M, Kunze D, Geller F, Geiß HC, obesity: systematic reviews and hopeful suggestions. Acta
Hesse V, et al. Perzentile für den Body-mass-Index für das Kindes- Paediatr 2006;95:904–8.
und Jugendalter unter Heranziehung verschiedener deutscher 30. Ong KK, Emmett P, Northstone K, Golding J, Rogers I, Ness AR,
Stichproben. Monatsschr Kinderheilkd 2001;149:807–18. et al. Infancy weight gain predicts childhood body fat and age
19. Heese V, Schnabel O, Judis E, Cammann H, Hinkel J, Weissenborn at menarche in girls. J Clin Endocrinol Metab 2009;94:
J. Longitudinal study of the growth of German children aged 0 to 6 1527–32.
years: Part 2. Monatsschr Kinderheilkd 2016;164:892–912. 31. Howe LD, Tilling K, Benfield L, Logue J, Sattar N, Ness AR, et al.
20. Heese V, Schnabel O, Judis E, Cammann H, Hinkel J, Weissenborn Changes in ponderal index and body mass index across
J. Longitudinal study of the current growth of German children childhood and their associations with fat mass and
aged 0 to 6 years: part 1. Monatsschr Kinderheilkd 2016;164: cardiovascular risk factors at age 15. PLoS One 2010;5: e15186.
478–96. 32. Carrascosa A, Yeste D, Moreno-Galdo A, Gussinye M, Ferrandez A,
21. Heese V, Schnabel O, Judis E, Cammann H, Hinkel J, Weissenborn Clemente M, et al. [Body mass index and tri-ponderal mass index
J. Longitudinal study of the current growth of German children of 1,453 healthy non-obese, non-undernourished millennial
aged 0 to 6 years: part 3. Monatsschr Kinderheilkd 2017;165: children. The Barcelona longitudinal growth study]. An Pediatr
148–70. 2018;89:137–43.
22. Braegger C, Janni O, Konrad D, Molinari L. Neue 33. van Dommelen P, de Gunst M, van der Vaart A, van Buuren S,
Wachstumskurven für die Schweiz. Paediatrica 2011;22:9–11. Boomsma D. Growth references for height, weight and body mass
23. Ashley-Martin J, Ensenauer R, Maguire B, Kuhle S. Predicting index of twins aged 0–2.5 years. Acta Paediatr 2008;97:1099–104.
cardiometabolic markers in children using tri-ponderal mass
index: a cross-sectional study. Arch Dis Child 2019;104:577–82.
24. Braun T, Husar A, Challis JR, Dudenhausen JW, Henrich W, Supplementary Material: The online version of this article offers
Plagemann A, et al. Growth restricting effects of a single course of supplementary material (https://doi.org/10.1515/jpm-2020-0204).You can also read