LIVERPOOL COVID-SMART COMMUNITY TESTING PILOT - STRONGERTOGETHER TESTINGTOGETHER
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Liverpool Covid-SMART
Community Testing Pilot
Evaluation Report I 17 June 2021
Stronger Together Testing Together
Liverpool Covid-SMART Community Testing Pilot
This report Inputs to the report have been combined
from the pilot delivery partners and the
This is the report from an evaluation led by
evaluation group:
the University of Liverpool into the Liverpool
pilot of community open-access testing Pilot delivery partners: Liverpool City
for the Covid-19 virus SARS-CoV-2 among Council; NHS Test and Trace (DHSC); Army
those without symptoms. The evaluation (8 Engineer Brigade); NHS Liverpool Clinical
was invited by the joint local and national Commissioning Group; Merseycare NHS
command of the pilot and sponsored by Trust; Cheshire & Merseyside Health & Care
the Department of Health and Social Care Partnership; Merseyside Local Resilience
(DHSC). Forum; Liverpool Charity and Voluntary
Services (LCVS).
This report extends an interim report
published 23 December 2020,1 and presents Evaluation partners: The University of
findings to help policymakers with Liverpool; Public Health England; Joint
community approaches to Covid-19 testing. Biosecurity Centre; Office for National
Statistics (ONS); NHS Test and Trace; Scientific
Advisory Group for Emergencies (SAGE) and
its contributing universities.
Liverpool
Clinical Commissioning Group
Liverpool Mersey Care
Clinical Commissioning Group NHS Foundation Trust
Liverpool Mersey Care
NHS Foundation Trust
Clinical Commissioning Group
Mersey Care
NHS Foundation Trust
2
Liverpool Covid-SMART Community Testing Pilot
CONTENTS
EXECUTIVE SUMMARY 6
THE PILOT 8
Background 8
Approach 8
Goals 8
Governance 8
Multi-agency working within Liverpool 10
Data and intelligence 10
Community engagement and communications 11
Timeline of the pilot 12
Summary of test numbers 13
EVALUATION FRAMEWORK 16
ETHICS AND APPROVALS 17
SYSTEMS 18
Aim 18
Key findings 18
Sources and Methods 18
Multi-agency working 18
Governance and operations 18
Adapting operations according to intelligence 19
Sustainability and knowledge transfer 19
Digital access, dataflows and intelligence 20
Communications and community engagement 21
System developments from 3 December 2020 23
Sector specific arrangements 23
Scale and sustainability 24
BIOLOGY 25
Aim 25
Key findings 25
Performance of the Innova SARS-CoV-2
Antigen Rapid Lateral Flow Test 25
3
Liverpool Covid-SMART Community Testing Pilot
Sources and methods 25
Findings 26
Repeated lateral flow testing 27
Confirmatory PCR tests 28
Symptomatic individuals 29
New variants 29
Schools testing and plausibility of self-reported results 30
Device handling, reading and labelling 30
Repeated testing 31
BEHAVIOURS 31
Aim 31
Key findings 31
Overall testing 32
Sources and methods 32
Testing site attendance survey 32
News and social media analysis 32
Interviews with those who did vs did not take part
in testing 33
Findings 33
Awareness of and attitudes towards testing 33
Motivators, facilitators and barriers to participation 34
Perceptions of access to testing 36
Response to a positive test result 36
Response to a negative test 37
Behavioural responses to testing in specific contexts 38
Enhanced test-to-protect in care homes 38
Sources and methods 38
Findings 38
Test-to-release for key workers 39
Sources and methods 39
Findings 39
Test-to-enable in schools 40
Sources and methods 40
Findings 40
4
Liverpool Covid-SMART Community Testing Pilot
Behaviours impacting systems of testing
in specific settings 41
Care homes 41
Aim 41
Sources and methods 41
Findings 41
Workplaces: SMART-release (daily contact testing) 43
Aim 43
Sources and methods 43
Findings 43
PUBLIC HEALTH 45
Aim 45
Key findings 45
Sources and methods 46
Background 46
Data 46
Statistical analyses 47
Findings 52
Uptake 52
Case detection 58
Simulation of plausible impact on infections 58
Impact on transmission 59
Impact on hospitalisation 60
REFERENCES 61
GLOSSARY 64
APPENDIX: PUBLICATIONS 65
FURTHER INFORMATION 66
5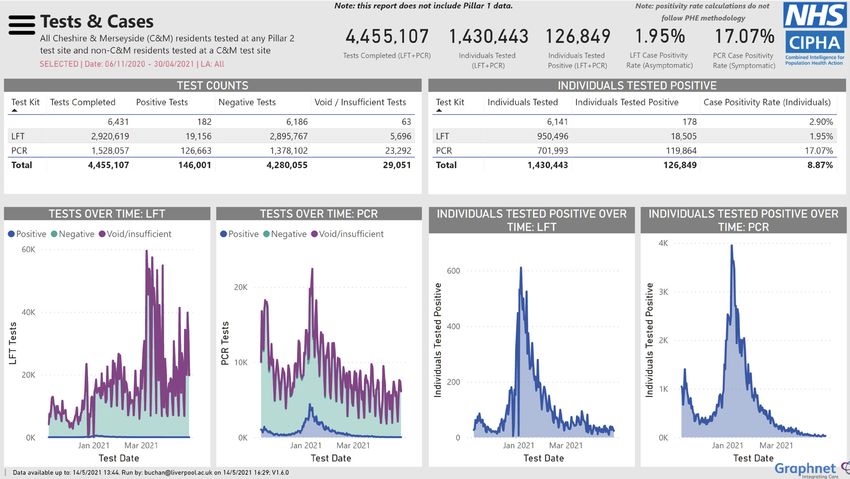
Liverpool Covid-SMART Community Testing Pilot
Military personnel instructing medical staff on Covid-19 testing procedure at Wavertree Tennis Centre
EXECUTIVE SUMMARY
The City of Liverpool and national agencies • Repeated: fit testing regimens to
partnered to pilot community testing for transmission, consequences and the scale
SARS-CoV-2 antigen, open to all people of testing
without symptoms of Covid-19, living or
• Testing: quality assure end-to-end not just
working in the City.
biological performance of lateral flow test
Community testing was valuable as part of (LFTs)
an agile, intelligence-led local public health
SMART targets: test-to-protect (vulnerable
intervention. We recommend a SMART
individuals/settings/services), test-to-release
(Systematic, Meaningful, Asymptomatic/Agile,
(sooner from quarantine), and test-to-enable
Repeated Testing) approach:
(safer return to key activities for social fabric
• Systematic: end-to-end system-wide, from and the economy).
intention, to test, to adequately supported
Between 6 November 2020 and 30 April
isolation
2021, 283,338 (57%) Liverpool residents took
• Meaningful: clear, action-focused meaning a test using the Innova SARS-CoV-2 antigen
and equity of access/use across the whole rapid antigen lateral flow device (LFD). Of
population these, 47% had more than one test (27% of
residents), and in the same period, 152,609
• Asymptomatic/Agile: plus (pauci-)
residents were tested by PCR.
symptomatic and rapid contact testing; flex
to prevailing needs • 6,300 individuals declaring no symptoms
tested positive by LFT (case positivity 2.1%)
6
Liverpool Covid-SMART Community Testing Pilot
• 22,567 individuals declaring symptoms actions across NHS, local authority and
tested positive by PCR (case positivity 14.8%) public health agencies and their partners –
informing multi-agency Gold/Silver/Bronze
The estimated impacts (with 95% confidence
command-and-control structure. The role
intervals) of Liverpool’s community testing
of the Director of Public Health was vital
compared with other areas were:
to effective coordination of services and
• 18% (7% to 29%) increase in case detection engaging the public.
vs control areas
A low-cost, rapid, no-lab test of
• 21% (12% to 27%) reduction in cases up infectiousness saves time and extends the
to mid-December (after which the Kent reach of health protection measures. SARS-
variant surge made it difficult to compare CoV-2 antigen rapid lateral flow testing
areas) vs control areas meets this need when coordinated by an
• Pessimistic model suggests 850 (500 to effective local public health service. The end-
1350) infections were prevented to-end testing service was found valuable
and has been continued beyond pilot as a
• Optimistic model suggests 6600 (4840 to
core part of Liverpool’s Covid-19 response.
9070) infections were prevented
• Small but non-significant reduction in
hospital admissions
Socio-economic inequalities were a
substantial challenge. Test uptake was lower
and infection rates were higher in deprived
areas, in areas with fewer digital resources or
lower digital literacy, and among non-White
ethnic groups. Fear of income loss from self-
isolation was a key barrier to testing.
The LFD worked as expected, identifying
most cases with high viral load, likely to be
most infectious.
There was strong public awareness of,
and a largely positive attitude toward
community testing, motivated by shared
identity, civic pride and a wish to protect
others. Misinformation, particularly over
test performance was a substantial problem
needing intensive local communications to
address.
Multiple national testing initiatives in
different contexts from care homes
to schools and workplaces made
communication too complex and would have
been better integrated into a community
testing with integrated support from the
local authority. Shared data/intelligence (e.g.,
www.cipha.nhs.uk) was vital for coordinating
7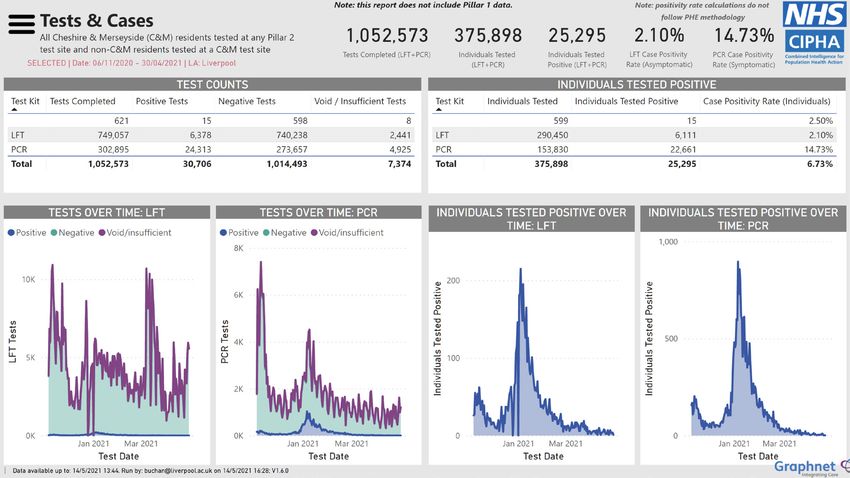
Liverpool Covid-SMART Community Testing Pilot
THE PILOT 2. ‘test-to-release’ contacts of confirmed
infected people sooner from quarantine
than the stipulated period (for example,
Background key workers in quarantine); and
The Department of Health and Social Care 3. ‘test-to-enable’ careful return to restricted
(DHSC) approached Liverpool City leaders activities to improve public health, social
on 31 October 2020 offering Covid-19 fabric, and the economy (for example,
testing for everyone living or working in visits to care homes or sports events).
Liverpool, regardless of whether they had
From 3 December 2020, a more targeted
symptoms. The initial offer to test 75% of the
approach was taken to implementing SMART
asymptomatic population in two weeks with
in response to changing Covid restrictions
military assistance was renegotiated by the
and infection levels and patterns.
city to a serial testing approach, with value
seen in having access to large-scale, flexible
testing for coronavirus control and socio- Goals
economic recovery. Preparations started on 1
November 2020. Pre-publication information Partners set a mission to:
on the testing device (Innova SARS-CoV-2 “To identify the virus, wherever it is in the City,
lateral flow) that had already been purchased and empower local communities to suppress
nationally was made available. The pilot its transmission while being supported well
plan was agreed on 5 November 2020 as when they need to isolate or quarantine.
national lockdown started, and testing At the same time, to identify those who are
commenced on 6 November 2020 as a needlessly self-isolating and empower them
collaboration between NHS Test & Trace, to return to usual activities.”
Liverpool City Council, NHS Liverpool Clinical
The goals were
Commissioning Group, the Army (8 Engineer
Brigade), Cheshire & Merseyside Health & 1. saved lives and improved health
Care Partnership and Liverpool Charity and outcomes for the City’s residents;
Voluntary Services, with evaluation led by 2. saved livelihoods and businesses,
The University of Liverpool with NHS Test protecting the City’s economy and social
and Trace, Public Health England (PHE), the fabric; and
Joint Biosecurity Centre (JBC) and Office for
National Statistics (ONS). 3. sooner and safer reopening of the City as
a whole.
Approach
Governance
The pilot was originally called MAST (mass,
asymptomatic, serial testing), and the name Partners established a Gold/ Silver/Bronze
was later changed to SMART (systematic, Command-and- Control system: Gold set the
meaningful, asymptomatic/agile, repeated direction and was responsible for the pilot;
testing) to better reflect the partnership’s Silver led the delivery and coordination of the
approach to testing. pilot; Bronze provided operational control
for the pilot, in collaboration with the Army.
SMART has three components: Bronze, Silver and Gold teams met daily to
1. ‘test-to-protect’ vulnerable people and review situations, assess risks, make decisions,
settings (for example, people living in care and deploy operations.
homes);
8
Liverpool Covid-SMART Community Testing Pilot
This Command-and-Control has delegated A STAC (Science and Technical Advice Cell)
mandates from the Mayor of Liverpool and was established on 6 November 2020 as part
Liverpool Local Authority Chief Executive of the Merseyside Local Resilience Forum
Officer, Merseyside Local Resilience Forum governance structure and reported into
(LRF), Merseyside Test & Trace Cell, Cheshire the Command-and-Control system. STAC
& Merseyside Testing Cell, and Cheshire members were drawn from PHE, DHSC,
& Merseyside Health & Care Partnership NHS Test and Trace, University of Liverpool,
Combined Intelligence for Population University of Oxford, and Liverpool City
Health Action (CIPHA, www.cipha.nhs.uk) Council. All testing operations conformed
Governance Board. The Command-and to NHS Test and Trace Clinical Framework
Control structure sits within North West Standard Operating Procedure (SOP), and
region’s Incident Coordination Centre (ICC). queries about it were directed via STAC.
Military support maintained a parallel
operational governance to the Command-
and-Control structure, under a formal
MACA (Military Aid to the Civil Authorities)
protocol (to 6 December 2020). Military
representatives were embedded in the MAST
Command-and-Control at all three levels.
Figure 1: Command-and-control structure
GOLD SILVER BRONZE
• Strategic leadership / • Manage Bronze operations • Implement operational deliverables
national oversight • Manage communications / • Manage inter-dependencies /
• Oversee / assure testing messaging relationships on the ground
at high level • Inter-dependencies and
• Co-ordinate lessons learned and
• Set objectives organisational co-ordination
produce how-to guide
• Make strategic decisions • Project governance
• Identify and operationalise sites /
• Define scope / approach • Tactical/operational decisions
workforce
• Assurance to Gold
• Develop sustainability and
• Evaluation/lessons learnt
transition plans, and civilian
• Quality standards operating procedures and
• Options considered and processes
preferred • Protect vulnerable groups
• Recommend to Gold for
decision
9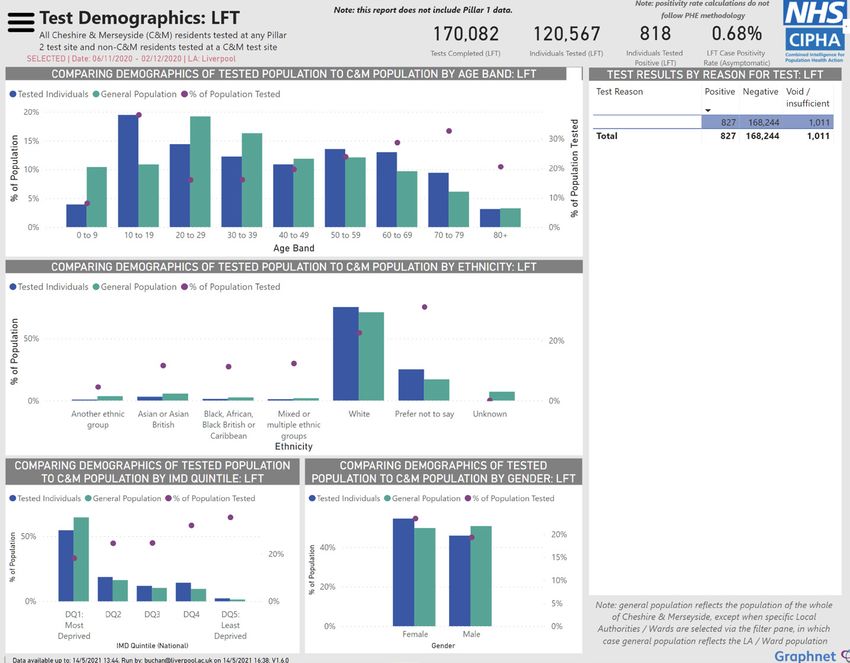
Liverpool Covid-SMART Community Testing Pilot
Multi-agency working within Liverpool of the second and third phases of further sites
for ATS required more complex negotiation
In March 2020, the Local Resilience Forum
with site owners and DHSC. The process was
system, managed centrally by the Ministry of
informed by combined intelligence from the
Housing Communities and Local Government
CIPHA system and analytic expertise from
(MHCLG), was operationalised in response to
military, City Council and University partners.
Covid-19. Strategic and Tactical Coordination
Groups were stood up, and supporting cells
created. These brought together representatives
from local organisations responsible for service
planning and delivery. Local Authorities, such
as Liverpool City Council, also activated their
own Covid-19 coordination groups. This is how
Liverpool City Council responded quickly to the
approach from DHSC outlined above.
Pilot planning was overseen by Liverpool City
Council Covid-19 Strategic Coordination Group
with DHSC ahead of the Command-and-Control ©Jennifer Bruce, Liverpool City Council
system being activated on 6 November 2020. Military personnel constructing a testing station
The DHSC, as pilot sponsor, provided the Following a briefing on Thursday 8 November
initial directive to the military unit (8 Engineer 2020 for secondary school headteachers to
Brigade) to establish 48 new asymptomatic prepare for testing at schools, an opt-in consent
testing sites (ATS) in the City of Liverpool using process was agreed. However, one school (not at
pre-purchased Innova lateral flow devices. Two the briefing) misunderstood their school would
military staff were seconded to DHSC to act as begin testing on the following Monday and
liaison. The role of the DHSC during the pilot sent an opt-out letter to parents on the Friday.
was to approve the location of test sites, provide Although this was recalled and replaced with
financial indemnity for site operators, approve an opt-in letter on Sunday, it fuelled negative
costings, lead initial clinical governance, and discussion on social media, which damaged
establish an evaluation steering group. uptake of testing at schools.[1] Rates of consent
Approximately 2,000 personnel from 8 Engineer varied considerably by school. An average
Brigade arrived on Merseyside by 2 November of 52.6% of pupils at participating secondary
and established an operational headquarters at schools (31 out of 33) were tested. A total of 32,411
HMS Eaglet in Liverpool. Liverpool City Council’s tests (84% pupils; 16% staff) were done at schools
Assistant Director for Supporting Communities in the period to 2 December 2020.
was designated as military liaison officer, leading
local negations over ATS and linking the military
Data and intelligence
into the Command-and-Control structure.
Each person tested was asked questions and
Six initial ATS were in Liverpool City Council
a record was created for getting result back
premises as these could be approved quickly.
to them, and for monitoring the programme.
Military personnel took responsibility for the
Registration involved linking individuals to test
buildings and set up the testing infrastructure
kits via a unique identifier (bar coded). For PCR,
(signage; registration desks; testing booths;
swabs were sent to laboratories and results
queueing systems) on 5 November 2020 for start
returned around 24 hours later. LFTs were
the next day. The selection and confirmation
processed (see LFT Process) at the testing sites
10Liverpool Covid-SMART Community Testing Pilot
Lime Street digital screen
and results sent approximately 30-60 minutes Community engagement and
later by text message or email, including the communications
required actions depending on whether the
The aim to engage the city’s whole population in
result is positive or negative. The national
the pilot drove DHSC’s estimate of 48 test sites
guidance for positive individuals was the same
(20 bays testing 6 people per hour from 07:00 to
for LFT and PCR and did not change over the
19:00 each day to generate a capacity of 69,120
pilot. A supplementary local text message
tests – around 14% of the population per day).
for LFT positives was added on 23 November
2020 to overcome logistical challenges with A communications plan was developed
confirmatory PCR described later. and delivered by Liverpool City Council. This
employed multimedia strategies and was
Test results flowed from NHS Test and Trace,
updated in response to data on testing uptake,
via NHS Digital, into the regional combined
feedback from the military on engagement at
NHS, local authority care and public health
ATS, analysis of social media and commissioned
data/intelligence system CIPHA, which was
surveys. An interactive map of ATS was deployed
established across Cheshire & Merseyside in
on Liverpool City Council website to show
May 2020 as a Covid-19 response from the
waiting times at sites.
NHS Out of Hospital and Hospital Cells with
NHSX support. CIPHA aligns with NHS Covid Discussion at Gold/Silver/Bronze command
Phase 3 directions on local integrated care levels translated into communications plans
data and is designed to support multi-agency for informing residents of uptake (daily press
working in the Cheshire & Mersey Health & Care releases via the Liverpool Express website;
Partnership. regular media appearances by the Director of
Public Health and other senior stakeholders).
Dashboards were established by CIPHA for
the pilot, providing reports updated every In the third week of the pilot, Liverpool City
30 minutes on testing by sites and socio- Council liaised with Liverpool Charity and
demographic groups. In addition to on-line Voluntary Services [LCVS] organisation to target
dashboards, summaries were emailed three specific neighbourhoods with low attendance
times per day to the Command-and-Control at ATS. A funding request for community
members and field teams and used to inform involvement in co-creating testing engagement,
the evolution of the testing site network. incentives, and support, including tackling
inequalities, was submitted to DHSC.
11Liverpool Covid-SMART Community Testing Pilot
Timeline of the pilot • (13) First meeting of the University of
Liverpool evaluation group
The preparation phase and three main
implementation phases covered by this report • (20) Re-configuration of resources: 15
map largely to the following months and public popular ATS kept; other resources were
messages: 1) November 2020 “Let’s All Get redeployed to smaller ATS in low uptake
Tested”; 2) December 2020, “Test Before You Go”; areas
3) January-April “Testing Our Front Line”.
• (23) System for confirmatory PCR changed
OCTOBER from national communication and delivery
of a home test kit to swabbing at one
• (14) The new three-tier system of Covid-19 designated local testing site (with outreach
restrictions begins in England; with Liverpool swabbing if needed) and an invitation
City Region in Tier 3, the highest level of message tailored to the local area
restrictions at the time
DECEMBER
• (31) Government offers Liverpool mass testing
with military assistance • (2) Liverpool moved into Tier 2 with all
surrounding regions in higher Tiers /
NOVEMBER restrictions.
• (1) Liverpool City Council Covid-19 Strategic • (3) Handover of management of ATS from
Coordination Group with Mersey Resilience military to Liverpool City Council contractors;
Forum accepts in principle but with the targeting becomes more focused as the pilot
freedom to develop a more targeted moves to Liverpool Covid-SMART and adapts
approach to fewer Covid-19 restrictions
• (2) Military arrive in Liverpool to establish test • (3) Liverpool Covid-SMART care home visiting
sites pilot begins; and the communications plan
• (3) Liverpool accepts a MAST; an emergency shifts priority to “test before you go” for
response is stood up implementation as the population returned
to high transmission risk settings such as
• (5) National lockdown; a communications hairdressers
drive begins in Liverpool on MAST
• (4) Liverpool Covid-SMART test-to-release for
• (6) Six ATS open for LFT testing (alongside some key workers begins
mobile units for symptomatic PCR testing,
which were already operating); QA teams for • (17) More areas including Cheshire and
dual LFT PCR swabbing mobilised Warrington move into Tier 2. Hotels in
Liverpool booked heavily with people from
• (7) 16 ATS open for LFT testing London.
• (10) First meeting of DHSC convened • (31) Move back into Tier 3 with all surrounding
Evaluation Steering Group; schools-based regions in Tier 4.
testing starts
JANUARY 2021
• (11) Capacity increased: 37 community ATS
plus schools; home PCR kits delivered • (4) National lockdown
(one-off, unsolicited mailing to sample MARCH 2021
households); local evaluation group
established • (8) Schools and colleges return with twice
weekly rapid antigen testing
12Liverpool Covid-SMART Community Testing Pilot
Summary of test numbers
Test numbers for Liverpool City residents from 6 November 2020, the start of the pilot, until 30 April
2021 are shown in Figure 2. The PCR test numbers represent both symptomatic and asymptomatic
uses, as a large one-off postal drop of home PCR kits was made from 11 to 16 November.
Figure 2: Summary testing dashboard for the City of Liverpool (0.5m population)
Equivalent numbers for the wider Cheshire & Merseyside region, where people working in
Liverpool may live, are shown in Figure 3.
Figure 3: Summary testing dashboard for Cheshire and Merseyside (2.6m population)
13Liverpool Covid-SMART Community Testing Pilot
The phases of the pilot dictated by prevailing infection patterns and changes to Covid-19 restrictions,
as seen through the dashboards that the pilot teams used to coordinate actions are shown below
(detailed results behind the captions are given later in the Public Health chapter):
Figure 4: Socio-demographic summary of testing in the pilot’s first month from 6 November 2020
Quarter of population tested
‘mass testing’ first month
with military assistance
#let’s all get tested
Lower uptake in young adults
Lower uptake in non-Whites
Lower uptake in males
Half uptake in most vs least
deprived fifth of population
Figure 5: Socio-demographic summary of testing with Liverpool in Tier 2 in December 2020
Tier 2 month
using local testing service/staff
#test before you go
Increased uptake in young adults
14Liverpool Covid-SMART Community Testing Pilot
Figure 6: Socio demographic summary of Liverpool testing in Lockdown in early 2021
SMART testing in lockdown
using local testing service/staff
#testing our front line
Uptake among non-White groups
increases
Uptake among deprived
communities increases
(workforce in lockdown)
Figure 7: Socio demographic summary of Liverpool testing after schools return in March 2021
SMART testing in lockdown
#testing our front line
alongside schools testing
Secondary schools testing
Ethnic inequalities reduce
Lockdown worker and schools
testing flatten social gradients
15Liverpool Covid-SMART Community Testing Pilot
EVALUATION FRAMEWORK 2. BIOLOGY: To evaluate:
The DHSC, as sponsor for the pilot, established a) the performance of the Innova LFT in
an Evaluation Steering Group, which ran from context of use
November to December 2020 with inputs b) the uptake and utility of PCR tests to confirm
from SAGE, NHS Test and Trace, ONS, PHE, positive results from LFTs
JBC, and academic specialists. The University
of Liverpool was invited to lead the evaluation c) repeated testing for test-to-protect (the
on 10 November 2020. The national Testing vulnerable); test-to-release (from quarantine;
Initiatives Evaluation Board – formed in isolation) and test-to-enable (safe return to
January 2021 – later reviewed outputs from usual activities)
the University of Liverpool evaluation team. A
framework was adopted for evaluating four
3. BEHAVIOURS: Understand the factors
principal components of community testing:
determining:
1) operational systems, 1) biological meaning,
3) behavioural responses, and 4) public health a) uptake of tests on first and subsequent
impacts. occasions, by socio-demographic groups
b) acceptance of the testing programme
by the public in general and by specific
1. SYSTEMS: Develop nationally generalisable
vulnerable groups
systems for:
c) drivers for accessing or declining testing for
a) establishing pathways - identifying who
an individual and those they care for
to test, communicating the need for a
test, taking the test, carrying out the test, d) responses to a positive test result
communicating the result to the person e) responses to a negative test result
tested and to others who need to know, and
ensuring that appropriate next steps happen f) effective and ethical incentives for
participation
b) combining intelligence from NHS, local
authority, and public health data sources for g) public trust, understanding, and cooperation
promoting and optimising access to testing
for specific groups
4. PUBLIC HEALTH: Identify the public health
c) multi-agency mutual aid to coordinate impacts on:
communications, public health responses
a) uptake overall and by gender, age,
and economic recovery activities
geographical area, deprivation, ethnicity,
d) delivering strong community engagement occupation, high risk and vulnerable groups
e) providing clear, impartial, and accurate b) tackling inequalities in the uptake of testing
information to the community, which and its effects
explains the purpose of testing in this
c) virus transmission during the pilot and
context
beyond
f) assessing the indirect effects of the pilot on
d) protecting vulnerable groups
other systems such as welfare support and
clinical pathways e) contact-tracing of cases and their contacts
f) the proportion of the population who isolate
or quarantine
16Liverpool Covid-SMART Community Testing Pilot
g) compliance with isolation, and consequently ETHICS AND APPROVALS
transmission
This work was invited as a service evaluation
h) unintended consequences, such as a not research. DHSC/NHS Test and Trace wrote
potential reduction in Covid-safe behaviours confirming the status as service evaluation
after a negative test and liaised with the Medicines and Healthcare
This was a rapid evaluation of a developing pilot Devices Regulatory Authority (MHRA) over the
with after-action, continuous learning at the use of the Innova lateral flow device in this post-
forefront. It was not always possible to examine validation pilot service.
and mitigate systematic biases from data Whether MAST/SMART was ‘a screening process’
collection. or ‘an emergency public health intervention
This was a rapid evaluation of a developing pilot during an extraordinary event’ was discussed
with after-action, continuous learning at the by the evaluation team and with DHSC.2,3 A
forefront. It was not always possible to examine distinction was drawn between identification of
and mitigate systematic biases from data cases of non-communicable disease dispersed
collection. in the community and primarily impacting
the person tested (e.g., cervical cancer), and
Qualitative and survey work on the ground identification of cases of a highly infectious
was targeted at explaining differences in test disease that by its nature amplifies within a
uptake therefore it should not be interpreted community with wider societal impacts. It was
as representative of the general population. agreed without dissent that MAST and SMART
ONS survey work was undertaken to generate a were urgent public health interventions subject
representative sample. to the legal and ethical provisions of a health
The timing of the pilot meant that it was not protection activity and Covid-19 specifically.
possible to design a priori, sophisticated control With reference to the Health Research Authority
comparisons or establish randomised testing decision tool, the secondary analysis of data
patterns to build strong causal inferences provided in a health protection activity is not
on impacts of the testing on public health classified as research, and so does not require
outcomes or behavioural processes. research ethics committee review.4
This evaluation used routinely collected The quality assurance sample of dual LFT and
data and field observations, which might be PCR swabs was run as quality management of
replicated in other localities. The framework the service of NHS Test and Trace, with the data
is intended for formative use in guiding provided to the evaluation team for secondary
implementations of similar testing in other analysis of data provided in a health protection
localities, and for providing immediate activity.
summative policy evidence.
Where additional information required
interactions that were not a routine part of the
pilot service, local research ethics committee
approvals were obtained.
17Liverpool Covid-SMART Community Testing Pilot
SYSTEMS communities, and their practical support
(food hampers, collection services) reduced
Aim
the demand on LCC services (evidenced by
The aim was to understand the human a reduction in the number of calls to the LCC
and technical systems required to deliver helpline compared with the first lockdown
community testing in an end-to-end, civic period).
operation as part of wider Covid-19 measures.
The VCF [Voluntary, Charity and Faith]
sector organisations agreed to participate in
Key findings expectation of prompt reimbursement through
the LCVS/LCC contract. However, no payment
The handover period from the military in was made to LCVS during the period to 31
December 2020 was extremely tight. The March 2021. Many VCF organisations operate on
transition team should have been engaged very small financial margins and struggled to
much earlier. support their members during the pilot.
The management of clinical waste was not The CIPHA integrated data and shared analytics
included in the SOP and local registered waste system was vital as a single source of truth
contractors had to be brought in and outlets across NHS, public health, local authority and
found at short notice. academic organisations in coordinating and
Signage for the ATS, in terms of quantity and evolving the pilot.
timeliness of delivery, was a problem from the
start. It was a large and complex requirement,
which after internal delays had to be re-allocated Sources and methods
to an external contractor. The governance and operations systems
Although site accessibility was considered when were evaluated using material created by the
sites were selected, further issues needed to be Command-and-Control structure, and with
addressed such as wheelchair access, availability reference to individual discussions with key
of sign language trained staff and translators. stakeholders.
Questions about occupation in test booking
forms were often left unanswered, which Multi-agency working
hindered the ability to monitor uptake of LFTs by
Governance and operations
key worker groups.
The speed with which the pilot was established
Training in the use of LFTs for the pilot
(seven days from agreement to opening of first
extensions (schools, MFRS, Police, prison staff)
ATS) created logistical challenges. The initial
was initially managed by ATS personnel. Training
DHSC estimate of 48 geographically spread
co-ordination was later taken over by Liverpool
sites had to be revised with reference to local
City Council (LCC) who had important local
intelligence on Liverpool’s neighbourhoods
contextual knowledge of each setting.
and practical issues such as site ownership and
Financial management was ad hoc in the first access.
two months. It would have been preferable to
The governance structure was responsive to
have appointed a dedicated finance officer at
the fast-moving process. Verbal agreements
the start of the pilot.
were accepted for some actions to enable site
Anecdotal feedback from LCVS partners set-up. Command-and-Control action logs were
suggests that their support activities mobilised not fully operational until 11 November 2020
an increased number of LFTs in hard-to-reach and governance frameworks were not finalised
18Liverpool Covid-SMART Community Testing Pilot
until 13 November 2020. The military command bookings for positive LFT cases, and alerting
logged every operational decision within their DHSC to a communications failure on the postal
own system. drop of PCR kits to Liverpool Households.
Local organisations were already working NHS Test and Trace introduced a home PCR
together effectively and efficiently through the test delivery to addresses that were more than
Cheshire & Merseyside joint Covid-19 cells across 800m from a testing site. This was centrally
the two constituent LRFs. The governance and directed, and the local authority were advised
operational structures for the pilot therefore of the postal districts chosen by DHSC via their
drew on existing knowledge and networks. The national delivery partner company. The provision
co-chairs of the Gold/Silver/Bronze levels were of home PCR test kits was preceded by a letter
drawn from different organisations, resulting in with guidance sent by NHS Test and Trace up to
smooth identification and solution of emerging two days in advance of the Home Test kits being
issues. delivered by Amazon. Three home test kits were
sent in each parcel, with a total of 85,062 kits
being delivered to 28,354 households over 4
Adapting operations according to intelligence ‘Sprints’. The postal districts were L16, L25, L12,
An early adaptation was the rapid deployment L24 and L14, but did exclude addresses which
of clinical staff from local NHS organisations were within the radius of a testing centre.
to the ATS to ensure compliance with the As the completed home test kits had to be
clinical standard operating procedures and submitted through post boxes, to mitigate Royal
surveillance of attendees for vulnerable and Mail boxes being overwhelmed, Liverpool was
potentially symptomatic individuals. The initial asked to provide ‘collection points’ for the test
queues at the ATS on 6 and 7 November were kits for the day of delivery and the day following
effectively managed by the Council, who used the delivery. At the busiest point 12 vans were
their external stewarding contractor to supply provided in the identified areas to collect kits
additional staff. from residents between 08:30 and 17:00 and
At the start, existing Mobile Testing Units were then taken to a single point to transfer
(MTUs) for symptomatic testing and the pilot to Royal Mail who then delivered them to a
ATS were managed separately. This was quickly Lighthouse laboratory.
identified as a discoordination risk, so the Of the 85,062 kits delivered, 8,914 (10.5%) were
two systems were integrated at local level via registered by residents and 7,024 (8.3%) results
Bronze Command, with clearer signage for were provided. Of the kits registered 3,428 were
the three out of 37 community venues where collected over the four sprints by the collection
there were both types of testing available. The vans, all other completed kits would have been
communications plan was adapted to clarify the submitted via the post boxes. In response to the
purpose of each type of site, their location, and low registration numbers, a change was made
opening hours. centrally from 17 November 2020 to only send a
The DHSC approvals were streamlined by letter to household occupiers informing them of
bringing the Senior Regional Coordinator how to request a home test kit.
North West into the local Command-and-
Control structure (from the second week)
Sustainability and knowledge transfer
and identifying DHSC staff to act as conduits.
This enabled operational issues to be quickly The decision to continue LFT testing beyond
addressed, including facilitating the use of local the agreed period of military support placed
telephone numbers for follow-up PCR test a considerable strain on local partners to
19Liverpool Covid-SMART Community Testing Pilot
finalise procurement processes with external Digital access, dataflows and intelligence
contractors. This involved proceeding at risk,
Digital registration proved to be a key
with parallel negotiations with DHSC on the
determinant for attendance and ‘flow rate’
costing and agreement of a devolved budget;
through the ATS. The initial plan for pre-
taking over equipment leases and liaison with
registration online was abandoned after it
the military command to produce guidance
proved impractical to manage alongside the
for the incoming staff. The Sustainability Plan
walk-in option. Individuals presenting at ATS
was submitted and private sector providers in
were asked to self-register on their personal
place by 30 November 2020 for a start date of
devices. However, some ATS reported up to 40%
3 December 2020. Supply chain assurance (for
of attendees did not have suitable devices or the
LFTs and waste management) was a key issue
ability to operate them, and military personnel
for the transition period.
were required to complete the registration
Mobilisation of a pilot for visitor testing in process on ATS/NHS devices.
twelve Liverpool care homes (using multiple
Dataflows from national and local systems into
LFTs and a PCR test) was complicated by the
a combined intelligence facility, CIPHA
announcement of a national pilot. There was a
(www.cipha.nhs.uk), were important as a single
delay in the supply of kits, and public confusion
source of truth for agile command-and-control.
over which care homes were included –
The necessary Pillar 2 test result dataflows
nationally vs locally selected.
were granted to Cheshire and Merseyside on 5
Liverpool City Council managed a ‘Lessons November 2020. Analysts from NHS Liverpool
Learned’ process, in collaboration with Commissioning Group, Merseycare and The
military personnel in the format of 7-, 14- and University of Liverpool joined an extended
21-day reviews. A summary was published CIPHA team to inform and evaluate the pilot by
on Resilience Direct on 7 December and working on anonymised data extracts from the
disseminated via a workshop for Local Resilience information system provider Graphnet.
Forum partners.
CIPHA was also used under NHS Information
In May 2021, Gold/Silver/Bronze command Governance to guide testing workflows,
remains operational, coordinating testing including intercepting positive LFT results to
across the City of Liverpool, complemented by offer a local confirmatory PCR service when it
an equivalent Liverpool City Region command became apparent that take up of the national
structure. This structure has supported further system was low. A digital workflow from NHS
national Covid-19 response pilots including the Test and Trace via CIPHA to NHS Liverpool
Events Research Programme. was put in place on 23 November, offering a
local testing site dedicated to confirmatory
PCR testing, and rapid sample processing at
Liverpool Clinical Laboratories, which quickly
improved confirmatory PCR uptake from 19%
to 79% (from 6 November to 22 November
140/736 individuals receiving positive LFT results
received a PCR test within 5 days, from 23
November to 12 December these numbers were
184/234).
CIPHA dashboards, including maps and
socio-demographic summaries, showed wide
variation in uptake across the City, not all in
20Liverpool Covid-SMART Community Testing Pilot
Figure 8: Change in uptake, following local intervention, of PCR testing within 5 days of a positive LFT
Initial poor uptake of confirmatory PCR after LFT +ve Positive LFT
700
using national messages and home test kits. Positive LFT with PCR test within 5 days
Improved after local confirmatory PCR system
600
introduced, with swabbing at a local test site,
outreach swabbing and localised invitation
message…
500
Daily Test Counts
“This is NHS Liverpool. Following your positive
COVID-19 test you now need you to confirm
400
your result with a second, different type of
test. If your second test is negative, you will
no longer have to isolate unless you have
300
symptoms. Please book a test at
liverpoolccg.nhs.uk/confirmatory-pcr-test or
call 0845 111 0692.”
200
100
0
11 Jan
31 Jan
18 Feb
13 Jan
15 Jan
26 Feb
7 Jan
9 Jan
4 Feb
22 Feb
4 Dec
6 Feb
10 Feb
14 Feb
17 Jan
19 Jan
22 Nov
6 Dec
10 Dec
14 Dec
21 Jan
2 Feb
28 Feb
23 Jan
25 Jan
12 Feb
16 Feb
2 Dec
30 Dec
6 Nov
10 Nov
14 Nov
16 Dec
28 Dec
8 Feb
30 Nov
12 Dec
1 Jan
3 Jan
5 Jan
12 Nov
16 Nov
28 Nov
8 Dec
27 Jan
29 Jan
20 Feb
24 Feb
8 Nov
18 Dec
20 Dec
24 Dec
18 Nov
20 Nov
24 Nov
26 Dec
22 Dec
26 Nov
the expected patterns of NHS and social care Communications and community
utilisation inequities. Geospatial analysis was engagement
refined to include 15-minute walking times to
Consultation with residents (via surveys and
ATS and consideration of Covid-19 prevalence,
focus groups) identified that the “MAST” (Mass,
deprivation, and digital exclusion. This
Asymptomatic, Serial Testing) term was not well
highlighted areas that were not well-served, and
understood. ‘Asymptomatic’ and ‘serial’ proved
enabled the roll-out of temporary sites, and the
especially challenging terms to communicate.
closure of some sites with unviable attendance.
There was insufficient attention to briefing
CIPHA dashboards for the first phase of those attending for testing that they should
testing were expanded and improved for the return within five to seven days for another test.
subsequent SMART roll-out across the wider
Misinformation may have affected public
Liverpool City Region in December 2020.
confidence and uptake in the first phase of the
Related dashboards for vaccination, NHS
pilot. Misinformed issues included perception
capacity management and were built and
of the risk of infection at test sites, suspicion
CIPHA has become a core population health
around Government use of data collected
management tool for NHS, local authority and
(especially ‘DNA’), and the need to have physical
academic organisations in across the region.
contact with centre staff. The communications
CIPHA is now expanding to other regions
team responded through a page on the
including the whole of the NW and parts of the
Council website, daily stakeholder emails;
SE England.
Facebook messages targeted by postcodes
and regular press briefings and contact with
ward councillors and community leaders. Public
figures from the football and entertainment
communities provided short influencer videos
which were disseminated via social media
channels.
21Liverpool Covid-SMART Community Testing Pilot
Distribution of leaflets via pharmacy In the early months, community engagement
prescriptions bags was first discussed on 19 proved challenging without an existing city-
November. Targeted initiatives such as this wide Voluntary Plan. Although the Liverpool
would have been beneficial earlier in the pilot. Charity and Voluntary Services (LCVS) had
some capacity to act as a liaison service, and
Following the planned review on 19 November
knowledge of charities and neighbourhood
2020 the programme was re-branded as
groups, it proved impractical to mobilise these
‘SMART’ (Systematic Meaningful Asymptomatic
at such short notice to provide a community
Repeat Testing) – and colloquially ‘smart’. This
activation service. Liverpool City Council began
acknowledged the emerging scientific evidence
a leafleting drop to targeted neighbourhoods
on the sensitivity of LFTs and responded to
on 20 November 2020, after the main publicity
analysis that specific population sectors that
drive, missing the opportunity for a critical mass
were less likely to engage with testing. It
of ‘push-pull’ communications.
facilitated the development of three target-
based plans for the use of LFTs: Discussions around deploying third party
vehicles as testing centres (Red Cross; St John’s
1. Test-to-protect
Ambulance; Arriva buses) were hindered by
Testing to protecting the vulnerable and wider health and safety/protocol/sign-off concerns
society against direct harms from SARS-CoV-2 and did not proceed. These would have been
and indirect harms from Covid-19 control a very effective route into the hardest-to-
measures) reach communities that have poor digital
2. Test-to-release engagement.
Testing to release contacts of cases from having Focus groups and surveys suggested the
to quarantine, especially key-workers with major community reception of the military personal
societal consequence of absence from work – was very positive and welcoming (see
now termed “DCT: Daily Contact Testing” Behaviours chapter).
3. Test-to-enable
Testing to allow abeyance of restrictions
affecting health, social fabric, and economy, for
example enabling attendance at
music, theatre, business
and sports events
Visualisation of the mobile testing unit
22Liverpool Covid-SMART Community Testing Pilot
System developments from 3 December 2020 advisers, on the appropriate regime of daily
testing following contact with a positive case,
The City Council assumed direct management
to reduce the period of self-isolation. Staff were
of the ATS from the military on 3 December
trained in how to conduct LFTs at home and
2020 and was rebranded Covid-SMART
how to submit their results. By 3 March 2021
(Systematic, Meaningful, Asymptomatic/Agile,
there were 709 participants in the Keyworker
Repeated Testing). Testing became more
SMART Release scheme (655 were from
targeted in response to move of Liverpool into
Merseyside Police); 3,263 days of isolation had
a lower tier of restrictions when the public
been saved.
messaging moved from “let’s all get tested” to
“test before you go” (going to the hairdresser, A programme of targeted community
restaurant, shops etc.). The planned opening engagement was commissioned from LCVS
and closure of ATS was informed by a review in December 2020 (although the contract
of usage data at Bronze Command. By 31 between LCVS and LCC was not in place until
March 2021, the number of fixed sites had January 2021). LCVS identified several Local
been reduced to six. After the imposition of Trusted Organisations in areas of the city with
national lockdown on 5 January 2021 the public lower testing uptake and worked through their
messaging on use of the ATS changed to members to deliver information on testing and
prioritise use by workers who could not work support for self-isolation. This was achieved
from home, with “testing our front line”. through doorstep conversations, online contact
(Zoom sessions, social media such as WhatsApp
On 10 December 2020, a new rapid response
groups), and the delivery of food hampers
vehicle was brought into action, with an initial
and prescription collection. Local community
site in Sefton Park, an area of relatively low
leaders were involved with identifying hard-to-
engagement with the LFT pilot. This was moved
reach people. Information on testing was also
around the city, informed by data on testing
disseminated through the Positive About Play
uptake and data on areas of increased Covid-19
Christmas and February Half term programmes
positive cases.
and the Health and Wellbeing Network.
As part of SMART-reopening, training for school Feedback from LCVS partners was collated
staff in how to conduct LFTs commenced through a Survey Monkey and focus groups.
on 29 January 2021 at Wavertree ATS. The full
implementation of this pilot was dependent
on the lifting of the national lockdown. This Sector specific arrangements
happened on 8 March 2021, by which time all
As the pilot evolved, asymptomatic testing
schools in England and Wales were required to
schemes emerged across different sectors
implement a LFT protocol.
and settings that Gold and Silver Command
Further SMART-reopening initiatives included had to integrate into a civic whole, which
the provision of training for businesses within involved working with different Government
the LCC area from early February 2021. A pilot of organisations, including Department of Health
late-night ATC opening at Anfield (LFC) did not and Social Care (DHSC), Department for
prove effective and was discontinued. Education (DfE), Department for Culture Media
and Sport (DCMS), Cabinet Office, Department
‘Test-to-Release’ pilots commenced on 4
for Business, Energy and Industrial strategy
December 2020, initially with Merseyside Police
(BEIS) and Ministry of Housing, Communities
Force, and subsequently extended to Mersey
and Local Government.
Fire and Rescue, and HMP Liverpool. A protocol
was developed in collaboration with scientific University testing was devolved to universities
23Liverpool Covid-SMART Community Testing Pilot
whereas schools’ testing was driven directly by caused confusion where guidance for testing is
DfE. Some Universities, including University of different between settings, or where testing is
Liverpool, were asked to build capacity to deliver duplicated when a person has multiple roles.
an alternative testing method, LAMP (loop-
During surges of the pandemic, testing supplies,
mediated isothermal amplification), which did
coordination and communication needed
not take off as it was too labour-intensive. Lateral
local authority and DHSC intervention to bring
flow device supplies to Universities and local
cross-sector activities into a greater whole.
authorities were managed separately at national
For example, at one point the Police faced
level but needed re-integration locally, and the
abstractions from quarantine that put the
University CAMPUS Shield programme across
force’s ability to provide some frontline services
Liverpool was represented in local Command-
at risk if they could not ramp up daily testing.
and-Control.
As national support for ATS venues reduced,
Workplace testing was driven by BEIS and DHSC
so did the accessibility to some high need/risk
in two pilots: regular testing and Daily Contact
communities. In May 2021, the Liverpool ATS are
Testing (as an alternative to quarantine). This
reducing from 6 to 2 or 3. This will impact some
cut across earlier organised elements of the
sectors more than others, for example 41% of
Liverpool pilot on test-to-release contacts of
the domestic care sector staff in Liverpool do
cases from quarantine if they were key workers.
not have a car (LCC social care workforce survey,
Similarly, DHSC introduced a service directly to
2021). Home testing may compensate for this
care homes, cutting across care home specific
lack of access to testing, however, home testing
elements of the Liverpool pilot, which caused
requires a lot of digital interaction and many in
confusion for participants. Large organisations
this sector have low digital resources or literacy.
such as Fire, Police and NHS could cope with
this confusion and put their own systems As society reopens in Summer 2021 the scale of
in place to coordinate locally but smaller testing will grow, with a potential combinatorial
organisations had fewer resources to manage explosion of requirements for sector or setting
this. These agencies, rather than work with the based testing. For example, a care home worker
national programme structures chose to work going to a football match may be asked to
through the local Director of Public Health. NHS test twice within a day. At the population level,
Test and Trace offered LFD supplies to Directors residents will soon return to clusters of large
of Public Health for use in this way, under local and small mixing events, from a music festival
clinical governance – this was the preferred to working the afternoon in a crowded coffee
model in Liverpool. shop. Twice weekly community wide LFT
(with follow-up PCR and viral sequencing for
A DHSC project, Encore, for reopening events,
positives), alongside efficient symptomatic and
was planned with Liverpool then moved to
DCMS. Successful delivery of testing and
protocols for events required local Command-
and-Control.
Scale and sustainability
From November 2020 to May 2021, an increasing
number of sectors and organisation have been
invited into LFT pilots and many families and
individuals have been asked to engage with
these overlapping schemes. The overlaps have “Blossoms At Sefton Park” - part of the 2021 Events Research
Programme
24Liverpool Covid-SMART Community Testing Pilot
surge testing, may be the only practical solution Performance of the Innova SARS-CoV-2
to combining multiple SARS-CoV-2 testing Antigen Rapid Lateral Flow Test
requirements, for as long as they are needed.
Sources and methods
We conducted a quality assurance (QA) exercise
BIOLOGY to assess the performance and appropriate
implementation of the Innova SARS-CoV-2
Aim
rapid antigen LFT in Liverpool. Asymptomatic
The aim was to quality assure the biological individuals attending ATS between 8 and 29
performance of Innova SARS-CoV-2 antigen November were asked to participate in a QA
rapid lateral flow devices and the asymptomatic process and given the opportunity to opt out.
testing process, including the uptake and utility The sample of around 6,000 attendees received
of repeat LFTs and confirmatory PCR tests. a LFT and a reverse-transcriptase quantitative
polymerase chain reaction test, a ‘PCR’ test.
Two supervised, self-administered swabs were
Key findings
taken at the same appointment within minutes.
1) The Innova lateral flow device (LFD) The first swab was analysed by LFT, the second
performed as expected, identifying by the standard PCR test used in lighthouse
most SARS-Cov-2 cases without classical laboratories. The PCR results were sent from
symptoms but with high viral load – those NHS Test and Trace to CIPHA and analysed
likely to be the most infectious. by an independent team at the University of
Liverpool.
2) To maximise the value of lateral flow tests
(LTFs) care should be taken to: The primary analysis compared classifications
of SARS-CoV-2 infection status made by Innova
a) Train test operatives;
LFT with PCR from supervised, self-swab sample
b) Clearly and accurately communicate collection at general population scale. The
how to interpret test results; secondary analysis investigates the influence of
c) Target testing with reference to viral load on the paired LFT-PCR classifications,
background case rates; using PCR cycle threshold (Ct) as a proxy for
sample viral load.
d) Avoid single lateral flow tests for access to
vulnerable settings. Accuracy parameters (sensitivity, specificity,
and predictive values) were estimated, and 95%
3) Local messaging interventions appeared confidence intervals were generated using the
to be important for uptake of PCR tests to Clopper-Pearson method. Analyses were carried
confirm positive results from lateral flow out in R (version 3.6.1 or later) and checked by a
tests. second statistician using SAS software (version
4) From late December 2020 the UK Variant 9.4). Initial results from this QA evaluation have
VOC 202012/01 dominated SARS-CoV-2 been reported in our interim report,1,6 and in
transmissions detected in this pilot. national media.7-14 Our full analysis has been
submitted to a scientific journal for publication.15
25You can also read