Liverpool City Region Health Informatics Research Strategy 2017-2022 - www.liverpoolhealthpartners.org.uk
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Liverpool City Region Health Informatics Research Strategy 2017-2022 www.liverpoolhealthpartners.org.uk
LCR Health Informatics Research Strategy 3 Contents Executive summary 4 1. Mission, vision and objectives 6 2. Introduction 7 3. Learning healthcare systems 12 4. Regional data storage and access facility 14 5. Patient and public involvement and engagement 16 6. Permissions and consent governance 18 7. Current local and regional initiatives 20 8. Generating wealth 23 9. Phased approach 25 Appendix a 26
4 LCR Health Informatics Research Strategy 5
Executive summary
A joined-up approach to health data There are 5 vital elements to this 2. Working with the public 5. Identify the resources required
is essential to improving healthcare strategy: and bring investment in to the
and to supporting research. With We are committed to LCR digital economy Integration across the LCR and the wider Cheshire and Merseyside regions
the appropriate safeguards this 1. Building a vibrant communicating and working with
In order to ensure integration and linkage across the LCR and the wider Cheshire
will improve health outcomes for and effective network the citizens in our region. We will Delivering this strategy will require and Merseyside regional networks (“our region”)*, a Strategy Implementation
patients and communities, improve explore how personal health data significant investment into the Group will be convened with cross representation, including a representative from
We propose to work in partnership may be used for research, the local digital health economy. In the Cheshire and Merseyside Sustainability and Transformation Partnership’s
service delivery and efficiency, and and build upon the excellent talent potential benefits, and safeguards the first instance this will need (STP) Digital Group and a Patient and Public Involvement and Engagement (PPIE)
lead to new scientific discoveries. and leadership within the LCR: that permit personal health to come from the local health representative. The Strategy Implementation Group will report to the LHP Board on
we benefit from a vibrant digital a quarterly basis. The Terms of Reference will be agreed at the first meeting of the
This strategy document outlines data sets to be anonymised in economy but we must position group. Reciprocally, a representative from the Strategy Implementation Group will
the steps that are needed to create economy, and within the healthcare any analysis without identifying ourselves, working with the Local sit on the Clinical Informatics Advisory Group.
a trustworthy approach to enable sector there has been significant individuals. We also need to identify Enterprise Partnership (LEP) and
the use of personal health data, investment from local and national which uses of data are acceptable others, to attract further national Action Timeline
that are already routinely collected, sources. National funding includes to our local population. Public and international investment in
for research purposes. Our aim is four ‘Global Digital Exemplars’ at engagement work has already infrastructure and manpower. 1. Appoint a Chief Officer to oversee
January 2018 to
the following NHS Trusts: Alder the development and delivery of an
to work in partnership to create a started via some of the initiatives December 2018
Hey Children’s NHS Foundation In conclusion, we generate a huge implementation plan.
learning healthcare system for the mentioned above, and we are
Liverpool City Region (LCR), and Trust, The Royal Liverpool and committed to strengthening and amount of personal health data 2. Establish a Strategy Implementation Group
Broadgreen University Hospitals in our healthcare system, but are January 2018 to
the wider Cheshire and Merseyside widening this engagement. to oversee the delivery of the strategy and
December 2020
regions, where research findings NHS Trust, Mersey Care NHS not using it to its fullest extent. The implementation plan.
can be swiftly implemented into Foundation Trust and Wirral 3. Establishing and rolling out a Chief Medical Officer, Professor
3. Undertake a programme of work on public
practice. This has the potential University Teaching Hospitals NHS model of consent Dame Sally Davies recently stated,
engagement to describe the benefits of data January 2018 to
to transform healthcare delivery Foundation Trust. Local initiatives “Personal data must always be
Some uses of data require consent, use for research and identify uses that are December 2018
and population health, as well as include the Merseyside Digital stored securely, but using it acceptable to the people of LCR.
Roadmap and the iLINKS project. which in turn requires processes responsibly can bring huge benefits
bringing investment into our region.
Whilst these initiatives will impact and systems that meet national to patients and improve diagnosis 4. Identify the best model for gaining consent
From December
This is already happening in other on IT systems, local care delivery standards. Gaining consent is and treatment across the world”. to share data for research in keeping with
2018
parts of the UK, and it is important and the flow of information, complex as people need to identify Our strategy is consistent with this, national governance standards.
that we are not left behind. Indeed, research is not an integral part of which data they are happy to share and outlines our vision to effectively 5. Develop a programme of work in phases,
the potential of using personal their remit. and with whom. A system that utilise locally-generated personal initially identifying key clinical pathways/ First wave of
records consent needs to take into pathways from
health data to improve health data, with the public’s consent, to services for data analyses, but building it
This document describes the account that the public interacts up to encompass the whole healthcare June 2018
and the need for investment in improve the health and prosperity
infrastructure has been highlighted strategy for building a research with the NHS at various sites, and of our city and wider regions. economy, utilising the significant expertise and Second wave from
by the Medical Research Council, infrastructure integrated into that the public must have the ability experience already present in Liverpool and June 2019
these initiatives. We will expand to change their consent. the region.
The Wellcome Trust, and the Chief
Medical Officer. to include other stakeholders, 6. Identify the requirements and best provider
working in partnership with NHS 4. Creating a secure facility for
of a data ark/repository and commission its From June 2018
Trusts, the University of Liverpool, data analysis
development.
Professor Andrew Morris
Liverpool John Moores University We require a data facility that can Director of Health Data Research UK 7. Identify datasets for inclusion in the data ark,
and other local digital partners. anonymise and store data from building on existing programs of work including
This builds on our experience with a range of NHS and non-NHS the Global Digital Exemplar NHS Trusts, From June 2018
the Department of Health funded organisations (e.g. universities) iLINKS, Informatics Merseyside, and NW Coast
North West Coast (NWC) Connected Connected Health Cities.
that meets national regulatory
Health Cities (CHC) programme governance standards. This will 8. Identify workforce research health informatics
and we will also work with experts need the facility to link datasets training needs locally and develop and
across the UK, to ensure we are Professor Sir Munir Pirmohamed From June 2018
in a secure way, and allow trusted strengthen education programs for that
working to the highest possible Executive Director, LHP
researchers access to the data in an workforce.
standards. environment where they have the
tools to analyse it. *
For the purpose of this document, “our region” denotes the LCR, working in partnership with
the wider Cheshire and Merseyside STP footprint.
Professor Tony Marson
Professor of Neurology,
The Walton Centre NHS
Foundation Trust6 LCR Health Informatics Research Strategy 7
1 Mission, vision and objectives 2 Introduction
2.1. Why do we need a health informatics research strategy?
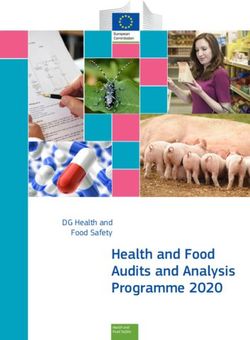
Our mission Our objectives This is a crucial time for the LCR We are one of only 3 City Regions Additionally, there are wider
Example – Northern and the Cheshire and Merseyside in England to have all of these networks across our region that
Our mission is to make our region • Work with the public to identify STP (see Figure 1), as resources developments, meaning that we have already carried out a significant
a world leader in health informatics appropriate uses of health data England amongst for health and social care are have greater freedom to make major amount of work in data sharing (e.g.
research. for research and gain consent. worst for multiple health squeezed, whilst demand for access decisions that affect all of our lives, Health Information Exchanges and
• Create an infrastructure that and social needs to services increases. At the same including those about health and the Cheshire Care Record). Ensuring
Our vision
links information systems, stores time power is being devolved investment in technologies. Health that the wide range of systems that
Our vision for health informatics data securely, and enables a Examining the relationship from central Government with the is a key concern for people in our influence health outcomes in our
research is to put the people of learning health system across between multiple different establishment of the Combined region, and in order for it to thrive, region can deliver the best possible
our region at the forefront to our region, linking in with wider metrics of health and Authority, coterminous with the improving the health of individuals, health for everyone depends
revolutionise healthcare delivery networks (e.g. the STP and other wellbeing using clustering LEP boundary, creating a functional children, families and communities fundamentally on research (see
and transform our ability to make Universities across Cheshire and methods, researchers from economic geography that includes a is essential. We have a proud and Figure 2). This research depends on
new scientific discoveries. Merseyside). Liverpool John Moores critical mass of research bodies and long tradition of working together access to and timely use of high-
• Bring together and add value University identified 5 distinct innovation assets. with our universities, the local NHS, quality data.
to on-going initiatives and clusters of public health need. city and local councils and voluntary
Despite accounting for only The formalised devolution sectors to improve health.
clinical systems within our
13% of all local authorities agreement with the Government
region by developing a research
mapped, Northern England includes the creation of a £458
infrastructure.
accounted for over 60% of million Single Investment Fund, a
• Undertake analyses of data that Single Growth Strategy and now an
local authorities in the worst
will improve health, the delivery elected Metro Mayor.
cluster. Examination of health
of services, and make new
outcomes data on a smaller
discoveries in both clinical and
geographical area would allow
non-clinical research.
us to pinpoint the areas of
• Create jobs and attract most need in the North West
investment into our region. for the appropriate targeting
• To work with organisations to of interventions and services.
build training programmes and
expand the health informatics
knowledge of those working in Figure 1: LCR Health Informatics Strategy Region
our region.
Cheshire and
Liverpool City Region Merseyside STP
Liverpool
Southport
Sefton
St Helens
Wirral
Cheshire
Halton
Knowsley Merseyside
St Helens
Liverpool
Birkenhead
Warrington
Runcorn
Macclesfield
Chester
Crewe8 LCR Health Informatics Research Strategy 9
2.2. The poor health in our region and the stark health inequalities
Whilst there are a number of on- The LCR serves a population of Liverpool Clinical Commissioning This is a critical time for health in
going local digital and informatics Figure 2: The stages of research nearly 1.5 million and includes Group (LCCG) highlight that 30% our region: health services, the city
initiatives, the main focus of most some of the highest levels of of people in the city live with one council and local voluntary agencies
This is a schematic of the full research and adoption pathway, covering the whole
initiatives is on creating clinical deprivation and poverty across the or more long-term conditions, are under considerable pressure
spectrum from research design (which includes discovery and early phase research),
systems. Crucially there is no research delivery (including recruiting patients into trials), adoption of research into country with some of its mortality with Liverpool having one of the for resources. The Five Year
overarching strategy for research, practice (including implementation) and diffusion of best practice into the NHS. rates 76% higher than the European highest cancer mortality rates in Forward View is part of the health
including non-clinical research, average. England. In addition, LCCG state service response to this agenda.
which is a threat to our future health Specialty Services there are 93,000 people affected Key themes in the plan include
and prosperity. People’s health
and Opportunities
A baby girl in Liverpool can expect by mental health problems, and by supporting people to live better
Research Design
is influenced by political, social, Service North West to live 15 fewer years in good 2021 there will be a 10.7% increase quality lives by working together
economic, environmental and HEIs and NHS health than a baby girl in Richmond, in the number of people living with partners in local government
cultural factors. (Figure 3). at
ion Re
se Research Informatics
London. Similarly, adult health with dementia (Healthy Liverpool and the voluntary sector to develop
in a
in the LCR is significantly worse Blueprint, 2015). more joined up models of care;
m
Innovation Hubs
rc
se
h
CHC Digital
The greatest influences on our than the England average for
Dis
De
standardising quality of care and
sign
health and wellbeing are factors Improving
early deaths due to cancer and reducing unwarranted variation,
such as poverty, education and Patient cardiovascular disease deaths; and using the latest technology to
Outcomes
employment, housing and the extent alcohol-related hospital stays; support people in their own homes.
to which our community facilitates rates of hip fractures; sexually
Res
ion
Research Facilities
ea
pt
healthy habits and social connection. transmitted infections and people
rc
do
h
Innovation Hubs A De
HEIs and NHS
killed and seriously injured on
liv
ery
These determinants of health are, NIHR Clinical Research
Network North roads. Figure 4 illustrates how life
to some extent, under the influence West Coast
expectancy changes dramatically
of local organisations, but in the Collaboration for Leadership in
Research Informatics between areas in our region.
current climate many are struggling Applied Health Research and Care
North West Coast
with budget cuts and increased
responsibilities.
More than ever, organisations
need to know what works best to Figure 4: Inequalities in life expectancy in Liverpool
inform targeting of increasingly This figure illustrates how life expectancy varies by region across the
scarce resources. In order to Figure 3: The factors that influence health in Liverpool Liverpool City Region.
understand and improve the This figure illustrates the social determinants of health starting with the individual
health of people in our region, it is and their lifestyle and including social and community networks and general 20 minutes on Merseyrail
necessary to make better use of the socioeconomic, cultural and environmental conditions.
data we collect to understand factors Life expectancy
Southport 78
that influence health over the course Birkdale 83
of people’s lives. ic, cult
ural and enviro
nem Hillside 83
conom ent Ainsdale 85
-e al
io co
oc
Freshfield 83
l s Living and Working nd
ra iti Formby 83
e Conditions on
en
Hightown 80
Hall Road 83
Work
s
G
Unemployment Blundellsands and Crosby 83
environment munity n
d co m Waterloo 76
etw
l an or Seaforth and Litherland 73
ocia ks Water and Bootle New Strand
Education S ua l lifestyle
73
id fac sanitation Bootle Oriel Road
div
73
to
In rs Bank Hall 74
Health care Sandhills 74
Agriculture services Moorfields 76
and food Wirral Line to James
Street and Birkenhead 76
production Brunswick
76
St Michaels
Housing 78
Aigburth 80
Age, sex and Cressington
80
constitutional Liverpool South Parkway 80
factors Hunts Cross 80
...10 fewer years of life
Southport10 LCR Health Informatics Research Strategy 11
2.3. Harnessing data to respond to these challenges to improve health 2.4 This strategy
There is international recognition Using routinely collected data in The SAIL databank has been the This strategy aims to put the people We desperately need to respond to
of the potential for better use of this way will require the creation basis for over 160 research papers, of our region at the forefront of the criticism and external view, that Action:
data for research to improve the of a skilled workforce, including spanning a wide range of topics, the advanced analytics and health the health economy in our region
delivery of services at local levels, information technology experts, including: informatics research agenda, is too fragmented; a view that has Appoint a Chief Officer to
improve population health, and researchers, clinicians and improving health and bringing in previously deterred investment. oversee the development and
• Evaluation of a housing
make new discoveries that can managers, bringing investment and investment. delivery of an implementation
programme offering early help to
drive development and investment. boosting employment. Working with the public is also key plan.
reduce demand on other services
Harnessing the rich data routinely Huge amounts of data are to this strategy. We need to ensure
such as health and social services. Establish a board to oversee
collected within our region offers The Welsh Secure Anonymised generated and the volume and the public are reassured about the
Information Linkage (SAIL) • Establishing a national multiple variety of data generated increases security of their personal health the delivery of the strategy and
the opportunity to improve the lives
Databank is a population level sclerosis registry hosted and every year. Each visit to a GP, a data and the potential uses of it implementation plan.
of people now, and to establish an
data linkage system for Wales, linked to the SAIL databank. hospital, or services provided by to facilitate research. However, at
essential data resource for future
research. For example, research established by Swansea University • Clinical trials using routinely local councils (e.g. by schools or the same time, we must not let this
using routinely collected data can with funding from the Welsh collected outcome data. social care services) generates data. impede their decision to consent
Government. It now holds over However, although a great deal of to the sharing of their data among Example – Co-location
help identify: • The establishment of the Welsh
15 billion anonymised records of Electronic Cohort of Children, work has already gone into data healthcare professionals providing of GP at A&E reduces
• Whether services are working
4-5 million people. There is much which tracks over a million sharing frameworks across our direct care. waiting times and
effectively and inform service
learning that we can take from children born in Wales across region, we do not currently have hospital admissions
improvements. We need to ensure that privacy
SAIL, including the collaborations health, education and social care. the infrastructure or systems in
• Whether new technologies are required, the development of a place to readily access and analyse concerns are addressed, When Alder Hey Children’s
being implemented and having robust governance framework. these data for research purposes. particularly given the lessons NHS Foundation Trust decided
an impact. This is to the detriment of our local from Care.data, and also learn to introduce a GP on site,
• Variation in mortality and SAIL began as a pilot in 2007, population and is impeding our from the successes of health next to their emergency
associated causes. linking an extract of hospital and ability to deliver efficient services, information exchanges nationally department, there was an
GP records, and social services data monitor them, make discoveries, (e.g. Southampton and Leeds). opportunity for researchers
• Previously unknown side
from a local authority area. SAIL and attract investment into our We want to enable access to to see whether this initiative
effects (or beneficial effects) of
now holds anonymised data from digital economy. data for research that is in the had an impact on waiting
treatments.
80% of Welsh GP practices and interest of people in our region, times, hospital admissions and
• Causes of diseases. large number of national datasets To deliver this strategy we will at the same time as maintaining antibiotic prescriptions. Of
• Genetic causes and determinants including: in-patient and out- need to overcome some significant confidentiality and the highest over 5,000 children deemed
of diseases or response to patient records, emergency care, challenges. There are clearly a standards for using data safely. appropriate to be seen by the
treatments. ONS births and deaths, screening number of technical, ethical and GP, and after taking account of
services, Welsh Cancer Intelligence governance issues to address. other factors that may explain
Surveillance Unit, Congenital However, the greatest initial some of the differences,
Anomaly Register and Information challenge may be to encourage children seen by the GP had
Service for Wales, All Wales more local organisations to work shorter waiting times, were
Perinatal Survey, Welsh Health together. Generally speaking there less than half as likely to be
Survey, Welsh Index of Multiple are major technical or governance admitted to hospital, but were
Deprivation, Welsh Fire and Rescue problems preventing organisations prescribed more antibiotics.
Service Data and National Pupil from sharing data with one This research would not
Database Wales. another; and there are barriers have been possible if GP
such as a lack of standardisation and hospital data were not
among data sets, and a lack of available in a linked form.
digital maturity across providers.12 LCR Health Informatics Research Strategy 13
3 Learning healthcare systems
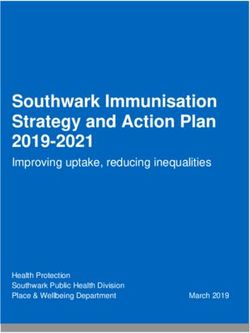
A primary goal of this strategy is Figure 5 illustrates the cycle of From the perspective of this To be useful, those analyses must The most useful analyses will likely
to develop a learning healthcare a learning healthcare system, strategy, steps four and five – be timely. That requires mimimal come from those that link various Action:
system that uses information starting with identifying a evaluation and adjustment - are time-lag between data being datasets held by different parts
effectively, rapidly and intelligently problem, designing and then crucial. Evaluation will require collected and being made available of the health service and other Identify datasets for inclusion
to inform prioritisation, underpin implementing an intervention, analysis of a range of routinely for analyses. Otherwise mutiple parties, enabling a broader view in the data ark, building on
improvements in the quality and evaluating that intervention, collected datasets, the range of cycles of evaluation and adjustment and better targeting of services existing programs of work
efficiency of services, and enable making necessary adjustments and which is illustrated in Figure 6. In will take many years, to the for the population, and more including the Global Digital
innovation and scientific discovery. wider dissemination. Through this the first instance analyses may detriment of patients and services. rapid development of innovative Exemplar NHS Trusts, iLINKS,
Whilst at a first glance this might process we will work with multiple focus on Hospital Episode Statistics At present, for example, there is a 3 solutions to the growing health Informatics Merseyside, and
seem an easy and obvious thing to stakeholders (e.g. the public, (HES) or primary care data such month lag between HES data being problems within our region. NWC Connected Health Cities.
do, it will require significant effort primary and secondary healthcare, as those held by Egton Medical collected and being made available Linking datasets and delivering
to bring our organisations and the public health, universities). Recent Information Systems (EMIS). To by NHS Digital. We will deliver a these analyses poses significant
public together. It will also require local examples include improving enable those analyses we require local solution that enables real-time challenges including the roll out of Example – ensuring
major investment in analytic and access to seizure clinics after investment in infratructure, and analytics. Similarly any analyses will a consent model as well as major
appropriate pathways for
research capacity, ulitmately presenting to the Emergency staff creating a data storage need to be swift and presented in a technical challenges. Analyses of
generating wealth and bringing Department, or improving vaccine facility, which will include a ‘trusted way that is useful and accessible to linked datasets will be addressed in people presenting with
investment in to our region. uptake rates. researcher environment’, as well clinical and managing teams. the latter phases of this strategy. seizure
as public consultation and the
Importantly we must ‘close the development of data governance Scientific discovery will come from It is important to highlight that Following a national audit
loop’ and ensure that analyses of processes. further analyses of datasets held, health data takes many forms and which highlighted variation
data really do impact on health which can harness the power of is often stored in such a way as to in treatment for people
care. That is, we need to put major assets in our region such make it very difficult for researchers presenting with seizure,
research into practice effectively as the Hartree Centre and IBM’s to access and analyse. To enable researchers from the NWC
and efficiently for the benefit of our Watson. The possiblities might timely and efficient analyses of have implemented a pathway
population. include discovery of risk factors data, it is fundamental to our to streamline referrals from
for disease, identification of strategy to create a data storage the emergency department
unanticipated harms or benefits of facility with robust governance or medical assessment
treatments (e.g. drug repurposing). process that meet national unit to neurology / seizure
standards, as described in the clinics. Data are fed back
following sections. to trusts via reports and
Figure 5: A Learning Heathcare System
an interactive dashboard
This figure illustrates the cycle of a learning healthcare system, starting with identifying a problem, designing and allow benchmarking of local
then implementing an intervention, evaluating that intervention, making necessary adjustments and wider dissemination. services, creating a learning
Figure 6: The Wheel of Data health system. Improvements
Internal External in the number of admissions
This figure illustrates the range of datasets that are already routinely collected,
starting with GP and hospital records, and including other health and social care referred to outpatient clinics
Evaluate
Adjust
records, and a range of non health datasets. has already increased by over
Collect data and
analyse results to show
Use evidence to 50% since its introduction in
influence continual
what works and what 2015.
tion • Crimina
improvement.
uca
doesn’t.
d l ju
t •E st
• Imag
Disseminate ions ing
ipt
ic
en
cr •
e•
Share results to improve
m
In a learning
care for everyone.
s
Em
Ge
port • Environ
re
health care system,
Pathology • P
ne
research influences
ployment • S
GP and
tics • Screenin
practice influences Internal and External Scan
research. Identify problems and potentially
innovative solutions.
hospital
records
•
ans
ry
Design
o
g
st
•R
c
r
Implement Design care and ti
ial
•T
eg en
istry
Apply plan in pilot and evaluation based on • D
ca
data
a
control settings. evidence generated (Figure adapted from Learning Health Care i re
ed •
here and elsewhere. Systems and Justice (Ruth R. Faden, Tom L. Nu
trition • Social m
Beauchamp, Nancy E. Kass). Hastings Center
Report, Volume 41(4), July-August 2011)14 LCR Health Informatics Research Strategy 15
4 Regional data storage and access facility
4.1 Architecture and Infrastructure
A key element of this strategy is the We can learn from, and adopt, This way of working influenced the Table 1 summarises a number
creation of a data storage facility best practice from similar projects Phase 1 design for data access in of relevant and ambitious
Table 1 – Shortlist of digital strategies, initiatives and
that can collate and store data elsewhere in the UK that are more the North West Coast Connected initiatives addressing aspects
recommendations guiding development of the Regional-scale Data
from a range of sources, and allow advanced in their development. For Health Cities (CHC) (a partnership of health informatics research. Storage and Access (TRE) Facility
analyses by ‘trusted researchers’. example, A Charter for Safe Havens between the Innovation Agency When developing our plans for a
Whilst there are a range of NHS in Scotland (2015) details a baseline (Academic Health Science Network regionally-scalable data storage Liverpool iLINKS Strategy (2014-2017) http://www.imerseyside.
informatics initiatives in our region set of principles for ethical uses of for the North West Coast), and access facility, it is imperative nhs.uk/Library/innovations_and_developments/ilinks_informatics_
that underpin or link clinical data that are in the public interest, Universities of Liverpool and that we are clear in what we want transformation_strategy_2014_2017.pdf
services and data, none allow for which are scientifically sound, and Lancaster, and AIMES Grid Services) to achieve. In the CHC design, it has Merseyside Digital Roadmap http://www.ilinksmersey.nhs.uk/
the storage and use of data for have patient identity and privacy project which currently holds been recognised that the power media/1554/the_merseyside_digital_roadmap.pdf
research; the primary objective of appropriately protected. anonymised (no patient identifiable of health informatics for radically Intra-Region Digital Exemplar strategies e.g. for the Global Digital
this strategy. data) hospital episode statistics improving research performance Exemplar Trusts: The Royal Liverpool and Broadgreen University
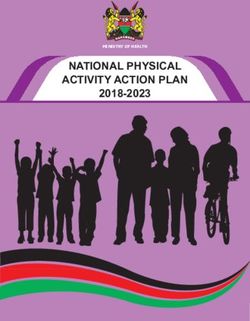
We plan to create what is currently data and is visualised in Figure 7 falls into a series of practice Hospitals NHS Trust, Alder Hey Children’s NHS Foundation Trust, Wirral
The creation of a data storage being called a ‘Trustworthy below. domains or use cases (green University Teaching Hospital NHS Trust, Mersey Care NHS Foundation
and access facility requires Research Environment’ (TRE) that boxes, below). This demarcation Trust and the Fast Followers programme.
significant technical know-how and allows authenticated researchers is useful because each
a complex governance structure access to data in order to undertake A Charter for Safe Havens in Scotland (2015) http://www.gov.scot/
application area could share Publications/2015/11/4783/4
that meets the requirements of analyses. One model that is being technology/infrastructure with
legislation as well as those of our used is in Genomics England’s subtle differentiating factors in The Digital Economy Act (2017) is now in force and provides a UK
local population. It also requires 100,000 Genomes project. The TRE deployment. This efficiency will regulatory framework for the use of data for research in an effective,
investment in infrastructure and is configured such that only outputs be key to delivery and the risk of safe and secure manner; see Chapter 5: Sharing for Research Purposes -
the workforce. of analyses (but not the source http://www.legislation.gov.uk/ukpga/2017/30/contents/enacted
fragmentation of solutions must be
data) can be taken away (exported). strongly avoided. Liverpool PRIME: Precision in Medicine proposals
(details available from LHP)
Learning Health/Service Improvement The Wachter Report https://www.england.nhs.uk/digitaltechnology/info-
Public Health revolution/wachter-review/
Clinical Research/Discovery Science UCL Partners Health Informatics Strategy (2014-2017) http://
uclpstorneuprod.blob.core.windows.net/cmsassets/UCLP%20
Citizen-Driven Health Informatics%20Strategy
Figure 7: A data storage facility and trusted researcher environment
Personalised/Precision Medicine NHS England Target Architecture for Learning Health Systems
This figure illustrates a data storage facility in which health data are securely stored behind a firewall according to national standards,
whereby trusted researchers can log in and have access to data for analyses but not take those data away from the secure The National Data Guardian https://www.gov.uk/government/
environment. organisations/national-data-guardian
Action:
NHS system supplier expertise and technologies e.g. EMIS Web, Cerner,
Scale Identify the requirements and Tiani Spirit, InterSystems, Endeavour Health, Patients Like Me, Patients
South Cumbria best provider of a data ark/ Know Best etc.
Lancashire
Merseyside repository and commission its
Cheshire
development. Expertise in national and international informatics initiatives e.g.
NHS Digital, Regional CSUs, The Farr Institute for Health Informatics
Secure research Research, Health Data Research UK (HDR UK), GA4GH, BRCs, HL7 UK etc.
lts
r e su s) data host
, ad
ion lo
l i sat own
ua a d
Vis dat Compute-intensive
(no services
Virtual machine
(VM) bespoke apps ,
ax
y nt s
s nd
a,
d at ma
e co m
Firewall nc
Known
f e re hes,
VPN/ portal
machine Re earc
locations login s
Authenticated
researcher(s)16 LCR Health Informatics Research Strategy 17
5 Patient and public involvement and engagement
5.1. Benefits 5.2. PPIE for this Strategy to date
Patient and public involvement and We will achieve our PPIE Our PPIE will help to inform the Obtaining consent from patients to The video of responses can
engagement (PPIE) is key to this objectives by a multifaceted development of the programme of use their personal health data for be viewed here: http://www.
Example – “Introducing
strategy. It is vital that we clearly approach, through identifying and work and help gain trust from the clinical research is a fundamental liverpoolhealthpartners.org.uk/
and effectively communicate the developing a relationship with key personalised risk based public in the data sharing model. step in the success of this strategy.
potential benefits to the health citizen engagement and public intervals in screening Data will, for the most part, be We need to understand what We recognise that this initial PPIE
and wealth of our population in involvement groups within our used in an anonymised form, but motivates patients to provide this work provides only a snapshot of
for diabetic retinopathy”
terms of using personal health data region. This engagement will be should data be required to be used consent and, more importantly, to opinion and much more detailed
ISDR trial engagement will be required in the
for research. It is also paramount facilitated by using social media and in a patient identifiable format establish what barriers may present
that we consult and work with creating digital areas for dialogue additional consent will be sought and how they can best be tackled. next steps of this strategy.
One of many complications
our population to identify ways blogs, web areas, social media, seen in people with diabetes and safeguards put in place. In the development of this strategy,
of using data that are acceptable events and twitter chats. is diabetic retinopathy – some PPIE work has already taken
Engagement with our community Action:
and to reassure them of the use of damage to the retina (the back place.
their data for research, whilst not We will also work with other will help assist in the development
of the eye) which can cause Undertake a programme of
impacting on their consent to share organisations and stakeholders, and implementation of a “Model In collaboration with several
blindness if not diagnosed work on public engagement to
data for clinical purposes. such as Cheshire and Merseyside for Consent”. Citizens will be able to organisations from within LHP, a
and treated. Current describe the benefits of data
STP, SMEs, Healthwatch, Health view the extent and degree of their series of ‘vox pop’ interviews from
recommendations in England use for research and identify
To achieve this, we need to develop North and technology partners, consent to data sharing and to have a number of pre-selected locations
suggest screening every 12 uses that are acceptable to the
an effective dialogue with people in industry and universities, to control over it. around Liverpool were conducted.
months but the evidence population of our region.
our region, enlisting trust and active enhance partnership and We were able to gather the
behind this is very limited, with
involvement, about how we would collaborative working. The aim opinions of members of the public
potential for better targeting
like to use their data across a range being to ensure involvement from through asking them the following
of services. The University
of agencies, both within the NHS diverse groups, including those questions: Example – University
of Liverpool and The Royal
and beyond, including partnering that are hard to reach, and to avoid of Liverpool researchers
Liverpool and Broadgreen Q1. Do you think it is important
with industry (as appropriate) to duplication with other initiatives.
University Hospitals NHS to support clinical research in the have developed a data
achieve breakthrough research
Trust are running the ISDR NHS? Why is that? linkage at small area level
objectives. Learning from other
trial, which is integrating
successful organisations, such
diagnostic data from hospitals, Q2. When you visit your doctor or The Integrated Longitudinal
as those in Manchester, Leeds
demographic data from GP nurse you share personal health Research Resource (ILRR)
and Southampton, and working
practices and imaging data data, would you be happy if this allows researchers to extract,
with colleagues within the patient
from eye-clinics to calculate an data was shared with clinical manage, and link data from
engagement teams across the
individual’s risk of developing researchers in the NHS? diverse, datasets for policy
Cheshire and Merseyside STP
retinopathy. Based on this relevant analytics, including
footprint, will be imperative to our Q3. Do you have any concerns
they will be called back for consumer, finance and welfare
success. about the sharing of your personal
screening at either 6, 12 or datasets not routinely used in
24 months. This study has health data? applied public health research.
necessitated the creation of Q4. If your personal health data Through a collaboration
bespoke data sharing systems could be made anonymous when between the NIHR CLAHRC
as mechanisms to link these shared would you still have any North West Coast, the ESRC
different sources of data are concerns? funded Consumer Research
not presently available in our Data Centre and 10 local
health data architecture. Q5. Would you be happy if we authorities across the North
shared personal health data with West we have established
other researchers in life science an Integrated Longitudinal
companies that may be outside the Research Resource (ILRR)
NHS? of linked neighbourhood
datasets, enabling the tracking
of the determinants of health
and health outcomes within
neighbourhoods.18 LCR Health Informatics Research Strategy 19
6 Permissions and consent governance
There is a complex range of Other uses of data do require It is important to realise that Facilitating patients to opt in or We need to work towards creating
legislation and permission required individual patient consent, such as consent is multi-layered (Figure 8). out of sharing their personal an infrastructure that meets Action:
for the use of health data for uses that require linkage of records For example, patients may choose information, for reasons other than all of these requirements and
research, which largely depend from a number of systems. In this to share anonymous data with their individual care and treatment, enables the people in our region Identify the best model for
upon the type of data and the circumstance, the NHS number some parties (e.g. other health is the subject of an English national to contribute their data and to gaining consent to share
intended use. It is essential that we is commonly used as a unique service organisations) but not development by NHS Digital that participate in research. Whilst the data for research in keeping
work with the public, as described identifier to link data. Data linkage others (e.g. industry), may want to is proposed for operation from text in this section has focussed with national governance
above, to navigate these processes can be undertaken by a trusted restrict which data are shared, and late 2017. It follows on from the on information technology, the standards.
when we create our learning health third party who then removes will need the ability to change those National Data Guardian’s (NDG) importance of working with the
system. patient identifiers to provide permissions. In the WCR, if a patient review of data security and consent public and integrating this into the
researchers with anonymised data. opts out of sharing of the record of July 2016. The patient opt out day to day working of our health Example – UK birth
In England, some uses of One example of a linked system there is a Read Code set on the preferences will be stored in a services must be emphasised. This
anonymised data (data are cohort shows impact of
in our region is the Healthy Wirral primary care system (EMIS). This central repository and systems will can only work if seamless processes
considered anonymised if they do Care Record (WCR), which links data code prevents data held in EMIS be made available so that it can are put in place to capture consent transition into poverty
not include information that allow from primary care, Wirral University for that patient being shared, and be securely accessed and applied and permissions at time points
an individual to be identified, such Using a specially conducted
Teaching Hospital NHS Foundation also prevents sharing of data from when personal information is being where patients interact with health
as date of birth or NHS number) study – the Millennium cohort
Trust, community, mental health other sources. In addition, national shared between organisations for services.
do not require individual patient study – which collected
and social care etc. In the WCR, standards exist that exclude the purposes.
consent (e.g. in public health, audit, information on children from
consent for use of data is managed sharing of certain data items,
NHS service improvement and The General Data Protection across the UK born between
with the GP record as a central for those that do not opt out of
some research studies). In the early Regulation (GDPR, https://ico. 2000 and 2002, researchers
point. sharing.
phases of this strategy the focus org.uk/for-organisations/data- from the University of
will be on the use of these data protection-reform/overview-of-the- Liverpool were able to show
given the complexities of setting up gdpr/), which becomes effective in that transitioning into poverty
systems to manage patient consent, May 2018, identifies additional and was associated with an
as described below. more sophisticated requirements increase in childhood social
to capture and manage patient and behavioural problems.
permissions for research. For This study collected data
example, the ability to include or directly from participants
exclude specific episodes of care, (socioemotional behaviour)
Figure 8: Gaining and managing consent in the NHS and also used data from
and the need for interoperability of
Starting in the bottom left hand corner, this figure illustrates how a patient attending an NHS organisation (e.g. their GP) can identify systems. government agencies including
which data they wish to share and with whom, give consent to do so, and have the option to change their preferences at a future the Department of Work and
time point. Pensions (benefits) and the
Department for Education
National Data
Guardian for
(educational achievement).
Health and care ID-linked sharing We plan to create a similar
Review of Data
Security, Consent
Consent/opt-out model “Sharing for purposes anonymised population level
for cross-organisational Other Than individual
and Opt-Outs
data sharing care and treatment”
Data Consumer
Organisation
child health and development
dataset for all children in
Liverpool from existing data
sources to allow researchers
Data
National Data Guardian
Patient selects preference
and policy makers to improve
Caldicott Review July 2016
child health in our region.
No preferences need
to be expressed for
data that is ID-Stored preference Stored Preferences
anonymised or Opt-in/out ID-Stored preference Control Sharing
pseudonymised is linked to
ID-Stored preference
NHS ID
ID-Stored preference
NHS Digital patient
preference-driven Central Repository Data
information sharing for NHS Digital
purposes other than (by 2020 all providers)
individual care and
treatment (May 2017) Data Source
Organisation20 LCR Health Informatics Research Strategy 21
Initiative Lead organisation Brief description Project ambitions / objectives Further information
7 Current local and regional initiatives iLINKS Liverpool CCG A shared vision of Liverpool CCG, 1. Create and deliver an information http://www.
Informatics South Sefton and Southport exchange across health and social care. ilinksmersey.nhs.
Transformation and Formby CCGs, to improve 2. To ensure informatics system-wide uk/
Programme health and social care by coherence and strategic leadership across
providing professionals with the health and social care.
information they need to work
3. To exploit the benefits and investment
and share collectively around the
of existing future technologies and
individual.
LHP serves to ensure close collaborative healthcare research through University of Liverpool and Liverpool John processes.
Moores University working together with local NHS organisations.
Global Digital Exemplars (GDEs)
This complements the ongoing digital initiatives locally and regionally, including our region’s hosting of four of the Alder Hey AHCH NHS England’s only specialist 1. Paperless medical record http://www.
NHS’s Global Digital Exemplar Trusts (GDEs); and we are the only area in the UK that has such a concentration of Children’s NHS children’s GDE. 2. Web portal for patients and families. alderhey.nhs.uk/
GDEs. These initiatives (Table 2) underpin this strategy and place our region in a strong position to succeed. Foundation
3. Web portal for healthcare professionals.
Trust (AHCH)
4. Patient ‘app’ platform.
We are creating a sharing environment that enlists the trust, and active involvement, of NWC citizens.
5. Collaboration with Hartree Centre and
IBM Watson to create the UKs first
Table 2. Local and Regional Digital Initiatives ‘Cognitive’ hospital.
Initiative Lead organisation Brief description Project ambitions / objectives Further information The Royal RLBUHT ‘Digital Liverpool’ is RLBUHT’s 1. Digital Innovation http://www.rlbuht.
Liverpool and digital vision and strategy 2. New Royal nhs.uk/
The Merseyside Liverpool CCG A strategic plan in response 1. Digitally empowered individuals http://www.
Broadgreen underpinned by it’s GDE
Digital Roadmap to the NHS Five Year Forward 2. A connected health and social care ilinksmersey.nhs.uk 3. Digital Transformation
University programme. With health and
View requirement to improve economy Hospitals NHS social care partners across the 4. Electronic Patient Record
health and care services by the
3. Exploiting the digital revolution Trust (RLBUHT) city, RLBUHT, through its GDE,
increased and improved use of
will revolutionise patient and staff
information and technology.
experience, transform quality and
EMIS Health EMIS Health Leading supplier in connected 1. Deployment of EMIS Web in Walk-in https://www. safety of its services and produce
healthcare software and Centres emishealth.com/ better health for the population.
services in the UK. EMIS Health 2. Electronic Patient Record (EPR) Viewer home/
Mersey Care MCT One of seven Mental Health 1. Flip the Clinic http://www.
and the LCR have enjoyed a long
3. Mobile working NHS Foundation GDEs in England. 2. Digitisation is about people, not just merseycare.nhs.uk/
and successful relationship with
Trust (MCT) technology.
Liverpool CCG and Informatics
Merseyside being key strategic
Wirral University WUTH WUTH is leading a programme 1. Organisation level electronic patient http://www.wuth.
partners through the EMIS
Teaching of work in Wirral as part of the records – based on the very mature GP nhs.uk/patients-
Pathfinder Programme.
Hospital NHS GDE programme. As well as records in the EMIS system in primary and-visitors/
FARSITE NWeHealth A powerful search and patient 1. To recruit over 90% of GP practices in http://nweh.co.uk/ Foundation developing the digital platform care WCR will also contain data from the
administration tool that allows Liverpool and surrounding environs to products/farsite Trust (WUTH) in the hospital, the community of other providers as shown above. Thus the
the rapid identification of, use FARSITE. provider organisations in Wirral content of the individual systems is a basic
and easy communication with are working to create a new building block.
2. To develop relationships with Industry to
cohorts of patients drawn shared Wirral Care Record (WCR). 2. Creating a single population long term
mount large scale trials that can test new
from primary care information This will support clinicians/carers record – as data flows from EPRs into
drugs, devices or models of care quickly.
systems for the purposes of on the ‘front-line’ of care delivery the WCR, it goes through a series of
3. Population health management as well as the system as a whole
research and population health algorithms to create a single unified
interventions to be designed and as it works to manage the health
management. view of the data which dedpiulicates and
implemented to achieve meaningful of the population. normalises the data to make more sense
and lasting improvements in the health
of it to the end user and also make it
and wellbeing of patients in our health
easier to analyse.
economy.
3. Registries / Care Plans – the data allows us
NWC Connected Innovation Agency NWC CHC is funded by the 1. Making information available to front-line http://www.
to target specific disease groups and link
Health Cities (Academic Health Department of Health and staff in timely ways that enable them to connected
the data from the various organisations
(CHC) Science Network brings together the Universities better plan and review the care they offer; healthcities.org/
to provide a single view of the patient,
for the North of Liverpool and Lancaster, the and develop new and more effective connected-health-
in a set of wellness and condition based
West Coast) Innovation Agency (Academic pathways. cities/north-west-
registries. These assist clinicians to identify
Health Science Network for the 2. Harness the power of data and data coast/
what has been done for the patient
North West Coast) and AIMES analytics by collecting, linking and already and also those things that have
Grid services. The programme collating data from health and social care not yet been achieved for each patient.
is creating learning healthcare and eventually from a wide range of other
systems. 4. Analytics – by bringing together all of
sources – finding new ways to use data to
the health issues and identifying the
transform care.
resources deployed in each sector to
3. Support industry and academia and deliver care, WCR is a rich source of data
others in using data to conduct research to understand how to manage population
that both improves understanding of health and where best to apply scare
health care efficiency and effectiveness resource.
and enables new techniques, ideas and
5. Future – in future we would expect the
organisational forms to be tested.
patient to be more involved digitally in
4. Create a sharing environment that enlists this process and for example services like
the trust and active involvement of North puffel.com will be linked to the WCR.
West Coast citizens.22 LCR Health Informatics Research Strategy 23
8 Generating wealth
The LCR has a population of 1.5m Initiatives aligned to the Growth The ambition of the Growth
Table 3. Informatics strengths within our local Universities
and a £28.3bn economy. This is a Strategy/SIF will: Strategy is for each sector to
University Summary of informatics strengths crucial and exciting time as power • Build on key assets: including LCR’s become a beacon of excellence,
University of Ranked in the top 1% of higher education institutions worldwide, the University of Liverpool (UoL) is a comprehensive is being devolved to the region role as a unique global port and a productivity and accelerated
Liverpool (UoL) university of global reach with campuses in China and Singapore. from the central Government, world-leading centre for innovation growth through investment in
In collaboration with its partners, UoL has developed an ambitious programme of health and biomedical informatics
with a Devolution Deal agreed and achievement in science, facilities, infrastructure, networks,
research, tackling important global challenges at scale, initiating new business links, influencing policy, and improving with Government in 2015, the LCR culture and civic life. people and innovation, creating
health and social environments. Over 50 academics across UoL carry out interdisciplinary health and biomedical Combined Authority established and more and higher skilled jobs and
• Focus on growth sectors:
informatics research. The UoL Healthcare Data Laboratory, established as part of the Connected Health Cities programme. the election of a first ever LCR Metro more growth businesses. Sector
investment will be maximised by
UoL uses novel informatics approaches to answer important clinical and public health questions. It supports industry, Mayor (Steve Rotherham) in May based interventions will focus
strategically focusing on those
academia and others to conduct research in its theme areas to improve understanding of health care efficiency, the 2017. particularly on those activities that
sectors with the greatest potential.
benefits of treatments and minimizes risk, and also enabling new techniques, ideas and organisational forms to be tested. accelerate growth, apply innovation
Devolution provides an opportunity • Respond to challenges: including commercially and deliver increased
Liverpool John LJMU is a modern civic university with a long history of applied teaching and research responding to the needs of
Moores University external stakeholders including the NHS. LJMU won the 2017 Educate North University of the Year award, and has the for LCR to direct its economic future, long-established challenges productivity.
(LJMU) highest number mainstream journal published articles co-authored by international collaborators of any University in to build on recent success and to regarding levels of health,
the UK. address the challenges, in particular business, jobs, worklessness, Sectors identified in the LCR Growth
LJMU offers degree apprenticeships working alongside employers to enable students to develop practical skills within those relating to inequalities productivity, skills and spatially Strategy include Digital and “Health
the workplace. Health research, scholarship and knowledge exchange within LJMU is embedded within the Institute for mentioned above. concentrated deprivation. and Life Sciences”, which clearly
Health Research (IHR) which has a portfolio of cross disciplinary expertise and facilities including digital health, applied align with the development of the
health informatics and health service delivery needs analysis. The LCR Growth Strategy (published The outcomes that the Growth LCR Health Informatics Research
June 2016) provides a 25-year Strategy will deliver across its Strategy. In addition, the LCR
strategic approach to how growth three pillars by 2040 can be has been recognised through
will be driven forward across the summarised as: the Government’s Science and
City Region via three pillars of • 100,000 additional jobs Innovation Audit (SIA) process as
Figure 9: North West Coast Connected Health Cities Productivity, People and Place, having world leading capabilities
• A net increase of 20,000
and building on LCR’s unique in infectious diseases, materials
This figure shows the partners in this programme and what they plan to deliver. businesses
strengths and assets. The Growth chemistry and high performance/
Strategy, through consultations • An additional 50,000 people living
cognitive computing, with further
with the City Region’s partners and in the City Region
commercial programmes in these
key stakeholders, has identified • An increase in the City Region’s areas under development.
NWC Connected Health Cities a framework for devolution and economy to around £50bn.
the achievement of long-term
Cultivating Innovation
sustainable economic growth. Key
to implementation of the Growth
Strategy is the attraction and
focused allocation of investment.
The Single Investment Fund (SIF) has
People Collaboration
LEd by Lancaster been established to fund delivery
Roles: Roles:
1. Lead on Therapeutic themes University 1. Lead industry research (TRL1-3) of the Growth Strategy. Over the
2. Develop CHC knowledge framework
3. Lead on evaluation approaches
2. Develop workforce digital skills
3. Build digital research capacity next five years the SIF will invest
4. Scale therapeutic themes 4. Link digital programmes, e.g. Testbed £458 million. This resource will help
leverage private sector and external
investment opportunities as they
Problem
Collaboration Led by
Technology become available.
Collaboration Led by
University of
AIMES Grid Services
Liverpool
Roles: Roles:
1. Strategic direction & leadership 1. Lead industry partnerships
2. Lead innovation spread (TRL7-9) 2. Technical Design Authority
3. Commission packages 3. Technical platforms
4. Drive economic growth 4. Solution prototyping (TRL4-6)
Innovation Spread Commercialisation
Intellectual Property Partnerships
* TRL = Technology Readiness Level (DoD)You can also read