JUST AS TALL ON TESTOSTERONE; A NEUTRAL TO POSITIVE EFFECT ON ADULT HEIGHT OF GNRHA AND TESTOSTERONE IN TRANS BOYS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Journal of Clinical Endocrinology & Metabolism, 2023, 108, 414–421
https://doi.org/10.1210/clinem/dgac571
Advance access publication 3 October 2022
Clinical Research Article
Just as Tall on Testosterone; a Neutral to Positive Effect
on Adult Height of GnRHa and Testosterone in Trans Boys
Lieve Anne Willemsen,1,2,3,* Lidewij Sophia Boogers,1,2,4,* Chantal Maria Wiepjes,1,2,4
Daniel Tatting Klink,5 Adrianus Sarinus Paulus van Trotsenburg,3,4 Martin den Heijer,1,2,4
and Sabine Elisabeth Hannema1,3,4
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
1
Center of Expertise on Gender Dysphoria, Amsterdam UMC location Vrije Universiteit Amsterdam, 1081 HV Amsterdam, the Netherlands
2
Department of Endocrinology, Amsterdam UMC location Vrije Universiteit Amsterdam, 1081 HV Amsterdam, the Netherlands
3
Department of Pediatric Endocrinology, Amsterdam UMC location University of Amsterdam, 1105 AZ Amsterdam, the Netherlands
4
Amsterdam Gastroenterology Endocrinology Metabolism, 1105 BK Amsterdam, the Netherlands
5
Division of Pediatric Endocrinology, Department of Pediatrics, Ghent University Hospital, Ghent, Oost-Vlaanderen 9000, Belgium
Correspondence: Sabine Elisabeth Hannema, MD PhD, Department of Pediatrics, Section Endocrinology, Amsterdam University Medical Centers, Amsterdam,
the Netherlands, PO Box 7057, 1007 MB Amsterdam. Email: s.e.hannema@amsterdamumc.nl.
*Both authors contributed equally
Abstract
Context: Growth is an important topic for many transgender boys. However, few studies have investigated the impact of puberty suppression
(PS) and gender-affirming hormone treatment (GAHT) on growth and adult height.
Objective: To evaluate the effect of PS and GAHT on growth and adult height.
Design: Retrospective cohort study.
Setting: Specialized gender identity clinic.
Participants: A total of 146 transgender boys treated with GnRH analogues and testosterone who reached adult height.
Main outcome measures: Growth, bone age (BA), adult height, and difference between adult height and predicted adult height (PAH) and
midparental height.
Results: In those with BA ≤14 years at start (n = 61), a decrease in growth velocity and bone maturation during PS was followed by an increase
during GAHT. Adult height was 172.0 ± 6.9 cm; height SD score was similar to baseline (0.1; 95% CI, −0.2 to 0.4). Adult height was 3.9 ± 6.0 cm
above midparental height and 3.0 ± 3.6 cm above PAH at start of PS. A younger BA at start PS was associated with an adult height significantly
further above PAH.
Conclusion: During PS, growth decelerated followed by an acceleration during GAHT. Although adult height SD score was similar to baseline,
adult height was taller than predicted based on BA at baseline, especially in those who started treatment at a younger BA. It is reassuring that PS
and GAHT do not have a negative impact on adult height in transgender boys and might even lead to a slightly taller adult height, especially in those
who start at a younger age.
Key Words: growth, gender dysphoria, transgender, testosterone, adult height, puberty suppression, GnRHa
Abbreviations: ACOG, Amsterdam Cohort of Gender; BA, bone age; BMI, body mass index; CA, chronological age; CV, coefficient of variation; GAHT,
gender-affirming hormone treatment; GnRHa, GnHR analogue; IQR, interquartile range; LOQ, limit of quantification; PAH, predicted adult height; PS, puberty
suppression; SDS, SD score.
Gender dysphoria involves an incongruence between the ex In transgender boys (female sex assigned at birth, male gen
perienced gender and the sex assigned at birth (1). Medical der identity), GAHT consists of intramuscular or transdermal
treatment for adolescents consists of puberty suppression testosterone. This induces physical changes such as increased
(PS) and subsequent gender-affirming hormone treatment facial and body hair, increased muscle mass, and lowering of
(GAHT). PS with GnRH analogues (GnRHa) inhibits the the voice. Growth and predicted adult height are also topics of
development of undesired secondary sex characteristics interest during consultation. Because Dutch males reach a
and gives adolescents more time to explore their gender mean adult height 13.1 cm taller than Dutch females (2),
identity. If the gender-dysphoric feelings persist during the height is also considered a sex characteristic. When treatment
puberty-suppressive phase, GAHT may be initiated from is initiated before adult height has been reached, transgender
the age of approximately 16 years to induce development boys may ask how treatment will impact their growth and
of secondary sex characteristics congruent with the affirmed whether they will reach an adult height within the male popu
gender (1). lation range. However, although the impact of GnRHa and
Received: 27 July 2022. Editorial Decision: 28 September 2022. Corrected and Typeset: 9 November 2022
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs licence (https://creativecommons.
org/licenses/by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any medium, provided the original work is not altered
or transformed in any way, and that the work is properly cited. For commercial re-use, please contact journals.permissions@oup.comThe Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2 415
GAHT on growth in transgender girls has recently been eval Treatment Protocol
uated (3), the effect on growth in transgender boys is still Adolescents were diagnosed with gender dysphoria by mental
unknown. health professionals according to the criteria of the Diagnostic
The limited data available in transgender boys solely describe and Statistical Manual of Mental Disorders, Fourth and later
the effects of GnRHa on growth. Several studies have observed Fifth Edition (10, 11). All individuals received PS for at least 6
a decrease in height SD score (SDS) (4–6). Furthermore, it re months followed by GAHT from the age of 15 to 16 years. PS
mains unclear whether testosterone can induce catchup growth consisted of GnRHa (triptorelin 3.75 mg every 4 weeks sub
and reverse the changes in height SDS that occur during cutaneously or IM; or 11.25 mg every 10 to 12 weeks intra
GnRHa treatment. muscularly). GAHT consisted of intramuscular testosterone
The timing of treatment initiation might also play a role in injections with a starting dose of 25 mg/m2every 2 weeks.
the effects on growth. It has been suggested that treatment As described in the Endocrine Society Guidelines, the dosage
with PS and GAHT might have a negative impact on adult was gradually increased every 6 months leading up to an adult
height (7). Therefore, some clinicians argue that postponing dose of 125 mg every 2 weeks or 250 mg every 3 to 4 weeks
treatment with GnRHa until growth is (nearly) finished may (1). If transgender boys had (nearly) completed endogenous
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
result in a taller adult height. This poses a dilemma for young puberty before the start of treatment, the testosterone dose
transgender boys between achieving maximal growth and pre was increased more rapidly, starting with 75 mg every 2 weeks
venting the development of unwanted secondary sex charac which was increased to 125 mg every 2 weeks after 6 months.
teristics such as breast development. The latter may give Treatments were individualized by treating clinicians. Before
great distress because of the need to wear binders for several 2014, subjects were treated with GnRHa until gonadectomy,
years and the wish to undergo a mastectomy (8). which nearly all individuals chose to undergo because this was
Another hypothesis is that the effect of testosterone on required before a legal sex change was possible. After a law
growth is dose dependent. Rapid increase of the testosterone change in 2014, it became more common to leave the ovaries
dose may cause rapid acceleration of bone maturation, there in situ. Thereafter, the protocol was adapted and GnRHa was
by shortening the period of growth. This may compromise discontinued when an adult dose of testosterone was reached.
adult height. In contrast, a more gradual increase of testoster
one dosage may induce an increase in growth rate during a
Measurements
longer period, leading to an increased adult height, which is
why a different dose schedule is proposed for adolescents Height and weight were assessed every 3 to 6 months from start
that have and have not finished linear growth (1). However, of PS. Height was measured using a wall-mounted stadiometer,
the effects of different testosterone dose schedules on growth and weight was measured using a digital floor scale. Height SDS
and adult height in transgender adolescents have not been was calculated according to Dutch reference data from
studied. Schönbeck et al. (2) and BMI SDS was calculated according
With this cohort study, we aim to evaluate the effect of to reference data from Cole et al. (12). Midparental height
GnRHa and testosterone treatment on growth in transgender was calculated using the following formula: Midparental
boys. Furthermore, the impact of timing of treatment, tempo height = (paternal height + maternal height)/2 – 6.5 (13). BA
of dose increase, and body mass index (BMI) will be investi was determined at start of PS and at start of GAHT by evaluat
gated. We hypothesize that PS will result in a decrease of ing X-rays of the left hand using female reference data from the
growth velocity and GAHT will result in subsequent catchup Greulich and Pyle atlas (14). Predicted adult height (PAH) was
growth that may be greater when the testosterone dose is determined using the female prediction tables according to
slowly increased. Additionally, we expect these effects to be Bayley and Pinneau (15). Parental height and BA were not rou
larger in subjects with a younger bone age (BA) at the start tinely obtained in individuals in whom it was clinically obvious
of PS. that they had attained their adult height.
Laboratory Investigations
Materials and Methods
To determine serum testosterone levels, a competitive im
Subjects munoassay (Architect, Abbott, Abbott Park, IL, USA) was
This study is part of the Amsterdam Cohort of Gender dys used (interassay coefficient of variation [CV] 6%-10%, lower
phoria (ACOG) study which includes the complete population limit of quantification [LOQ] 0.1 nmol/L) from January 2013.
of all ages seen at the gender identity clinic of the Amsterdam Serum estradiol levels were measured using liquid chromatog
University Medical Center, location VUmc from 1972 until raphy–tandem mass spectrometry (VUmc) with an interassay
December 2018 (9). Transgender boys were eligible for inclu coefficient of variation of 7% and an LOQ of 20 pmol/L from
sion if they had started PS before age 16 years, received testos July 2014. All values ≤20 pmol/L were entered as 20 pmol/L.
terone treatment for a minimum of 6 months, and if they had Serum testosterone and estradiol levels from before these dates
reached the age of 18 years at the time of data collection. were converted to Architect and liquid chromatography–tan
Transgender boys were excluded if they had not reached adult dem mass spectrometry values respectively as described by
height defined as height at skeletal age ≥14 years or a growth Wiepjes et al (16). From April 2012, the chemiluminescence
velocity416 The Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2
immunometric assay (Architect, Abbott) was used (interassay at start PS. Height SDS at start GAHT was compared between
CV 14 years at start of PS) The protocol for data collection for the ACOG dataset was as
sessed by the local medical ethical committee who determined
Characteristic Pubertal Postpubertal Total that the Medical Research Involving Human Subjects Act did
group group (n = 146) not apply to this data collection. The need for informed con
(n = 61) (n = 85) sent was waived because of the retrospective design of the
study and the size of the cohort.
Age at start PS (y) 12.7 ± 1.0 15.1 ± 0.9 14.1 ± 1.5
Height at start of PS (cm) 158.3 ± 8.5 166.4 ± 6.7 162.9 ± 8.5
Missing 0 (0) 4 (5) 4 (3)
Results
BMI at start of PS 18.8 ± 2.4 22.4 ± 3.8 20.4 ± 3.6 The ACOG dataset consisted of 8831 individuals, 3481 of
Missing 0 (0) 33 (39) 33 (23) whom were assigned female at birth and of whom 1320 had
their first appointment before the age of 18 years. After selec
BMI SDS at start of PS 0.3 ± 1.1 0.9 ± 1.1 0.6 ± 1.1
tion for GnRHa use (n = 693), testosterone use (n = 533), age
Missing 0 (0) 33 (39) 33 (23) ≥18 years at last visit from which data were available (397),
Bone age at start of PS (y) 12.4 ± 1.0 15.7 ± 1.1 13.7 ± 1.9 GnRHa initiation before the age of 16 years (148), exclusion
Missing 5 (8) 48 (56) 53 (36) of 1 subject who had not reached adult height, and 1 subject
PAH at start of PS (cm) 169.0 ± 7.6 167.3 ± 6.8 168.3 ± 7.3 who was treated with oxandrolone, a total of 146 transgender
Missing 5 (8) 48 (56) 53 (36) boys were included.
Midparental height (cm) 168.1 ± 6.2 166.4 ± 5.7 167.2 ± 6.0
Missing 5 (8) 26 (31) 31 (21) Baseline Characteristics
Tanner breast stage at The study population (n = 146) was divided into 2 subgroups
start of PS based on growth potential. The pubertal group consisted of 61
B2 8 (13) 0 (0) 8 (5) transgender boys with a mean age of 12.7 ± 1.0 years and BA
B3 20 (33) 0 (0) 20 (14) of 12.4 ± 1.0 at start of PS. The postpubertal group with little
or no growth potential consisted of 85 individuals with a
B4 23 (38) 10 (12) 33 (23)
mean age of 15.1 ± 0.9 years and BA of 15.7 ± 1.1 at start
B5 8 (13) 59 (69) 67 (46)
PS (Table 1). The outcomes of the pubertal group will be de
Missing 2 (3) 16 (19) 18 (12) scribed in detail. Data from the postpubertal group will be
Menarche before start of briefly described at the end of the Results section.
PS
Yes 20 (33) 81 (95) 100 (68)
Puberty Suppression
No 39 (64) 0 (0) 40 (27)
The mean duration of PS was 3.1 ± 0.9 years. At baseline,
Missing 2 (3) 4 (5) 6 (4) mean height was 158.3 ± 8.5 cm (female height SDS +0.1 ±
1.5, male height SDS −0.1 ± 1.5). During the puberty suppres
Data are presented as number (%) or mean ± SD.
Abbreviations: BMI, body mass index; PS, puberty suppression; PAH, sive phase, height increased by 8.6 cm (95% CI, 7.5-9.6) to
predicted adult height; SDS, SD score. 166.9 ± 7.0 cm at start of GAHT. Female height SDSThe Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2 417
decreased to −0.2 ± 1.0 (decrease of −0.2; 95% CI, −0.5 to 1 year (n = 39, 13.6 months to adult dose [IQR, 12.8-15.9]),
0.1). Transgender boys with BA >12 years at start PS declined no differences in change in height SDS during GAHT were ob
more in height SDS during PS compared with transgender served (Fig. 3). Additionally, adult height did not differ be
boys with BA ≤12 years (difference between groups −0.6; tween the 2 dosing regimens (difference between groups
95% CI, −0.7 to −0.4) (Fig. 1), but height SDS at start of 0.8 cm; 95% CI, −3.0 to 4.6). Both groups were comparable
GAHT did not differ between the groups (difference 0.3; at baseline regarding age, height, and BA at the start of PS,
95% CI, −0.3 to 0.9). Additionally, PS resulted in a deceler midparental height, and PAH at start PS. When analyzed as
ation of bone maturation. At the beginning of PS, BA was a continuous variable, time to adult dose was not associated
comparable to CA with a BA – CA of −0.3 ± 0.9 years. This with the difference between adult height and PAH at the start
difference was greater among those with BA ≤12 at start PS of PS and PAH at the start of HT either (data not shown).
compared with those with BA >12 years (difference, 0.7 years; When looking at the difference between adult height and
95% CI, 0.2-1.2). At start of GAHT, the difference between PAH at the start of PS, an inverse correlation with BA at start
BA and CA further increased to −2.2 ± 1.2 years (change since PS was found (Fig. 4). A younger BA at the start of PS was as
start of PS −1.9 years; 95% CI, −2.2 to −1.6). PAH increased sociated with an adult height further above PAH (1.2 cm/y;
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
by 2.4 cm (95% CI, 1.3-3.4) between start PS and start 95% CI, 0.3-2.1). A similar correlation was observed between
GAHT. BA at start GAHT and the difference between adult height and
PAH (1.2 cm/y; 95% CI, 0.5-2.0). Those with a younger BA at
the start of PS also had an adult height further above midpar
Hormone Treatment ental height, but this correlation did not reach statistical sig
GAHT was initiated at a mean age of 15.8 ± 0.5 years. From nificance (1.3 cm/y; 95% CI, −0.4 to 3.0).
the start of GAHT, height increased by 5.0 cm (95% CI, A lower BMI SDS at the start of PS was associated with an
4.3-5.8) to an adult height of 172.0 ± 6.9 (female height SDS adult height further above PAH at the start of PS. Per 1 SDS
+0.2 ± 1.1, male height SDS −1.7 ± 1.0) (Fig. 2). Female decrease in BMI, the adult height was 0.4 cm further above
height SDS increased by 0.3 SDS from the start of GAHT to PAH at the start of PS, but this was not statistically signifi
adult height (95% CI, 0.2-0.5) (Table 2 and Fig. 3). cant (95% CI, 0.0-0.8). In a multivariable analysis, associa
However, adult height SDS did not differ from height SDS tions between BA and BMI SDS at start PS on the 1 hand and
at the start of PS (difference, 0.1; 95% CI, −0.2 to 0.4). the difference between adult height and PAH at start PS on
Compared with male reference data, 22 subjects (36%) had the other hand were similar to those in the univariable
an adult height below −2.0 SDS. BA – CA remained stable analysis.
in the first 18 months of GAHT but after that, BA progressive
ly increased. In 45 subjects (74%), adult height was taller than
Laboratory Investigations
PAH at the start of PS. Adult height 3.9 ± 6.0 cm above mid
parental height (95% CI, 2.4-5.4) and 3.0 ± 3.6 cm above During the puberty suppressive phase, gonadotrophins were
PAH at start of PS (95% CI, 2.0-3.9), but adult height was suppressed (median LH 0.3 U/L [IQR, 0.3-0.4]; median FSH
close to PAH at the start of GAHT (difference, 0.2 ± 2.3 cm; 1.1 U/L [IQR, 0.8-1.7]). Median serum estradiol levels were
95% CI, −0.5 to 0.9). 20 pmol/L, which was the lower limit of detection (IQR,
20-20). IGF-1 levels did not significantly change after initi
ation of PS and remained stable during PS. Mean testosterone
Factors Influencing Growth levels in the first year of GAHT were not significantly higher
When comparing subjects who reached the adult testosterone in subjects who reached adult dose within 12 months com
dose within 1 year (n = 21, 10.8 months to adult dose [IQR, pared with >12 months (95% CI, −18.2 to 18.5 nmol/L).
9.5-11.6]) to those in whom the adult dose was reached after When adult testosterone dose was reached, median serum
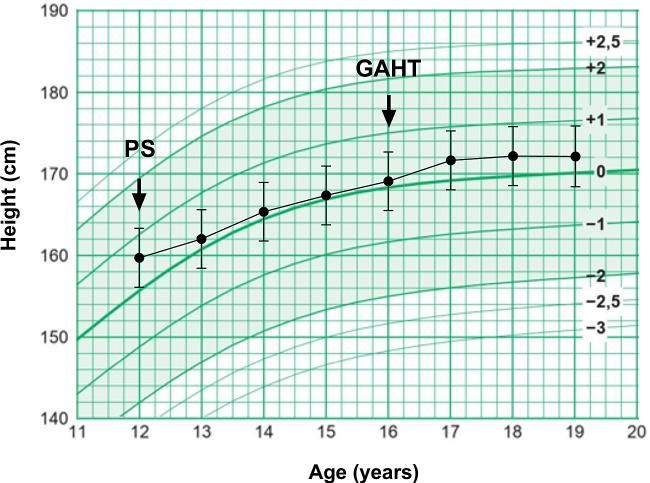
Figure 1. Effect of puberty suppression on female height SDS in Figure 2. Mixed model analysis of height during PS and GAHT of 17
subjects with BA ≤12 years (n = 32, 57%) and BA >12 years (n = 24, subjects who initiated PS at age 12 and GAHT at age 16, plotted on the
43%) at start of PS with 95% confidence intervals. PS, puberty growth chart for Dutch girls from Schönbeck et al (2). GAHT,
suppression. gender-affirming hormone therapy; PS, puberty suppression.418 The Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2
Table 2. Growth during puberty suppression and testosterone treatment in the pubertal and postpubertal group
Pubertal group (n = 61) Postpubertal group (n = 85) Pubertal vs postpubertal group (95% CI)
Height (cm)
Start of PS 158.3 ± 8.5 166.4 ± 6.7 8.0 (5.5-10.6)
Missing 0 (0) 4 (5)
Start of GAHT 166.9 ± 7.0 167.5 ± 7.0 0.6 (−1.7 to 2.9)
Missing 0 (0) 3 (4)
Adult height 172.0 ± 6.9 169.0 ± 6.8 3.0 (0.7-5.2)
Female height SDS
Start of PS +0.1 ± 1.5 −0.1 ± 1.0 0.1 (−0.3 to 0.6)
Missing 0 (0) 4 (5)
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
Start of GAHT −0.2 ± 1.0 −0.2 ± 1.1 0.0 (−0.3 to 0.4)
Missing 0 (0) 3 (4)
Adult height +0.2 ± 1.1 −0.3 ± 1.1 0.5 (0.1-0.8)
PAH at start of GAHT (cm) 172.3 ± 7.5 168.9 ± 7.5 3.5 (0.0-7.0)
Missing 18 (30) 53 (62)
Δ Adult height—PAH (cm)
PAH at start PS 3.0 ± 3.6 1.8 ± 2.0 1.2 (−0.1 to 2.4)
Missing 5 (8) 48 (56)
PAH at start of GAHT 0.2 ± 2.3 1.4 ± 1.6 1.2 (0.2-2.1)
Missing 18 (30) 53 (62)
Δ Adult height—midparental height (cm) 3.9 ± 6.0 3.0 ± 4.7 0.9 (−1.0 to 2.9)
Missing 5 (8) 26 (31)
Δ BA – CA (cm)
Start of PS −0.3 ± 0.9 0.9 ± 1.0 1.2 (0.8-1.6)
Missing 5 (8) 48 (56)
Start of GAHT −2.2 ± 1.2 0.1 ± 1.0 2.4 (1.8-2.9)
Missing 18 (30) 53 (62)
Data are presented as number (%) or mean ± SD.
Abbreviations: BA, bone age; CA, chronological age; GAHT, gender-affirming hormone treatment; PAH, predicted adult height; PS, puberty suppression; SDS,
SD score.
testosterone levels were 20 nmol/L (IQR, 11-35) and free tes initiation of testosterone and remained stable thereafter with
tosterone was 599 pmol/L (IQR, 338-1179). IGF-1 levels a mean serum level of 32.3 ± 5.9 nmol/L. No significant differ
slightly increased by 3.6 nmol/L (95% CI, 0.9-6.4) after ences in IGF levels during GAHT between participants who
Figure 3. Effect of hormone treatment on female height SDS in
transgender boys in whom adult testosterone dose was reached Figure 4. Diagram of the correlation between bone age at start
withinThe Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2 419
reached adult dose within 12 months and those who reached The effect of GnRHa and testosterone on adult height in
adult dose >12 months were observed. transgender boys was analyzed in 4 manners: (1) the change
in height SDS during the treatment; (2) the difference between
adult height and PAH at start PS; (3) the difference between
Adolescents With Little or no Growth Potential adult height and midparental height; and (4) comparison of
(Postpubertal Group) growth data from the pubertal group with the “control”
In total, 85 transgender boys had little or no growth potential group of postpubertal adolescents with little/no growth poten
at the start of PS (Table 1). The mean duration of PS was 1.2 ± tial at start of the treatment.
0.8 years. Height at start PS was missing in 4 subjects. From Adult height SDS was comparable to height SDS at start PS,
the start of PS, height increased by 2.5 cm (95% CI, 2.1-3.0) which would imply that PS and GAHT have no impact on
to an adult height of 169.0 ± 6.8 cm (female height SDS adult height.
−0.3 ± 1.1, male height SDS −2.1 ± 1.0) (Table 2). In 70 In contrast, adult height was 3.0 ± 3.6 cm above PAH at
(82%) subjects, height increased ≥1 cm during treatment. start PS. This deviation was greater than the slight underesti
Adult height was 3.0 ± 4.7 cm above midparental height mation of adult height by 1.2 ± 4.1 cm and 0.4 ± 4.3 cm de
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
(n = 57) and 1.8 ± 2.0 cm above PAH at start PS (n = 37). scribed by Zachmann et al in healthy girls with an age of 12
When comparing adult height in the pubertal group to that and 13 years, respectively, using the same method of Bayley
in the postpubertal group, individuals in the pubertal group and Pinneau to predict adult height (22). This might suggest
were taller (difference, 3.0 cm; 95% CI, 0.7-5.2). However, a slight enhancing effect of PS and GAHT on adult height.
the difference between adult height and midparental height This is further supported by the finding that adult height
was not significantly different between the groups (difference, was 3.9 ± 6.0 cm above midparental height.
0.9 cm; 95% CI, −1.0 to 3.0). Finally, the fact that subjects from the pubertal group were
3.0 cm taller than those with little/no growth potential at the
start of treatment also suggests a positive effect on growth.
Discussion However, when comparing the difference between midparen
This study is the first to investigate the effect of both GnRHa tal height and adult height in both groups, no significant dif
and testosterone treatment on growth and adult height in ferences were found. This might be explained by the fact
transgender boys. We observed a decrease in growth velocity that midparental height was missing in 31% of the postpuber
and bone maturation during PS and an increase in growth dur tal group. It is possible that physicians enquired about paren
ing GAHT. Adult height was taller than predicted at the start tal height more often when subjects were shorter to try and
of the treatment, and this difference was more pronounced understand if short stature was familial.
when the treatment was initiated earlier. In contrast, the tem When all 4 methods to evaluate the effect on adult height
po of the testosterone dose increase did not affect growth. are combined, we conclude that treatment with PS and
During the puberty suppressive phase, we observed a mean GAHT does not negatively influence adult height in trans
decrease in height SDS of −0.2. Ghelani et al reported no sig gender boys. When comparing adult height to height pre
nificant changes in height SDS of GnRHa treatment (6). This dicted at the start of treatment, to midparental height and to
was because their subjects were older (median age of 16.6 height in the control group, there even seems to be a slight
years) and were only followed for 1 year. Our data showed positive effect of PS and GAHT on growth.
a greater decrease in height SDS among those with more ad When looking at factors that might influence growth, tem
vanced BA (>12 years) at the start of PS. In subjects with po of testosterone dose increase was not found to affect
younger BA height, SDS did not decline. This may be due growth or adult height. In boys with constitutional delay of
the fact that the group with BA >12 years consisted of more growth and puberty and central hypogonadotropic hypo
early maturers, who were relative tall for their age, with a re gonadism it is thought that higher doses of testosterone induce
gression to the mean after the initiation of GnRHa treatment. accelerated skeletal maturation and thereby compromise
This is supported by the fact that baseline height SDS was adult height (23–25). We did not observe such an effect in
higher in the group with BA >12 years but height SDS at the transgender boys, nor was there a significant difference in tes
start of GAHT was similar in the groups with BA ≤12 and tosterone levels, but this might also be attributed to the un
>12 years. Our results are similar to findings in a previous timed blood tests resulting in a wide variation of serum
study by Weise et al in girls with central precocious puberty testosterone levels. Based on these findings, gradually increas
treated with GnRHa (18). A lower growth velocity in girls ing the dose over the first year of GAHT seems to allow ado
with BA ≥10 years was reported compared with girls with lescents to attain their growth potential. However, we did not
BA420 The Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2
slightly further above midparental height in those with a Data Availability
younger BA, which also indicates a positive impact of starting
The dataset generated during and analyzed during the current
treatment at a younger BA on adult height. This contradicts
study is not publicly available because of privacy regulations.
findings in girls with early-normal puberty in whom treatment
with GnRHa did not result in an increase of adult height (26).
An explanation might be found in the different treatment reg References
imens. Puberty suppression until the age of 16 years followed
1. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treat
by puberty induction with testosterone may have different ef
ment of gender-dysphoric/gender-incongruent persons: an
fects on the epiphyseal growth plates compared with a shorter Endocrine Society Clinical Practice Guideline. J Clin Endocrinol
period of PS followed by endogenous puberty with estradiol. Metab. 2017;102(11):3869-3903.
Although not statistically significant, there was a trend to 2. Schönbeck Y TH, van Dommelen P, Bakker B, et al. The world’s
ward a negative association between BMI SDS at start PS tallest nation has stopped growing taller: the height of Dutch chil
and the difference between adult height and PAH at start dren from 1955 to 2009. Pediatr Res. 2013;73(3):371-377.
PS. Earlier studies also described a negative effect of higher 3. Boogers LS, Wiepjes CM, Klink DT, et al. Trans girls grow tall:
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
BMI on adult height by accelerated growth and earlier epi adult height is unaffected by GnRH analogue and estradiol treat
physeal closure (27, 28). The absence of a statistically signifi ment. J Clin Endocrinol Metab. 2022;107(9):e3805-e3815.
4. Schagen SE, Cohen-Kettenis PT, Delemarre-van de Waal HA,
cant association in our study might be explained by the fact
Hannema SE. Efficacy and safety of gonadotropin-releasing hor
that BMI was within the normal range in most subjects.
mone agonist treatment to suppress puberty in gender dysphoric
Since 36% of the transgender boys had an adult height < −2 adolescents. J Sex Med. 2016;13(7):1125-1132.
SDS compared with the male population, which many, in our 5. Schulmeister C, Millington K, Kaufman M, et al. Growth in trans
clinical experience, are sad about, future research should in gender/gender-diverse youth in the first year of treatment with
vestigate possible therapeutic options to enhance adult height. gonadotropin-releasing hormone agonists. J Adolesc Health.
Because estradiol has an important role in epiphyseal closure, 2022;70(1):108-113.
aromatase inhibition alongside GnRHa and testosterone 6. Ghelani R, Lim C, Brain C, Fewtrell M, Butler G. Sudden sex hor
might be an effective treatment (29). However, there are no ef mone withdrawal and the effects on body composition in late pu
ficacy or safety data on such an approach in transgender boys, bertal adolescents with gender dysphoria. J Pediatr Endocrinol
Metab. 2020;33(1):107-112.
and it may have a negative impact on bone mineral accrual,
7. Roberts SA, Carswell JM. Growth, growth potential, and influences
which is already attenuated by GnRHa treatment. An
on adult height in the transgender and gender-diverse population.
American study by Grimstad et al reported a 5 cm taller height Andrology. 2021;9(6):1679-1688.
in transgender boys treated with oxandrolone, an androgen 8. van de Grift TC, van Gelder ZJ, Mullender MG, Steensma TD, de
which cannot be aromatized to estrogen, compared with un Vries AL, Bouman M-B. Timing of puberty suppression and surgi
treated individuals (30). However, the relatively small groups cal options for transgender youth. Pediatrics. 2020;146(5):
in this study were not comparable regarding age at the start of e20193653.
treatment. The use of oxandrolone, which is currently not 9. Wiepjes CM, Nota NM, de Blok CJM, et al. The Amsterdam cohort
available in Europe, or aromatase inhibitors to promote adult of gender dysphoria study (1972-2015): trends in prevalence, treat
height might be promising but needs further research. ment, and regrets. J Sex Med. 2018;15(4):582-590.
10. American Psychiatric Association. Diagnostic and Statistical
This study has strengths and limitations. Strengths are the
Manual of Mental Disorders. American Psychiatric Association
reasonable cohort size and the comparison with individuals
Publishing; 2000.
who (nearly) reached adult height before the start of treatment 11. American Psychiatric Association. Diagnostic and Statistical
as controls. The retrospective character of the study is a limi Manual of Mental Disorders. 5th ed. American Psychiatric
tation because this resulted in some missing data. Other limi Association Publishing; 2018.
tations are that X-rays for BA were assessed by various 12. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a stand
radiologists, possibly resulting in interobserver variability, ard definition for child overweight and obesity worldwide: inter
and that hormone regimens were individualized, making it national survey. BMJ. 2000;320(7244):1240-1243.
more difficult to compare treatment strategies. 13. Tanner JM, Goldstein H, Whitehouse RH. Standards for children’s
height at ages 2-9 years allowing for heights of parents. Arch Dis
Child. 1970;45(244):755-762.
Conclusion 14. Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development
of the Hand and Wrist. 2nd ed. Stanford University Press; 1959.
This study has provided new information on the impact of 15. Bayley N, Pinneau SR. Tables for predicting adult height from skel
GnRHa and testosterone treatment on growth and adult etal age: revised for use with the Greulich-Pyle hand standards. J
height, which can be used to counsel transgender boys. PS re Pediatr. 1952;40(4):423-441.
sulted in decelerated growth and bone maturation, which ac 16. Wiepjes CM, de Blok CJ, Staphorsius AS, et al. Fracture risk in trans
celerated after the initiation of testosterone. Although the women and trans men using long-term gender-affirming hormonal
growth pattern was altered by PS and GAHT, the treatment treatment: a nationwide cohort study. J Bone Miner Res.
does not have a negative impact on adult height. There may 2020;35(1):64-70.
even be a slight positive effect on adult height that is more pro 17. Twisk J, de Boer M, de Vente W, Heymans M. Multiple imputation
of missing values was not necessary before performing a longitudin
nounced in those who start GnRHa at a younger age.
al mixed-model analysis. J Clin Epidemiol. 2013;66(9):1022-1028.
Nonetheless, adult height was below −2 SDS compared with
18. Weise M, Flor A, Barnes KM, Cutler GB Jr, Baron J. Determinants
the general male population in 36%. Future research is needed of growth during gonadotropin-releasing hormone analog therapy
to assess the efficacy and safety of possible treatment options for precocious puberty. J Clin Endocrinol Metab. 2004;89(1):
for those who have a strong wish to increase adult height into 103-107.
the male reference range, such as oxandrolone or aromatase 19. Clemons RD, Kappy MS, Stuart TE, Perelman AH, Hoekstra FT.
inhibitors. Long-term effectiveness of depot gonadotropin-releasing hormoneThe Journal of Clinical Endocrinology & Metabolism, 2023, Vol. 108, No. 2 421
analogue in the treatment of children with central precocious pu 25. Boehm U, Bouloux P-M, Dattani MT, et al. European Consensus
berty. Am J Dis Child. 1993;147(6):653-657. statement on congenital hypogonadotropic hypogonadism—
20. Boepple PA, Mansfield MJ, Crawford JD, Crigler JF Jr, Blizzard pathogenesis, diagnosis and treatment. Nat Rev Endocrinol.
RM, Crowley WF Jr. Gonadotrophin-releasing hormone agonist
2015;11(9):547-564.
treatment of central precocious puberty: an analysis of growth
26. Bangalore Krishna K, Fuqua JS, et al. Use of gonadotropin-releasing
data in a developmental context. Acta Paediatr Scand Suppl.
1990;367:38-43. hormone analogs in children: update by an international consor
21. Stoffers IE, de Vries MC, Hannema SE. Physical changes, labora tium. Horm Res Paediatr. 2019;91(6):357-372.
tory parameters, and bone mineral density during testosterone 27. Brener A, Bello R, Lebenthal Y, Yackobovitch-Gavan M, Phillip M,
treatment in adolescents with gender dysphoria. J Sex Med. Shalitin S. The impact of adolescent obesity on adult height. Horm
2019;16(9):1459-1468. Res Paediatr. 2017;88(3-4):237-243.
22. Zachmann M, Sobradillo B, Frank M, Frisch H, Prader A. 28. Sopher AB, Jean AM, Zwany SK, et al. Bone age advancement in
Bayley-Pinneau, Roche-Wainer-Thissen, and Tanner height predic prepubertal children with obesity and premature adrenarche: pos
tions in normal children and in patients with various pathologic sible potentiating factors. Obesity (Silver Spring). 2011;19(6):
conditions. J Pediatr. 1978;93(5):749-755.
1259-1264.
Downloaded from https://academic.oup.com/jcem/article/108/2/414/6747528 by guest on 11 December 2023
23. Rogol AD. New facets of androgen replacement therapy during
29. Wit JM. Should skeletal maturation be manipulated for extra height
childhood and adolescence. Expert Opin Pharmacother.
2005;6(8):1319-1336. gain? Front Endocrinol (Lausanne). 2021;12:812196.
24. Young J. Approach to the male patient with congenital hypogona 30. Grimstad FW, Knoll MM, Jacobson JD. Oxandrolone use in trans-
dotropic hypogonadism. J Clin Endocrinol Metabol. 2012;97(3): masculine youth appears to increase adult height: preliminary evi
707-718. dence. LGBT Health. 2021;8(4):300-306.You can also read