Issue Brief Progressive or Regressive? A Second Look at the Tax Exemption for Employer-Sponsored Health Insurance Premiums
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
May 2009
Issue Brief
Progressive or Regressive? A Second
Look at the Tax Exemption for Employer-
Sponsored Health Insurance Premiums
Cathy Schoen, Kristof S tremikis , Sara Collins, and Karen Davis
T he C ommonwealth F und
The mission of The Commonwealth ABSTRACT: The major argument for capping the exemption of health insurance benefits
Fund is to promote a high performance from income tax is that doing so will generate significant revenue that can be used to
health care system. The Fund carries finance an expansion of health coverage. This analysis finds that given the state of insur-
out this mandate by supporting
ance markets and current variations in premiums, limiting the current exemption could
independent research on health care
issues and making grants to improve adversely affect individuals who are already at high risk of losing their health coverage.
health care practice and policy. Support Evidence suggests that capping the exemption for employment-based health insurance
for this research was provided by could disproportionately affect workers in small firms, older workers, and wage-earners in
The Commonwealth Fund. The views industries with high expected claims costs. To avoid putting many families at increased
presented here are those of the authors health and financial risk, and to avoid undermining employer-sponsored group coverage,
and not necessarily those of The
any consideration of a cap would have to be combined with coverage for all, changes in
Commonwealth Fund or its directors,
officers, or staff. insurance market rules, and shared responsibility for financing.
For more information about this study,
please contact:
Cathy Schoen, M.S.
Senior Vice President Overview
Research & Evaluation Eliminating or capping the exemption, or exclusion, of employer-based health
The Commonwealth Fund
E-mail cs@cmwf.org insurance from personal and Social Security taxes has often been described as
progressive tax policy, and as one way to raise revenue for an expansion of cov-
erage.1 This issue brief assesses some of the implications of proposals to change
the tax treatment of employer-sponsored health plans by reviewing current
sources of variation in insurance premiums. It also uses recent data on the benefits
To download this publication and
learn about others as they become
of the current income-based tax exemption in order to examine the tax incidence
available, visit us online at effect—the change in tax as a share of income—of eliminating the exemption.
www.commonwealthfund.org and
Our analysis finds that given the state of insurance markets and present vari-
register to receive Fund e-Alerts.
ations in premiums, limiting the current exemption could adversely affect indi-
Commonwealth Fund pub. 1269
Vol. 53 viduals who are already at high risk of losing their health coverage. Evidence2 T he C ommonwealth F und
suggests that capping the exemption for employment- businesses will save approximately $100 billion in
based health insurance could disproportionately affect payroll tax.3 Five-year (2008–12) estimates of uncol-
workers in small firms, older workers, and wage-earn- lected revenue run from $799 billion to $835 billion.
ers in high-risk industries (those with high expected The CBO further estimates that limiting the
claims costs, such as farming and construction). exemption for employer-provided health benefits to
Without adjusting for cost of living, such a cap would the 75th percentile of health insurance premiums, and
also disproportionately affect those working in high- indexing the cap to inflation, would save $452.1 bil-
cost geographic areas. lion over the 10-year period 2009–18.4 In examining a
Claims that the current tax treatment of health range of potential revenue sources in the context of
insurance benefits is regressive are typically based on comprehensive health reform, a recent Commonwealth
changes in absolute tax dollars rather than changes in Fund report analyzed the revenue effect of capping the
tax rates. In economics, tax increases are defined as tax exemption at the premium level of a nationwide
“progressive” if they represent a greater share of benchmark health plan offered to everyone within a
income for higher-income households. Defined as a national health insurance exchange implemented along
share of income, the value of the current tax exemp- with broad insurance market reforms (e.g., community
tion is larger for low- and middle-income households rating and pooling of health risks).5 Taxing health ben-
with employer-provided coverage than for high- efits in excess of the benchmark plan premiums of
income households. Elimination of the exemption $3,000 for single coverage and $9,000 for family cov-
would thus introduce a much greater increase in fed- erage was projected to generate $344 billion over the
eral tax liability for households with incomes below 2010–2019 period. Phasing down the tax exemption
$50,000 than for those with incomes above $200,000, for workers with incomes between $250,000 and
and increase the tax rate of lower-income households $500,000 and eliminating the exemption above
with employer coverage more than those higher- $500,000 were projected to generate $24 billion during
income households. Therefore, a cap on the tax that same period.
exemption of health benefits would represent a regres-
sive—not progressive—change in tax policy. Concerns with Caps: Premium
Variation by Firm Size, Region,
Capping the Exemption: Revenue for and Risk
Financing a Coverage Expansion While eliminating or limiting the exemption for
The major argument for capping the exemption of employer-provided health benefits would generate a
health insurance benefits from income tax is that doing significant amount of federal revenue, any change to
so will generate significant revenue that can be used to the current tax policy must be carefully assessed for
finance an expansion of health coverage. The potential unintended consequences. Employment-
Congressional Budget Office (CBO) estimates that the related group insurance is currently the primary source
existing personal income and payroll tax exemptions of coverage for the under-65 population, insuring two-
for employee health benefits resulted in $246 billion of thirds of working-age adults, and the tax exemption
forgone federal revenue in 2007.2 These exemptions for such coverage has helped support the pooling of
translate into tax savings that are divided among work- health risks and group health insurance.
ers and their employers. Projections by the CBO and Some believe that the current exemption should be
congressional Joint Committee on Taxation show that limited to create incentives for individuals to select
workers with employment-based health benefits will less-comprehensive insurance benefits or more cost-
save roughly $145 billion to $175 billion in individual effective health plans. The concern is that the tax sub-
income taxes in FY2009, while both employees and sidy for premiums may, at the margin, undermineP rogressive or R egressive ? Tax E xemption for E mployer -S ponsored H ealth I nsurance P remiums 3
incentives to choose higher-value, lower-cost health proportionately increase taxes for employees of small
plans.6 This view often assumes that health insurance firms, irrespective of their benefit package.
benefits in plans with premium costs that are above the
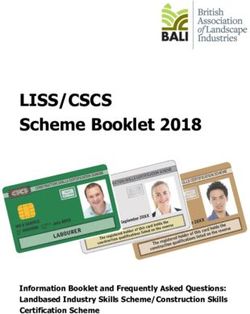
national average are “excessive.” Geographic location. Premiums also vary by where
In truth, however, many so-called “gold-plated” employees live. Analysis by EBRI’s Fronstin of the
health benefit premiums are high only because insur- Kaiser Family Foundation/Health Research and
ance costs vary according to the size of the firm, the Educational Trust Employer Health Benefits Annual
geographic region in which it is located, and the com- Survey shows that, in 2008, the average total health
position of the employer’s risk pool.7 In today’s insur- insurance premium for family coverage in the
ance markets, establishing a universal cap will have a Northeast was $13,656, while coverage for a family in
disproportionate impact on workers in small firms, the South averaged $12,252 (Exhibit 2). Furthermore,
high-cost areas, and expensive risk pools.8 premiums for MediGap policies with the same benefits
also vary widely—an indication that underlying health
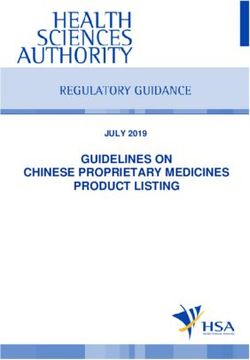
Firm size. Without economies of scale and the ability care markets and costs, rather than benefit design, are
to pool risk broadly, small businesses tend to pay driving premium variations.
higher premiums, despite having less-comprehensive
benefits. Recent analysis of Medical Expenditure Exhibit 2. Average Total Family Premium at Private-Sector
Establishments, by Geographic Region, 2008
Panel Survey (MEPS) data for employers, conducted
$16,000
by Paul Fronstin of the Employee Benefit Research $13,656
$14,000 $12,680 $12,809 $12,351 $12,252
Institute (EBRI), shows that the average total premium $12,000
for employee-only coverage in a business with fewer $10,000
than 10 workers was $4,498 in 2006, about 10 percent $8,000
$6,000
greater than the average premium in firms with more
$4,000
than 1,000 workers (Exhibit 1). Research by Jon Gabel $2,000
demonstrates that this excess cost is not going toward $0
Average Northeast Midwest West South
additional “gold-plated” coverage.9 Overall, the higher Region
Data: Kaiser/HRET 2008.
average premiums paid by small businesses typically Source: P. Fronstin, Capping the Tax Exclusion for Employment-Based Health Coverage:
Implications for Employers and Workers (Washington, D.C.: Employee Benefit Research
buy less-comprehensive benefit packages with much Institute, Jan. 2009).
higher deductibles and cost-sharing. Capping the tax
exemption at the “average” premium could thus dis- A uniform cap at the national average would thus
increase taxes in higher-cost states and regions. Even
Exhibit 1. Average Total Employee-Only Premium at
if policies were put in place to moderate costs in
Private-Sector Establishments, by Firm Size, 2006
expensive health care markets where there is evidence
$5,000 $4,498
$4,500 $4,118 $4,241 $4,112
of inefficient or wasteful care, without adjusting for
$4,035 $4,066
$4,000 the cost of living the cap would still disproportionately
$3,500
$3,000 affect workers living in high-cost areas.
$2,500
$2,000
$1,500 Risk pool. The composition of an employer’s risk pool
$1,000 is directly correlated with the employees’ coverage
$500
$0 premium. Through the process of medical underwrit-
Total4 T he C ommonwealth F und
employed by a firm where workers are sicker or older of after-tax income for workers earning more than
than the norm, or where all workers face higher health $200,000 a year (Exhibits 3 and 4).12 Although it is
risks, are likely to face higher premiums than individu- true that low-income workers are far less likely than
als insured in a lower-risk group. A non-targeted cap high-income workers to have employment-based
on the employer-provided health benefits exemption health insurance, the value of the current tax treatment
would result in additional taxes for workers in high- is high as a share of income for low- and middle-wage
cost groups, even though their benefits may be equiva- workers that have such health benefits.13 Further, tax
lent to, or worse than, those received by their counter- changes in the context of health reform that requires
parts in lower-cost groups. employers to provide health insurance to workers or
Without substantial market reforms, a uniform cap contribute to a fund would result in nearly all workers
would have the unintended consequence of differen- receiving coverage from their employers.
tially taxing benefits for workers in small firms, old Employers typically pay the same premium for
and high-risk groups, and high-cost geographic areas. health insurance for all eligible workers, irrespective
Although it would be possible to adjust for some of of income level, although payments vary based on
these factors, the technical challenge of varying limits whether the plan is for single or family coverage. Over
in the tax code and the complications encountered the past decade, premiums have generally increased
while attempting to value health benefits under now- far faster than wages.14 As a result, employer payments
repealed Section 89 of the Tax Reform Act of 1986 for health insurance premiums represent a substantial
may give policymakers pause.11 share of total compensation for low-and middle-
income employees and a much lower share for upper-
Regressive Consequences of income employees and corporate executives.15 Thus,
Eliminating the Current Exemption the federal tax exemption for employer-paid premiums
Eliminating the current tax exemption for employer- is of particular value to low-wage and middle-income
provided health benefits would also have important, workers and their families.
often overlooked regressive consequences for low- and Currently, premium payments for employer-
middle-income individuals and families. While the sponsored plans are exempt from Social Security taxes
average tax subsidy for health benefits in absolute dol- as well as federal income taxes. This exemption is
lars is larger for workers higher on the income ladder, especially valuable to low- and middle-income
the subsidy amounts to nearly 10 percent of after-tax employees, because all of their income is subject to
income for very low-wage workers and only 1 percent Social Security taxes. As of 2009, employees pay a
Exhibit 3. ESI Tax Subsidies in Absolute Dollars and as a Exhibit 4. Current ESI Tax Subsidies in Absolute Dollars and as a
Percentage of After-tax Income, for Tax Units with ESI, 2004 Percentage of After-tax Income, for Tax Units with ESI, 2004
Subsidy as a Percentage Average Subsidy (Dollars) Subsidy as a Percentage of Income
Income Average Subsidy of After-Tax Income $3,500 12
2,943
Less than $10,000 $580 9.7% $3,000 2,690 10 9.7
$10,000–$20,000 $1,168 8.4% $2,500 2,298
8.4
8 7.6
$20,000–$30,000 $1,622 7.6% $2,000
1,960
1,733
$30,000–$40,000 $1,621 5.8% 1,622 1,621 6 5.8
5.0
$1,500 1,168 4.4
$40,000–$50,000 $1,733 5.0% 4 3.9
3.2
$1,000
$50,000–$75,000 $1,960 4.4% 580
2
$500 1.0
$75,000–$100,000 $2,298 3.9%
$0 0
$100,000–$200,000 $2,690 3.2%P rogressive or R egressive ? Tax E xemption for E mployer -S ponsored H ealth I nsurance P remiums 5
6.2 percent FICA tax for Social Security and employ- incomes in excess of $200,000 will see an average
ers pay an additional 6.2 percent on incomes up to change in tax rates of only 0.1 percent.
$106,800. Employees with incomes below this thresh-
old would therefore pay additional FICA tax (as well Conclusion: Costs and Consequences
as additional income tax) on employer-paid premium Changes to the federal income tax treatment of health
amounts if these were not exempt. insurance benefits were a feature of many leading
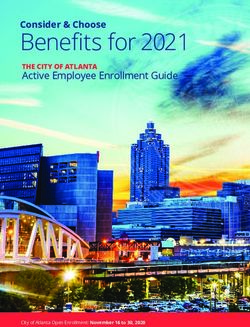
Eliminating the health benefits exemption would health reform bills in the 110th Congress and are likely
substantially increase federal tax liability for those to continue to be proposed in the 111th.16 While
lower- and middle-income families who receive health modifications may bring significant increases in fed-
benefits through their jobs. Preliminary analysis by the eral revenue that could be used for coverage expan-
Urban Institute and Brookings Institution indicates that sion, any change to the current tax policy must be
workers with employer-sponsored insurance who earn carefully targeted.
between $30,000 and $40,000 per year would see total As shown in this brief, high premiums are not an
federal tax increases of 48 percent. Eliminating the indication that insurance coverage is excessive or that
exemption for workers with employer-provided health a plan is “gold-plated.” Moreover, it was shown that
benefits who earn between $40,000 and $50,000 and establishing a universal cap on the tax exemption for
between $50,000 and $75,000 would increase tax lia- health benefits would have a disproportionate impact
bility by 28 percent and 20 percent, respectively on workers in small firms, high-cost areas, and expen-
(Exhibit 5). sive risk pools. To avoid putting sicker, older, and low-
or modest-income families at increased health and
Exhibit 5. Effect of Ending Current ESI Tax Subsidies, financial risk, and to avoid potentially undermining
for Tax Units with ESI, 2004
current employer-sponsored pooled-risk group cover-
Percentage Increase in Changes in Average
Total Income Taxes Income Tax Rates age, any consideration of a cap would have to be
60 14
12.6 combined with coverage for all, changes in insurance
50 48.1 12
10 market rules, and shared responsibility for financing.
40
30 28.4 8 In the context of market rules that require community
19.9 6 4.9
20 17.4
12.6 4 rating and broadly pooled risk, a cap pegged to a
1.7
10
1.9
2 1.0 0.6 0.7 0.7
0.1 benchmark-quality health plan could potentially avoid
0 30-40 40-50 50-75 75–100 100 –200 200+ 0
10-20 20-30 30-40 40-50 50-75 75 100 200+
–100 –200 disproportionately increasing taxes on employees
Income (thousands), Tax Units with ESI
working for small businesses or on employee groups
Note: Percentage increase in total income taxes is change in tax liability divided by baseline
tax liability. Data on percentage increase is not shown for tax units with less than $30,000 in with a higher health risk. And by requiring employers
income due to very low baseline tax liability. Change in average income tax rates is new tax
divided by new income minus baseline tax divided by baseline income.
Data: Tax Policy Center calculations based on HIPSM database.
either to provide health coverage or to contribute to an
insurance trust, the risk that a cap might unravel finan-
The resulting total change in average federal cial support for health benefits could be avoided.
income tax rates—defined as (after-repeal tax liabil- Still, this source of revenue for financing a cover-
ity)/(after-repeal income) – (baseline tax liability)/ age expansion would continue to be more regressive
(baseline income)—would also be greater for low- that other potential sources. Even with the implemen-
wage workers who have employer-paid health benefits. tation of comprehensive insurance reform, it would
The average income tax rates are projected to increase be important to recognize that changing the current
by 5 percent to 13 percent of income for families with tax treatment of employer-provided health benefits
incomes below $30,000 (12.6 percent below $20,000) will have consequences for low-income individuals
and 1 percent to 2 percent for families with incomes and families. Viewed from the perspective of tax
between $30,000 and $50,000. Meanwhile, those with increases as a share of income, eliminating the tax6 T he C ommonwealth F und
exemption for employee health benefits would be a income households. Eliminating it would thus increase
regressive—not progressive—tax policy change. The the tax burden on low-income households, as a percent-
current exemption represents a larger tax break as a age of income and as a percentage of current tax liabil-
percentage of income for low-income households with ity, more than it would for higher-income households.
employer coverage and a smaller tax break for higher-
N otes
10
1
B. Lyke, The Tax Exclusion for Employer-Provided S. R. Collins, K. Davis, C. Schoen, M. M. Doty,
Health Insurance: Policy Issues Regarding the S. K. H. How, and A. L. Holmgren, Will You Still
Repeal Debate (Washington, D.C.: Congressional Need Me? The Health and Financial Security of
Research Service, Nov. 2008), p. 2. Older Americans (New York: The Commonwealth
2
Fund, June 2005).
Congressional Budget Office, Budget Options,
11
Volume 1: Health Care (Washington, D.C.: CBO, P. Fronstin, Capping the Tax Exclusion, 2009, p. 15.
Dec. 2008), p. 23. 12
L. E. Burman, B. Garrett, and S. Khitatrakun, “The
3
U.S. Joint Committee on Taxation, Estimates of Tax Code, Employer-Sponsored Insurance and the
Federal Tax Expenditures for Fiscal Years 2008– Distribution of Tax Subsidies,” in H. J. Aaron and
2012 (Washington, D.C.: U.S. Government Printing L. E. Burman (eds.), Using Taxes to Reform Health
Office, Oct. 2008); CBO, Budget Options, ibid. Insurance: Pitfalls and Promises (Washington, D.C.:
4
Brookings Institution, 2008).
CBO, Budget Options, 2008, p. 24.
13
5
The likelihood of having employment-based health
Commonwealth Fund Commission on a High insurance increases with income. Analysis of the
Performance Health System, The Path to a High March Current Population Survey, 2001–2008, by
Performance U.S. Health System: A 2020 Vision Elise Gould, Economic Policy Institute, in S. R.
and the Policies to Pave the Way (New York: The Collins, “Rising Health Care Costs: Implications
Commonwealth Fund, Feb. 2009). and Prospects for U.S. Health Reform,” presenta-
6
B. Lyke, Tax Exclusion, 2008, p. 12. tion to the Manufacturers Alliance/MAPI Presidents
7 Council Meeting, Nov. 20, 2008.
P. Fronstin, Capping the Tax Exclusion for
14
Employment-Based Health Coverage: Implications Commonwealth Fund Commission, Path to High
for Employers and Workers, (Washington, D.C.: Performance, 2009, p. 12.
Employee Benefit Research Institute, Jan. 2009), 15
B. G. Auguste, M. Laboissiere, and L. T. Mendonca,
p. 11. How Health Care Costs Contribute to Income
8
Insurance companies, for example, charge higher Disparity in the United States (San Francisco:
premiums for industries with greater likelihood of McKinsey Global Institute, March 2009).
physical injury, safety hazards, or catching infec- 16
S. R. Collins, J. L. Nicholson, and S. D. Rustgi,
tious diseases. An Analysis of Leading Congressional Health Care
9
J. Gabel, R. McDevitt, L. Gandolfo et al., Bills, 2007–2008: Part I, Insurance Coverage,
“Generosity and Adjusted Premiums in Job-Based (New York: The Commonwealth Fund, Jan. 2009).
Insurance: Hawaii Is Up, Wyoming Is Down,”
Health Affairs, May/June 2006 25(3):832–43; J. Gabel
and J. Pickreign, Risky Business: When Mom and
Pop Buy Health Insurance for Their Employees
(New York: The Commonwealth Fund, April 2004).P rogressive or R egressive ? Tax E xemption for E mployer -S ponsored H ealth I nsurance P remiums 7
A bout the A uthors
Cathy Schoen, M.S., is senior vice president for research and evaluation at The Commonwealth Fund and
research director for The Commonwealth Fund Commission on a High Performance Health System, oversee-
ing the Commission’s Scorecard project and surveys. From 1998 through 2005, she directed the Fund’s Task
Force on the Future of Health Insurance. She has authored numerous publications on policy issues, insurance,
and health system performance (national and international), and coauthored the book Health and the War on
Poverty. She has also served on many federal and state advisory and Institute of Medicine committees. Ms.
Schoen holds an undergraduate degree in economics from Smith College and a graduate degree in economics
from Boston College. She can be e-mailed at cs@cmwf.org.
Kristof Stremikis, M.P.P., is research associate for the president of The Commonwealth Fund. Previously, he was a
graduate student researcher in the School of Public Health at the University of California, Berkeley, where he evalu-
ated various state, federal, and global health initiatives while providing economic and statistical support to faculty
and postdoctoral fellows. He has also served as consultant in the director’s office of the California Department of
Healthcare Services, where he worked on recommendations for a pay-for-performance system in the Medi-Cal
program. Mr. Stremikis holds three undergraduate degrees in economics, political science, and history from the
University of Wisconsin at Madison. In May 2008, he received a Master of Public Policy degree from the Goldman
School at the University of California, Berkeley. He can be e-mailed at ks@cmwf.org.
Sara R. Collins, Ph.D., is assistant vice president at The Commonwealth Fund. An economist, she is responsible for
survey development, research, and policy analysis, as well as program development and management of the Fund’s
Program on the Future of Health Insurance. Prior to joining the Fund, Dr. Collins was associate director/senior
research associate at the New York Academy of Medicine, Division of Health and Science Policy. Earlier in her
career, she was an associate editor at U.S. News & World Report, a senior economist at Health Economics Research,
and a senior health policy analyst in the New York City Office of the Public Advocate. She holds an A.B. in eco-
nomics from Washington University and a Ph.D. in economics from George Washington University. She can be
e-mailed at src@cmwf.org.
Karen Davis, Ph.D., is president of The Commonwealth Fund. She is a nationally recognized economist with a
distinguished career in public policy and research. In recognition of her work, Ms. Davis received the 2006
AcademyHealth Distinguished Investigator Award. Before joining the Fund, she served as chairman of the
Department of Health Policy and Management at The Johns Hopkins Bloomberg School of Public Health, where she
also held an appointment as professor of economics. She served as deputy assistant secretary for health policy in
the Department of Health and Human Services from 1977 to 1980, and was the first woman to head a U.S. Public
Health Service agency. A native of Oklahoma, she received her doctoral degree in economics from Rice University,
which recognized her achievements with a Distinguished Alumna Award in 1991. Ms. Davis has published a number of
significant books, monographs, and articles on health and social policy issues, including the landmark books Health
Care Cost Containment; Medicare Policy; National Health Insurance: Benefits, Costs, and Consequences; and
Health and the War on Poverty. She can be e-mailed at kd@cmwf.org.
Editorial support was provided by Christopher Hollander.You can also read