Health Status and Portfolio Choice: Does Feeling Better Affect your Attitude Towards Risk?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Published in Health and Ageing Newsletter No. 26, April 2012
Invited Article II
.....................................................................................................................................................................
Health Status and Portfolio Choice: Does Feeling Better
Affect your Attitude Towards Risk? *
.....................................................................................................................................................................
by Silvia Bressan +, Noemi Pace ++ and Loriana Pelizzon++
1. Introduction
Modern Portfolio Theory (MPT) postulates risk averse investors who choose their investment portfolios
in order to maximise their expected return for a predetermined level of risk. Which optimal portfolio the
investors will choose depends on the shape of their utility function. In recent years the basic
assumptions of MPT have been widely challenged by the behavioural finance approach which has
thrown new interesting insights on investment decision theory. Behavioural finance evaluates risk by
relying mostly on laboratory experiments and survey or questionnaire instruments, and concentrates on
beliefs, attitudes and risk perception in particular circumstances. Among other factors, individual health
status has recently gained attention as a potential determinant of risk perception and, as a
consequence, of stockholding. Recent literature has developed a portfolio choice theory that includes
the presence of “background” risk. It constitutes an uninsurable component of individuals´ income risk
that decreases additional financial risks (Guiso and Paiella, 2001).
Whether bad health status can be regarded as a form of background risk is still an open issue, and
there is no consensus on the fact that health can have an impact on financial risk taking. With this work
we attempt to contribute to the debate by studying the relationship between health status and portfolio
choice.
The literature has surveyed different ways for health to exercise an effect on portfolio choice, though
the general statement is that a negative health shock tends to shift resources to safer types of financial
investment. Some authors (e.g. Heaton and Lucas, 2009; Berkowitz and Qiu, 2006; Atella, Brunetti and
Maestas, 2011) maintain that because of precautionary saving purposes the threat of future medical
expenditures shifts resources from financial investments. In some other works (e.g. Edwards, 2008;
Love and Smith, 2010) health is regarded as a direct argument of the investor utility function and a
health shock is found to raise the marginal utility of consumption. Finally, the interrelation of health with
some other features that affect the life span horizon, such as ageing (Coile and Milligan, 2009) or
bequest motives (Feinstein and Li, 2006), can impact household portfolio choice.
In this study, we use data contained in the first wave of SHARE, the Survey of Health, Ageing and
Retirement in Europe. Its main focus is to paint a picture of the lives of Europeans aged 50 and over,
collecting data in 11 countries from Scandinavia to the Mediterranean. The survey covers 19,548
*
The full version of the article can be obtained from the authors.
+
University of Vienna.
++
Department of Economics, Ca' Foscari University of Venice, Italy.The Geneva Association Health and Ageing Newsletter N° 26 / April 2012
households and 28,517 individuals on a wide range of topics, encompassing health, socioeconomic
status, financial transfers and intensity of social interaction. For our research, particular attention goes
to variables expressive of wealth and health conditions. From these, we manage to construct indicators
for portfolio choice and to relate them to different health proxies. A peculiar feature of our work is that
we always look at health in its different dimensions (objective, subjective and mental), so that we can
identify which particular profile of health is in fact capable of having an impact on portfolio composition.
Moreover, once we have surveyed the decision of holding some stocks in the investment portfolio, we
also look at the weight associated with such securities with respect to other safer assets. Finally, our
analysis attempts to explore different channels of health risk transmission to understand the driving
forces of the relationship between health status and portfolio choice.
2. Measuring Health Status
SHARE devotes a section of the questionnaire on measuring health status. Empirically, health status is
an intrinsically unobservable variable. A formal definition of health status involves unavoidably a
number of facets. It would be hard to provide an explanation of “health conditions” that would point in a
single direction. This suggests that we must explore different variables available in SHARE to take into
account these multiple dimensions. At first approximation, we can divide the information of health status
into “objective” and “subjective”. Regarding the first category, SHARE provides the number of
limitations in activities of daily living (ADL) and the number of chronic diseases. The former includes
difficulty in dressing, walking, bathing, eating, getting in or out of bed, and using the toilet. The latter
includes heart attack, high blood pressure, high blood cholesterol, diabetes, asthma, arthritis,
osteoporosis, Parkinson’s and cancer (chronic). Regarding the second category, SHARE provides
information on self-perceived health status (SPHEU), reported on a 5-point scale (1 = Excellent, 2 =
Very Good, 3 = Good, 4 = Fair, 5 = Poor). The last significant health variable included in SHARE is
mental health. This is measured by a depression scale variable (EUROD), which runs from 0 to 12,
depending on whether or not the individual reported having problems during the previous month with
one or more negative feelings among a list that includes depression, pessimism, guilt, irritability and
tearfulness.
3. Stockownership and Risky Investment
SHARE respondents are asked about the amount of money they have invested in the following financial
products: bank accounts, bonds, stocks, individual retirement accounts, contractual savings for
housing, whole and term life insurance. As in Christelis, Jappelli and Padula (2010), we distinguish
between direct stockownership and total stockownership, which includes stocks held directly plus
stocks held through mutual funds and investment accounts (assuming that whoever holds mutual funds
and retirement accounts has some stocks in them). In addition, we are also interested in providing
some statements on the fraction of the portfolio attributed to such securities. In particular, we define the
“risky” fraction of the investment portfolio as the sum of stocks, mutual funds and individual retirement
accounts over the total gross financial wealth. Thirteen per cent of our sample invests directly in stocks,
while more than the double (26.7 per cent) holds stocks either directly or through mutual funds and
individual retirement accounts.
4. Unconditional Relationship between Stock Market Participation and Health Status
Our purpose is to investigate the relationship between the investment variables we have just described
(namely stockholding and risky investment) with health conditions identified by four variables
(disabilities in ADL, chronic conditions, SPHEU and mental health. To get a first glance on the type of
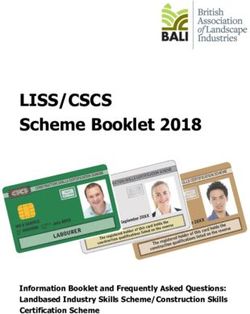
connection, in Figures 1 and 2 we plot stockholding and risky investment (respectively) as functions of
the four proxies of health conditions. In general, the objective health seems to affect negatively both
stockholding and the relative amount of risky investments, though the path is not continuous and some
jumps are observable for a large number of limitations or chronic diseases (see Figures 1a and 1b).
The effect of SPHEU, the self-reported health condition, is easier to see. The dependent variables in
Figure 1c decrease in a monotonic way, suggesting that as soon as the individual reports a worse view
of himself, he tends to leave the equity market and places resources in other different and “safer” forms
of investments. While people reporting excellent health conditions hold 20 per cent of their resources in
risky assets, individuals in poor health reduce this proportion to below 5 per cent. The effect is the same
when we consider the mental health indicator EUROD. Figure 1d shows that the stronger the
depression symptoms, the more investment participation drops.
2The Geneva Association Health and Ageing Newsletter N° 26 / April 2012
Figure 1. Direct and total stock market participation by health conditions
30% 35%
25% 30%
20% 25%
15% 20%
15%
10%
10%
5%
5%
0% 0%
0 1 2 3 4 5 6 0 1 2 3 4 5 6 7 8 9
Number of Limitations in Daily Life Number of Chronic Conditions
Direct Stockholding Total Stockholding Direct Stockholding Total Stockholding
50% 40%
40%
30%
30%
20%
20%
10% 10%
0% 0%
Excellent Very Good Fair Poor 0 1 2 3 4 5 6 7 8 9 10 11
good
Depression Scale (EUROD)
Self-perceived Health Status (SPHEU)
Direct Stockholding Total Stockholding Direct Stockholding Total Stockholding
Note: 1a) number of limitation in ADL, 1b) number of chronic conditions, 1c) SPHEU, 1d) depression scale
(EUROD).
5. Conditional Relationship between Stock Market Participation and Health Status
An unconditional analysis may hide the role of other explanatory variables affecting stockholding. For
this reason, we estimate a regression model for each of our three dependent variables (direct
stockholding, total stockholding, share of risky investment) 1 in which we consider stockholding on the
left-hand side and health status plus a set of control variables on the right-hand side. In particular, we
include the following control variables: age and its square, education level, number of household
components, employment characteristics, indicators of household resources (gross financial income,
real assets and household disposable income), a variable for social activities, a set of indicators for
cognitive abilities, the expectations of leaving an inheritance and country dummies. The four proxies of
health status (number of limitations in ADL, number of chronic conditions, SPHEU and mental health)
are considered separately.
That is, for each dependent variable, the health proxy is changed and the regression is run over again,
according to which health explanatory variable is considered. Moreover, we consider the four health
proxies simultaneously and, to overcome possible multicollinearity issues among health variables, we
replace the original variables with the corresponding set of orthogonal variables, using a modified
Gram-Schmidt procedure (Golub and Van Loan, 1996). This allows us to filter in part the effect of each
proxy over the other.
Before presenting the results, we would like to mention some of the other variables included as control:
Household gross income, gross financial wealth and real assets: in our framework, these key
indicators of well-being and quality of life are particularly relevant, as wealth is a buffer against the
financial risk of investment portfolios, as well as against the health risk that elderly increasingly
face. 2
1
We estimate a probit regression model when we consider direct or total stock holding as dependent variable, and a
tobit model when we consider the percentage of risky investment.
2
The variables are adjusted for the purchasing power parity, using Germany in 2004 as basis.
3The Geneva Association Health and Ageing Newsletter N° 26 / April 2012
Education: we used a scale variable that denotes the highest level of education reported (levels 0-2
pre-primary, primary and lower secondary education, 3 upper secondary education and 4-6 post-
secondary education of the international standard classification of education—ISCED).
Cognitive abilities: these are defined in the neuro-psychological literature as an individual’s capacity
to use brain networks more efficiently. We included areas that seemed more relevant to financial
planning: the ability to perform numerical operations, planning and executive functions, and
memory. 3
Investor’s horizon and bequest motives: our empirical analysis focuses on a sample of aged people
for whom the shortening time horizon plays a key role in driving many of their choices and
behaviours. For this reason we always check for age and squared age, in order to consider possible
non linearities in the relationship between time horizon and the dependent variable. Moreover, since
expectations of future events also matter in portfolio allocation, we included a variable that proxies
the expectation of leaving a bequest.
Social interactions: previous studies have noted that many individuals make economic decisions
based on information received via social interaction. Therefore we included an indicator for social
activities (sport, social club, participation in a political or community-related organisation).
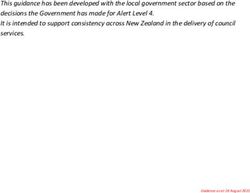
Figure 2. Share of risky investment by health conditions
14% 16%
12% 14%
12%
10%
10%
8%
8%
6% 6%
4% 4%
2% 2%
0% 0%
0 1 2 3 4 5 6 0 1 2 3 4 5 6 7 8 9 10
Number of Limitations in Daily Life Number of Chronic Conditions
Percentage of Risky Investments Percentage of Risky Investments
25% 20%
20%
15%
15%
10% 10%
5% 5%
0%
0%
Excellent Very Good Fair Poor
good 0 1 2 3 4 5 6 7 8 9 10 11
Depression Scale (EUROD)
Self-perceived Health Status (SPHEU)
Percentage of Risky Investments Percentage of Risky Investments
Note: 2a) number of limitation in ADL, 2b) number of chronic conditions, 2c) SPHEU, 2d) depression scale
(EUROD).
The whole set of health variables has negative effect both on stock market participation decision as well
as on the percentage of risk carried by the portfolio. Between the two proxies of objective health status
(ADL and chronic), statistically significant effects are found only for the indicator of chronic diseases
with respect to direct stockholding. The results become highly significant when the health indicator is
allowed to coincide with self-reported health conditions. Results show that SPHEU has a significantly
negative coefficient for all the dependent variables, so that a negative view of personal health status
pushes downwards equity investment and risk taking.
3
The numeracy score is constructed basing on four questions requiring some mental calculations; the indicator
fluency, corresponds to the number of animals that the respondent can list in exactly one minute of time; for the
evaluation of memory has been asked to listen to a list of ten items and then to report after a while the recalled ones.
4The Geneva Association Health and Ageing Newsletter N° 26 / April 2012
6. Disentangling Health Risk Transmission
In this section we try to disentangle the different channels through which health risk may explicate an
effect on investment decision that consists of a disaffection from the equity market and a decrease in
the level of assumed financial risk. As mentioned in Section 1, previous contributions identify three main
channels: precautionary saving motive, pure risk aversion and shortening of the life span. Let us start
with the latter. Bad health is perceived as a factor that shortens the individual time horizon, with the
immediate consequence of setting up safer portfolio choices. In our specifications, we always control for
age and age squared, and the results show that these variables are almost never significant,
suggesting that age per se has no explanatory power on portfolio choice. To support this statement, we
also split the sample into people aged less than 65 and people aged 65+. The negative relationship
between health conditions and stockholding and between health conditions and the fraction of risky
investment still holds. Again, the proxy of subjective health status is always statistically significant at 1
per cent, and the marginal effect for stock market participation is even slightly lower in absolute value
for people aged 65+, evidence that reinforces our idea that the results are not driven by the older
fraction of the population. Moreover, as already noticed, the expectation to leave a bequest can have
effects on the perception of lifespan. For this reason, we also check in our specifications for the bequest
motive, and the negative relation between stockholding and the proxies of health status still holds.
Overall, the results seem to suggest that the shortening of the lifespan is not a channel of health risk
transmission.
There are two other potential channels that need to be explored: the precautionary saving motive and
pure risk aversion. In general, we observe that it is quite difficult to disentangle these two effects.
Nevertheless, in order to test for precautionary saving motive, we have also performed the analysis on
a sub-sample of financial respondents who own private health insurance (under the hypothesis that
people would buy health insurance as a buffer against future expenditures due to health shocks) and
check whether health status still affects investments. 4 Preliminary results (obtained without taking into
account potential endogeneity problems related to the choice of acquiring private health insurance)
show that the negative relationship between health conditions and portfolio choice is confirmed. Even if
individuals insure themselves against health shocks, it seems that this protection is not sufficient to
overcome the suffering of health risk. In the same spirit, we then consider the payment at the household
level of out-of-pocket (OOP) medical expenditures. 5 We concentrate on households that have not faced
any OOP in the previous year, in order to verify whether health risk still weakens financial market
participation, even when there is no need for health care utilisation which can attack household savings.
The results show that (see footnote 5) for the sub-sample of people who do not face any OOP medical
payment the effect of health is still negative and significant for the subjective health indicator.
Summing up, on the basis of this analysis, we can state that precautionary saving and especially the
shortening of the life span are not channels of health risk transmission in our sample. First, we find
evidence that the negative relationship between health status and stockholding holds even controlling
for proxies of the individual time horizon. Secondly, we do not find evidence that buying health
insurance is sufficient for health risk coverage. The interpretation that we favour lies instead in the
direct effect that health shocks have on individual risk aversion. Negative health shocks impact directly
individual attitudes and, in particular, financial risk aversion is altered, namely augmented. Unavoidably,
this leads to a revision of the investment portfolio composition with a larger amount of resources
devoted to lower risk products.
7. Conclusions
Using data from the Survey of Health, Aging and Retirement in Europe, we studied the relationship
between health conditions and portfolio choice. We find that stockownership and the share of risky
assets in the portfolio react always correlate negatively with deteriorating health conditions, even after
controlling for a large set of individual characteristics. One of the major results is that the health variable
that we find to be significantly and consistently negative across specifications is the self-perceived
health status. While the literature has proposed different channels of health risk transmission, a further
econometric investigation suggests that the negative relationship between health conditions and
4
These results are not reported but are available under request.
5
OOP includes non-refunded expenses for inpatient care, outpatient care, prescribed drugs and nursing homes
sustained in the previous 12 months, with monetary values expressed in euro and adjusted by the purchasing power
parity.
5The Geneva Association Health and Ageing Newsletter N° 26 / April 2012
portfolio choice is mainly due to an increase in individual risk aversion, rather than a precautionary
saving intent or the shortening of the lifespan. While our analysis suggests that we can be pretty
confident in rejecting this latest channel, more work needs to be done to explore the precautionary
saving motive. This will be the objective of our future research.
References
Atella, V., Brunetti M. and Maestas, N (2011) “Household Portfolio Choices, Health status and Health Care Systems: A
Cross-Country Analysis Based on SHARE”, Journal of Banking & Finance.
(http://dx.doi.org/10.1016/j.jbankfin.2011.11.025)
Berkowitz M. K. and Qiu, J. (2006) “A further look at household portfolio choice and health status”, Journal of Banking &
Finance, 30, 1201–1217.
Coile, C. and Milligan, K. (2009) “How Household Portfolios Evolve After Retirement: The Effect Of Aging And Health
Shocks”, Review of Income and Wealth, 55(2), 226–248.
Christelis, D., Jappelli, T. and Padula, M. (2010) “Cognitive Abilities and Portfolio Choice”, European Economic Review
54, 18–38.
Edwards, R.D. (2008) “Health Risk and Portfolio Choice”, Journal of Business & Economic Statistics, 26( 4), 472-485.
Feinstein, J. S. and Lin, C. (2006) Elderly Asset Management, SSRN Working Paper 956399.
Golub, G. and Van Loan, C. (1996) Matrix computations, Third edition. London: The Johns Hopkins University Press.
Guiso, L. and Paiella, M. (2008) “Risk Aversion, Wealth, and Background Risk”, Journal of the European Economic
Association, 6(6), 1109-1150.
Heaton, J. and Lucas, D. (2000) “Portfolio Choice in the Presence of Background Risk,” Economic Journal, 110, 1–26.
Love, D.A. and Smith, P.A. (2010) “Does health affect portfolio choice”, Health Economics, Vol. 19, Issue 12: 1441–1460.
Pang G. and Warshawsky, M. J. (2010) “Optimizing the Equity-Bond-Annuity Portfolio in Retirement: The Impact of
Uncertain Health Expenses”, Insurance: Mathematics and Economics, 46(1), 198-209.
This article was published by The Geneva Association (The International Association for the Study of
Insurance Economics). Articles, documents and recent publications of the Association can be found on its
website, at www.genevaassociation.org
6You can also read