Intraoperative assessment of ureter perfusion after revascularization of transplanted kidneys using intravenous indocyanine green fluorescence imaging
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
Intraoperative assessment of ureter perfusion after
revascularization of transplanted kidneys using intravenous
indocyanine green fluorescence imaging
Potchara Kanammit1, Pokket Sirisreetreerux1^, Sarinya Boongird2, Suchin Worawichawong3,
Kittinut Kijvikai1
1
Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Division
of Nephrology, Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Department of
Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Contributions: (I) Conception and design: P Sirisreetreerux, K Kijvikai; (II) Administrative support: S Boongird; (III) Provision of study materials
or patients: P Kanammit; (IV) Collection and assembly of data: P Sirisreetreerux; (V) Data analysis and interpretation: P Sirisreetreerux, S
Worawichawong; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Correspondence to: Pokket Sirisreetreerux. Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol
University, Bangkok 10400, Thailand. Email: pokket.sir@mahidol.edu.
Background: Kidney transplantation is the most valuable renal replacement therapy. One of the most
common urologic complications following kidney transplantation is ureter anastomosis leakage, which leads
to high morbidity along with kidney graft loss. We hypothesized that indocyanine green (ICG) fluorescence
videography can assess ureter perfusion after revascularization of transplanted kidneys.
Methods: We conducted a prospective cross-sectional study in end-stage renal disease patients who
underwent deceased donor kidney transplantation at Ramathibodi Hospital from September 2019 to January
2020. The segments of transplanted ureters were categorized as having good or poor perfusion based
on the percentage from ICG fluorescence videography images. Then the results from ICG fluorescence
videography were compared with histopathology which is considered the gold standard.
Results: Thirty-one sections of dissected ureters were evaluated from 10 patients. Compared with
pathological diagnosis of ureteral ischemia, ICG videography had sensitivity, specificity, positive predictive
value (PPV), negative predictive value (NPV), and positive likelihood ratio of 100%, 92.6%, 66.7%, 100%,
and 14, respectively. Accuracy was 93.6%. The area under the curve of ICG fluorescence videography was
0.96. The average ureter length that maintained good perfusion was 14 cm from the ureteropelvic junction.
Adverse events from ICG were not observed in this study.
Conclusions: We conclude that ICG fluorescence videography is beneficial for detection of early ureteral
ischemia in kidney transplantation patients, with negligible adverse events. However, further studies with
larger numbers of patients are necessary to confirm our results and clinical outcomes regarding complication
rates.
Keywords: Accuracy; fluorescence imaging; indocyanine green (ICG); kidney transplantation; ureter perfusion
Submitted Feb 24, 2021. Accepted for publication Apr 14, 2021.
doi: 10.21037/tau-21-160
View this article at: http://dx.doi.org/10.21037/tau-21-160
^ ORCID: 0000-0002-6900-8356.
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-160
2298 Kanammit et al. Assessment of ureter transplanted perfusion using ICG
Introduction intraoperative quantitative assessment of delayed graft
function during kidney transplantation (14). According to
Chronic kidney disease (CKD) ranks among the most
a previous report, the use of ICG fluorescence videography
common diseases and negatively affects quality of life and
is a valuable adjunctive modality in intraoperative
life expectancy. Based on the registry from Asian-Pacific,
monitoring of free flap surgeries and kidney graft
Australian and New Zealand, Canada, Europe, Japan
function, and appears to be a sensible tool for detecting
and United States, the prevalence of CKD has increased
compromised microcirculation (15). Because of the basic
by 29.3% since 1990 (1,2). KT is the most cost-effective
pharmacokinetic and pharmacodynamic properties of
procedure for renal replacement therapy which was found
tricarbocyanine dye, most ICG is distributed exclusively in
to be performed around 69,400 KTs annually worldwide.
blood vessels. Furthermore, ICG has a short half-life and
Among them, 64% were from deceased donors (3).
is rapidly eliminated without enterohepatic and urinary
Compared with dialysis, KT reduces the risk of death by
circulation (16). Additionally, images can be obtained
over 60%, doubles expected survival time, and greatly
relatively quickly using this process. ICG has also been
improves quality of life (4).
found to induce a low incidence of adverse reactions and is
Urological complications in KT recipients remain
considered safe. However, on the basis of previous studies,
common. Complications such as urine leakage, ureteral
information on using ICG primarily for assessing ureteral
stenosis, lymphocele, lithiasis, urethral stricture, and
viability during KT is limited (17).
vesicoureteral reflux are reported in recipients with
With the aim of preventing complications associated with
incidence of 2.5–30% (5). One of the most common
ureteral necrosis, we hypothesized that ICG fluorescence
urologic complications following KT is ureter anastomosis
videography could accurately assess ureter perfusion
leakage, which leads to high morbidity along with kidney
following vascular anastomosis (11,18). The objective of
graft loss. At Ramathibodi Hospital, the incidence of
this study was to evaluate the accuracy of ICG fluorescence
urinary leakage complications was reported as roughly
imaging in the diagnosis of hypoperfusion of transplanted
4.4% (6). Compromising blood supply to the distal ureter
ureters, while comparing it with pathological evidence of
during organ procurement is the primary risk factor for
ureteral ischemia, which is the gold standard diagnostic
ureteral necrosis and urinary leakage, and can lead to high
method. Because of limited knowledge on the effect of
morbidity and kidney graft loss (7,8). Following vascular
ureteral length on urological complications after KT, our
anastomosis during KT, assessing the quality of the ureter is
secondary objective was to estimate the average ureter
an important step, although it remains difficult to properly
length that maintains good perfusion before performing
evaluate and can be problematic in some patients. Owing
ureteral reimplantation using fluorescence imaging. Finally,
to the anatomical features of the ureter, the branches
we evaluated the safety of ICG in patients with ESRD. We
of its arteries are small and are easily injured because of
present the following article in accordance with the STARD
tearing (9). Currently, no accurate method exists for
reporting checklist (available at http://dx.doi.org/10.21037/
diagnosing vascular compromise of the ureter, necessitating
tau-21-160).
an attempt to identify a method for assessing the ureter
during KT by determining the area of the ureter that
has insufficient blood supply before ureter anastomosis is Methods
performed (7,8,10).
Study population
Indocyanine green (ICG) is widely used for evaluating
function and perfusion after various procedures, such After ethical approval from the Committee on Human
as free flap surgery and assessing burn depth (11). The Rights Related to Research involving Human Subjects,
applicability and potential advantages of ICG fluorescence Faculty of Medicine, Ramathibodi Hospital (No.
during organ transplantation are limited and incompletely MURA2018/405), we conducted a cross-sectional study
understood. In liver and pancreas transplantations, ICG is with all ESRD patients who underwent deceased donor
used to assess graft bile duct perfusion and the perfusion kidney transplantation (DDKT) from September 2019 to
level of the duodenal graft stump for identifying perfusion January 2020. The study was conducted in accordance with
defects that may be transected before anastomosis (12,13). the Declaration of Helsinki (as revised in 2013). Inclusion
Furthermore, fluorescence angiography with ICG allows criteria were male and female ESRD patients aged over
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-160Translational Andrology and Urology, Vol 10, No 6 June 2021 2299
ESRD patients underwent KT
in Ramathibodi Hospital between Jan. 2019 - Dec. 2019
Exclusion criteria
• Allergic to Indocyanine Green
• Allergic to Iodine (sodium iodide in ICG)
• Poor liver function
At IPD
• Withdraw/Deny from participation
Data collection was done. Inform consent was done
0.25 mg/kg ICG Injection
Fluorescence Videography
Good perfusion Hypoperfusion Ischemia
(Green) (Red) (Blue)
Distal ureter was dissected.
Transition zone of each perfusion level was labelled
Wait for the histopathology results in 2 weeks
Dissected for Pathologic diagnosis • Normal
• Ureteral Necrosis
Data analysis of accuracy
Figure 1 Flow chart of the study procedure.
18 years admitted to the hospital for DDKT. We excluded was completed, a single dose of ICG (Diagnogreen ®
patients with history of ICG or iodine allergy, poor liver Injection, Daiichi Sankyo Propharma, Japan) was injected
function, and those who refused to participate in the study. intravenously. The dose of ICG was 0.25 mg/kg body
When the patients were admitted for the DDKT, written weight (13,17), and the maximum dose was 12.5 mg, which
informed consent was obtained from all participants and was decreased from the amount used in ICG videography
patients’ anonymities were preserved. We reviewed the for other indications based on renal function. Fluorescent
database containing information on the patients. Baseline videography (Fluoptic, Fluobeam ® 800 Clinical System,
features and perioperative data including age, sex, cold Parvis Louis Néel, CS 20050 38040 Grenoble Cedex 9, France)
ischemic time, and recipient warm ischemic time were was then used to evaluate ureter perfusion, and was shown
collected. as the spectrum of color along with the percentage of
The study flow diagram is shown in Figure 1. Patients perfusion. Digital photographs and video recordings of the
who met the inclusion criteria underwent DDKT as a area were captured until 5 min after ICG injection. The
standard procedure. Kidney graft was prepared, preserving picture with maximal perfusion, which was defined as the
in Euro-Collins solution and renal vessels and ureter were picture when the perfusion colour persisted, was used for
identified. After that, kidney graft was perfused and vascular the analysis. Quantification of perfusion was then performed
anastomosis was subsequently performed using external on the saved images after completing the operation. The
iliac artery and vein. Ten minutes after vascular anastomosis assessor was blinded from the histopathology result.
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-1602300 Kanammit et al. Assessment of ureter transplanted perfusion using ICG All patients were performed antirefluxing extravesical procedure were presented as percentage or mean ± standard ureteroneocystostomy using Lich-Gregoir technique. The deviation (SD). Sensitivity, specificity, positive predictive ureter was anastomosed to the bladder mucosa using maxon value (PPV), negative predictive value (NPV), positive 4-0. The seromuscular layer was closed over the ureter likelihood ratio (+LR), negative likelihood ratio (−LR), creating the tunnel with chromic 3-0. Foley catheter was and accuracy were analyzed. The test of equality of area placed for 7 days and ureteral stent was placed for 14 days. under the receiver operating characteristic curve was used Perioperative outcomes were recorded, including time to to determine differences in terms of accuracy. Statistical visualize ureter perfusion, and ureter length. Adverse events analyses were performed using Stata version 14, and P
Translational Andrology and Urology, Vol 10, No 6 June 2021 2301
Eligible participants
(no. of patients =10)
ICG Videography
(no. of patients =10)
ICG Videography positive ICG Videography negative
(ureter segments, n=6) (ureter segments, n=25)
Histopathology test as standard test Histopathology test as standard test
(ureter segments, n=6) (ureter segments, n=25)
Final diagnosis Final diagnosis
(ureter segments, n=6) (ureter segments, n=25)
Figure 2 Flow of participants.
Table 1 Demographic data and perioperative outcomes
Parameter Total (n=10)
Sex, n (%)
Male 7 (70%)
Female 3 (30%)
Age (years), mean ± SD 45.80±5.55
Cold ischemic time (min), mean ± SD 1,057.10±239.54
Recipient warm ischemic time (min), mean ± SD 43.20±8.40
Initial ureter length after vascular anastomosis (cm), mean ± SD 16.20±2.25
Cut ureter before reimplantation (cm), mean ± SD 11.15±1.25
Dissected ureter for pathology (cm)*, mean ± SD 5.05±1.86
Time to first visualize ureter perfusion (sec.), mean ± SD 15.0±6.63
Time to visualize high ureter perfusion (sec.), mean ± SD 126.0±54.2
Perfused ureter length at thigh (cm), mean ± SD 12.75±1.49
Time to visualize maximal ureter perfusion (sec.), mean ± SD 187.0±45.71
Perfused ureter length at Tmax (cm), mean ± SD 14.0±2.13
*Dissected ureter for pathology was calculated from the difference in length between the initial ureter length after vascular anastomosis
and the cut ureter before ureteroneocystostomy. SD, standard deviation.
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-1602302 Kanammit et al. Assessment of ureter transplanted perfusion using ICG
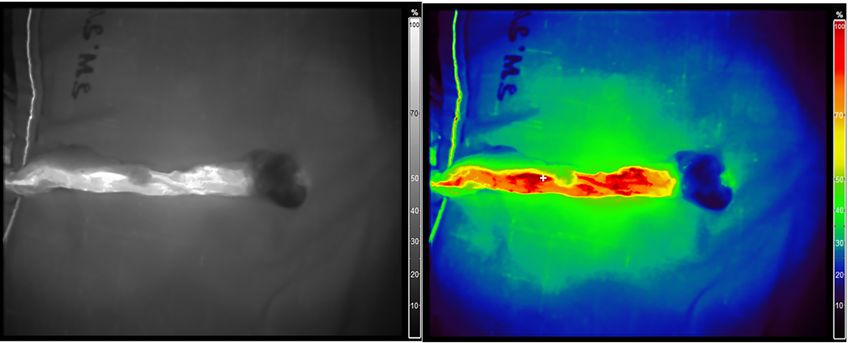
Figure 3 Imaging from paired structures identified in both monochrome (left) and multicolor (right) phases from before ureter anastomosis
in the same patient.
Ureter
Length
(cm)
Ureter perfusion diagram by ICG fluorescence videography
20
18
16
14
12
10
8
6
4
2
0
1 2 3 4 5 6 7 8 9 10 Patient
ID
Red (100%) Yellow (75%) Green(50%) Blue (25%)
Figure 4 Ureter perfusion diagram by indocyanine green fluorescence videography.
Table 2 Sensitivity, specificity, positive predictive values, negative predictive values, and accuracy
ICG Videography
Pathology Total Sensitivity Specificity PPV NPV Accuracy
Positive Negative
Positive 4 0 4 100% 92.6% 66.7% 100% 93%
Negative 2 25 27
Total 6 25 31
imprudent dissection, unskilled suturing, or prolonged absence of technical difficulties during surgery. Transplanted
cold ischemic time. Other factors that may contribute to ureters depend solely on blood supplied by the branches of
development of urological complications after KT are the renal artery that traverse periureteric tissues. This area
graft-related, such as ureteral vascularization and arterial is also known as the golden triangle. Indeed, the importance
multiplicity. Distal ureteral ischemia and necrosis secondary of preserving periureteral connective tissue to prevent
to compromised blood supply are believed to be the main disastrous urinary complications is well documented (5,7-10).
causes of early ureteral complications in most patients in the We believe that gentle manipulation of the ureter and
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-160Translational Andrology and Urology, Vol 10, No 6 June 2021 2303
1.00 Moreover, fluorescence has been extensively employed in
gynecological, endocrinological, and colorectal surgeries
0.75
(29-31). However, the applicability and potential advantages
of using ICG fluorescence during organ transplantation are
Sensitivity
limited and incompletely understood. Fluorescent imaging
0.50
can clearly visualize reconstructed vessels in living donor
liver transplantations, kidney allograft perfusion, and renal
0.25 vasculature after revascularization of transplanted kidneys.
Rother et al., found that fluorescence angiography reflects
0.00
preexisting morphological changes of the renal cortex which
0.00 0.25 0.50 0.75 1.00 may serve as a method for the assessment of microperfusion
1-Specificity
Area under ROC curve =0.9333 of the kidney allograft (32). Siddighi et al. reported that
intraurethral injection of ICG and visualization under near-
Figure 5 Receiver operating characteristic curve for predicting
infrared light allow for real-time delineation of the ureter (33).
early ureteral ischemia using indocyanine green fluorescence
Lee et al. found that intraurethral injection of ICG and
videography.
subsequent visualization under near-infrared fluorescence
facilitates robot-assisted ureteral reconstructions by aiding
in rapid and accurate identification of the ureter and precise
adequate preservation of periureteral tissue, while properly
localization of the proximal and distal ureteral stricture
maintaining the length of the ureter without tension, are
margins (34).
of key importance. A ureter with ischemic appearance
The role of ICG fluorescence videography in
after reperfusion should be resected until a good area of
intraoperative assessment of ureter perfusion after
perfusion is achieved (22-25).
revascularization of a transplanted kidney, still remains
In DDKT, it remains difficult to evaluate whether
questionable. Vignolini et al. reported the first preliminary
transplanted ureters are sufficiently perfused. In
experience with intraoperative ICG fluorescence
current practice, assessment of ureter viability depends
videography for assessing graft and ureteral reperfusion
on visualization by the surgeon, which is a subjective
during robot-assisted KT, and concluded that ICG provides
measurement and requires the surgeon to have sufficient
a reliable assessment of graft reperfusion. However, larger
experience. Furthermore, renal transplantation after
studies are required to standardize the technique (35).
ex vivo normothermic perfusion (EVNP) (26) was recently
Herein, we present our initial experience with ICG
introduced in clinical practice using an EVNP circuit
fluorescence videography for evaluating ureter perfusion
designed to deliver an oxygenated, warmed, red cell-based during DDKT.
perfusate to the kidney. Creating a clear line of demarcation Our results showed that ICG fluorescence videography
between a well-vascularized renal pelvis and proximal ureter allows for high sensitivity and specificity in differentiating
and a distal ureter that appears to completely lack a blood between normoperfused and hypoperfused segments of
supply, allows the ureter to be marked and transected at a transplanted ureters. Compared with histopathology, the
point where the blood supply is deemed optimal. It should gold standard diagnostic method, the accuracy of ICG was
be noted that EVNP provides additional information over 90%.
on the adequacy of the ureteral blood supply before One patient in our cohort exhibited a large perfusion
revascularization in the recipient (27). However, EVNP has deficit in the kidney graft after initial positioning in the
long been costly and limited availability. iliac fossa. After reperfusion, the graft was suspected of
ICG is a molecule with mass of 776 Daltons that was homogeneous impaired perfusion. However, this patient
approved for clinical use in 1959 by the Food and Drug experienced vascular thrombosis that ultimately led to graft
Administration. It has been used in medicine since the late loss and was required to undergo nephrectomy within the
1950s to assess liver function before major liver resections subsequent 3 weeks. There were no complications with
in cirrhotic patients (28). The applicability of fluorescence ICG injection or the video-imaging device. No adverse
in the diagnosis of hepatic tumors such as hepatocellular events from ICG were observed in our study. However, the
carcinomas was initially described in a report from Japan. safety of ICG cannot be concluded because our study had a
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-1602304 Kanammit et al. Assessment of ureter transplanted perfusion using ICG
small number of patients. Larger study with adverse event Footnote
assessment will be required.
Reporting Checklist: The authors have completed the STARD
The strength of our study was that all participants
reporting checklist. Available at http://dx.doi.org/10.21037/
underwent both the index test and pathological examination
tau-21-160
of ureters, which is considered the gold standard for
diagnosis. These examinations eliminate verification bias.
Peer Review File: Available at http://dx.doi.org/10.21037/
However, our study also had limitations. First, the number
tau-21-160
of participants was small and our study can be considered
a pilot study. Larger studies are required to standardize
Data Sharing Statement: Available at http://dx.doi.
the technique and to evaluate the association between
org/10.21037/tau-21-160
perioperative parameters and acute ureteral ischemia.
Second, we measured ureteral ischemia, which is considered
a surrogate outcome rather than a clinical outcome of Conflicts of Interest: All authors have completed the ICMJE
ureteral necrosis or anastomosis leakage. Further studies uniform disclosure form (available at http://dx.doi.
evaluating clinical outcomes are therefore warranted. org/10.21037/tau-21-160). The authors have no conflicts of
Finally, regarding technical issues, the psychomotor skills interest to declare.
of users, including the distance and angle from camera to
targeted ureter, may affect the interpretation of results. Ethical Statement: The authors are accountable for all
Interobserver variation should also be further validated. aspects of the work in ensuring that questions related
In our study, ICG fluorescence videography provided to the accuracy or integrity of any part of the work are
reliable and relevant additional information to surgeons appropriately investigated and resolved. The study was
for guiding intraoperative decisions in DDKT without conducted in accordance with the Declaration of Helsinki (as
adverse events, and should be used as an adjunct to clinical revised in 2013). The study was approved by the Committee
assessments in cases with ureters with an indeterminate on Human Rights Related to Research involving Human
state of perfusion. Subjects, Faculty of Medicine, Ramathibodi Hospital (No.
MURA2018/405). Informed consent was taken from all
individual participants and patients’ anonymities were
Conclusions preserved.
ICG fluorescence videography is beneficial for the detection
of early ureteral ischemia in DDKT patients with negligible Open Access Statement: This is an Open Access article
complications because it is minimally invasive and displays distributed in accordance with the Creative Commons
high accuracy. However, further studies with larger Attribution-NonCommercial-NoDerivs 4.0 International
numbers of patients and follow-up for clinical outcomes are License (CC BY-NC-ND 4.0), which permits the non-
necessary to further validate our results. commercial replication and distribution of the article with
the strict proviso that no changes or edits are made and the
original work is properly cited (including links to both the
Acknowledgments
formal publication through the relevant DOI and the license).
The authors thank The Ramathibodi Excellence Center See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
for Organ Transplantation, The Division of Plastic and
Maxillofacial Surgery, Department of Surgery, Ramathibodi
References
Hospital, Mahidol University, Bangkok, Thailand. The
authors would like to express sincere gratitude for major 1. Cockwell P, Fisher LA. The global burden of chronic
assistance with statistical analysis and valuable advice from kidney disease. Lancet 2020;395:662-4.
Ms. Suraida Aeesoa. We thank Richard Robins, PhD, from 2. Schena FP. Epidemiology of end-stage renal disease:
Edanz Group (https://en-author-services.edanz.com/ac) for International comparisons of renal replacement therapy.
editing a draft of this manuscript. Kidney Int 2000;57:S39-S45.
Funding: This research project was supported by the Faculty 3. Transplantation. GOoDa. World Health Organization
of Medicine, Ramathibodi Hospital, Mahidol University. collaborating centre on Donation and Transplantation:
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-160Translational Andrology and Urology, Vol 10, No 6 June 2021 2305
Centers for Disease Control and Prevention. 2020. green: observations on its physical properties, plasma decay,
Available online: http://www.transplant-observatory.org and hepatic extraction. J Clin Invest 1960;39:592-600.
4. Purnell TS, Auguste P, Crews DC, et al. Comparison 17. Hoffmann C, Compton F, Schafer JH, et al. Intraoperative
of life participation activities among adults treated assessment of kidney allograft perfusion by laser-assisted
by hemodialysis, peritoneal dialysis, and kidney indocyanine green fluorescence videography. Transplant
transplantation: a systematic review. Am J Kidney Dis Proc 2010;42:1526-30.
2013;62:953-73. 18. Sawada T, Solly M, Kita J, et al. An alternative tool
5. Slagt IK, Ijzermans JN, Visser LJ, et al. Independent risk for intraoperative assessment of renal vasculature after
factors for urological complications after deceased donor revascularization of a transplanted kidney. Am J Surg
kidney transplantation. PLoS One 2014;9:e91211. 2010;199:e69-71.
6. Jenjitranant P, Tansakul P, Sirisreetreerux P, et al. 19. Speich R, Saesseli B, Hoffmann U, et al. Anaphylactoid
Risk Factors for Anastomosis Leakage After Kidney reactions after indocyanine-green administration. Ann
Transplantation. Res Rep Urol 2020;12:509-16. Intern Med 1988;109:345-6.
7. Cullmann HJ, Prosinger M. Necrosis of the allograft 20. Benya R, Quintana J, Brundage B. Adverse reactions
ureter--evaluation of different examination methods in to indocyanine green: a case report and a review of the
early diagnosis. Urol Int 1990;45:164-9. literature. Cathet Cardiovasc Diagn 1989;17:231-3.
8. Sinha M, Lewis MA, Riad H, et al. Complete necrosis 21. Moyer HR, Losken A. Predicting mastectomy skin flap
of allograft ureter after cadaveric renal transplantation. necrosis with indocyanine green angiography: the gray
Pediatr Transplant 2004;8:91-3. area defined. Plast Reconstr Surg 2012;129:1043-8.
9. Elkoushy MA, Andonian S. Campbell-Walsh Urology: 22. Buttigieg J, Agius-Anastasi A, Sharma A, et al. Early
Surgical, Radiographic, and Endoscopic Anatomy of the urological complications after kidney transplantation: An
Kidney and Ureter. Campbell-Walsh Urology: Surgical, overview. World J Transplant 2018;8:142-9.
Radiographic, and Endoscopic Anatomy of the Kidney and 23. Buresley S, Samhan M, Moniri S, et al. Postrenal
Ureter, 2015:967-77. transplantation urologic complications. Transplant Proc
10. Fjeldborg O, Kim CH. Ureteral complications in human 2008;40:2345-6.
renal transplantation. An analysis of 180 cases. Urol Int 24. Samhan M, Al-Mousawi M, Hayati H, et al. Urologic
1972;27:417-31. complications after renal transplantation. Transplant Proc
11. Alander JT, Kaartinen I, Laakso A, et al. A review of 2005;37:3075-6.
indocyanine green fluorescent imaging in surgery. Int J 25. Ooms LS, Slagt IK, Dor FJ, et al. Ureteral length in live
Biomed Imaging 2012;2012:940585. donor kidney transplantation; Does size matter? Transpl
12. Panaro F, Benedetti E, Pineton de Chambrun G, et al. Int 2015;28:1326-31.
Indocyanine green fluorescence angiography during 26. Marshall MV, Rasmussen JC, Tan IC, et al. Near-Infrared
liver and pancreas transplantation: a tool to integrate Fluorescence Imaging in Humans with Indocyanine
perfusion statement's evaluation. Hepatobiliary Surg Nutr Green: A Review and Update. Open Surg Oncol J
2018;7:161-6. 2010;2:12-25.
13. Sekijima M, Tojimbara T, Sato S, et al. An intraoperative 27. Nicholson M, Hosgood S. Preoperative Assessment of
fluorescent imaging system in organ transplantation. Renal Transplant Ureteric Blood Supply Using Ex Vivo
Transplant Proc 2004;36:2188-90. Normothermic Perfusion. Transplantation 2015;99:e166.
14. Gerken ALH, Nowak K, Meyer A, et al. Quantitative 28. De Gasperi A, Mazza E, Prosperi M. Indocyanine green
Assessment of Intraoperative Laser Fluorescence kinetics to assess liver function: Ready for a clinical
Angiography with Indocyanine Green Predicts Early dynamic assessment in major liver surgery? World J
Graft Function after Kidney Transplantation. Ann Hepatol 2016;8:355-67.
Surg 2020. [Epub ahead of print]. doi: 10.1097/ 29. Boni L, David G, Mangano A, et al. Clinical applications
SLA.0000000000004529. of indocyanine green (ICG) enhanced fluorescence in
15. Holm C, Tegeler J, Mayr M, et al. Monitoring free flaps laparoscopic surgery. Surg Endosc 2015;29:2046-55.
using laser-induced fluorescence of indocyanine green: a 30. Diana M, Noll E, Diemunsch P, et al. Enhanced-reality
preliminary experience. Microsurgery 2002;22:278-87. video fluorescence: a real-time assessment of intestinal
16. Cherrick GR, Stein SW, Leevy CM, et al. Indocyanine viability. Ann Surg 2014;259:700-7.
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-1602306 Kanammit et al. Assessment of ureter transplanted perfusion using ICG
31. Kudo H, Ishizawa T, Tani K, et al. Visualization of intraoperative localization of ureter. Am J Obstet Gynecol
subcapsular hepatic malignancy by indocyanine-green 2014;211:436.e1-2.
fluorescence imaging during laparoscopic hepatectomy. 34. Lee Z, Moore B, Giusto L, et al. Use of indocyanine green
Surg Endosc 2014;28:2504-8. during robot-assisted ureteral reconstructions. Eur Urol
32. Rother U, Amann K, Adler W, et al. Quantitative 2015;67:291-8.
assessment of microperfusion by indocyanine green 35. Vignolini G, Sessa F, Greco I, et al. Intraoperative
angiography in kidney transplantation resembles assessment of ureteral and graft reperfusion during robotic
chronic morphological changes in kidney specimens. kidney transplantation with indocyanine green fluorescence
Microcirculation 2019;26:e12529. videography. Minerva Urol Nefrol 2019;71:79-84.
33. Siddighi S, Yune JJ, Hardesty J. Indocyanine green for
Cite this article as: Kanammit P, Sirisreetreerux P, Boongird
S, Worawichawong S, Kijvikai K. Intraoperative assessment of
ureter perfusion after revascularization of transplanted kidneys
using intravenous indocyanine green fluorescence imaging.
Transl Androl Urol 2021;10(6):2297-2306. doi: 10.21037/tau-21-
160
© Translational Andrology and Urology. All rights reserved. Transl Androl Urol 2021;10(6):2297-2306 | http://dx.doi.org/10.21037/tau-21-160You can also read

















































