Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Focus | Professional
Implications of new clinical
practice guidance on familial
hypercholesterolaemia
for Australian general
practitioners
Tom Brett, Jan Radford, Clare Heal, RECENT CONSENSUS ADVICE on integrated guidance to enhance the
Charlotte Mary Hespe, Jacquie Garton-Smith, care of patients with familial hypercholesterolaemia (FH) in Australia
Andrew Kirke, Dick C Chan, Jing Pang, Gerald F Watts provides a timely reminder and opportunity for general practitioners
(GPs) to increase their awareness and skill in diagnosing and managing
Background
the condition.1
Familial hypercholesterolaemia (FH) is a monogenic lipid With 88% of Australians presenting to their GPs annually,2 GPs are
disorder that may be overlooked in the diagnostic process. well placed to play a more active part. Currently, fewer than 10% of
Australia’s 100,000 patients with FH are diagnosed, with most failing
Objective
to achieve optimum management and therapeutic targets.3
The aim of this article is to review the key areas for
identification and management of FH that affect The hereditary nature of FH, with its high cholesterol burden present
Australian general practitioners (GPs). from birth,3 causes premature atherosclerotic cardiovascular disease
(ASCVD), principally coronary artery disease (CAD), and death if left
Discussion
untreated.4,5 FH is caused by a defect in the low-density lipoprotein
Recent consensus advice on the care of patients with FH
(LDL) receptor pathway, and it affects one in 250-300 Australians.6,7
in Australia provides an opportunity for GPs to increase
their awareness and skills in diagnosing and managing Among first-degree relatives, 50% are affected because of its
FH. New Medicare Benefits Schedule items for genetic autosomal dominant, monogenic inheritance and high penetrance.3
testing and Pharmaceutical Benefits Scheme listing for General practice is central to the continuity of care and advocacy for
the use of proprotein convertase subtilisin/kexin 9 all patients with FH and their families. This involves a role in screening,
(PCSK9) inhibitors offer GPs additional supports to diagnosis, shared care with specialists, overseeing cholesterol-lowering
improve the care of patients with FH. A shared-care
medications and multimorbidities, as well as applying context-specific
approach between GPs and non-GP specialists with
expertise in multiple disciplines offers the best option to
models of care for FH.1,8
facilitate genetic testing and management of index cases This article focuses on key recommendations for the identification
and affected family relatives. Implementation of this and management of heterozygous FH derived from the recently
guidance in the primary care setting remains an ongoing published integrated guidance,1 with particular reference to GPs.
challenge and needs to be embraced as a high priority. The aim of this article is to help translate this updated guidance into
everyday health policy and practice, and facilitate the provision of
high-quality healthcare for patients with FH and their families in the
primary care setting.
New genetic tests and impact on clinical care
The Australian Government has introduced new pathology services
to assist with detection of heritable mutations predisposing to FH:
616 Reprinted from AJGP Vol. 50, No. 9, September 2021 © The Royal Australian College of General Practitioners 2021Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners Focus | Professional
Medicare Benefits Schedule (MBS) Item publications, awareness about FH in the can improve risk re-stratification and
73352 for index cases and Item 73353 general community and among many optimise treatment.3
for cascade testing of close relatives.9 health professionals remains suboptimal.3
Item 73352 requires non-GP specialist The concept of increased cholesterol Electronic health record screening
authorisation, but Item 73353 can be burden from birth in affected individuals FH meets all the criteria for worthwhile
requested by the patient’s GP. is not well understood. In addition, the disease screening.8 Various approaches
These new tests provide diagnostic hereditary ‘familial’ component of FH, with have been suggested – including universal,
precision, offering GPs added incentive its associated premature ASCVD, tends to opportunistic and selective screening –
to increase diagnosis in the young when remain unrecognised and untreated.3 but all require effective coordination for
treatment can be most effective.4,9 The Young people have most to gain maximum benefit.8,10
level of evidence is high, and the class from early diagnosis and appropriate Reverse child–parent screening,18
of recommendation is strong for using treatment.4,15,16 Apart from lifestyle targeting premature myocardial infarcts
genetic testing to confirm the diagnosis. interventions, most patients will need in coronary care units and screening
This is especially important when cascade lifelong cholesterol-lowering medications, electronic health records (EHRs) in general
testing is planned.1,10,11 especially statins. Ezetimibe and proprotein practice all offer promise.8,19,20 Laboratory
Since more than 20% of probable convertase subtilisin/kexin 9 (PCSK9) report alerts also help with index case
or definite FH may not have a inhibitors may be needed for cases that are detection.1,8,20
detectable mutation,11 FH should not more difficult to control.3,4,17
be totally excluded if a pathogenic, or Failure to diagnose FH before middle Purposeful clinical examination
likely pathogenic, gene variant is not age results in up to 50% of untreated Once FH diagnosis is considered,
detected.1,4,12 men developing myocardial infarction or clinical examination should focus on
A shared-care approach between GP angina by the age of 50 years, and 30% physical stigmata including premature
and non-GP specialists (ie lipidologist, of untreated women similarly affected by corneal arcus and tendon xanthomata.3
cardiologist, pediatrician)13 can facilitate the age of 60 years.5 Early recognition and Periorbital xanthelasmata are suggestive of
genetic testing of index cases. Pre- and treatment produces significant reductions hypercholesterolaemia, and their presence
post-test counselling should be an integral in cardiac morbidity and mortality.15,16 Strict should alert the GP to the potential of
part of the process.1 Once an index case is adherence to treatment allows affected underlying FH. Additional training for
genetically proven, GPs can offer cascade individuals to live a normal lifespan.3 GPs in pattern recognition and early
testing among first- and second-degree consideration of FH among close family
relatives, arrange appropriate counselling History-taking members could help increase awareness of
and collaborate with non-GP specialists The importance of effective history- key hereditary features.
in risk stratification and treatment.8,12 taking in clinical medicine is one of The DLCNC score combines personal
As discussed later, screening requires the fundamental tenets of diagnostic and family history of premature CAD,1,3,8
appropriate GP education, screening tools evaluation. However, poor-quality medical elevated LDL-C levels and physical
and skill training in the care of patients information in practice records may affect stigmata to establish phenotypic FH
with FH. the diagnosis. GPs will often be aware diagnosis in high-risk patients. In a
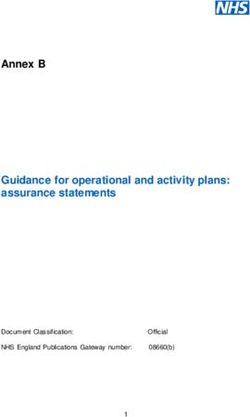
Figure 1 summarises genetic screening of patients and families with a history of genetic analysis of FH in Australia, 70% of
and management of an individual at high premature coronary events attending their patients with a definite FH diagnosis were
risk of FH. practice. Linking such histories, combined found to have an FH-causing mutation,
Risk notification of family members with a lipid profile showing total cholesterol but only 29% of patients with probable FH
requires special skills to overcome >7.5 mmol/L or LDL cholesterol (LDL-C) and 11% of patients with possible FH were
potential barriers, such as privacy laws, >5.0 mmol/L, should alert the GP to the mutation positive.21
poor communication in families, poor possibility of FH. Potential secondary
health literacy, geographical location and causes of hypercholesterolaemia (diabetes,
psychological issues.8,11 Coordination hypothyroidism, steroid use, renal and liver Diagnosis in children and
of the overall process remains a disease) should be excluded before FH is adolescents
significant challenge, especially from further assessed.3 The cumulative LDL-C burden in patients
current inadequate general practice Personal or family history of premature with FH starts from birth and progressively
infrastructure.1,8,14 CAD and markedly elevated cholesterol increases over their lifetimes.4 However,
levels, both central to the Dutch Lipid most children with FH are asymptomatic
Clinic Network Criteria (DLCNC) score, and have no clinical signs. Hence, the
Diagnosis in adults are the chief drivers for establishing a current largest gap is the early detection of
Awareness of FH among Australian GPs phenotypic FH diagnosis. Assessment children with FH.3
Despite the high prevalence of FH and of non-cholesterol risk factors, genetic Early detection is an important
an ever-increasing number of research testing and cardiovascular imaging component of providing optimum
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 9, September 2021 617Focus | Professional Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners
General practice clinics
Patient clinically reviewed
and scored according to DLCNC
Identification of high risk of FH
• DLCNC score
• LDL-C ≥6.5 mmol/L in the absence of secondary causes
• LDL-C 5.0–6.6 mmol/L with signs of premature or accelerated atherogenesis
GP standard GP referral to a specialist to GP arrangement of
care for Mutation request FH genetic testing Mutation genetic testing for
phenotypic FH negative MBS Item 73352 positive first- or second-degree
Care plans (if not previously tested) family members†
721/723 MBS Item 73353
(if not previously tested)
Mutation
positive
Mutation
positive
Management of FH*
Care plans 721/723
Low complexity Intermediate complexity High complexity
• Absence of CVD • Stable CVD and risk factors • Numerous uncontrolled CVD risk
• Absence of risk factors for CVD • Close to LDL-C goal with statin factors
• Reached LDL-C goal with a statin • Low-grade statin intolerance • Symptomatic CVD
• HeFH aged 18 years or HoFH
• Help with cascade screening
Primary care Shared care Tertiary care
Figure 1. Process for genetic screening and management of an individual at high risk of familial hypercholesterolaemia
*Refer to Sturm AC, Knowles JW, Gidding SS, et al, Clinical genetic testing for familial hypercholesterolemia: JACC Scientific Expert Panel, J Am Coll
Cardiol 2018;72(6):662–80. doi: 10.1016/j.jacc.2018.05.044.
†Genetic cascade testing may be undertaken by a general practitioner with skills in the care of patients and families with FH, under the guidance of an
appropriate specialist. Consent is obtained from the index case to contact family. The process of risk notification of family members should be consistent
with relevant local legislation and institutional guidelines. Risk notification may be indirect (providing a family letter for the notifier to pass to relatives) or
direct (clinical service writes to relatives); pre-and post-test genetic counselling should be offered to all at-risk family members.1
CVD, cardiovascular disease; DLCNC, Dutch Lipid Network Criteria; FH, familial hypercholesterolaemia; GP, general practitioner; HeFH, heterozygous
familial hypercholesterolaemia; HoHF, homozygous familial hypercholesterolaemia; LDL-C, low-density lipoprotein cholesterol; PCSK9, proprotein
convertase subtilisin/kexin 9
618 Reprinted from AJGP Vol. 50, No. 9, September 2021 © The Royal Australian College of General Practitioners 2021Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners Focus | Professional
management, most likely statins, from specialist.28 Follow-up consultations therapy adherence are essential for
the age of 8–10 years.1 Use of statins can be managed in primary care for enhancing care.1,8 If uncertainty exists and
in children will need parental consent patients with low-complexity FH. Greater GPs feel reluctant to initiate or continue
with adequate explanation of its benefit awareness by Australian GPs would help statin treatment, support from a paediatric
and possible side effects. The benefits optimise shared-care responsibility with specialist with expertise in lipidology
outweigh any risks for most children. specialists in multiple disciplines for should be sought.1,3
The LDL-C level drives the phenotypic patients at greatest risk.8 Box 1 summarises recommendations
diagnosis, but genetic cascade testing FH treatment from childhood is and therapeutic targets, based on
offers the definitive diagnosis.4,11 Risk supported by good-quality observational moderate levels of evidence and class
stratification helps to facilitate more studies.4,8 Modest, sustained reductions of recommendation, for managing
rational and precise treatment.8 in LDL-C starting early in life can have FH.1,24,26,29,30
The DLCNC score is not suitable for a major effect in preventing future
use in children and adolescents.3 Children premature mortality due to ASCVD.4,8,10,18 Pregnancy
with an LDL-C ≥5 mmol/L have a high A healthy lifestyle, while important, does Statins and other systemically absorbed
risk of FH; for children with premature not sufficiently lower LDL-C. cholesterol-lowering medications should
CAD in close relatives and/or baseline A low-potency statin, with or without be ceased three months before planned
high cholesterol in one parent, an LDL-C ezetimibe, may be required from the age conception as well as during pregnancy
≥4 mmol/L is indicative of high FH risk.4 of 10 years.4,8,10,15,29,30 LDL-C targets do and while breastfeeding.1 All women
The current guidelines do not not need to be as low as for adults,8,16 but of childbearing age with FH should
recommend specific cut-off LDL-C levels for medication safety should be continually be offered pre-pregnancy counselling
parental hypercholesterolaemia.1,4 The value monitored.4,8 prior to starting treatment with statins.
of non-invasive cardiovascular imaging Family-based clinics with paediatric Appropriate contraceptive advice that is
tools, such as the carotid intima-media specialist involvement that address reinforced at least annually helps minimise
thickness test to improve the early diagnosis
of FH in children, needs further evaluation.
Box 1. Low-density lipoprotein cholesterol treatment targets and recommendations for
the management of familial hypercholesterolaemia
Management
Adults Adults
• Commencement of statin treatment should be considered once a diagnosis of FH
There is compelling evidence from
is confirmed.1
extensive clinical trial, registry and
• LDL-C targets can be divided as follows:
genetic data for patients with FH to be
– LDL-CFocus | Professional Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners
cardiovascular risk. GPs should always • GPs are ideally placed to play a GFW reports research grants and personal fees from
Arrowhead, Amgen, Sanofi, and Regeneron, and
seek specialist support for patients with FH proactive part in diagnosing FH and grants from Novartis and advisory board personal
who are considering pregnancy.3 then co-managing these patients in fees from Kowa and AstraZeneca, outside the
submitted work.
The importance of early diagnosis and conjunction with other specialists.
Provenance and peer review: Not commissioned,
treatment of FH in girls should never be • New MBS and PBS items enable more externally peer reviewed.
underestimated.31 Pregnancy and lactation precise diagnosis and treatment of FH. Correspondence to:
can result in the loss of effective years of tom.brett@nd.edu.au
statin treatment due to childbearing.31
Authors References
Adherence to statin treatment can be
1. Watts GF, Sullivan DR, Hare DL, et al. Integrated
Tom Brett MA, MD, FRACGP, MRCGP, Professor and
difficult, especially in young people. The guidance for enhancing the care of familial
Director, General Practice and Primary Health Care
need for early and ongoing treatment hypercholesterolaemia in Australia. Heart
Research, School of Medicine, University of Notre
Lung Circ 2021;30(3):324–49. doi: 10.1016/j.
at optimal doses should be stressed to Dame, Fremantle, WA; General Practitioner, Mosman
hlc.2020.09.943.
Park Medical Centre, Mosman Park, WA
improve future ASCVD outcomes.31 The 2. The Royal Australian College of General
Jan Radford MBBS, MPsychMed, MEd, FRACGP,
cost-effectiveness of such an approach is Practitioners. General practice: Health of the
FARGP, GAID, AFANZAHPE, Associate Professor
nation 2018. East Melbourne, Vic: RACGP, 2018.
increasingly recognised.32 of General Practice, Launceston Clinical School,
Available at www.racgp.org.au/download/
Tasmanian School of Medicine, University of
Documents/Publications/Health-of-the-Nation-
Tasmania, Launceston, Tas; General Practitioner,
2018-Report.pdf [Accessed 10 December 2020].
West Tamar Health, Riverside, Tas; Provost, The
Royal Australian College of General Practitioners 3. Pang J, Sullivan DR, Brett T, Kostner KM, Hare DL,
Conclusion Tasmanian Faculty, Hobart, Tas Watts GF. Familial hypercholesterolaemia in
This guidance is aligned with a recent Clare Heal MBChB, DRANZCOG, DipGUMed, 2020: A leading tier 1 genomic application. Heart
Lung Circ 2020;29(4):619–33. doi: 10.1016/j.
international global call to action on FH.33 FRACGP, MPHTM, PhD, Promotional Chair, Discipline
hlc.2019.12.002.
of General Practice and Rural Medicine, Mackay
The recommendations are designed to Clinical School, James Cook University College of 4. Wiegman A, Gidding SS, Watts GF, et al.
be incorporated into healthcare pathways Medicine and Dentistry, Mackay, Qld Familial hypercholesterolaemia in children
and adolescents: Gaining decades of life by
that meet the needs of the Australian Charlotte Mary Hespe FRACGP, MBBS (Hons), DCH
optimizing detection and treatment. Eur Heart
(Lon), Associate Professor and Head of General
population.3,8 Several efforts have been Practice and Primary Care Research, School of J 2015;36(36):2425–37. doi: 10.1093/eurheartj/
ehv157.
made to improve care of patients with FH Medicine Sydney, University of Notre Dame, Sydney,
NSW; General Practitioner, Glebe Family Medical 5. Marks D, Thorogood M, Neil HA, Humphries SE.
in primary care. These include increased Practice, Glebe, NSW A review on the diagnosis, natural history, and
recognition of phenotypic diagnosis of Jacquie Garton-Smith MBBS, FRACGP, Clinical treatment of familial hypercholesterolaemia.
Atherosclerosis 2003;168(1):1–14. doi: 10.1016/
FH, greater consideration of screening in Co-Lead, Cardiovascular Health Network, Western
Australian Department of Health, East Perth, WA; s0021-9150(02)00330-1.
children, increased awareness of the need Clinical Services, Royal Perth Hospital, Perth, WA 6. Watts GF, Shaw JE, Pang J, Magliano DJ,
to employ implementation science and Andrew Kirke MBBS, FRACGP, FACRRM, Head, Jennings GL, Carrington MJ. Prevalence and
treatment of familial hypercholesterolaemia
practice to optimise health service delivery, Rural Clinical School of Western Australia, University
of Western Australia, West Busselton, WA in Australian communities. Int J Cardiol
and advocacy groups. The introduction 2015;185:69–71. doi: 10.1016/j.ijcard.2015.03.027.
Dick C Chan BSc, MPhil, PhD, FRCPath, Senior
of MBS items for genetic testing and Research Fellow, School of Medicine, Faculty of 7. Pang J, Martin AC, Mori TA, Beilin LJ, Watts GF.
Prevalence of familial hypercholesterolemia
PBS-supported use of PCSK9 inhibitors Health and Medical Sciences, University of Western
Australia, Crawley, WA; General Practice and Primary in adolescents: Potential value of universal
is likely to improve considerably the care Health Care Research Unit, School of Medicine, screening? J Pediatr 2016;170:315–16.
of patients with FH in the future.9,12,28 University of Notre Dame, Fremantle, WA doi: 10.1016/j.jpeds.2015.11.019.
8. Watts GF, Gidding SS, Mata P, et al. Familial
Education and skill training for GPs, such Jing Pang BSc, PhD, National Health and Medical
Research Council Early Career Fellow, School of hypercholesterolaemia: Evolving knowledge
as cascade screening, risk notification, and Medicine, Faculty of Health and Medical Sciences, for designing adaptive models of care. Nat Rev
pre- and post-test genetic counselling, are University of Western Australia, Crawley, WA Cardiol 2020;17(6):360–77. doi: 10.1038/s41569-
019-0325-8.
paramount for implementing effective care Gerald F Watts DSc, PhD, MD, FRACP, FRCP,
Winthrop Professor and Consultant Physician, 9. Australian Government Department of Health.
in general practice. School of Medicine, Faculty of Health and Medical Medicare Benefits Schedule 2020 – Item
The challenge we now face is how to Sciences, University of Western Australia, Crawley, 73352. Canberra, ACT: MBS Online, 2020.
WA; Lipid Disorders Clinic, Cardiometabolic Service, Available at www9.health.gov.au/mbs/
implement this guidance into health policy fullDisplay.cfm?type=item&q=73352&qt=ItemID
Departments of Cardiology and Internal Medicine,
and high-quality care. Implementation Royal Perth Hospital, Perth, WA [Accessed 10 December 2020].
research and practice will need to be Competing interests: TB reports that Amgen 10. Gidding SS, Champagne MA, de Ferranti SD, et al.
supported travel and accommodation costs for The agenda for familial hypercholesterolemia:
embraced as a high priority to increase the A scientific statement from the American Heart
attendance at FH Summit in Melbourne (February
impact of this guidance on improving the 2019), and provided honorarium for FH meeting in Association. Circulation 2015;132(22):2167–92.
Dublin (September 2018). JGS reports employment doi: 10.1161/CIR.0000000000000297.
care of all Australians who have, or are at
with WA Primary Health Alliance. JR reports that 11. Sturm AC, Knowles JW, Gidding SS, et al. Clinical
risk of, FH.33 Amgen supported travel and accommodation genetic testing for familial hypercholesterolemia:
costs for attendance at FH Summit in Melbourne JACC Scientific Expert Panel. J Am Coll
(February 2019). Cardiol 2018;72(6):662–80. doi: 10.1016/j.
Funding: The authors acknowledge current National jacc.2018.05.044.
Key points Health Medical Research Council (NHMRC) 12. Hooper AJ, Burnett JR, Bell DA, Watts GF. The
• Recent guidelines support improved Partnership Grant Funding (GNT11428830). TB, present and the future of genetic testing in familial
CMH, CH and JGS report grant funding from hypercholesterolemia: Opportunities and caveats.
care of patients with FH in the primary Sanofi-Aventis (Study Number DIREGL07823). CMH Curr Atheroscler Rep 2018;20(6):31. doi: 10.1007/
care setting. reports an independent research grant from Amgen. s11883-018-0731-0.
620 Reprinted from AJGP Vol. 50, No. 9, September 2021 © The Royal Australian College of General Practitioners 2021Implications of new clinical practice guidance on familial hypercholesterolaemia for Australian general practitioners Focus | Professional
13. Vickery AW, Bell D, Garton-Smith J, Kirke AB, coronary artery disease, and cholesterol-
Pang J, Watts GF. Optimising the detection and lowering medication. J Clin Endocrinol Metab
management of familial hypercholesterolaemia: 2012;97(11):3956–64. doi: 10.1210/jc.2012-
Central role of primary care and its integration 1563. Erratum in: J Clin Endocrinol Metab
with specialist services. Heart Lung Circ 2014;99(12):4758–59.
2014;23(12):1158–64. doi: 10.1016/j.hlc.2014.07.062. 26. Pang J, Sullivan DR, Hare DL, et al. Gaps in
14. Brett T, Qureshi N, Gidding S, Watts GF. the care of familial hypercholesterolaemia in
Screening for familial hypercholesterolaemia in Australia: First report from the national registry.
primary care: Time for general practice to play Heart Lung Circ 2021;30(3):372–79. doi: 10.1016/j.
its part. Atherosclerosis 2018;277:399–406. hlc.2020.07.012.
doi: 10.1016/j.atherosclerosis.2018.08.019. 27. Arnold-Reed DE, Brett T, Troeung L, et al.
15. de Ferranti SD, Steinberger J, Ameduri R, Detection and management of familial
et al. Cardiovascular risk reduction in high- hypercholesterolaemia in primary care in Australia:
risk pediatric patients: A scientific statement Protocol for a pragmatic cluster intervention study
from the American Heart Association. with pre-post intervention comparisons. BMJ
Circulation 2019;139(13):e603–34. doi: 10.1161/ Open 2017;7(10):e017539. doi: 10.1136/bmjopen-
CIR.0000000000000618. 2017-017539.
16. Luirink IK, Wiegman A, Kusters DM, et al. 28. Australian Government Department of Health. The
20-year follow-up of statins in children Pharmaceutical Benefits Scheme schedule: Code no.
with familial hypercholesterolemia. N Engl 10958R. Canberra, ACT: Commonwealth of Australia,
J Med 2019;381(16):1547–56. doi: 10.1056/ 2020. Available at www.pbs.gov.au/medicine/
NEJMoa1816454. item/10958r [Accessed 10 December 2020].
17. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 29. Raal FJ, Hovingh GK, Catapano AL. Familial
ACC/AHA guideline on the primary prevention of hypercholesterolemia treatments: Guidelines and
cardiovascular disease: A report of the American new therapies. Atherosclerosis 2018;277:483–92.
College of Cardiology/American Heart Association doi: 10.1016/j.atherosclerosis.2018.06.859.
Task Force on Clinical Practice Guidelines.
30. Ramaswami U, Humphries SE,
Circulation 2019;140(11):e596–646. doi: 10.1161/
Priestley‑Barnham L, et al. Current management
CIR.0000000000000678.
of children and young people with heterozygous
18. Wald DS, Bestwick JP, Morris JK, Whyte K, familial hypercholesterolaemia – HEART UK
Jenkins L, Wald NJ. Child-parent familial statement of care. Atherosclerosis 2019;290:1–8.
hypercholesterolemia screening in primary care. doi: 10.1016/j.atherosclerosis.2019.09.005.
N Engl J Med 2016;375(17):1628–37. doi: 10.1056/
31. Pang J, Chan DC, Watts GF. The knowns and
NEJMoa1602777.
unknowns of contemporary statin therapy for
19. Troeung L, Arnold-Reed D, Chan She Ping‑Delfos W, familial hypercholesterolemia. Curr Atheroscler
et al. A new electronic screening tool for identifying Rep 2020;22(11):64. doi: 10.1007/s11883-020-
risk of familial hypercholesterolaemia in general 00884-2.
practice. Heart 2016;102(11):855–61. doi: 10.1136/
32. Ademi Z, Norman R, Pang J, et al. Health
heartjnl-2015-308824.
economic evaluation of screening and treating
20. Kirke AB, Barbour RA, Burrows S, et al. Systematic children with familial hypercholesterolemia
detection of familial hypercholesterolaemia early in life: Many happy returns on investment?
in primary health care: A community based Atherosclerosis 2020;304:1–8. doi: 10.1016/j.
prospective study of three methods. Heart atherosclerosis.2020.05.007.
Lung Circ 2015;24(3):250–56. doi: 10.1016/j.
33. Representatives of the Global Familial
hlc.2014.09.011.
Hypercholesterolemia Community, Wilemon KA,
21. Hooper AJ, Nguyen LT, Burnett JR, et al. Genetic Patel J, et al. Reducing the clinical and public health
analysis of familial hypercholesterolaemia burden of familial hypercholesterolemia: A global
in Western Australia. Atherosclerosis call to action. JAMA Cardiol 2020;5(2):217–29.
2012;224(2):430–34. doi: 10.1016/j. doi: 10.1001/jamacardio.2019.5173.
atherosclerosis.2012.07.030.
22. Kinnear FJ, Wainwright E, Perry Ret al. Enablers
and barriers to treatment adherence in
heterozygous familial hypercholesterolaemia:
A qualitative evidence synthesis. BMJ Open
2019;9(7):e030290. doi: 10.1136/bmjopen-2019-
030290.
23. Mach F, Baigent C, Catapano AL, et al. 2019
ESC/EAS guidelines for the management of
dyslipidaemias: Lipid modification to reduce
cardiovascular risk: The Task Force for the
management of dyslipidaemias of the European
Society of Cardiology (ESC) and European
Atherosclerosis Society (EAS). Eur Heart J
2020;41(1):111–88. doi: 10.1093/eurheartj/ehz455.
24. Grundy SM, Stone NJ, Bailey AL, et al. 2018
AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/
AGS/APhA/ASPC/NLA/PCNA guideline on the
management of blood cholesterol: A report of
the American College of Cardiology/American
Heart Association Task Force on Clinical Practice
Guidelines. Circulation 2019;139(25):e1082–143.
doi: 10.1161/CIR.0000000000000625. Erratum
in: Circulation 2019 Jun 18;139(25):e1182–86.
25. Benn M, Watts GF, Tybjaerg-Hansen A,
Nordestgaard BG. Familial hypercholesterolemia
in the Danish general population: Prevalence, correspondence ajgp@racgp.org.au
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 9, September 2021 621You can also read