International Journal of Case Reports - (ISSN:2572-8776)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Ali Al Bshabshe et al.,IJCR, 2021 5:226
Case Report IJCR (2021) 5:226
International Journal of Case Reports
(ISSN:2572-8776)
PICC Insertion could be an optimal choice of central venous access
in prone position mechanically ventilated COVID-19 ARDS patient
Ali Al Bshabshe1, Ali Abdullah Kablan2, Nasser Mohammed Alwadai3, Omprakash Palanivel3,
Ghaida Nawi A. Alharthi4, Khloud Faleh S. Alahmari4, Hala Khamis S. Alghamdi4, Raghad
Abdullah M. Brkout 4, Lamees Abdullah M. Brkout 4, Lama Abdullah M. Brkout 4
1
Intensive Care Consultant, Aseer Central Hospital & Professor, Department of Medicine/Critical
Care, College of Medicine, King Khalid University, Abha, Aseer Region, Saudi Arabia. 2Intensive
Care Senior Specialist, Department of Intensive Care Unit, Aseer Central Hospital, Abha, Aseer
Region, Saudi Arabia. 3Consultant Respiratory Therapist, Department of Respiratory Care Unit,
Aseer Central Hospital, Abha, Aseer Region, Saudi Arabia. 4Medical Students, Department of
Medicine, College of Medicine, King Khalid University, Abha, Aseer Region, Saudi Arabia.
ABSTRACT
During the management of critically ill covid-19 patients obtaining an *Correspondence to Author:
appropriate centrally inserted central catheter (CICC) can be a prime Ali Al Bshabshe
necessity. Traditionally, a CICC is inserted in a supine position. How- Department of Medicine/Critical
ever, a CICC may not be possible in some COVID-19 patients with Care, College of Medicine, King
severe hypoxia or sudden clinical deterioration who need urgent intu- Khalid University, Saudi Arabia.
bation and immediate proning. Therefore, CICC in pronated COVID-19
ARDS patients is challenging. Recent studies limited to case reports How to cite this article:
have shown that peripherally inserted central catheters (PICC) are Ali Al Bshabshe, Ali Abdullah Kab-
safer in pronated ARDS patients. PICC lines minimize mechanical lan, Nasser Mohammed Alwadai,
complications and lower catheter-related bloodstream infections when O mprakash Palanivel, Ghaida
compared to standard CICC. However, there is a scarcity of evidence Nawi A. Alharthi, Khloud Faleh S.
showing the efficacy of PICC in pronated COVID-19 ARDS patients, Alahmari, Hala Khamis S. Algham-
possibly due to the complex precautionary safety measures, insertion di, Raghad Abdullah M. Brkout,
techniques, and expertise team deficit. Herein, we present a 57-year- Lamees Abdullah M. Brkout, Lama
old male as a case of COVID-19 ARDS, mechanically ventilated in Abdullah M.Brkout. PICC Insertion
a prone position with existing subcutaneous emphysema. Our case could be an optimal choice of cen-
illustrates PICC insertion challenges in the prone position, ultrasound tral venous access in prone position
guidance in PICC insertion to comprehend the vein’s diameter for ac- mechanically ventilated COVID-19
curate vein needling in proportion to the external catheter diameter, ARDS patient. International Journal
and intracavitary electrocardiographic (ECG) navigation method to of Case Reports, 2021 5:226.
confirm catheter tip location. So that chest X-ray and radiology risk of
contamination is avoided. Long-term research urged to validate the ef-
ficacy of PICC in this group of patients.
Keywords: Central Venous access devices (VAD) Central venous
access devices (CVAD), Centrally inserted central catheter (CICC),
eSciPub LLC, Houston, TX USA.
peripheral inserted central catheter (PICC), Blood gas analyses
Website: http://escipub.com/
(BGA), Subcutaneous emphysema (SE), Electrocardiography (ECG),
Intracavitary electrocardiography (IC-ECG).
IJCR: https://escipub.com/international-journal-of-case-reports/ 1
Ali Al Bshabshe et al.,IJCR, 2021; 5:226
Introduction position.[5] In particular, patients with severe
hypoxia or any sudden clinical deterioration may
The rapid global transmission of novel
need urgent, rapid sequence intubation and
coronavirus has alarmed the health care system
immediate proning. Considering the proning
for urgent revision of current clinical methods. As
therapy in such a group of patients is vital as it
an outcome, many standard clinical maneuvers,
improves regional ventilation, oxygenation, and
treatment protocols, and policies are revised and
alveolar recruitment. Therefore, perfusion
refined to decrease the risk of virus exposures
redistribution increases and the recruitment of
and transmissions.[1] In particular, utilizing
perfused tissue of dorsal regions exceeds the
modern medical technologies and associating
ventral derecruitment and enhancing the
with the clinical procedures may enhance health
ventilation and perfusion ratio.[6] CICC is highly
care professionals' safety and patient safety,
recommended for the extended treatment of
thereby reducing morbidity, mortality, and cost
covid-19 ARDS patients. Since it holds long-life
values. The standard first-line invasive
durability, with various benefits of continuous
procedure of hospitalized patients is to obtain
multiple high flow infusions including sedation,
venous access through appropriate venous
muscle relaxants, vasopressors, and infusions
access devices (VAD). Generally, VAD is
of solutions with pH greater than 9 and lesser
classified into peripheral venous access device
than 4 (e.g., dopamine, vancomycin,
(PVAD), central venous access device (CVAD).
levofloxacin), or hyperosmolar parenteral
The peripheral venous access (PVAD) is sub-
nutrition (whose osmolarity exceeds 800-900
classified into short peripheral cannula (15cm). Further, the central venous
jugular or subclavian vein) in mechanically
access device (CVAD) classified into a femoral
ventilated prone patients is challenging.
inserted central catheter (FICC), subclavian, and
Moreover, it is critical to turn the prone patient to
internal jugular centrally inserted central
supine as it may disrupt the regional ventilation,
catheter (CICC), and peripheral inserted central
resulting in oxygenation impairment,
catheter (PICC).[2] According to the database of
hemodynamic instability, and life-threatening
the United States of America, approximately five
events. Recent studies have demonstrated that
million CVAD inserted annually.[3] Although the
PICC is safer in prone ARDS patients. It
absolute number of CVAD insertions in covid
minimizes the risk of pulmonary-pleural
patients has not been reported yet, it is vivid to
complications and catheter site contamination
believe that all critically ill COVID-19 ARDS
as it is isolated from the patients' oral and
patients claim a CVAD for the optimal
tracheal secretions. Additionally, it lowers the
management of their illness. COVID-19 ARDS is
exposure risk of a patient's nasal, oral and
relevant to the customary ARDS pathology. It
tracheal secretions to the operator, his
begins with increased capillary permeability and
associates and non-contraindicated to the
hyaline membrane formation characterized by
anticoagulated patients. Furthermore, PICC can
interstitial widening and edema, resulting in a
preserve the upper central regions (internal
protein-rich fluid collection in the alveoli of lungs
jugular and subclavian vein) for prospective
resulting in oxygen impairment as patients
dialysis and ECMO cannulation if needed.[8]
advance further into their covid sickness leading
to lung fibrosis which is the significant character Herein, we report an innovative, unique, rare
of COVID‐19 ARDS. [4] Patients in ICU may need PICC line insertion in a prone position
CICC, and the standard position of CICC mechanically ventilated patient with existing
insertion is supine. However, in some covid-19 subcutaneous emphysema to treat COVID-19
ARDS patients, CICC is not possible in a supine ARDS disease. We describe our challenges
IJCR: https://escipub.com/international-journal-of-case-reports/ 2
Ali Al Bshabshe et al.,IJCR, 2021; 5:226
concerning the prone patient, operator, and mmHg. Oxygen saturation on room air was 60 %
associates' precautionary safety measures. treated with a non-rebreathing mask of 15 l/min.
Also, ultrasound guidance is essential to Oxygen saturation rose to 88%. Initial blood gas
determine the vein's diameter for cannulation analyses were Ph; 7.39 Pco2; 45.7 Po2; 56
combining modified seldinger technique HCO3; 25 So2; 68.7. On physical examination,
approach for accurate vein needling. Following mild jugular distension, the weight of 90kg, the
insertion, it is imperative to check the location of height of 174cm, and BMI of 29.7 kg/m2. On
the tip of the central venous catheter by non- auscultation, severe bronchospasm and diffuse
radiological methods, such as intracavitary bilateral wheezes. Anterior-posterior x-ray
electrocardiography (IC-ECG). Thereby, x-ray reveals COVID-19 pneumonia. In ED, two short
radiation is avoided. peripheral venous access obtained on both
Case report hands to administer intravenous fluids and
methylprednisolone of 120 mg/kg and repeated
The 57-year-old male COVID-19 positive with a
back-to-back nebulized salbutamol 2.5 mg,
medical history of diabetes mellitus type 2
ipratropium bromide 0.5 mg, and budesonide 0.5
presented to the emergency department (ED)
mg were given for his bronchospasm. The
after 6 days of home quarantine with symptoms
repeated ABG showed pH: 7.29 PaCO2:50.7
of progressive shortness of breath, chest
PaO2: 48 HCO3; 20.7 So2 63.6. Despite the
tightness, dry cough, fever, and myalgia. His
therapy, the patient's condition deteriorated, and
initial vitals are Glasgow coma scale (GCS)
he was diagnosed with acute hypoxic respiratory
15/15, respiratory rate 36 breath per minute
failure associated with COVID-19 pneumonia
(bpm) using accessory muscles, temperature 39
0 and transferred to ICU for close observation.
C, heart rate 116 bpm, blood pressure 130/88
Figure 1 Depicts COVID-19 ARDS X-ray with diffuse subcutaneous emphysema
IJCR: https://escipub.com/international-journal-of-case-reports/ 3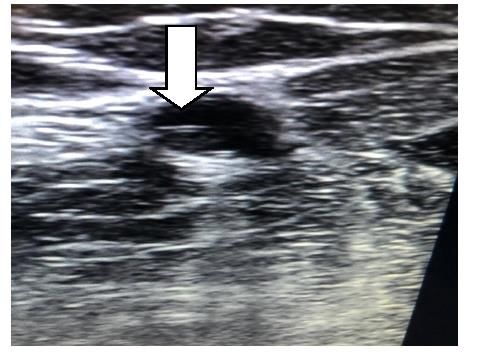
Ali Al Bshabshe et al.,IJCR, 2021; 5:226
Figure 2 A view of a prone patient with right arm tourniquet
A high flow nasal cannula (HFNC) 60LPM with the patient complained of sudden chest
fio2 100% was initiated, and the patient tightness, difficulty breathing, restlessness with
admirably responded, with spo2 of 91%. After 48 spo2 of 68%, respiratory rate of 50 bpm, and
hrs of HFNC, the patient started to deteriorate hypotension. Dexmedetomidine was
with spo2 of 70% and an increased respiratory commenced on 0.4 mcg/kg/hour, and inotropes
rate of 48 bpm using accessory muscles. We (non-adrenaline) escalated to a maximum of 16
decided to hook the patient on NIV (CPAP) mcg/per minute on short periphery venous
ventilation with a peep of 8 cmh2o, pressure access to reach targeted mean arterial blood
support of 15 cmh2o to promote oxygenation pressure. Repeated BGA showed metabolic
and reduce work of breathing. The patient is acidosis (Ph; 7.23 pCO2;65 PO2 52.9 HCO3;
subjected to nursing in proning and lateral 20.7 So2; 69.9), and Chest X-ray revealed
positions periodically. Repeated BGA after 1 subcutaneous emphysema with severe ARDS.
hour of NIV was satisfactory. On 3 days of NIV, (Figure 1)
Figure 3 A view of basilic vein (white arrow depicts PICC line) through ultrasound guidance
IJCR: https://escipub.com/international-journal-of-case-reports/ 4
Ali Al Bshabshe et al.,IJCR, 2021; 5:226 Figure 4 Navigation ECG technology showing the patient electrocardiogram tracing above and the intravenous tracing below showing maximal P-wave confirming superior vena cava placement. Following this sudden clinical deterioration, our therapy is required to improve his oxygenation. team decided on elective intubation as a life- We considered that the insertion of CICC in the saving emergency. With complete personal supine position would interrupt the prone protective equipment (PPE), the intensivist therapy and consequently hinder the intubated the patient with a 7.5 Endotracheal improvement of oxygenation. In this clinical tube (Portex, USA) at 22cm level respectively setting, we decided to insert PICC in the prone from central incisors and connected to the position provided that potential benefits are mechanical ventilator (Maquet servo-i) with more than standard central venous catheters PRVC mode tidal volume of 420 ml, peep 12 (CVC). After guaranteed mechanical ventilation cmh2o, RR 20 with I:E of 1.2.5. Despite all these stability in the prone position, the patient's right measures, oxygen saturation is
Ali Al Bshabshe et al.,IJCR, 2021; 5:226
With precautionary safety measures, a maximal The advancement of the healthcare system in
barrier drape was placed to cover the patient and this century has extended the human life span
mayo table used at the procedure. Then a sterile significantly. However, the emergence of diverse
PICC tray was prepared (PowerPICC catheter co-morbidity, new clinical diseases, and its
with sherlock Tip positioning system, 5 Fr, triple severity has increased frequent hospitalization,
lumen, US). An estimated PICC length was and in such circumstances obtaining long-life
measured was from the tip of the 3rd finger to venous access through appropriate central
the middle of the elbow crease to the most venous access devices (CVAD) for critically ill
prominent point of the acromion process to the patients is imperative. In this perspective, CVAD
sternal head of the clavicle and to the end of the has become the standard first-line device for
xiphoid process to place the catheter tip in the central venous access. Studies before the
superior vena cava and avoid the invasion COVID-19 pandemic has shown that annually
catheter tip into the right atrium. The ultrasound Clinicians insert millions of CICC, with an overall
probe was draped with a double sterile plastic complication rate of 15% (5% to 19%). such as
cover, and the depth was set to 3.5cm. Through catheter-related infection (5% to 26%), a
ultrasound guidance, the patient's right basilic thrombotic event (2% to 26%) and power-driven
vein accessed by a short-axis out of plane mechanical complications (5% to19%).[9] Power-
approach followed by a 22 G over needle driven mechanical complications usually happen
catheter penetrated the superficial basilic vein in the following circumstances 1. insertion of
using a long axis in-plane approach (6-15 MHz, CVAD in an emergency, 2. inserting large
SonoSite Edge, SonoSite Japan Co., Tokyo, catheters size (dialysis), 3. increased number of
Japan) using modified seldinger technique. needle pricks, 4. complex central vein anatomic
Next, a triple lumen PICC catheter (proximal) anomaly, 5. inexperienced operator, which
advanced into a basilic vein, and with the ECG results in hematoma, hemothorax,
navigation assistance method, reached the pneumothorax, arterial-venous fistula, air
superior vena cava (superior Cavo atrial embolism, nerve injury, left side thoracic duct
junction) until the maximal P-wave was noticed injury, intraluminal dissection, punctured aorta,
on the screen (Figure 4). and jugular. [10] However, pneumothorax is one
Furthermore, distal PICC lumens were towards of the prime complications of CVAD insertion
the arm's posterior aspect placed with a sterile serving up to 30% of all power-driven
dressing (Figure 5). Overall, the procedure time mechanical adverse complications. [11]
was 20 minutes, resulting in 100% technical Likewise, covid-19 patients admitted through
success and obviating the necessity for a chest this current pandemic were more likely to require
radiograph. The PICC line was used for 21 days high critical care support with prolonged
continuously. Patients did not develop catheter- hospitalization and prolonged ICU stay with the
related bloodstream infections or upper provision of a long-life span of venous access,
extremity deep venous thrombosis related to which may put them at greater risk of power-
PICC placement. No line malfunction was driven mechanical complications and central
reported, and no requests were received to line-associated bloodstream infections
replace PICC. Institutional anticoagulation (CLABSI). Moreover, the timeline from COVID-
protocol based on d-dimer levels and PTT ratio 19 diagnosis to the incidence of CLABSI is 18
was followed. the patient was tracheostomized days on average [12], implying that the CLABSI
and weaned from the mechanical ventilator and episodes can befall COVID-19 patients with
discharged to peripheral hospital on day 22 for prolonged hospitalization. According to the US
rehabilitation and nursing care. nation's surveillance system for healthcare-
Discussion associated infections (HAIs) reports during
IJCR: https://escipub.com/international-journal-of-case-reports/ 6Ali Al Bshabshe et al.,IJCR, 2021; 5:226
(COVID-19) pandemic has exhibited the required immediate central venous access.
standardized infection ratio (SIR) of CLABSI rate Generally, intensivists prefer to use Internal
has increased to 39% in the critical care unit.[13] jugular, subclavian, femoral vein (CICC) rather
similarly, a study conducted by Kathleen M. et al. than PICC in covid patients. However, few
reported that in 2 hospitals where the study was studies report the effectiveness of PICC for
conducted report the highest impact on the central venous access in critically ill patients. [18]
healthcare-associated infection (HAI) is CICC insertion with existing SE can worsen
expected to be CLABSI rates. With the marked further. Furthermore, in the pronated patient, the
increase in CLABSI rates in both hospitals of dressing of a CVAD is inevitably more
420% increase to rate = 5.38 cases per 1,000 uncomfortable to manage with difficulty in
central line days, and a 327% increase to rate = periodic monitoring of the exit site and the
3.79 cases per 1,000 central line days. Also, the connection/disconnection of the infusion lines.
proportion of COVID-19 patients with CLABSI During the maneuvers of pronation-supination, it
events was 5 times greater than for non–COVID- can result in stretching, drawing, and kicking at
19 patients during the pandemic period. [14] CVAD insertion sites. [19] However, no case was
Based on the recent studies above, we decided reported previously about PICC insertion in the
to keep our patient on limited short peripheral prone position with existing SE like the case we
venous access in the ICU since the patient had present in this paper.
hemodynamic stability with GCS15/15 and no Intensivists must contemplate the jeopardies of
inotropes requirement. Although barotrauma catheter-related complications in selecting the
incidence is rare in NIV, a recent single-center, CVAD, which incorporates deep vein thrombosis
retrospective, observational cohort study has and bloodstream infections. Although there are
shown that 21% of 75 patients with COVID-19 no variations in infectious complications
treated in an intensive care unit (ICU) sustained between PICC and CICC approaches in critically
barotrauma (including pneumothorax, ill patients. [20] Still, there remains a controversy
pneumomediastinum, pneumopericardium, and concerning the thrombotic complications
subcutaneous emphysema). In that, 33% of between these approaches of PICC and CICC.
patients receiving IMV, 8% of patients receiving Apart from barotrauma, induction of a CICC in
(NIV). [15] Similarly, our patient-reported surgical sitting or upright positions carries a risk of air
emphysema on standard NIV recommended embolism. Contrarily, there was no report of
settings and SE were managed conservatively PICC-related air embolism. Usually, PICC is
by lowering the NIV pressure. However, our inserted in a peripheral vein. A peripheral vein
patient's condition has worsened suddenly with pressure is higher than atmospheric pressure,
a spo2 of 68%. The patient was intubated on 3rd resulting in no air embolism during PICC
day of his hospitalization and required insertion. [21] Hence, a patient in the prone
immediate prone positioning for severe hypoxia. position with existing SE can be secured safely
Consequently, spo2 rose to 94%, and the P/F by PICC. The Perception of PICC insertion in
ratio was 114, which correlates to the data COVID 19 patients in the prone position is
presented by Atsushi et al., that among 125 feasible and straightforward with ultrasound
patients, 121 patients (96.8%) are intubated guidance. The number of failed attempts
within 14 days of their clinical onset. [16] Also, decreases to 86% with ultrasound by decreasing
Tyler et al. stated that after the first prone the number of attempts and procedure time-
positioning session, the Pao2/Fio2 ratio outs. Also, several clinical studies have
increased from 17.9 (7.2) to 28.2 (12.2) kPa demonstrated a high precision rate for ECG-
within 81 (61–119) minutes in 36 subjects. [17] guided CVC placement with 97.3% sensitivity
Although prone positioning improved and 100% specificity. [22]
oxygenation instantly, severe hypotension
IJCR: https://escipub.com/international-journal-of-case-reports/ 7Ali Al Bshabshe et al.,IJCR, 2021; 5:226
In summary, The COVID-19 pandemic indeed [5]. D. M. Nguyen J. K. Christopher R. G. Day Central
modified today's clinical practices of Central Venous Access in the Prone Patient: Using a
Traditional Approach to Solve a Contemporary
venous accesses. The positive outcome of this
Problem. Am J Respir Crit Care Med
PICC procedure in critically ill covid-19 patients 2020;201:A1760.
with subcutaneous emphysema who require [6]. Vasilios Koulouras, Georgios Papathanakos, and
immediate intubation and prone positioning has Georgios Nakos. Efficacy of prone position in
significantly created a new awareness to acute respiratory distress syndrome patients: A
pathophysiology-based review. World J Crit Care
implement expertise, intensivist, and nurses' Med. 2016 May 4; 5(2): 121–136.
team to employ the suitable Central venous [7]. Paolo Cotogni and Mauro Pittiruti. Focus on
accessibility. Furthermore, our case highlights peripherally inserted central catheters in critically
that daily prompt investigation of the inserted ill patients. World J Crit Care Med. 2014 Nov 4;
PICC line integrity, position, and daily catheter 3(4): 80–94.
[8]. Mauro Pittiruti, Fulvio Pinelli. Recommendations
dressing care minimize the incidence of PICC- for the use of vascular access in the COVID-19
related complications and save resources patients: an Italian perspective. GAVeCeLT
through ultrasound-guided catheter positioning Working Group for Vascular Access in COVID-19.
and IC-ECG to check for catheter tip location Crit Care. 2020; 24: 269. 2020 May 28.
abandon the routine use of chest X-ray. [9]. Nikolaos Tsotsolis, Katerina Tsirgogianni, Paul
Zarogoulidis. Pneumothorax as a complication of
Conclusion central venous catheter insertion. Ann Transl
PICC line is a safe procedure and feasible to be Med. 2015 Mar; 3(3): 40.
[10]. Polderman KH, Girbes AJ. Central
done on prone positioned mechanically
venous catheter use.Part 1: mechanical
ventilated patients. In addition, this procedure complications. Intensive Care Med 2002;28:1-17.
may be applicable for patients in whom central [11]. Mitchell SE, Clark RA. Complications of
venous access is not possible in a supine central venous catheterization. AJR Am J
position and patients at the risk of barotrauma. Roentgenol 1979;133:467-76.
[12]. Mohamad G. Fakih , Angelo Bufalino, Lisa
Acknowledgment Sturm , Ren-Huai Huang , et.al. Coronavirus
We thank Moosa Oatif RT, Mofareh alisheri RT, disease 2019 (COVID-19) pandemic, central-line–
associated bloodstream infection (CLABSI), and
Abdulwahab RT, Ibrahim Eissa RT, Ali
catheter-associated urinary tract infection
Mushashab Assiri RT. (CAUTI): The urgent need to refocus on
Conflict of interest hardwiring prevention efforts.Infection Control &
Hospital Epidemiology (2021), 1–6.
None
[13]. Prachi R. Patel, Lindsey M. Weiner-
References Lastinger,, Margaret A. Dudeck, Lucy V. Fike et
[1]. Mauro Pittiruti, Fulvio Pinelli, Maria Giuseppina al.,Impact of COVID-19 pandemic on central-line–
Annetta, Sergio Bertoglio, Daniele et al. associated bloodstream infections during the
Considerations on the use of vascular access early months of 2020, National Healthcare Safety
devices in patients with COVID-19 (and some Network. Infect Control Hosp Epidemiol. 2021 Mar
practical recommendations). Medical Alley. 15 : 1–4.
https://medicalalley.org/2020/04. [14]. Kathleen M. McMullen, Barbara A. Smith, Terri
[2]. Mid & Long-term Vascular Access & Imaging Rebmann. Impact of SARS-CoV-2 on
Equipements for COVID-19 patients. hospital-acquired infection rates in the United
https://www.vygon.com/patients-covid-19/ States: Predictions and early results. Am J Infect
[3]. Craig Kornbau, Kathryn C Lee, Michael S Control. 2020 Nov; 48(11): 1409–1411.
Firstenberg. Central line complications Int J Crit [15]. Michael R. Kahn, Richard L. Watson, Jay T.
Illn Inj Sci. 2015 Jul-Sep; 5(3): 170–178. Thetford, Joseph Isaac Wong, Nader
[4]. Sabrina Setembre Batah, Alexandre Todorovic Kamangar. High Incidence of Barotrauma in
Fabro. Pulmonary pathology of ARDS in COVID- Patients With Severe Coronavirus Disease 2019.
19: A pathological review for clinicians. Respir Journal of Intensive Care Medicine 2021, Vol.
Med. 2021 Jan; 176: 106239. 36(6) 646-654.
IJCR: https://escipub.com/international-journal-of-case-reports/ 8Ali Al Bshabshe et al.,IJCR, 2021; 5:226
[16]. Atsushi Hirayamaa,b, Jun Masuia, Ayumi
Murayama, Satomi Fujitaa, Jun Okamotoa.The
characteristics and clinical course of patients with
COVID-19 who received invasive mechanical
ventilation in Osaka, Japan. Int J Infect Dis. 2021
Jan;102:282-284.
[17]. Tyler T. Weiss, Flor Cerda, J. Brady Scott,
Ramandeep Kaur et al. Prone positioning for
patients intubated for severe acute respiratory
distress syndrome (ARDS) secondary to COVID-
19: a retrospective observational cohort study.
British Journal of Anaesthesia, (2021) - 126 (1):
48e55.
[18]. Ashley Snyder, Scott A. Flanders, Vineet
Chopra. Peripherally Inserted Central Catheters
(PICCs) in the ICU: A Retrospective Study of Adult
Medical Patients in 52 Hospitals. Crit Care Med.
2018 Dec; 46(12): e1136–e1144.
[19]. Kathleen M. McMullen, Barbara A. Smith, Terri
Rebmann, Impact of SARS-CoV-2 on
hospital-acquired infection rates in the United
States: Predictions and early results. Am J Infect
Control. 2020 Nov; 48(11): 1409–1411.
[20]. Paolo Cotogni and Mauro Pittiruti. Focus on
peripherally inserted central catheters in
critically ill. World J Crit Care Med. 2014 Nov
4;3(4):80-94.
[21]. P Mitsuda S, Tokumine J, Matsuda R,
Yorozu T, et al. PICC insertion in the sitting
position for a patient with congestive heart failure:
A case report. Medicine (2019) 98:6(e14413)
[22]. 22.Y.L.A. Velascoa, O.C. Torres b, R.A.S.
Mendoza, W.G.P. Amayaa, et al. Proper
electrocardiography-guided placement of a
central venous catheter. Rev Med Hosp Gen Méx.
2016.http://dx.doi.org/10.1016/j.hgmx.2016.09.00
7
IJCR: https://escipub.com/international-journal-of-case-reports/ 9You can also read

















































