CROSSING THE BORDER FOR HEALTH CARE: ADDING VALUE FOR PATIENTS AND HEALTH SYSTEMS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Eurohealth 28(1) 51
CROSSING THE BORDER FOR
HEALTH CARE: ADDING VALUE FOR
PATIENTS AND HEALTH SYSTEMS
By: Matthias Wismar, Robert Touret, Jonathan Clottes, Gabrielle Dubois, Apolline Damez-Fontaine,
Vincent Rouvet and Ewout van Ginneken
Summary: In the European Union, patients are able to receive health
care in another Member State. This has made life much easier
for people travelling, working, studying, and residing abroad and
provided options for patients facing long waiting times at home or
suffering from rare diseases. These opportunities have been especially
important during the COVID-19 pandemic, which has led to increased
demand for COVID-19 care as well as catch-up care following the
disruption to routine health services. As we are progressing towards
a European Health Union, we suggest where improvements to cross-
border health care could be made.
Keywords: Cross-Border Care, Border Regions, Bilateral Agreements, COVID-19
Introduction Cross-border health care helps European
patients who fall sick abroad, increases
Cross-border health care adds substantial
options to receive planned care in another
value for European patients and citizens.
European Union (EU) country, can help
It has been gradually developed since
patients with rare diseases, and provides
the beginning of the European Economic
Matthias Wismar is Programme opportunities to develop cross-border
Manager, European Observatory Community to ensure free movement
collaboration between providers and
on Health Systems and Policies, in the European labour market. Cross-
Brussels, Belgium; Robert Touret payers. It also has the capacity to help
border health care rests on various legal
is Head of the Office of European, alleviate health system pressures in times
frameworks. The two most important
International and Overseas Affairs, of crisis.
Jonathan Clottes is Project legal frameworks are: 1) the regulation
Manager, Gabrielle Dubois on the coordination of social security
is Project Manager and Learning from experiences during the
systems (European Commission
Apolline Damez-Fontaine COVID-19 crisis, Europe is moving
is Project Manager, General Regulation 883/2004); and 2) the patients’
towards the creation of a European Health
Directorate of Healthcare Services, rights directive (Directive 2011/24/EU)
French Ministry of Solidarity and Union, in which EU countries work more
(see Box 1). Cross-border care received an
Health, Paris, France; Vincent closely together to protect the health of
Rouvet is the General Director of important impetus when Directive 2011/24
Europeans and to collectively respond to
the Hospital of Cerdanya, Puigcerdà, on the application of patients’ rights in
Spain; Ewout van Ginneken is cross-border health crises (see the article
cross border health care passed in 2011
Berlin Hub Coordinator, European by Mauer et al. in this issue on a European
Observatory on Health Systems (Table 1 distinguishes between the
Health Union). In this context, cross-
and Policies, Berlin University of regulation and the directive), though
border health care must not be forgotten
Technology, Germany. further progress towards implementation
Email: wismarm@obs.who.int and warrants further attention.
in practice and user-friendliness
is necessary.
Eurohealth — Vol.28 | No.1 | 202252 Eurohealth 28(1)
were reported up from 232,054 in 2018.
The growth occurred predominantly in
Box 1: The legal framework for cross-border health care in the EU: cross-border care not requiring prior
general principles for better access to care authorisation. These numbers are not
directly comparable because of variations
The regulation on the coordination of social security systems (European
in the number of countries reporting
Commission Regulation 883/2004) provides the legal framework for unplanned
each year. The total expenditure on all
care and planned care organised by the competent authority (i.e. those with the
reimbursements reported by the Member
power to perform the designated function, such as a sickness fund or national
States also rose in 2019 to €92 million
government). The coordination of social security systems was introduced to
up from €73.3 million in 2018. 3 The
facilitate cross-border mobility for workers, which is a precondition for a European
impact of the directive on national health
labour market. Therefore, the predecessor or the regulation on the coordination
budgets appears marginal estimated at
of social security systems, Regulation of the Council Number 3 on social security
only 0.004% of the EU-wide annual health
of cross-border workers, came into force almost in parallel with the creation of the
care budget. 4 However, as mentioned
European Economic Community. The regulation has been reformed several times
above, the data are incomplete.
and renamed but retained its function in guaranteeing cross-border social security.
The patients’ rights directive (Directive 2011/24/EU) is more recent and
How does the cross-border European
establishes the right to seek health care in another Member State. It was passed
care framework benefit EU citizens?
after a long political process in 2011 with an implementation period of three years. It
codifies a series of landmark rulings from the European Court of Justice (CJEU) on It covers European patients who fall
cross-border health care. The case law focused on demands of European citizens sick abroad
that the free movement of services also applies to health services and goods
EU nationals, who are crossing the border
and therefore they derived from this an entitlement to access cross-border health
to live, work, study or retire can rely on
care. 1 In a series of rulings, the CJEU followed these demands with the exception
the European Health Insurance Card
of ‘hospital care’, or what is now called ‘planned care’ allowing pre-authorisation
(EHIC) when falling sick. It allows anyone
through competent authorities. 1
who has health coverage in their country
Beyond codifying case law, the patient’s rights directive is of particular importance of origin to receive medical treatment
to the development of cross-border health care as it stipulates provisions with in another Member State for free or at a
regards to ‘cooperation in health care’. The topics addressed are instrumental reduced cost if that treatment becomes
to the improvement and accessibility of cross-border health care for patients, necessary during their visit abroad. Pre-
e.g. assistance and cooperation, recognition of a prescription issued in another existing chronic conditions which require
Member State, the European Reference Networks (ERNs), action in the area of rare care, such as kidney dialysis, are also
diseases, eHealth, and cooperation on Health Technology Assessment (HTA). covered. Students who study in another
country can also use the EHIC for health
There is a host of other hard- and soft-law instruments surrounding the regulation
care. Posted workers, who are sent by their
and the directive. Their purpose is to specify, implement or explain the legal
employers for up to 24 months to another
frameworks.
EU Member State can use the EHIC to
obtain health care in the country of work,
though their employer needs to request a
form prior to the posting as a statement
The number of patients using cross- Switzerland, from Austria to Germany,
of the applicable legislation. The same
border health care is currently small from Luxembourg to Belgium, and from
is applicable for workers, who work in
Belgium to Luxembourg. 2 The number
Overall, the number of patients using more than one country. Frontier workers,
of patients using cross-border health care
cross-border health care under both legal that commute on a daily or weekly basis
under the regulation is difficult to assess
frameworks – the regulation and the to another Member State may choose
and clear trends cannot be identified.
directive – appear small and the budgetary between health care in their country of
There are many reasons for inaccuracies.
impacts are very limited. residence or country of work. This right is
There are severe data gaps 3 and some
retained at retirement and extended to their
Member States do not make a distinction
It is estimated that unplanned health families and their survivors.
between planned care under the regulation
care under the regulation amounts to
and the directive. Moreover, some of the
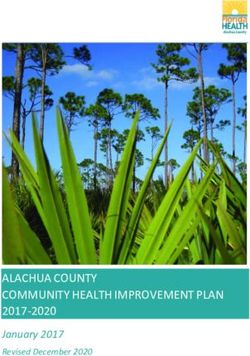
around 2 million patients per year. Figure 1 It increases the option to receive
bilateral agreements for cross-border
provides an overview on the budgetary planned care abroad
health care do not routinely report
impact of cross-border health care under
their data. EU nationals can also ask for access
the regulation, which amounts to 0.4% of
to cross-border health care for planned
the total health care budget in the EU. For
The numbers of patients using the directive procedures. This is particularly attractive
planned health care, the most prominent
for cross-border health care and the costs when long waiting lists exist in the
flows took place from France to Belgium,
reimbursed by the competent authorities country of residence or if the health care
from Luxembourg to Germany, from
is much smaller. In 2019, 290,890 cases facility may be closer to the place of
Germany to Austria, from Germany to
Eurohealth — Vol.28 | No.1 | 2022Eurohealth 28(1) 53
Table 1: Cross-border health care legal frameworks in comparison
Regulation on the coordination of social security Directive on patients’ rights in cross-border health care
Countries included EEA and Switzerland EU Member States, Iceland, Norway and Liechtenstein
Patients covered EU nationals, stateless people and refugees who reside in the Insured persons
territory of a Member State
Sectors covered Public health care Private and public health care
Services covered Unplanned necessary care and planned care organised Planned and unplanned/necessary care initiated through
through the competent authority the patient
Expenditure covered Competent authority covers the expenditure incurred; Reimbursement of health care costs according to national
travel expenses are not covered tariffs in country of affiliation; travel expenses are not covered
Note: After the United Kingdom’s withdrawal from the EU, British citizens can continue to use their EHIC card until expiry date or they can apply for the Global Health Insurance Card which covers
unplanned but not planned care in the countries covered by the regulation; Norway, Iceland and Liechtenstein joined the legal framework in 2015.
Figure 1: Budgetary impact of cross-border health care under the regulation, rare diseases, which affect 30 million
by type, 2019 European Union citizens. 5 While a
number of countries have strategies or
0.45
% plans to address rare disease, the scarcity
of cases and knowledge in this area
0.4%
0.40 makes a European approach necessary
healthcare spending related to benefits in kind
and cross-border cooperation is needed
Cross-border healthcare as a share of total
0.35
to promote better, faster and more
0.3%
0.30 accurate diagnosis. According to a survey
conducted by Eurordis, which covered 8
0.25
rare diseases, 25% of patients waited from
0.20 five to 30 years for a correct diagnosis,
and during that time 41% received a
0.15
misdiagnosis. 6 To help patients with
0.10
0.1% rate diseases, the directive of 2011 led to
the creation of 24 European Reference
0.05 Networks (ERNs), including 900 highly
0.02%
specialized units from over 300 hospitals
0.00
in 26 EU countries. 7 Through the pooling
Unplanned Health care provided to Planned Total cross-border
health care persons living in a MS health care health care of medical expert knowledge, the ERNs
other than the competent MS provide common expertise thus offering
patients potential benefits in terms of
2
Source:
early diagnosis and improved treatment.
Note: No data is available on prior authorised care from countries with prior-authorisation procedures from Germany. No data Meanwhile, The Rare 2030 (Eurordis)
is available on health care not requiring prior authorisation from Germany, Hungary, Luxembourg, the Netherlands. foresight study, initiated by the European
Parliament and supported by the European
residence. There is, however, always a procedure. Some Member States, Commission, emphasises the importance
requirement to seek prior approval under however, require pre-authorisation for of European cross-border cooperation
the regulation. But once authorisation has the obtained care subject to specific and innovation in this area and will help
been granted, all financial aspects are conditions. In contrast to the previously guide a reflection on rare disease policy
taken care of by the competent authority, mentioned process, the patient needs in Europe over the next decade. 8
be it a sickness fund or a health authority. to pay in advance and can only claim
In case of undue delay, e.g. if care cannot reimbursement upon completion of
Bilateral agreements have been
be provided within a medical justifiable the procedure.
developed to allow for cross-border
time, the pre-authorisation requirement is
collaboration across Member States
not applicable. It can help patients with rare diseases
and regions
who cannot access treatment at home
EU nationals can seek cross-border A mapping exercise commissioned by
Cross-border health care under the
health care on their own initiative under the European Commission in 2016/2017 9
directive also provides substantial benefits
the directive. They are free to choose a identified 1,167 projects of which 423
for patients living with rare diseases at the
provider across the border for a planned projects were listed, showcasing a great
European level. There are more than 6000
Eurohealth — Vol.28 | No.1 | 202254 Eurohealth 28(1)
a tri-national competence centre for
cross-border collaboration between
Box 2: The bi-national Hospital de Cerdanya /Hôpital de Cerdagne Germany, France and Switzerland in the
Upper Rhine Region. TRISAN conducts
The AECT-HC/GECT-HC is a cross border hospital, situated in the Est Pyrenees.
studies, provides information, connects
Its very name (AECT/GECT stands for European Grouping of Territorial
stakeholders for best-practice exchanges,
Cooperation) speaks of its vocation as a bi-national instrument, devised
and supports the cross-border cooperation
to facilitate access to specialised medical care for a local population of
project. 10
around 33,000 (although this greatly increases during peak tourist seasons)
inhabiting 50 municipalities on a 1340 km2 territory.
Several Member States have bilateral
The founding partners of the AECT-HC/GECT-HC are the public health care cross-border agreements for planned
systems of France and Catalonia, Spain. The EU contributed 60% of the building health care in place. They help to
costs through FEDER funds; CatSalut and ARS-Occitanie shared the rest, and overcome temporary capacity shortages
funded 100% of the equipment. The facility is managed jointly by both health care and the long waiting lists resulting
systems with a yearly operating budget of €20 million. from it. According to a study on the
Franco-Belgian ZOAST-initiative
The project for a bi-national, shared hospital that is pivotal to a future cross-border
(Zones Organisées d’Accès aux Soins
health care network, was long in the making. It originated in 2005 with a declaration
Transfrontaliers), the largest share
of intent signed by the French and Catalan authorities, and in 2007 the EGCT
of inpatient interventions provided
was registered. The need for a new hospital was particularly important for the
were gastroplasty for the treatment
local French population whose main reference hospital was in Perpignan, which
of obesity, stent placement, treatment
was difficult to access through mountain roads or by the helicopter emergency
of diaphragmatic hernia or hiatal
medical service.
hernia, therapeutic ureteroscopy, hip
Since its opening in September 2014, the centre offers access to 11 medical and replacement, pacemaker, knee prosthesis,
surgical specialties to the local population and tourists in a small but modern local polysomnography, treatment of bilateral
hospital that is well equipped. Through strategic alliances with sister organisations, inguinal, femoral or obturator hernia
in Catalonia and Occitanie, a further 15 specialities, comprising facilities for and cholecystectomy. For outpatient
haemodialysis and (soon to be available) for chemotherapy treatments have and ambulatory care, the most common
also been made available. interventions involved ophthalmological
operations, mainly for cataract.
Can cross-border health care help
variety in European collaboration in for France. In France, those agreements
COVID-19 patients and alleviate
health care, social care and public health. are intended to provide a legal framework
pressure on health systems?
These collaborations can provide concrete for the establishment of local cross-border
advantages for EU citizens. The projects health or medico-social cooperation The COVID-19 pandemic has put great
not only address patient mobility but agreements. The aim is to promote the stress on EU Member States’ health
also target workforce mobility, sharing development of cooperation in health or systems, in some cases leading to
of knowledge and infrastructure, medico-social care between France and situations in which acute beds, intensive
emergencies, and joint investment in bordering countries and to ensure better care unit (ICU) beds and workforce
medical infrastructure. access to quality care in border regions by: were not sufficient to meet the surge
in demand for COVID-19-related care.
– guaranteeing continuity of care and
The findings show that most activity During the first wave of the pandemic in
faster recourse to emergency assistance
takes place in central and western Europe the spring of 2020, within a two month
between countries, particularly those – optimising the organisation of the period, almost 300 European COVID-19
with similar welfare traditions (e.g. health care offer and by encouraging patients were treated in another Member
Scandinavian countries), or a shared the sharing of capacities (material and State. Most transfers took place from the
history (e.g. Italy and Slovenia or Italy human resources) French Region of Grand Est, Northern
and Austria). Furthermore, cross border Italy and the Netherlands to Austria,
– encouraging the sharing of knowledge,
collaborations can be aimed at overcoming Germany, Luxembourg and Switzerland
practices, and human and material
gaps in regional provision, which occurs, (see the article by Winkelmann et al. in
resources (see Box 3).
for example, in the cross-border bi- this issue). These transfers were a measure
national hospital of Cerdanya in the of last resort aimed to help countries
These cross-border framework
Pyrenees (see Box 2). and regions on the brink of collapse due
agreements are intended to complement
to capacity shortages. 11 Even though
the measures already provided for by
This type of bilateral cooperation can some of these initiatives were organised
Regulations 883/2004 and 987/2009,
take the form of cross-border framework outside the European frameworks, they
and by Directive 2011/24 EU on cross-
agreements and conventions, as is the case nevertheless serve as a reminder of the
border care. An example is TRISAN,
Eurohealth — Vol.28 | No.1 | 2022Eurohealth 28(1) 55
Box 3: The case of Franco-German cross-border cooperation When the COVID-19 crisis began, cross-border cooperation
before and during the COVID-19 crisis led the ARS Grand-Est and the Prefecture to reinforce their
cooperation and to innovate actions on areas including
France has several cross-border framework agreements that contact tracing and the exchange of practices. Indeed,
allow, at the regional level, the directors of the Regional Health the Grand-Est region was very strongly affected at the
Agencies (Agences Régionales de santé, ARS) to sign local beginning of the crisis in March 2020. Thanks to the solidarity
health cooperation agreements in order to promote patient care provided by neighbouring countries, including Germany,
and the mobility of health professionals in border regions. transfers of patients in intensive care units were organised.
Thus, between 22 March and 5 April 2020, 160 patients
ARS Grand-Est has four framework agreements for health
were transferred from France to neighbouring countries of
cooperation between France and Belgium, Luxembourg,
the Grand-Est Region (Belgium, Luxembourg, Germany,
Switzerland and Germany.
Switzerland) or other EU countries (Austria), of which 74% of
The Franco-German cross-border health cooperation which were transferred to Germany.‡
framework agreement,* covers the border area of the former
In the same spirit, France has offered to receive patients in
regions Alsace and Lorraine regions of the Grand-Est on
intensive care if the health situation so requires.
the one hand, and the German Länders (States) of Baden-
Württemberg, Rhineland-Palatinate and Saarland on the other. Furthermore, in order to consolidate cross-border cooperation
It aims to ensure better access to care for the populations of in light of the lessons learned from the COVID-19 crisis, ARS
the border region, to guarantee continuity of care and faster Grand-Est has proposed to develop a joint cross-border
access to emergency assistance, to optimise the supply of observatory on health data for the border areas § in order to
care and promote the sharing of professional knowledge and facilitate a harmonised exchange between the parties.
practices, and to facilitate crisis management.
On the Franco-German border, with regard to the prospects
Further conventions have also been added in specific areas. offered by the Treaty of Aix,¶ this common desire to work on
For example, the field of cross-border emergency medical strengthening health cooperation would apply particularly to
assistance, is the subject of several conventions between the cross-border living areas that are institutionally embodied
the ARS Grand-Est, the health structures concerned, the by the Eurodistricts.
SAMU (Service d’Aide Médicale Urgente; Emergency medical
service) and fire departments and the neighbouring Länder.†
These specific conventions allow the emergency call centre
responsible for the region to call on the emergency resources
of the neighbouring region to shorten the response time or to
compensate for the temporary unavailability of means. 13
‡ Data from the ARS Grand-Est.
§ Bassins de vie frontaliers.
* Signed in 2005 and entered into force in April 2007. ¶ Treaty between the French Republic and the Federal Republic of Germany on Franco-
† Between Alsace and Rhineland-Palatinate as well as between Alsace and German cooperation and integration, signed on 22 January 2019 and entered into force
Baden-Württemberg both on 10 February 2009. on 22 January 2020.
potential of cross- border care in crisis Cerdanya Hospital between France and there are pending issues that need to be
situations. Countries could explore the Spain cooperates with French hospitals addressed for cross-border health care to
European frameworks better to facilitate to share intensive care capacity and be realised in its full potential:
the continued demand for COVID-19- personnel, working with the border police
related services as well as new demand to ensure access for patients and health ●E
HIC needs improvement: In 2019,
for backlog care (see the article by van professionals. 12 there were close to 250 million EHIC
Ginneken et al.). cards issues amounting only to 53.1%
of insured persons in the EU. The
What needs to be done to reap the full
Furthermore, several countries have been EHIC has also faced some acceptance
potential of cross-border care?
working together, with assistance from problems with health care providers. 2
the EU and its frameworks, in providing Cross-border health care adds value
● Better information for patients and
emergency care for COVID-19 patients for patients in many circumstances. At
health professionals: Patients and
in the Interreg regions. For example, present, there is limited utilisation of
health professionals are not always
the Euregio Meuse-Rhine confronted cross-border care and the budgetary
informed on the options for cross-
with the pandemic set up a trilateral impact is negligible. The European
border health care, even in border
crisis management centre (Task Force Commission is carrying out an evaluation
regions. 14 The expansion of cross-border
Corona)*. Furthermore, the cross- border of the cross-border health care directive
digital services for both patients and
to assess its effects (see Box 4). However,
* The Euregio fosters regional cross-border collaboration professionals will be important.
on all economic, social, and cultural aspects. It was created in
1976, with judicial status achieved in 1991.
Eurohealth — Vol.28 | No.1 | 202256 Eurohealth 28(1)
● Strengthening the evidence base and 5
Nguengang Wakap S, Lambert DM, Olry A, et al.
monitoring of bilateral agreements: Estimating cumulative point prevalence of rare 255
Box 4: Evaluation of the patients’ information on the prevalence and diseases: analysis of the Orphanet database. Eur J
right directive analysis on the effectiveness of
Hum Genet 2020;28(2):165 – 73.
bilateral agreements and a continuous
6
EURORDIS. Survey of the delay in diagnosis for
The European Commission is 8 rare diseases in Europe (‘eurordiscare 2’), 2007.
monitoring would help to provide a
carrying out an evaluation of the Available at: https://www.eurordis.org/sites/default/
stronger evidence base. files/publications/Fact_Sheet_Eurordiscare2.pdf
cross-border health care directive
to assess how the rules are working ●B
etter integrate and support the 7
European Commission. European Reference
(or not working) in the interests of possibility of having bilateral Networks, 2017. Available at: https://ec.europa.eu/
patients. 16 It will focus, in particular, agreements within the European health/ern_fr
on patients access to safe and framework: Similar to the agreements 8
Rare 2030. Foresight in Rare Disease Policy.
high-quality health care in another between France and some of its border Recommendations from the Rare 2030 Foresight
country and how it encourages countries, the measures provided are Study. The future of rare diseases starts today.
2021. Available at: http://download2.eurordis.org/
cooperation between national health already complimented by the regulation
rare2030/Rare2030_recommendations.pdf
care providers, also on rare diseases and the directive mentioned above,
while addressing local issues.
9
Bobek J, Schmidt AE, Bachner F, Röhrling I,
and ERNs. Following an extensive
Seethaler J. Cross-border. Care – Study on
consultation of stakeholders
cross-border cooperation: capitalising on existing
across the EU including national Conclusion initiatives for cooperation in cross-border regions.
and regional authorities, health Main Results, 2018.
Cross-border health care adds value
professionals, health insurers, patient
for patients and helps to provide timely 10
TRISAN web site. Available at: https://www.trisan.
organisations and citizens, its report
access to high quality health care. This org/
is expected to be published in the
may be especially important during the 11
Winkelmann J, Scarpetti G, Hernadez-Quevedo C,
Spring of 2022.
COVID-19 pandemic which has led to van Ginneken E. How do the worst-hit regions
increased demand for COVID-19 care manage COVID-19 patients when they have no spare
capacity left? 23 April 2020. Available at: https://
as well as catch-up care following the
eurohealthobservatory.who.int/monitors/hsrm/
● End financial risk for patients: disruption to routine health services. If we analyses/hsrm/how-do-the-worst-hit-regions-
In many countries, the directive is are to strive towards a European Health manage-covid-19-patients-when-they-have-no-
implemented in a way that discourages Union, we should continue to invest in spare-capacity-left
patients to use it; in particular, it does cross-border health care by improving 12
European Commission. Communication from the
not contain information on tariffs the user-friendliness, providing help for Commission: Guidelines on EU Emergency Assistance
and levels of reimbursement. Patients cross-border collaboration, strengthening on Cross-Border Cooperation in Healthcare related
therefore often prefer to use cross- the ERNs, and further expanding the to the COVID-19 crisis. Available at: https://eur-lex.
europa.eu/legal-content/EN/ TXT/?uri=celex%3A520
border health care under the regulation. cooperation of cross-border regions,
20XC0403%2802%29
Member States, and at European level.
● Improve continuity of care: Cross- 13
France-Germany cooperation agreements
border hand-over and continuity of care (Conventions de coopération France-Allemagne).
remains a difficult task. In general, References Available at: https://www.cleiss.fr/docs/cooperation/
electronic patient records or paper 1
Wismar M, Palm W, Figueras J, Ernst K, Van
cc-france-allemagne.html
records do not travel with the patient Ginneken E. Cross-border health care in the European 14
Beuken JA, Bouwmans ME, Verstegen DM,
or is inadequately acknowledged. 15 Union: mapping and analysing practices and policies. Dolmans DH. Out of sight, out of mind? A qualitative
The EU eHealth network has created Copenhagen: World Health Organization, on behalf study of patients’ perspectives on cross-border
of the European Observatory on Health Systems and healthcare in a European border region. Patient Educ
the MyHealth@EU infrastructure to
Policies, 2011. Couns 2021;104(10):2559 – 64.
facilitate the transfer of medical records
and by 2025 all EU countries are
2
De Wispelaere F, De Smedt L, Pacolet J. 15
Beuken JA, Verstegen DM, Dolmans DH, et al.
Coordination of social security systems at a glance Going the extra mile – cross-border patient handover
expected to be connected.
2020 Statistical Report. European Commission in a European border region: qualitative study of
● Improve user-friendliness: The legal Directorate-General for Employment, Social Affairs healthcare professionals’ perspectives. BMJ quality
and Inclusion, 2021. & safety 2020 ;29(12):980 – 7.
provisions are complicated and deter
potential patients from using cross- 3
Wilson P, Andoulsi I, Wilson C. Member State 16
Cross-border healthcare – evaluation of patients’
border health care. Data on cross-border healthcare following Directive rights web site. Available at: https://ec.europa.
2011/24/EU. European Commission, 2019. eu/info/law/better-regulation/have-your-say/
● Strengthening the ERNs: The 4
initiatives/12844-Cross-border-healthcare-
European Commission. Report from the
ERNs had a promising start. With Commission to the European Parliament and the
evaluation-of-patients%E2%80%99-rights_en
the expansion of the networks and Council on the operation of Directive 2011/24/
the uptake of more patients with EU on the application of patients’ rights in
rare disease in the virtual panel cross-border healthcare. COM(2018) 651 final.
Available at: https://eur-lex.europa.eu/resource.
consultations the question of additional
html?uri=cellar:bc5ac6d2-bd7c-11e8-99ee-
investment in infrastructure and 01aa75ed71a1.0019.02/DOC_1&format=PDF
expertise needs to be answered.
Eurohealth — Vol.28 | No.1 | 2022You can also read