INFECTION PREVENTION AND CONTROL (IPC) IN PEDIATRIC HOME HEALTH CARE 2022 - TENDER CARE PEDIATRIC SERVICES ELLYN E. CAVANAGH, PHD, MN, RN AUGUST, 2022
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Infection Prevention and
Control (IPC) in Pediatric
Home Health Care
2022
Tender Care Pediatric Services
Ellyn E. Cavanagh, PhD, MN, RN
August, 2022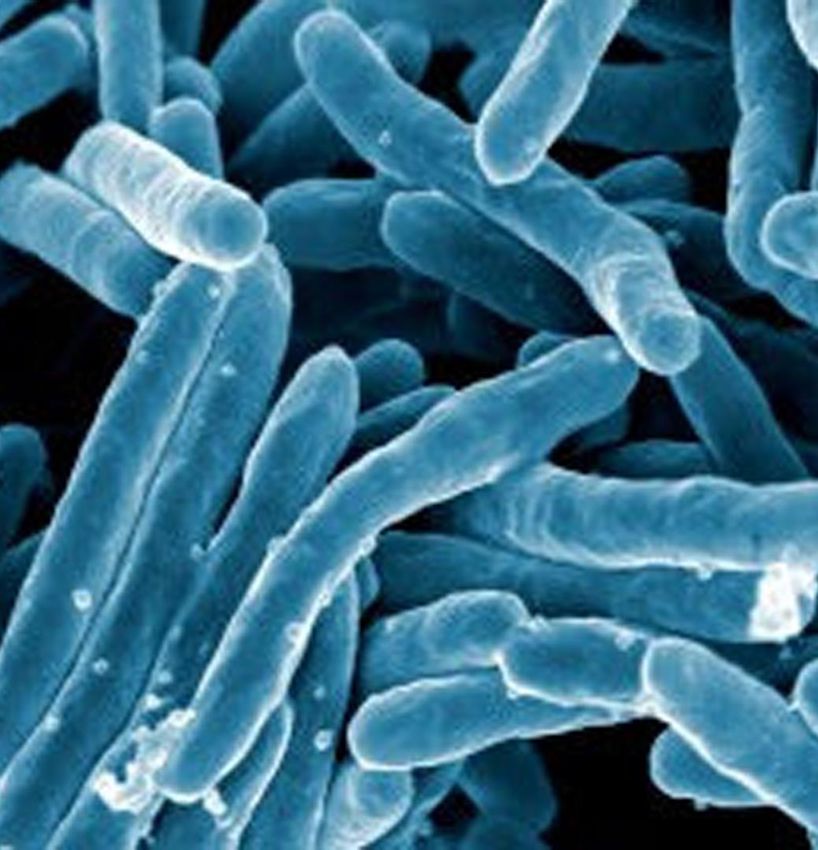
Objectives • Review basics of infection prevention and control (IPC) specific to home health care (HHC). • Provide annual Tuberculosis update. • Review 4 infectious diseases specific to care of Children and Youth with Special Health Care Needs (CYSHCN) : Influenza; Norovirus; Respiratory Syncytial Virus (RSV); Coronavirus. • Review risks for health associated infections. • Review the incidence and symptoms of newly emerging disease, Monkeypox. • Understand the priority of handwashing.

“We Do It for the Kids” • Children and youth with special health care needs (CYSHCN) are defined as those who have or are at increased risk for chronic physical, developmental, behavioral, or emotional conditions and who also require health and related services of a type or amount beyond that required by children generally. • The most important approach to minimizing the risk of infection are mitigation of community transmission and utilizing policies that decrease spread (i.e., handwashing). • Other approaches include promotion of immunization for all eligible CYSHCN, family and community members (and others who come into close contact with CYSHCN), and indoor masking when spread is moderate to high, including universal masking in school.


• Coronaviruses • Norovirus
Infectious •
•
Dengue
Diphtheria
• Pneumococcal
• Polio
Diseases •
•
Ebola
Flu
• Rabies
• Rotavirus
• Hepatitis
• Hib • RSV
• HIV/AIDS • Rubella
• HPV
• Shingles
• Japanese Encephalitis
• Tetanus
• Measles
• Meningococcal • Tuberculosis
• Monkeypox • Whooping Cough
• Mumps • Zika
Tuberculosis • Annual TB testing of health care personnel is not recommended unless there is a known exposure or ongoing transmission at a healthcare facility. • TB education should include information on TB risk factors, the signs and symptoms of TB disease, and TB infection control policies and procedures. • 7,860 reported TB cases in the United States in 2021 (a rate of 2.4 per 100,000 persons) • Up to 13 million people in the United States are living with latent TB infection • During the COVID-19 pandemic, reported TB disease diagnoses fell 20% in 2020 and remained 13% lower in 2021 than pre- pandemic levels.

Tuberculosis (TB) Fast Facts • Tuberculosis is preventable and treatable but remains the world’s deadliest infectious-disease killer. • Caused by Mycobacterium tuberculosis (M. tuberculosis) germs that are spread from person to person through the air. TB usually affects the lungs, but it can also affect other parts of the body, such as the brain, the kidneys, or the spine. • General symptoms of TB disease include feelings of sickness or weakness, weight loss, fever, and night sweats. The symptoms of TB disease of the lungs also include coughing, chest pain, and the coughing up of blood. • TB bacteria are put into the air when a person with TB disease of the lungs or throat coughs, sneezes, speaks, or sings. These germs can stay in the air for several hours, depending on the environment. Persons who breathe in the air containing these TB germs can become infected; this is called latent TB infection.

Is TB Reportable ? • TB is a communicable disease notifiable by law because it has the potential to become a significant epidemic with high transmission rates in some foci. Moreover, there may be a rapid emergence of multidrug-resistant TB (MDR-TB) and extensively drug- resistant TB (XDR-TB) hot spots. • Colorado is classified as a low-incidence state (

How Do You Get Tested for TB? • A skin test or TB blood test. The Mantoux tuberculin skin test is performed by injecting a small amount of fluid (called tuberculin) into the skin in the lower part of the arm. A person given the tuberculin skin test must return within 48 to 72 hours to have a trained health care worker look for a reaction on the arm. Normal results are signified with negative outcome of the test, which is when the bump size is < 5mm. Abnormal results are signified when the outcome is positive when the bump is ≥ 5 mm and the patient is also HIV positive or had an organ transplant or had contact with a tuberculosis patient. • A positive test for TB infection only tells that a person has been infected with TB germs. It does not tell whether or not the person has progressed to TB disease. Other tests, such as a chest x-ray and a sample of sputum, are needed to see whether the person has TB disease.
TB high risk factors
• Persons who have been recently infected with TB bacteria
• Close contacts of a person with infectious TB disease
• Persons who have immigrated from areas of the world with high
rates of TB
• Children less than 5 years of age who have a positive TB test
• Groups with high rates of TB transmission, such as homeless
persons, injection drug users, and persons with HIV infection
• Persons who work or reside with people who are at high risk for
TB in facilities or institutions such as hospitals, homeless shelters,
correctional facilities, nursing homes, and residential homes for
those with HIV
• Persons with medical conditions that weaken the immune system.
• Babies and young children often have weak immune systems.If a child has TB disease, s/he will need to take several
different medicines. This is because there are a lot of
germs to be killed. Taking several medicines will do a
better job of killing all of the germs and preventing them
from becoming resistant to the medicines.
The most common medicines used to cure TB disease
are:
• isoniazid (INH)
TB disease • rifampin (RIF)
• ethambutol
• Pyrazinamide
The course of treatment is long because TB bacteria die
very slowly—it takes at least six months for the medicine
to kill all the TB germs in the child's body. No one likes
long courses of treatment—whether you're taking or
administering—but it's absolutely necessary that it be
completed fully.Annual TB Screening For
Employees
Complete annual TB screening TB Form
(electronic). Use the link below to access the
electronic screening form and follow the
instructions to submit the form to the office.
https://namelyesign.na4.echosign.com/public/esignWidget?wid=C
BFCIBAA3AAABLblqZhCw9GYn7hEb1rvyr4kb7JfKnyPE8ZaGQmhMA-
86v2PJprxryzaOBjoYe899PIjJ5Ek*Influenza Seasonal influenza is an acute respiratory infection caused by influenza viruses which circulate in all parts of the world. It represents a year-round disease burden. It causes illnesses that range in severity and sometimes lead to hospitalization and death. There are 4 types of seasonal influenza viruses, types A, B, C and D. Influenza A and B viruses circulate and cause seasonal epidemics of disease. • Influenza A viruses are further classified into subtypes according to the combinations of the proteins on the surface of the virus. Currently circulating in humans are subtype A(H1N1) and A(H3N2) influenza viruses. The A(H1N1) caused the pandemic in 2009 and subsequently replaced the seasonal influenza A(H1N1) virus which had circulated prior to 2009. Only influenza type A viruses are known to have caused pandemics. • Influenza B viruses are not classified into subtypes. • Influenza C virus is detected less frequently and usually causes mild infections, thus does not present public health importance. • Influenza D viruses primarily affect cattle and are not known to infect or cause illness in people.
Influenza Transmission • Seasonal influenza spreads easily, with rapid transmission in crowded areas including schools. When an infected person coughs or sneezes, droplets containing viruses (infectious droplets) are dispersed into the air and can spread up to one meter, and infect persons in close proximity who breathe these droplets in. • The virus can also be spread by hands contaminated with influenza viruses. To prevent transmission, people should cover their mouth and nose with a tissue when coughing and wash their hands regularly. • Children consistently have the highest attack rates of influenza in the community during seasonal influenza epidemics. • Children and adolescents with certain underlying medical conditions have a high risk of complications from influenza
Diagnosis and Management • Infection of other respiratory viruses (i.e., respiratory syncytial virus) can also present as Influenza-like Illness (ILI) which makes the clinical differentiation of influenza from other pathogens difficult. • Treatment focuses on relieving symptoms of influenza such as fever. • Neuraminidase inhibitors (i.e. oseltamivir) should be prescribed as soon as possible (ideally, within 48 hours following symptom onset) to maximize therapeutic benefits. • Oseltamivir available as a generic version or under the trade name Tamiflu®) is approved for treatment of flu in children 2 weeks old or older.
American Academy of Pediatrics
• Recommends annual influenza immunization of all children without
medical contraindications, starting at 6 months of age. Any
licensed, recommended, age-appropriate vaccine available can be
administered, without preference for one product or formulation
over another.
• Injectable flu vaccines introduce small doses of an inactivated version of the flu virus into the
body so the immune system can develop antibodies that can fight the flu virus. This usually
takes about two weeks to be effective. Since the flu virus changes each year, the flu shot
must be given annually.
• Antiviral treatment of influenza with any licensed, recommended,
age-appropriate influenza antiviral medication is recommended for
children with suspected or confirmed influenza who are
hospitalized, have severe or progressive disease, or have underlying
conditions that increase their risk of complications of influenza.
• https://publications.aap.org/pediatrics/article/148/4/e2021053744
/183303/Recommendations-for-Prevention-and-Control-
of?autologincheck=redirectedRespiratory Syncytial Virus (RSV) Transmission • RSV transmission occurs by coming in contact with infectious material either from another individual or inanimate object. The secretions from the eye, mouth, nose, and possibly from a sneeze contain the virus. The virus can also survive for many hours on inanimate objects such as doorknobs, hard surfaces, and toys. It can also live on human hands for up to 30 minutes. • RSV activity in the United States usually begins in the late fall and extends through spring; peak activity typically occurs in early February, although there can be regional variation. • Annually, RSV disease is estimated to cause 3.4 million hospitalizations and 100,000 deaths globally.
RSV is a common cause of pneumonia and
bronchiolitis—inflamed airways in the lungs.
RSV is a virus, antibiotics do not helpPeople infected with RSV usually show symptoms within 4-6 days after getting
infected. It usually causes mild, cold-like symptoms such as: runny nose
(rhinorrhea), coughing, sneezing, fever, wheezing, and/or decrease in appetite.
In babies, symptoms include irritability, decreased activity, and breathing
difficulties. RSV can be life-threatening, especially for infants and older adults. It is
the most common cause of bronchiolitis and pneumonia – more severe infections
Severity of RSV – in children less than 1 year of age. Primary infection with RSV is generally
exhibited as lower respiratory tract disease, pneumonia, bronchiolitis,
tracheobronchitis, or upper respiratory tract illness.
Two medications are recommended for babies and children at high risk for RSV to
protect them against the serious complications of the illness. This includes
children with weakened immune systems, organ recipients, and premature
infants. These are usually given monthly during the RSV "season" from late fall
through spring.
These medications are not vaccines, and they do not prevent the virus. However,
they do lessen the severity of the illness and may help shorten the hospital stay.Palivizumab (Synagis)
• Palivizumab was licensed in June 1998 by the Food and Drug Administration for
the reduction of serious lower respiratory tract infection caused by respiratory
syncytial virus (RSV) in children at increased risk of severe disease.
• Since that time, the American Academy of Pediatrics has updated its guidance for
the use of palivizumab.
• The AAP supports the use of palivizumab in eligible infants in any region
experiencing rates of RSV activity at any time in 2022 similar to a typical fall-
winter season.
• The AAP recommends initiating the standard administration of palivizumab,
which consists of 5 consecutive monthly doses. This regimen provides serum
levels associated with protection for 6 months, the length of a typical RSV season.
Download the link below for eligible children:
https://synagishcp.com/content/pdfs/SYNAGIS_Commercial_US_Patient%20ID%20K
it%20Eligibility%20Grid.pdfVaccines are available for free at a wide range
of locations. Most insurance companies over
the cost of a flu shot.
Influenza
Vaccine
Availability You can get a flu shot wherever you choose:
doctors’ offices, clinics, grocery stores, drug
stores, county health departments.
Tender Care is not offering flu shots this year.
Please contact human resources if you need
assistance finding a place or time to get one.
970-686-5437Proof of influenza
Submit proof of influenza immunization to the office
Submit
Immunization
by October 31, 2022
Send your record to Alicia Anderson via Tiger
Send Connect, alicaa@tcpskids.com, or in person at the
office.
If you have a medical contraindication or cannot get
Complete a flu shot for other reasons, complete an influenza
declination form instead. Click here for the form.Covid-19 and kids
• 13,911,565 total child COVID-19 cases reported with children representing
about 19 % of all cases.
• While children are as likely to get COVID-19 as adults, kids are less likely to
become severely ill. Up to 50% of children and adolescents might have
COVID-19 with no symptoms.
• AAP recommend COVID-19 vaccination for all children 6 months of age
and older who do not have contraindications. Download the AAP Pediatric
Covid-19 Vaccination Schedule below
https://downloads.aap.org/AAP/PDF/COVID%20Vaccine%20Dosing_Quick
%20Reference.pdf?_ga=2.16559605.2108570033.1658330631-
1771716655.1636469312
Reference https://www.aap.org/en/pages/2019-novel-coronavirus-covid-
19-infections/children-and-covid-19-state-level-data-report/What is Long Covid ? Long COVID — also known as “post-COVID syndrome” and “post-acute sequelae of SARS-CoV-2 infection (PASC)”— is the presence of one or more lingering symptoms that remain long after a child or teenager has recovered from COVID-19. The prevalence of long-COVID in children and adolescents was 25.24%. The five most prevalent clinical manifestations were mood symptoms (16.50%), fatigue (9.66%), sleep disorders (8.42%), headache (7.84%), and respiratory symptoms (7.62%). https://www.thelancet.com/journals/lanchi/article/PIIS2352- 4642(22)00154-7/fulltext
Covid-19 Vaccine and Kids • The AAP recommends that all children and adults who meets criteria, as recommended by the Advisory Committee on Immunization Practices, receive the COVID-19 vaccine. Some adolescents who are immunocompromised may be eligible for an additional primary series dose of the vaccine. All who are eligible are urged to get a booster dose for additional protection. Policy makers should consider the unique needs of CYSHCN, their families/caregivers, educators, therapists and other individuals involved with the care of CYSHCN when making determinations about access to the vaccine. Reference : https://www.aap.org/en/pages/2019-novel- coronavirus-covid-19-infections/clinical-guidance/caring-for- children-and-youth-with-special-health-care-needs-during-the- covid-19-pandemic/
Viral tests, including Nucleic Acid Amplification Tests (NAATs, such as
Reverse Transcription – Polymerase Chain Reaction), antigen tests
and other tests (such as breath tests) are used as diagnostic tests
to detect current infection with SARS-CoV-2 and to inform an
individual’s medical care.
SARS-CoV-2 Viral tests can also be used as screening tests to reduce the transmission of
SARS-CoV-2 by identifying infected persons who need to isolate from others.
Test Types You can order your free test kits for home delivery
https://special.usps.com/testkits
Antibody or serology tests are used to detect previous infection with
SARS-CoV-2 and can aid in the diagnosis of multisystem
inflammatory syndrome in children (MIS-C) and in adults (MIS-A).
CDC does not recommend using antibody testing to diagnose current
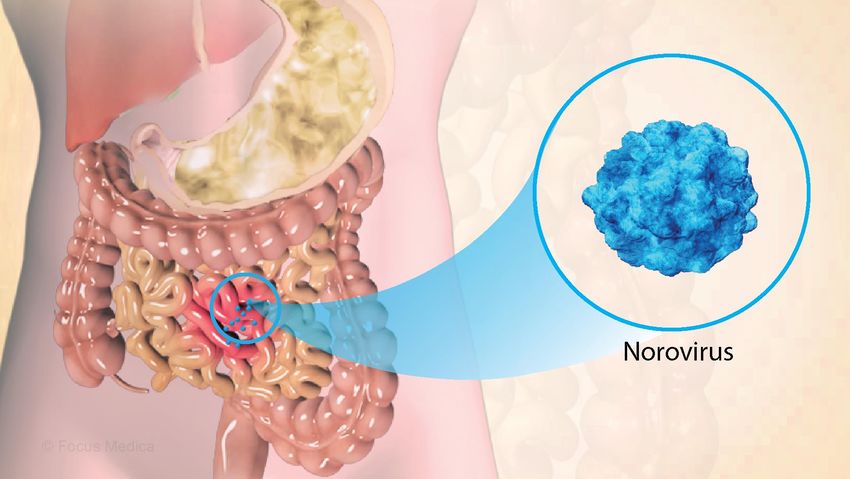
infection.Norovirus
• Outbreaks are common. The virus spreads very easily and quickly
and anyone can acquire norovirus.
• Noroviruses are the leading cause of foodborne illness.
• Norovirus illness is not related to the flu, which is caused by
influenza virus.
• Norovirus spreads:
• From infected people to others
• Through contaminated foods and surfaces
• Outbreaks can happen anytime, but they occur most often from
November to April
• Antibiotics do not help as this is a viral infection.
• Many children with complex medical conditions have significant GI
involvement, and a stomach virus may make that worse. Children
who are already prone to reflux or vomiting may vomit even more;
kids with pre-existing diarrhea or ostomies may see a greater
increase in output.Management of Norovirus
• Transmitted through fecal-oral route
• Wash hands thoroughly and frequently with soap
water.
• Washing hands is critically important. Since the
virus is passed on through fecal matter, being
careful with hygiene and diapering practices can
stop the spread.
• Disinfect contaminated surfaces and objects.
• Flush away any infected stool or vomit in the toilet
• Cleaning up https://youtu.be/TAkH4jakLYAHome Care Management Strategies to increase infection prevention and control
What does Medicaid Require ? • The Centers for Medicare and Medicaid Services has recently updated the Conditions of Participation for HHC to place a greater emphasis on infection control (IC) practices, to ensure they are more in line with other providers, such as hospitals and skilled nursing facilities. • Many infections are preventable through compliance with evidence-based IC strategies. HHC nurses’ compliance with standard precautions, including hand hygiene, adherence to aseptic techniques, and use of personal protective equipment (including gloves, gowns, masks, eye protection, and face shields), can be instrumental in preventing the spread of infections among patients and providers.
Basics • Keep hands clean by washing thoroughly with soap and water. Hands should be wet with water and plain soap and be rubbed together for 15 to 30 seconds. Special attention should be paid to the fingernails, between the fingers, and the wrists. Hands should be rinsed thoroughly and dried with a single-use towel (eg, paper towels). • Alcohol-based hand sanitizers are a good alternative for disinfecting hands if a sink is not available. Hand sanitizers should be rubbed over the entire surface of hands, fingers, and wrists until dry and may be used several times. Hand sanitizers are available as a liquid or wipe in small, portable sizes that are easy to carry in a pocket or attached to equipment. When a sink is available, visibly soiled hands should be washed with soap and water. • Keep cuts and scrapes clean, dry, and covered with a bandage until healed.
Handwashing • Keeping hands clean can prevent 1 in 3 diarrheal illnesses and 1 in 5 respiratory infections, such as a cold or the flu. • Soap and water are more effective than hand sanitizers at removing certain kinds of germs like norovirus, Cryptosporidium, and Clostridioides difficile, as well as chemicals. • Hand sanitizers also may not remove harmful chemicals, such as pesticides and heavy metals like lead. • Do not touch your eyes, nose, or mouth without washing your hands first (Soap and water and disinfectants easily inactivate viruses)
Infection Control Measures • Use a tissue to cover the mouth when sneezing or coughing. Used tissues should be disposed of promptly. Sneezing/coughing into the sleeve of one's clothing (at the inner elbow) is another means of containing sprays of saliva and secretions and has the advantage of not contaminating the hands. • Use disinfectant (antimicrobial cleaning agent) on surfaces (i.e., counters, doorknobs, phones, computer keyboards) can help to reduce or eliminate bacteria.
Face Masks • The appropriate use of face masks should be prioritized 1) when unvaccinated individuals are present, particularly children who are not eligible for the SARS- CoV-2 vaccine, 2) when environmental exposure risk is elevated with crowds, closed spaces and close contacts, particularly in the setting of high community transmission, and 3) in homes and especially in the same room with other household members or visitors when intrahousehold spread is an increased concern. • Families can promote the practice of facemask use at home to enable CYSHCN to become accustomed to situations where face masks are more necessary.
Environmental Cleaning • Hand-touch surfaces that may come in contact with child should be wiped clean by detergent solution and allowed to dry. • Surfaces may be disinfected according to home health care plan. • Wipe classroom surfaces and any items that are shared among students. • At school, wash your hands frequently and encourages child’s friends to wash their hands as well.
N95 Masks • Close contacts should have access to appropriately fitted N95 respirators and eye protection for aerosol-generating procedures (ie, airway suctioning, airway clearance procedures, tracheostomy changes, noninvasive ventilation, manual ventilation and nebulizer treatments). • In some situations, child use of an appropriately sized face shield may help protect contacts.
Tracheostomy Risk • Children with tracheostomy may not be able to cough and clear the airway as well as others, which could increase the risk of infection with a respiratory virus. • Children with tracheostomy breathe differently than an individual without a tracheostomy. The airflow is mostly directed in and out of the tracheostomy tube. • Coughing is also redirected out of the tracheostomy tube. Since the tracheostomy tube is located below the level of the vocal folds, children with tracheostomy often have a weaker cough than an individual without a tracheostomy. • The aerosols generated from the cough may then actually be less than aerosols generated by coughing by someone without a tracheostomy tube.
Risk for Covid-19 There is no evidence that children with tracheostomy are at any increased risk of contracting or transmitting Covid-19. There are evolving recommendations for PPE as the prevalence rates of Covid-19 reduce in certain communities. Allowing for less restrictive PPE for procedures such as suctioning for communities with a low prevalence rate of Covid-19 for children with negative testing or low risk, can allow for children with tracheostomy to get back to schools. However, PPE should still be worn. Emergency plans should be in place with hospital specialists to provide information about what to do in an emergency.
Additional
Precautions
Arrange separate areas
for aerosol-generating
procedures (ie bi-level airway
pressure ventilation (BiPAP),
Continuous positive airway
pressure ventilation (CPAP), and
respiratory tract suctioning (not
including oro-pharynx suctioning).
Aerosol-generating means that
these devices or procedures may
release particles into the air that
contain COVID-19, which can be
breathed in by others or land and
contaminate surfaces.If child uses a nebulizer or ventilator • Using these presents a risk because the air is typically at a higher pressure and humidify. • If child is not sick with COVID-19, there is no risk of spread. • If child DOES have COVID-19, performing these procedures may make it more likely that COVID-19 will spread to other family members or nurses in the home. In addition, if another family member or friend also requires one or more of these procedures, that individual may spread COVID-19 to the child.
Recommendations for Use of Respiratory Equipment • Keep children with trachs, vents, oxygen, and other respiratory equipment at home during the course of the pandemic, primarily for their own safety, but also to minimize spread. • If you must take the child to a medical clinic or other public place, it is best not to perform procedures such as neb treatments, suctioning, or cough assistance in public, especially if you suspect the child might be sick. Alternatives include bringing the child back to the car or home for procedures or asking the hospital or clinic if there is a separate room (a negative-pressure room is preferred) child can use for procedures. • When at home, perform procedures such as trach changes, cough assistance, suctioning, and nebulizer treatments in a separate room with a closed door whenever possible. • Use personal protection equipment, such as mask and gloves, during procedures. https://journal.chestnet.org/article/S0012-3692(20)31639- 1/fulltext?_ga=2.17280570.2088753115.1605032374-1994087558.1605032374
Healthcare Associated Infection (HAI) • A healthcare associated infection (HAI) is an infection that develops in a patient who is cared for in any setting in which healthcare is delivered (e.g., acute care hospital, chronic care facility, ambulatory clinic, dialysis center, surgicenter, home) and is related to receiving health care (i.e., was not incubating or present at the time healthcare was provided). • In ambulatory and home settings, HAI applies to any infection that is associated with a medical or surgical intervention. Since the geographic location of infection acquisition is often uncertain, the infection is considered to be healthcare associated, rather than healthcare acquired.
Risk factors for HAI
The predominant risk factor for a HAI is the presence of a medical
device (i.e., tracheostomy). Additionally, 20% of home health care
patients require wound management.
Children are at risk of chronic pressure injuries if the s/he:
• Is nutritionally compromised
• Has a tracheostomy (trach site wounds)
• Has peristomal skin breakdown at enteral tube sites (gastrostomy and
jejunostomy)
• Is immobile
• Has neuropathic conditions
• Uses multiple medical devices
• Has poor oxygen perfusion
• Has incontinent associated dermatitis
• Is exposed to excess moisture on the skinMonkeypox (May, 2022) • The U.S. has confirmed the first two cases of monkeypox in children, Centers for Disease Control Prevention and Control (CDC) . Both are "likely the result of household transmission. Currently 2,593 cases of monkeypox in the U.S. ( July 23, 2022 ) • After infection, there is an incubation period of roughly 1-2 weeks. The development of initial symptoms (e.g., fever, malaise, headache, weakness, etc.) marks the beginning of the prodromal period. • A feature that distinguishes infection with monkeypox from that of smallpox is the development of swollen lymph nodes (lymphadenopathy). Swelling of the lymph nodes may be generalized (involving many different locations on the body) or localized to several areas (e.g., neck and armpit). • Shortly after the prodrome, a rash appears. Lesions typically begin to develop simultaneously and evolve together on any given part of the body. The evolution of lesions progresses through four stages—macular, papular, vesicular, to pustular— before scabbing over and resolving. https://www.cdc.gov/poxvirus/monkeypox/response/2022/index.html
Barriers to Infection Prevention • Clutter • Dirty environment • Limited availability of some IPC supplies including personal protective equipment. • Nurses’ reports of feeling rushed or spending additional time to complete care tasks Reference : https://www.ncbi.nlm.nih.gov/p mc/articles/PMC8093314/
Some IPC Barriers in Home Health Care • Unsanitary conditions are a special concern, since the spread of infectious disease within the household is well documented. • One household area of potential concern in this regard is the bathroom. Bathroom surfaces must not be used for other purposes such as cleaning enteral feeding tubes. • Dirty kitchen surfaces, rags, sponges, mops, etc., are potential sources of cross contamination and can spread disease causing microorganisms in the home care setting. Clean surfaces must be available for feeding and medication preparation. • No access to personal protective gear such as gowns. • No access to other protective gear, such as eye goggles, gloves and face masks. • Poor ventilation in child’s bedroom or space where majority of caregiving is done.
Supplies provided by Tender Care • Face masks – surgical and N-95 • Face shields • Goggles • Disposable gloves in small, medium and large • Hand sanitizer • Disposable gowns • Sharps containers • Disposable wipes • Alcohol wipes
Feedback ? • Contact your Case Manager about any concerns related to Infection Prevention, especially if you identify barriers (i.e., PPE supplies, environmental cleaning) • If you have any suggestions for improvement, please notify Leadership Team with your ideas.
References • Centers for Medicare & Medicaid Services (CMS), HHS. Medicare and medicaid program: conditions of participation for Home Health Agencies. Final rule. Fed Regist. 2017;82:4504. [PubMed] • McDonald MV, Brickner C, Russell D, et al. Observation of hand hygiene practices in home health care. [e-pub ahead of print]. J Am Med Dir Assoc. 2020. 10.1016/j.jamda.2020.07.031, accessed November 9, 2020. [PMC free article] • Russell D, Dowding DW, McDonald MV, et al. Factors for compliance with infection control practices in home healthcare: findings from a survey of nurses' knowledge and attitudes toward infection control. Am J Infect Control. 2018;46:1211–1217. [PMC free article] • Shang J, Larson E, Liu J, Stone P. Infection in home health care: results from national outcome and assessment information set data. Am J Infect Control. 2015;43:454–459. [PMC free article] [PubMed] [Google Scholar
Resources Overview of testing for SARS-CoV-2 https://www.cdc.gov/coronavirus/2019- ncov/hcp/testing-overview.html • https://covid19.colorado.gov/covid-19-resources-for-health-care-providers-and-lphas Home modifications to increase ventilation • https://www.epa.gov/coronavirus/how-can-i-increase-ventilation-home-help-protect- my-family-covid-19 Infection control within the home https://www.ahrq.gov/downloads/pub/advances2/vol1/advances-gershon_88.pdf
Diseases Tuberculosis https://www.cdc.gov/tb/topic/testing/healthcareworkers.htm#:~:text=All%20health%20care%20personn el%20with,after%20the%20last%20known%20exposure. TB Centers for excellence and Training https://www.cdc.gov/tb/education/tb_coe/default.htm Norovirus https://www.cdc.gov/norovirus/index.html Respiratory Syncitial Virus (RSV) https://www.cdc.gov/rsv/about/transmission.html Monkeypox https://www.who.int/emergencies/situations/monkeypox-oubreak-2022
Covid-19 Tracheostomy and Ventilated Children and Covid-19 https://www.tracheostomyeducation.com/children-with-tracheostomy-and-covid-19/ AAP Guidelines https://covid.cdc.gov/covid-data-tracker/#new-hospital-admissions. CMS Covid-19 Vaccine Information for Children and Teens https://www.cdc.gov/coronavirus/2019-ncov/index.html Current Pediatric Covid-19 Vaccine Statistics https://www.cdc.gov/mmwr/volumes/71/wr/mm7126a3.htm?s_cid=mm7126a3_e&ACSTrackingID=USCDC_921- DM85107&ACSTrackingLabel=This%20Week%20in%20MMWR%20-%20Vol.%2071%2C%20July%201%2C%202022&deliveryName=USCDC_921-DM85107 Moderna https://www.fda.gov/media/144636/download Pfizer https://www.fda.gov/media/150386/download
You can also read