HEALTHCARE CLAIMS PAYMENT OPTIMIZATION: 7 THINGS TO CONSIDER
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
HEALTHCARE CLAIMS PAYMENT OPTIMIZATION:
7 THINGS TO CONSIDER
Executive Summary
START
In the game of healthcare
payments, the idea is
not to spin perpetually
Provider requests
around the board, but ACH CCD+
to land on the finish
line in the least costly
and most effective way
possible. But too many
healthcare payers are
simply “rolling the dice” on
these outcomes instead
of making calculated,
analytical decisions on
what the best mix of
payment options should
be for them and their
providers. Illustrated by
a board game, this paper
ACH CCD+ Virtual Check
Card
presents a methodology
to determine an optimal
healthcare payment Payment Payment Payment
SH
SH
SH
mix that depicts logical
FI FI FI
NI
NI
branches where payment NI
by check, Virtual Card,
or Automated Clearing
House (ACH) is specified by quantitative criteria measured against objective thresholds. The analysis considers
industry regulation, readiness, adoption concerns, benefits, costs and complexity that maximizes the mutual benefit of
healthcare buyers and suppliers.
HEALTHHealthcare Claims Payment Optimization: 7 Things to Consider
THE HEALTHCARE PAYMENTS GAME
The current pace of change in healthcare and in healthcare payments is unprecedented. The general drive to cut costs, while complying
with Affordable Care Act (ACA) operating rules is altering the healthcare payments landscape. As of January 1st, 2014, when healthcare
providers request it, payers must use the ACH CCD+ (Cash Concentration or Disbursement) format. This is the standard mandated by ACA
operating rules, enabling re-association of the EFT (Electronic Funds Transfer) and the ERA (Electronic Remittance Advice).
While ACH is an efficient, reliable payment method, the majority of healthcare payments are still made via check with the use of Virtual
Cards is increasing. All three methods will continue to be part of the payment mix for the foreseeable future. In fact, an optimal strategy
will employ all three payment methods. The key is knowing when to employ each. Ultimately, the payment method should be mutually
agreed upon by and mutually beneficial to healthcare trading partners.
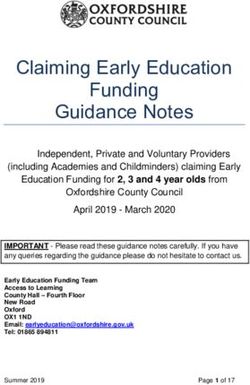
Currently, as a percentage of payments,
checks dominate. 64% Healthcare Other Industries
Small providers will have the most difficulty
moving away from receiving checks. As
ACH and Virtual Card payments increase,
59%
check acceptance will decline, even for small
providers.
With multiple payment options, how can
healthcare payers determine their optimal
payment mix? To keep it interesting, let’s
visualize the process using the analogy of
a good old-fashioned board game. Games 22%
14%
like Monopoly and Life taught us that our
14% 6% 13%
decisions impact our financial success. 9%
Real-life payment decisions are a bit more
Checks ACH Wires P-Cards
complicated, but ultimately the goal should
be to minimize cost, maximize process Paystream Advisors, Healthcare ePayables, Curing Inefficiencies in the Healthcare Payments Market, Q2 2013.
efficiency, and have a positive impact on
payer-provider relationships. So let’s look Small U.S. Healthcare Commercial Remittance
at one example payment game-plan, with Transactions by Payment Type, 2012 to e2016
particular emphasis on the decision points on (in millions of transactions)
the game board.
First, as a foundation, it will help to discuss 443
371 387
the pros and cons of each payment method 360 349
in the context of industry goals, regulation,
and preparedness. Then we will be in a good 316 323 343 335 318
position to consider the details of creating a
payment strategy and selecting a payment
method mix.
124 137 150
103 113
e2012 e2013 e2014 e2015 e2016
Paper check ACH Payment card
Aite Group, Healthcare Remittance Payments: Sizing the Small-Provider Market, March 12, 2013.
HEALTH 2Healthcare Claims Payment Optimization: 7 Things to Consider
PROS AND CONS OF PAYMENT METHODS
Check
Increasingly, checks are viewed as an outdated payment method: Inefficient. Expensive. Not green. But here’s what checks have going for
them: they work and people know how to use them.
Check Pros Check Cons
Universally Accepted: de-facto default payment Slow: time for printing, mailing, transit, deposit, and posting.
method.
Less Secure: prone to fraud, and payment not assured.
Technology: no specialized equipment or expertise
is required. Expensive: most costly payment method for payers and
providers.
Inefficient: processing checks is manual, time consuming, and
costly for payers and providers.
ACH
ACH is known to be reliable, efficient, and cost effective, but considerable administrative and technical investment may be required for
some providers to see these benefits.
ACH Pros Cost of Implementation: the payer must be able to provide the
right data in the right format, and the provider must be able to
Efficient: can enable full electronic (straight through) consume it, re-associate it, and make sense of it. IT resources,
processing when systems and trading partners are testing, and project administration should be considered
fully configured to implement and take advantage of when evaluating costs.
the ACH CCD+ format.
Competing Priorities: ICD-10 code standardization1 and other
Reliable: ACH has been around for years and, once mandates may make implementation impractical.
implemented, is highly reliable.
Enrollment: campaigns to sign up trading partners require
Cost Effective: transaction fees vary, but are resourcing and investment and need concerted, sustained
generally low. effort. Suppliers may be reluctant.
ACH Cons Financial Privacy: providers must be willing to share banking
information, which payers and providers must store and
Not Free: the provider’s bank may charge fees to update.
provide ACH CCD+ healthcare data.
1
Electronic Health Records (EHR) Meaningful Use
3 HEALTHHealthcare Claims Payment Optimization: 7 Things to Consider
Virtual Cards
Virtual Cards are widely accepted, precise, and fraud-resistant. However, the cost of acceptance may be a point of resistance for some
providers. Virtual Card payments have been around for 15 years, but are a relatively new, growing payment method in healthcare.
Providers are presented with credit card information (including card number, expiration date, and security code), which they enter
through their Point of Sale (POS) system. Funds are settled through the credit card network, and data necessary for
re-association is provided with the remittance.
Virtual Card Pros Remittance Detail: Virtual Card payments created
through most banks and clearinghouses can include
Ease of Acceptance: with Virtual Cards, it is not necessary robust remittance data appended including the TRN.
to enroll providers to accept payment; over 600,000 US This detail can include the entire 835 which can be
healthcare providers already accept credit cards. confirmed like ACH.
Ease of Implementation: Virtual Cards may be an especially Virtual Card Cons
good alternative when payers and providers want to move
away from check but are not ready for payment modes Cost of Acceptance: the provider pays a merchant
that require implementation resources. No new processes, discount fee to accept Virtual Cards. This can be
technology, or cost is involved. lowered by bundling transactions or depositing credit
card funds directly into the provider’s account. For
Funds Availability: this method offers the quickest infrequent or small payments, Virtual Card payments
availability of funds for providers, and funds are guaranteed. are often less expensive than other payment modes,
considering the process efficiencies and low cost of
Float: because the credit card issuer extends payment implementation.
terms, Virtual Cards offer cash flow advantages for payers
compared to other payment modes.
Risk: to minimize fraud and misuse, payments can be locked
down to only medical providers and have check-like controls
to manage down to the penny. No banking information
needs to be exchanged and maintained, reducing the
chance of data compromise.
HEALTH 4Healthcare Claims Payment Optimization: 7 Things to Consider
Considering the pros and cons of each payment method, payers need to involve providers in a mutually agreeable decision regarding
the payment method. The provider might want ACH but not have the resources to do the work to reap the benefits of ACH. On the other
hand, the payer might want to use Virtual Cards, but the provider may not think the benefits are worth the cost of acceptance. What’s
needed is a solution that is flexible enough to match each payer-provider scenario. Increasingly, this solution includes multiple payment
modes. Each payer (or game player), and situation, is unique and requires a unique payment solution.
A HEALTHCARE PAYER DECISION SUPPORT MODEL
Payer Perspective
It stands to reason that each payer plays the game differently. Each payer’s strategy is distinct, informed by its payment objectives and
paper reduction goals, while considering existing and future provider relationships.
In our example game, let’s consider a medium-sized payer, such as a regional health plan, or larger TPA (Third-Party Administrator).
Payments are made to a wide variety of healthcare providers, from single-physician practices to large hospital networks. Like most
healthcare payment scenarios, a majority of the payment dollar volume goes to the large providers (the classic 80/20 rule). However,
in terms of sheer quantities, most payments are smaller, going to a fragmented supplier base. A minority of payments are non-HIPAA-
related, such as for workers’ compensation or other non-HIPAA-covered entities such as payments to chiropractors.
In this example, the strategy is to target high-frequency, high-share payers for ACH (which has long-run cost advantages to providers,
after non-trivial start-up costs). Others will be targeted with Virtual Cards. Check is the last-resort, as the most expensive, least efficient
option. This example uses an “opt-in” strategy. That is, providers are given the option to select which payment mode makes the most
sense for them, potentially in consultation with the payer. Opt-in strategies confer a higher level of provider choice (with high regard
for payer-provider relationships). Alternate approaches may employ “opt-out” strategies with providers; that is, designating and
communicating a preferred payment mechanism, and requiring providers to actively disagree and request an alternate payment method.
Our example maximizes the benefit of each payment type, while actively discouraging costly, manual, less secure check payments.
Provider Perspective
A winning strategy in any game considers the other players and their likely responses to your moves. After all, the game isn’t played in
a vacuum. The board-game analogy may be somewhat unrealistic here because, in an efficient market, we want our fellow players to
succeed. After all, we can’t play the game alone. So we look for mutually beneficial (win-win) outcomes. How should we consider our
providers’ perspectives? The decision criteria below strongly consider the provider’s perspective—the provider needs to see benefit to be
willing and able to cooperate.
THINGS TO CONSIDER IN IMPLEMENTING A PAYMENT STRATEGY
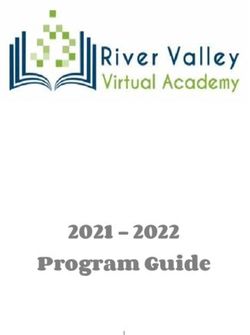
Each payer’s considerations and priorities can be depicted as a decision tree (or a game board), which can visually represent specific
decision nodes, payment criteria, decision thresholds, and optimal payment outcomes. Threshold decision values in our example are for
purposes of example only and will vary according to payer objectives. Other variables, such as average payment size, may also contribute
to the payment-type decision.
5 HEALTHHealthcare Claims Payment Optimization: 7 Things to Consider
START
Provider requests
ACH CCD+
Providers
considering ACH
Consider acceptance should
consult their bank
Fees about additional
charges
Need to
enroll pa
yers
Payer’s % Upgraded ACH
acceptance to
Recurring Payment HIGH
contribution meet ACA
requirements is
payment frquency >15% to provider timely
LOW
revenueHealthcare Claims Payment Optimization: 7 Things to Consider
1) Provider Request
Let’s ease into the game with a decision that’s really a no-brainer. If providers ask for ACH CCD+ payment, by law, payment needs to
be provided in that format. In this case, go directly to ACH CCD+; do not pass go. Hopefully, the payer is ready. However, if providers
don’t request ACH payment, the decision should be based on a conversation between trading partners, considering the factors that
follow, including payment specifics and respective levels of readiness.
2) Recurring Payment
It may be impractical to have conversations with all trading partners, especially with many smaller,
infrequently paid providers. So how do we approach these situations? First off, if the payment is not
recurring, ACH setup and enrollment will not have a high return and will not be worth it for either
Recurring
trading partner.
payment
3) Frequency of Payment
We’re not just playing for fun. We need some discipline to
increase our odds of winning. We need some “game-logic” to For infrequent or
small payments,
direct us. Of the total number of payments, what percentage virtual card
payments are
of payments does each provider represent? If it’s a relatively cheaper than ACH
or check
Payment HIGH low percentage, the communication and administrative
frquency >15%
setup required for ACH will not make economic sense to the
payer or provider. We need a threshold. Let’s say 15 percent.
LOW If more than 15 percent of payments go to the provider, we should encourage themHealthcare Claims Payment Optimization: 7 Things to Consider
So again let’s draw a line in the sand. If the payer contributes more than 10 percent of the provider’s claims revenue, we will put them
on the track to ACH (if the provider can accept ACH payment). If not, we need to consider more decision criteria. As with frequency of
payment, the threshold for percentage contribution should be based on the payer’s differential cost/benefit of moving to Virtual Cards
versus ACH. The payer should also model providers’ cost/benefit in transactions with payers like us (as a proxy for their incentive to invest
in payment methods).
5) Average Size of Payment
So far, we’ve set up the game-board on two major tracks, pointing towards ACH or Virtual Cards. If certain well-designed thresholds (high
frequency of payments, high percentage contribution to provider claims revenue) are met, then the provider is on a track towards ACH.
Otherwise, Virtual Cards are a good option. But remember this model is collaborative (win-win), using an opt-in strategy that has high
regard for provider choice.
We haven’t added them to this game scenario for simplicity, but it might be worth considering other financial metrics on the game board.
For example, a threshold for the average size of the payment can be set in a way similar to payment frequency and revenue contribution.
With average payment size, payers should consider that with Virtual Card acceptance fees to the provider are generally proportional to
the transaction size. However, this is mitigated when providers can take advantage of special lower merchant discount rates for very large
payments, or when multiple payments to the same provider can be aggregated, without sacrificing 835 re-association. Also, Virtual Card
payments deposited directly into provider accounts can qualify for a lower merchant discount rate, which also can be modeled. Payment
size probably overlaps with the previously discussed decision thresholds in that there is a usually a strong correlation between the size of
the provider, frequency of payment, revenue contribution, and average size of payment. In other words, payment size may act as a proxy
for the previous decision thresholds, simplifying the game board.
6) Is your Provider Ready and willing for ACH-CCD+ payment?
On the high frequency, high contribution track, if the provider is willing and able to accept ACH CCD+ payment, great! Move your game
piece to the last space on the board—the payer and
provider are happy.
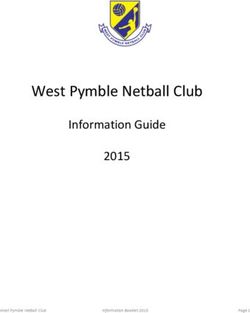
Payment Frequency
On the lower frequency, low contribution, Virtual Card
track, it makes sense to assume the provider will be Low High
more likely to accept Virtual Cards. But since this is a
collaborative game, let’s ask them if they’re ready. Based Virtual Card Virtual Card
on a Black Book 2012 user survey, 86 percent of provider
Low Payment or
business managers are certain their practice management or ACH
Check
and revenue cycle systems cannot accommodate Payer’s %
upcoming regulatory requirements and updates. Nearly
100 percent stated the practice’s financial software and revenue
workflows are unprepared for ACA participation. The contribution
provider may not have the capability to benefit from the Virtual Card
ACH-CCD+ standard; this may especially affect smaller High or ACH ACH
providers who (remembering the 80/20 rule) receive the
majority of the payments in terms of quantity.
Another potential barrier is that the provider may not
agree to supply its banking information. The provider
needs to set up their account to accept credits and debits from the payer, and the provider and payer need to store and update bank
account information.
HEALTH 8Healthcare Claims Payment Optimization: 7 Things to Consider
Additionally, the provider or payer might not have the capability to mount ACH enrollment campaigns. Remember one of the
benefits of Virtual Cards is that it is not necessary to ensure that the provider’s account is properly set up to accept payment—
nearly all providers already accept credit cards, without new processes, cost, or technology. It is easy to create and accept
payments. No provider enrollment is required.
What if providers are not ready, or willing to accept ACH payment, and also do not opt-in to Virtual Card payments? While some
strategies may employ a more aggressive approach, in this scenario, the last-resort default option is check. For very infrequent,
low-volume payments to small providers, the effort to coerce them to move away from checks just may not be worthwhile. For
higher-volume providers, negotiation may be practical.
7) Payments to Non-HIPAA Covered Entities
Payment via ACH may be impractical for certain non-HIPAA covered activities, including workers’ compensation, property and
casualty, and payments to non-HIPAA service providers. These organizations may not be prepared to accept payment detail in
the CCD+ standard or may not want it, as it is not mandated. Small, non-covered entities would probably prefer to accept credit
card payment and collect remittance detail via a means other than CCD+ re-associated with electronic 835.
CAN THE PAYER COMPLY WITH EFT & ERA OPERATING RULE IMPLEMENTATION?
Hopefully the answer is yes. If providers ask for ACH CCD+ payment, by law the payer needs to provide it. But if providers don’t
request it, the decision should be based well-constructed decision thresholds, and if warranted, conversations between trading
partners, considering economics and respective levels of readiness. Even providers that wish to accept and integrate the new
ACH CCD+ format may not be able to do so immediately; in which case, Virtual Card acceptance offers an easy, quick solution
to reduce paper and increase data and remittance availability, without the investment in advanced payment and payment
acceptance capabilities. Regardless, it’s probable that checks won’t disappear immediately, and Virtual Cards and ACH will
continue to support choice and provide flexibility in a collaborative market. The key is to optimize the mix based on rational,
objective criteria.
ABOUT WEX HEALTH
WEX simplifies the application of electronic payments for complex transactions with a seamless interface into healthcare
insurers’ existing claims processing systems. The WEX Health solution passes information between your operational software
and our payment system to create single-use, virtual accounts for provider payment. We support multiple virtual payment types
and offer a range of healthcare-specific features that address even the most complex payment scenarios.
Find out more at http://www.wexinc.com/wex-health.
9 HEALTHYou can also read