Graduate Medical Education (GME) Policy - Mark D Schwartz, MD NYU Grossman School of Medicine LEAHP Program 2021-6-2 - Society of General Internal ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Graduate Medical Education
(GME) Policy
Mark D Schwartz, MD
NYU Grossman School of Medicine
LEAHP Program 2021-6-2
https://www.nap.edu/read/18754/
Sunday, Dec 19, 2021
Congress Debates Federal Subsidies for
Graduate Education for Pre-K Teachers
Need more teachers for universal pre-k
for 3 and 4-year-olds recently passed in
the American Families Act of 2021.
• 0.25% increase in payroll tax
proposed
http://savegme.org

GME policy is a microcosm of US health care policy… “…where professional associations, including the Association of American Medical Colleges, the American Hospital Association, and the Council of Teaching Hospitals, have lobbied Congress and state legislatures to use an outmoded formula to give $20 billion annually to their members, leveraging national catastrophes into an opportunity to ask for more GME funding and raising the specter of “unintended consequences” to derail GME reform that would be in the public’s interest, including a reform proposal from the National Academy of Medicine.” Grischkan J, et. al. Moving the Financing of GME Into the 21st Century. JAMA 2020.
15.8% Increase
20132018
Vs. 1997 BBA: GME cap (~100k)
• For each hospital at 1996 level
• Increased by ~30% since then
Chen C, et.al. JAMA Intern Med 2020;180(1):148–150.
doi:10.1001/jamainternmed.2019.4429
+ 20%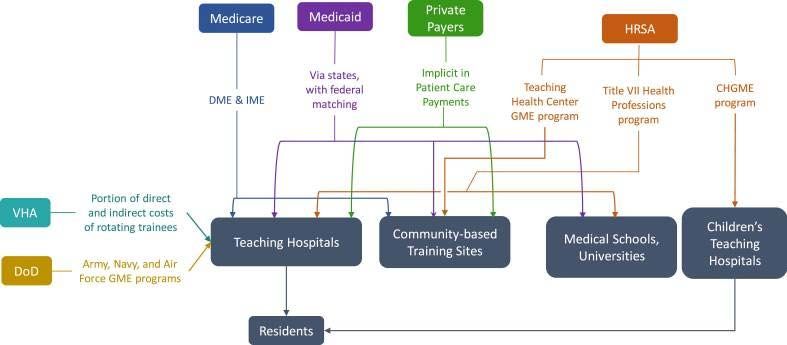
Core Policy Questions
• Is GME a public good or a hospital cost?
– Should American taxpayers subsidize the cost of GME?
• Should (How) Medicare GME shape the physician workforce?
– If GME is a public good, what role should the public have in shaping
the outcome?
US Graduate Medical Education
• GME in the US is the envy of the world, graduating >100,000
new physicians for practice annually
• However, there is broad consensus* that current GME policy
and practice are not well aligned with the needs of the US
healthcare system in the 21st century
*Inglehart JK. Financing Graduate Medical Education — Mounting
Pressure for Reform. N Engl J Med 2012; 366:1562-1563.
GME Policy Problems • Poor alignment of GME funding policy and US workforce needs • Inadequate accountability by hospitals and GME programs for outcomes • No transparency regarding use of funds by hospitals • Inadequate curricular focus on competencies needed for healthcare reform

GME Policy History
• Pre 1965, GME was responsibility of hospitals
• Medicare’s founders debated its role in funding GME
– Congress concluded that it was inappropriate to pay for
these training costs with funds intended for health careReagan: “Nothing is as permanent as a
temporary government program”
• Congress reluctantly and temporarily decided Medicare
would pay its share
– GME enhances value of patient care
• Subsequent commissions concluded:
– “It is inappropriate to pay for GME through Medicare”
• Medicare GME funding is now securely ensconced in the
Medicare trust fund and has grown
– 1984: GME incorporated into Medicare’s Inpatient Prospective
Payment System (IPPS)• 1,100 (26%) teaching hospitals in the US
• 375 of the largest - Council of Teaching Hospitals and Health Systems (COTH)
• Train about 75% of residents yearly and provide >40% of all hospital charity care
eHealth, 2019JAMA. 2017;317(20):2105-2113. doi:10.1001/jama.2017.5702
Sources of Public GME Financing
Billions of Dollars (~$20B in 2018)
DoD, 0.02
THC
Child GME
Title 7 HRSA,
1.8
VA, 1.8
Medicaid, 4.2 Medicare, 12.5
CRS Report, 2018Follow the Money
He K. Graduate medical education funding mechanisms,
challenges, and solutions. Am J Surg. 2021;221(1):65-71.Stewardship of Medical Education
Medicare GME Finance Policy: Direct and Indirect
• Since 1984, GME funding has been split into
– Direct (DGME) and Indirect (IME) payments
• DGME:
– Subsidizes costs of resident and faculty salary/benefits, and administrative
costs
• IME:
– percentage added on to the usual DRG payment to hospitals to account for
the higher costs incurred by teaching hospitals that care for sicker patients
and inefficiencies of care by traineeshttps://fas.org/sgp/crs/misc/R44376.pdf
DGME = # Residents * PRA($) * Medicare Share
• # Residents based on 3-year rolling average/hospital
– FTEs capped at 1996 levels
• PRA: Per-Resident Amount from 1984, updated annually by CPI
– PRA weighted by
– 1.0 FTE for initial residency period (IRP), usually first 3 years
– 0.5 FTE beyond IRP (subspecialty fellowships)
• Medicare Share: % of Medicare inpatient days/Total inpatient
daysIME = c * [(1 + IRB ratio) 0.405 -1]
• Percentage add-on to Medicare DRG payment to adjust for
teaching intensity
– IRB: intern/resident to bed ratio
– C is a multiplier set by Congress (c=1.34)
• 5.5% increase in IME adjustment for every 10% increase in IRB
• ~1,100 teaching hospitals get IME add-on to IPPS payments
– Ranges from +1% to +48%
– ~200 hospitals get 2/3 of the funds
• MedPAC estimates Medicare pays 2x the amount justified
– i.e., a 10% increase in teaching intensity results in only a 2.7% increase
in Medicare costs per dischargeGoals of GME Policy
• Align GME funding strategy with physician workforce needs
– Geographic distribution – increase physician/population ratio in rural
and inner city regions
– Specialty distribution – increase PC physicians >40%
• Increase GME grads in PC to 50%
– Incentivize GME in competencies needed for reform
• Ambulatory, team, evidence-based, coordination, cost-effective
• Increase transparency and accountability of hospitals and GME programs in
their use and outcomes of GME fundsGME Advisors/Stakeholders
Advisory Organizations Stakeholders
• MedPAC • AAMC & COTH
• HRSA • ACGME
– COGME • AHA and FAH
– ACTPCMD
Reform
GMEMedPAC
• Hold back ½ of IME and pay out via pay for performance program
• HHS should collect data and publish annual report GME funding,
costs, and use per institution
• Conduct workforce analysis number and mix of physicians needed
• HHS to report on financial impact of GME on institutions with focus
on variable impact by specialty
• HHS to study strategies for increasing the diversity of our health
professional workforce
http://www.medpac.gov/-public-meetings-AAMC • We need more docs! • Lift the GME cap • “Cuts to GME would jeopardize our ability to train physicians, nurses, and other health care providers, and limit critical services to the community” • “Cutting physician training at a time when our nation faces a critical shortage of doctors would threaten the health of all Americans”
GME Policy Strategies • Market-based approach – feds hands-off educational policy and workforce distribution • Incentive-based approach – influence GME education and workforce via funding policy • Regulatory approach – explicitly align support with educational and workforce outcomes
• Growing pressures to reduce deficit • $4+B in empirically unjustified Indirect GME funding • Physician shortage – desire to raise GME cap by hospital community • Desire to increase accountability and transparency of GME by MedPAC, CMS, and policy-makers • trade increased GME funded positions for P4P
Resident Physician Shortage Reduction Bills
• 10th Congressional attempt to increase the GME funding cap!
– 2007: First introduced by Sen Bill Nelson (D-FL)
• Most have bipartisan sponsorship in House and Senate
• All have died in Committee
– 15,000 new slots Cost > $20B over 10 years
– Members loath to choose winners and losers
– No political air cover of a non-partisan, expert estimate of workforce
need
• ACA’s National Health Professions Workforce CommissionResident Physician Shortage Reduction Act of 2021
Resident Physician Shortage Reduction Act of 2021 • 2.3T spending bill Dec, 2020: 900B COVID relief + 1.4T Appropriation for FY21 – Congress increased GME positions by 1,000 – the first increase since 1997 • New 2021 bill would increase GME positions by 14,000 over seven years, with >10% allotted to hospitals… – in rural areas; – training over their GME cap; – in states with new medical schools or new branch campuses; and – that serve areas designated as health professional shortage areas (HPSAs) • Missing from prior versions – Allocate to hospitals training residents in outpatient sites and in shortage specialties
JGIM 2014
April 2017
Establish a GME Strategic Planning Committee • Independent, ad hoc, non-partisan Committee within DHHS • Work with, but independent of, the National Center for Health Workforce Analysis in HRSA’s Bureau of Health Workforce • Independent, nonpartisan experts and representatives of the healthcare and the health services research communities
GME Strategic Planning Committee: Charge • Educational methods consistent with society’s needs, including the sites of education and training such as inpatient and ambulatory locations; • Develop strategies that address geographic maldistribution of medical specialists, workforce diversity; • Recommend public and private funding options for GME; and • Identify informational gaps and recommend methods for obtaining data.
You can also read