Fasting Might Not Be Necessary Before Lipid Screening: A Nationally Representative Cross-sectional Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ARTICLES
Fasting Might Not Be Necessary Before Lipid Screening:
A Nationally Representative Cross-sectional Study
AUTHORS: Michael J. Steiner, MD, Asheley Cockrell WHAT’S KNOWN ON THIS SUBJECT: Fasting lipid panels are
Skinner, PhD, and Eliana M. Perrin, MD, MPH recommended to screen for lipid abnormalities; however, fasting
Division of General Pediatrics and Adolescent Medicine, can be difficult for children and make screening difficult. Results
Department of Pediatrics, School of Medicine, University of of studies in adult patients are raising questions of whether
North Carolina, Chapel Hill, North Carolina fasting is needed before lipid screening.
KEY WORDS
cholesterol, fasting WHAT THIS STUDY ADDS: In a nationally representative sample
ABBREVIATIONS of children, small but likely unimportant differences in lipid panel
AAP—American Academy of Pediatrics results were found between children who had fasted and those
TC—total cholesterol
who had not fasted before testing, which indicates that fasting
HDL—high-density lipoprotein
LDL—low-density lipoprotein before lipid screening in children might not be necessary.
VLDL—very low-density lipoprotein
NHANES—National Health and Nutrition Examination Survey
Drs Steiner, Perrin, and Skinner all made substantial
contributions to the conception and design of the study and
interpretation of the data; Dr Skinner acquired and analyzed all
of the data; Dr Steiner drafted the manuscript; and all authors
abstract
contributed to ongoing revision of the manuscript. All authors BACKGROUND: There are barriers to fasting lipid screening for at-risk
have approved the article for submission and publication.
children. Results of studies in adults have suggested that lipid testing
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0844 might be reliably performed without fasting.
doi:10.1542/peds.2011-0844
OBJECTIVE: To examine population-level differences in pediatric lipid
Accepted for publication May 13, 2011
values based on length of fast before testing.
Address correspondence to Michael J. Steiner, MD, CB 7600, 101
Manning Dr, Chapel Hill, NC 27599. E-mail: msteiner@med.unc.
METHODS: We used the National Health and Nutrition Examination Sur-
edu vey (1999 –2008) to examine total cholesterol (TC), HDL (high-density
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). lipoprotein), LDL (low-density lipoprotein), and triglyceride cholesterol
Copyright © 2011 by the American Academy of Pediatrics components on the basis of the period of fasting. Young children fasted
FINANCIAL DISCLOSURE: The authors have indicated they have for varying times before being tested, and children older than 12 years
no financial relationships relevant to this article to disclose. were asked to fast; however, adherence was variable. We used ordi-
Funded by the National Institutes of Health (NIH). nary least-squares regression to test for differences in lipid values that
were based on fasting times, controlling for weight status, age, race,
ethnicity, and gender.
RESULTS: TC, HDL, LDL, or triglyceride values were available for 12 744
children. Forty-eight percent of the TC and HDL samples and 80% of the
LDL and triglyceride samples were collected from children who had
fasted ⱖ8 hours. Fasting had a small positive effect for TC, HDL, and
LDL, resulting in a mean value for the sample that was 2 to 5 mg/dL
higher with a 12-hour fast compared with a no-fast sample. Fasting
time had a negative effect on triglycerides ( ⫽ ⫺0.859; P ⫽ .02),
which resulted in values in the fasting group that were 7 mg/dL lower.
DISCUSSION: Comparison of cholesterol screening results for a non-
fasting group of children compared with results for a similar fasting
group resulted in small differences that are likely not clinically impor-
tant. Physicians might be able to decrease the burden of childhood
cholesterol screening by not requiring prescreening fasting for these
components. Pediatrics 2011;128:000
PEDIATRICS Volume 128, Number 3, September 2011 1
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015There is heightened concern about the values, and therefore triglycerides HDL, LDL, and non-HDL cholesterol be-
current and future cardiovascular change in response to fasting sta- tween blood samples from fasting and
health of children and adolescents. tus.9,10 In most clinical laboratories, nonfasting study participants. Second,
The high prevalence of obesity,1 the the total cholesterol (TC), HDL, and tri- if there were important differences,
recognition that hyperlipidemia in glyceride levels in standard lipid pan- we sought to understand how these
childhood has an immediate impact els are directly measured, and the LDL varied on the basis of length of fast and
and might have a long- term impact on is estimated by use of the Friedewald the underlying weight status and the
cardiovascular physiology,2–4 and the calculation (LDL ⫽ [TC ⫺ HDL] ⫺ [tri- gender of the children. Finally, we
increasing number of treatment op- glycerides/5]).11 Since triglycerides sought to determine if differences in
tions for hyperlipidemia in children5,6 vary according to fasting status, calcu- cholesterol values based on fasting
have all led the American Academy of lated LDL is also affected.12,13 Because status would lead to changes in classi-
Pediatrics (AAP) and the American of the potential impact of eating on tri- fication or differences in treatment op-
Heart Association to recommend fast- glyceride and LDL values, nonfasting tions. We hypothesized that there
ing lipid panel screening for children lipid testing is often used only for mea- would be differences in triglyceride
as young as 2 years who are at risk for suring TC, HDL, and the difference be- values that were based on fasting sta-
dyslipidemia.6,7 tween the 2, or non-HDL cholesterol. tus, but that subsequent difference in
the calculated LDL value would actually
Screening of children for lipid disor- Despite the physiologic explanation of
be minimal, and likely not great
ders presents unique challenges. Most lipid changes related to fasting status,
enough to cause a change in interpre-
children will not have fasted before a results of recent research in adults
tation of screening results.
routine physician office visit.8,9 There- and children have raised questions re-
fore, most fasting lipid panels must be garding the importance of fasting be-
PATIENTS AND METHODS
either planned before visits or fore the measurement. Researchers
checked at subsequent office visits or have suggested that for the majority of In this cross-sectional study we took
additional visits to outpatient phlebot- people who take in an average-size advantage of the natural experimental
omy centers. These arrangements re- meal, the overall lipid profiles will have conditions resulting from the variable
quire many parents to miss work and minimal postprandial change.12,14,15 In fasting times in children before labora-
children to miss school to arrive for an addition, some research in adult pa- tory testing in the NHANES 1999 –2008
early morning test, and enforcing the tients has suggested that abnormal surveys. The NHANES is a stratified, mul-
requirement that children fast might postprandial triglyceride levels might tistage probability sample of the civilian,
be more difficult and unpleasant than actually be more highly associated noninstitutionalized population of the
asking adults to fast. All of these barri- with cardiovascular disease than ab- United States. The data-collection pro-
ers to fasting in children might de- normal fasting levels.16,17 Finally, in re- cess includes computer-based inter-
crease physician and parental adher- ports of studies of both adults and chil- views, an in-home questionnaire on a va-
ence to lipid screening guidelines in dren, various authors have questioned riety of demographic and health topics,
an examination including a thorough
children. the added value of cardiovascular risk
physical examination with measured
Fasting of 8 to 12 hours is recom- assessment of LDL cholesterol levels
heights and weights, and laboratory
mended before lipid screening be- beyond TC, HDL, and non-HDL choles-
measures.23
cause of the theoretical dynamic terol levels.18–22
changes that can occur in test results Because of the added burden of fasting Sample
for some lipid components during a before screening and the emerging re-
We included children aged 3 to 17
postprandial test.10 Cholesterol travels search data that call into question the
years who had at least 1 of the 4 com-
in the blood in 5 major forms: low- value of fasting before lipid assess-
mon lipid measurements available (TC,
density lipoproteins (LDLs), intermedi- ment of cardiovascular risk in adults,
HDL, LDL, or triglycerides).
ate density lipoproteins, high-density we sought to determine the effect of
lipoproteins (HDLs), very low-density li- fasting on complete lipid panels in chil- Independent Variables
poproteins (VLDLs), and chylomi- dren. Specifically, we took advantage
crons.9,10 Chylomicrons, which are of variable fasting times within the na- Fasting Time
found after intestinal cells absorb fat- tionally representative National Health All children aged 3 years and older
containing food, and VLDL comprise and Nutrition Survey (NHANES) to de- were eligible for lipid testing and were
the majority of the serum triglyceride termine if there are differences in TC, evaluated in either a morning or after-
2 STEINER et al
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015ARTICLES
noon session. Children evaluated in Control reference standard were tutional review board review (under
the morning had TC, HDL, LDL, and tri- within the acceptable range, and did federal regulation 45 CFR §46.101), be-
glycerides measured; those aged 12 not necessitate additional adjustment cause it included the use of only de-
years or older were asked to fast, with our focus on fasting-based differ- identified secondary data.
whereas those younger than 12 years ences averaged over the period.25
were given no specific fasting instruc- Triglycerides were measured enzymat- RESULTS
tions. Children evaluated in the after- ically in serum for all years. A total of 12 744 children aged 3 to 17
noon had TC and HDL measured and years had values for at least 1 of the 4
LDL was calculated from TC, HDL, and
were not given any specific fasting in-
triglycerides as follows: LDL ⫽ (TC ⫺ lipid components. The mean age was
structions regardless of age. Informa-
HDL) ⫺ (triglycerides/5). 11 years, most of the children were
tion on time since last food or drink healthy weight (64%), and the fewest
consumed was recorded and available Non-HDL cholesterol was calculated by
children were in the age range of 3 to 5
on all children, regardless of session subtracting the HDL cholesterol value
years because starting in 2006 the
time or specific instructions. We ex- from the TC value.
NHANES measured lipid values only for
tracted fasting time as reported for children older than 5 years. Triglycer-
each child, and by taking advantage of Statistical Methods
ides and LDL results from morning
the different fasting instructions and We first used ordinary least-squares blood tests were available for 38.6%
variable adherence to those instruc- regression to test for differences in and 37.5% of the sample, respectively,
tions, we examined the relationship lipid values based on fasting times. We and with the use of AAP cutoffs, mea-
between fasting time and lipid values. controlled for weight status, race, eth- sured values were normal for 63% of
nicity, gender, and, because lipid val- TC values, 95% of HDL, 79% of LDL, and
Weight Status ues differ by age,26 we also controlled 97% of triglyceride values. Nearly half
We used height and weight as mea- for age, as well as squared and cubic
(48%) of the TC and HDL samples were
sured during the examination compo- transformations of age. We used these
obtained from children who had fasted
nent to calculate BMI and determine equations to predict lipid values based
for at least 8 hours, and 80% of the LDL
percentiles by using a SAS code devel- on fasting time, and graphed mean
and triglyceride sample was from chil-
oped for that purpose (SAS Institute, lipid values across hours of fasting.
dren who had fasted for at least 8
Cary, NC).24 Second, we used seemingly unrelated hours (Table 1).
regression models to examine if the ef- The data in Table 2 demonstrate the
Dependent Variables fect of fasting time on lipid values var- mean difference in each lipid compo-
Equipment used for lipid analyses var- ied on the basis of whether the child nent measurement per hour of fasting
ied according to year. During 1999 – was healthy weight or overweight/ status. After adjustment for subject
2004, a Roche Hitachi 704 Analyzer obese. Healthy weight was defined as age, weight status, self-identified race/
(Roche Diagnostics, Fishers, IN) was ⬍85th percentile, and overweight and ethnicity, and gender, there were only
used; during 2005, a Roche Hitachi 717 obese were collapsed at ⱖ85th per- small changes in lipid components
was used; during 2006 a Roche Hitachi centile for all children. based on hours of fasting, although
912 was used; and during 2007–2008, a Finally, using our adjusted equations values for all measurands except non-
Roche Modular P was used 25. and baseline distribution of choles- HDL cholesterol did reach statistical
TC was measured enzymatically in se- terol results in the sample, we calcu- significance. For example, for each
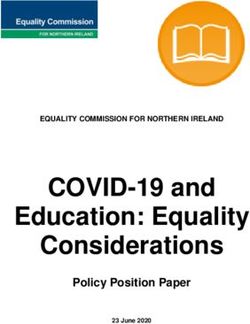
rum or plasma for all years. lated predicted lipid values for groups hour of fasting, the TC increased by an
HDL cholesterol in 1999 –2002 was mea- of children from the population who average of 0.17 mg/dL (P ⫽ .05). Stated
sured by using heparin-manganese pre- had blood drawn immediately post- another way, if an average child were
cipitation or direct immunoassay mea- prandially instead of subsequent to an screened immediately postprandially,
surement, depending on sample size ideal 12-hour fast. his or her TC would be ⬃2 mg/dL lower
and patient age. Beginning in 2003, all All analyses were adjusted for the than another average child after a 12-
samples were tested by using a direct complex survey design of the NHANES hour fast. These results are displayed
immunoassay. Despite the difference and were performed by using the sur- graphically in Fig 1. The peak mean
in laboratory methods, the changes for vey estimation routines in Stata 11.0 cholesterol values appear at fasting
HDL values over the period, compared (Stata Corp, College Station, TX). This times of ⬃5 and 14 hours, with a min-
with those for the Centers for Disease study was deemed exempt from insti- imum value at ⬃10 hours of fasting.
PEDIATRICS Volume 128, Number 3, September 2011 3
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015TABLE 1 Demographic and Mean
Characteristics (N ⫽ 12 744)
Variable Value
Gender, %
Female 48.3
Male 51.7
Race/ethnicity, %
White 59.6
Black 14.9
Hispanic 19.3
Other race 6.2
Age, mean (range), y 11.02 (3–17)
3–5 y, % 9.4
6–8 y, % 20.5
9–11 y, % 22.0
12–14 y, % 23.8
15–17 y, % 24.3
Weight status (percentile), %
Very obese (⬎99th) 4.0
Obese (95th–99th) 13.1
Overweight (85th–95th) 15.8
Healthy weight (5th–85th) 63.7
Underweight (⬍5th) 3.4 FIGURE 1
Total cholesterol, mean 162.2 (62–575) Predicted values of TC based on hours of fasting before testing.
(range), mg/dL
Normal 63.4
Borderline 27.7
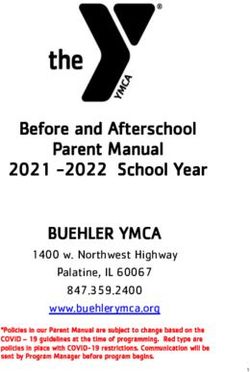
High 8.9 averaged LDL cholesterol values in with healthy weight children. However,
HDL, mean (range), mg/dL 51.8 (16–131) children who had fasted for varying the degree of these changes was still
Normal 94.7
Low 5.3 amounts of time. This line has a gener- small relative to overall lipid value re-
Non-HDL 110.4 (0–521) ally linear increase over time that sults, and there were no statistically
LDL, mean (range), mg/dL 91.9 (19–311)
Normal 79.1 peaks at 15 hours of fasting. The calcu- significant differences when the
Borderline 13.9 lated LDL change graphed over time changes in cholesterol values accord-
High 7.1 seems to be the inverse of the triglyc-
Triglycerides, mean (range), 88.4 (15–1750) ing to weight status were compared
mg/dL eride graph, which decreases in a lin- (Table 3). The age of the child at time of
Normal 96.7 ear fashion over time. The HDL choles- screening did not have a consistent im-
High 3.3
Total fasting time, mean 6.9 (0–180)
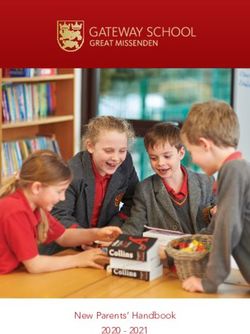
terol increases by an average of 0.08 pact on the response to fasting time of
(range), h mg/dL per hour (Fig 3). The graph of the cholesterol result (Table 4).
the HDL cholesterol over time does
not demonstrate clinically important Effect of Fasting on Lipid
The LDL cholesterol increased in the ad- change, and because the TC is also rel- Classification
justed model by 0.46 mg/dL per hour of atively stable, the calculated non-HDL
cholesterol does not show a dramatic For TC, nonfasting screening inappro-
fasting (Table 2). Again, the LDL of an
priately classifies ⬃1% of children as
average child would be ⬃5 mg/dL change over time (Fig 3).
normal, who would have had border-
lower immediately postprandially Overweight children had slightly in-
compared with the LDL subsequent to creased mean changes in lipid compo- line values with fasting. In addition,
a 12-hour fast. Figure 2 displays the nents per hour of fasting compared ⬃1% of children with borderline non-
fasting values would actually have ele-
vated results if fasting. For LDL, 1.2% of
TABLE 2 Ordinary Least-Squares Regression of the Effect of Number of Hours (Continuous) on children with borderline fasting levels
Total Cholesterol, HDL, LDL, and Triglycerides, Unadjusted and Adjusted for Age, Race, would have normal results postprandi-
Gender, and Weight
ally, and 1.6% of children with in-
Unadjusted P 95% Confidence Adjusted P 95% Confidence
Coefficient Interval Coefficient Interval creased calculated LDL while fasting,
Cholesterol 0.033 .669 ⫺0.120 to 0.186 0.174a .048a 0.002 to 0.346a would now be considered to have bor-
HDL 0.034 .179 ⫺0.016 to 0.085 0.078a .007a 0.022 to 0.133a derline results. For triglycerides, ⬃4%
Non-HDL ⫺0.001 .992 ⫺0.156 to 0.154 0.097 .271 ⫺0.077 to 0.270
LDL 0.243 .115 ⫺0.061 to 0.548 0.456a .013a 0.099 to 0.813a
of the children classified with normal
Triglycerides ⫺0.664a .022a ⫺1.229 to ⫺0.100a ⫺0.859a .019a ⫺1.573 to ⫺0.144a triglycerides when fasting would have
a Statistically significant effects. elevated values postprandially.
4 STEINER et al
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015ARTICLES
lesterol values in our sample based on
fasting status are actually smaller
than other causes of variation not ac-
counted for in the current screening
guidelines. A recent study revealed
large variations in fasting LDL choles-
terol over time in children.27 These dif-
ferences could cause clinically impor-
tant changes in diagnosis and
treatment. For example, up to 1 in 3
children with elevated LDL levels at 10
years of age will have normal-range
levels 3 years later.27 The changes in
cholesterol values over time have also
been studied in relation to retesting of
adult patients with normal and abnor-
mal baseline cholesterol values. In
these subjects, coefficients of varia-
tion for results of retests within a per-
son over time ranged between 6% and
11% for the various cholesterol com-
ponents.28,29 For adult patients with el-
evated TC, this would result in individ-
ual variation with an SD of between 15
and 23 mg/dL.29 Although the testing
procedure we used was different, and
the variation in our study was across a
sample instead of within a person, the
change in mean values based on fast-
ing status is likely less important clin-
ically than longitudinal changes over
time or even than test-retest variation.
FIGURE 2 Although studies on nonfasting lipids
Predicted values of LDL cholesterol and triglycerides based on hours of fasting before testing. generally assume that fasting choles-
terol levels are the gold standard to
DISCUSSION subjects within the sample did not con- which other testing strategies should
Comparing a nationally representative sistently affect the variation based on be compared, research results in
cross-section of children who had fasting status. adult patients suggest that nonfasting
fasted for various lengths of time, we lipid panels also predict, and might
demonstrated that nonfasting mea- Previous studies in adult patients have even better predict, cardiovascular
surements of TC, calculated LDL, and also documented minimal differences disease.12,15 It is particularly notewor-
HDL cholesterol values had only small in lipoprotein profiles after normal thy that nonfasting triglycerides in
differences from fasting values. Al- food intake in the general population.12 adult patients are a risk factor for future
though statistically significant, these In fact, a recent study by Langsted et al myocardial infarction and death,16 and
differences are unlikely to result in im- in adults found that when LDL samples that nonfasting triglycerides might actu-
portant clinical changes in the results were corrected for the hemodilution ally better predict cardiovascular events
of screening for cholesterol abnormal- that occurred with fasting while un- in some populations do than fasting val-
ities. Triglyceride values differed more sweetened fluid intake was allowed, di- ues.17 In children and young adults, fast-
dramatically on the basis of fasting rectly measured LDL did not change ing values continue to be used for epide-
status. The weight status and age of with fasting.14 The differences of cho- miologic research,2,3,30–33 although the
PEDIATRICS Volume 128, Number 3, September 2011 5
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015does not change with fasting status,
and Frontini et al determined that
it predicted future cardiovascular
events as well as other lipoprotein
measurements.20
The major limitation of our research
was that all analyses were conducted
across a large sample and on a cross-
sectional basis. We were not able to
analyze the cholesterol results from
an individual child repeatedly after
various periods of fasting. Although
our research allows us to confidently
demonstrate the population-level dif-
ferences in cholesterol values at vari-
ous periods of time after eating, we
assume that some children will have
greater or less dramatic differences in
fasting and nonfasting values. For ex-
ample, although not statistically differ-
ent, values for obese children had a
trend toward more dramatic lipid re-
sult changes with fasting. In addition, it
is possible that there was a systematic
difference within our sample between
children who fasted and children who
did not fast before testing. We did con-
trol for weight status, which should
mitigate 1 risk for unmeasured sys-
tematic differences associated with
which of the children fasted, but there
might be others. A third limitation of
FIGURE 3 our work was that all of our LDL cho-
Predicted values of HDL and non-HDL cholesterol based on hours of fasting before testing. lesterol values were calculated values
determined by use of the Freidewald
equation used in the NHANES.11 Directly
TABLE 3 Effect of Fasting Time (in Hours) on TC, HDL, LDL, and Triglycerides According to Weight measured LDL values are increasingly
Status After Adjustment for Age, Race, and Gender being used in clinical laboratories, and
Healthy Weight Overweight or Obese Difference, studies comparing directly measured
Pa
 95% Confidence  95% Confidence LDL to calculated LDL after various
Interval Interval
fasting times in children are war-
Cholesterol 0.089 ⫺0.102 to 0.279 0.292 0.029 to 0.555 .163
HDL 0.054 ⫺0.016 to 0.124 0.107 0.020 to 0.194 .336
ranted. However, in previous work
Non-HDL 0.035 ⫺0.155 to 0.225 0.185 ⫺0.079 to 0.449 .299 with adult patients, directly measured
LDL 0.360 ⫺0.054 to 0.775 0.688 0.224 to 1.152 .223 and calculated fasting LDL values were
Triglycerides ⫺0.970 ⫺1.705 to ⫺0.234 ⫺0.717 ⫺1.726 to 0.292 .656
similar and equally predicted future
a P value for the difference between coefficients in the healthy weight and overweight regressions.
cardiovascular events.34
The AAP currently recommends a fast-
degree to which fasting improves risk predictive values of non-HDL choles- ing lipid panel on any child or adoles-
prediction in children is questionable. terol of children in the Bogalusa Heart cent with an increased risk of hyperlip-
For example, Frontini et al analyzed the Study database. Non-HDL cholesterol idemia or other cardiovascular risk
6 STEINER et al
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015ARTICLES
TABLE 4 Effect of Fasting Time on TC, HDL, LDL, and Triglycerides According to Age After Adjustment for Gender, Race, and BMI Percentile According to
Age
Age 3–5 y Age 6–8 y Age 9–11 y Age 12–14 y Age 15–17 y
 95% Confidence  95% Confidence  95% Confidence  95% Confidence  95% Confidence
Interval Interval Interval Interval Interval
Cholesterol 0.238 ⫺0.231 to 0.708 0.072 ⫺0.279 to 0.424 0.365a 0.057 to 0.673a 0.186 ⫺0.017 to 0.388 0.282 ⫺0.051 to 0.615
HDL 0.034 ⫺0.142 to 0.210 0.162a 0.018 to 0.306a 0.196a 0.066 to 0.325a 0.089a 0.000 to 0.178a ⫺0.008 ⫺0.105 to 0.089
Non-HDL 0.208 ⫺0.279 to 0.695 ⫺0.090 ⫺0.402 to 0.223 0.169 ⫺0.126 to 0.465 0.097 ⫺0.099 to 0.292 0.290 ⫺0.045 to 0.625
LDL 0.618a 0.218 to 1.018a 0.265 ⫺0.276 to 0.805 0.640 ⫺0.067 to 1.346 0.717 ⫺0.234 to 1.668 1.240a 0.129 to 2.351a
Triglycerides ⫺0.480 ⫺1.815 to 0.855 ⫺1.371a ⫺2.496 to ⫺0.246a ⫺0.711 ⫺1.561 to 0.140 0.038 ⫺1.856 to 1.932 ⫺0.451 ⫺2.244 to 1.343
a Statistically significant effects.
factors.6 However, preparing for the missed screening or increased warranted. If those results confirm
fasting state makes screening recom- screening cost as a result of recom- our findings, professional societies
mendations more burdensome. In fact, mending fasting status raise ques- might wish to reconsider their rec-
although no formal cost analyses has tions regarding any benefits achieved. ommendations and encourage pro-
been done, the fasting requirement viders follow lipid screening guide-
likely makes the screening process CONCLUSIONS lines at the point of care, regardless
more expensive because of the need Across a large, nationally representa- of fasting status.
for return office visits, increased tive sample of children, the levels of TC,
transportation expenses, and missed HDL, non-HDL cholesterol, and LDL cho- ACKNOWLEDGMENTS
work and/or school. This increased lesterol vary minimally on the basis of Dr Skinner was supported by a Na-
burden and cost are not only likely to fasting time. It is not known if these tional Institutes of Health Building In-
undermine appropriate screening, but small differences in lipoprotein com- terdisciplinary Careers in Women’s
also potentially worsens the utility of ponents consistently weaken or Health award (K12-HD01441), and Dr
screening in any formal cost analysis. strengthen the usefulness of lipid val- Perrin was supported by a National In-
Because research findings in other ues for the assessment of current stitutes of Health career development
populations suggest that nonfasting health risks or prediction of future award (K23 HD051817).
lipid panels can predict cardiovascu- cardiovascular risks, but it is clear We acknowledge the members of the
lar events, and that the difference be- that testing regardless of fasting sta- Scientific Collaborative for Overweight
tween fasting and nonfasting lipid pan- tus would reduce barriers to screen- and Obesity Prevention and Treatment
els in children is small and likely ing. Therefore, future research with at the University of North Carolina for
clinically insignificant, the risks of people in longitudinal samples is their contributions to this work.
REFERENCES
1. Ogden CL, Carroll MD, Curtin LR, Lamb MM, 5. Avis HJ, Vissers MN, Stein EA, et al. A system- 9. National Cholesterol Education Program
Flegal KM. Prevalence of high body mass atic review and meta-analysis of statin ther- (NCEP) Expert Panel on Detection, Evalua-
index in US children and adolescents, apy in children with familial hypercholes- tion, and Treatment of High Blood Choles-
2007–2008. JAMA. 2010;303(3):242–249 terolemia. Arterioscler Thromb Vasc Biol. terol in Adults (Adult Treatment Panel III).
2. Pletcher MJ, Bibbins-Domingo K, Liu K, et al. 2007;27(8):1803–1810 Third Report of the National Cholesterol Ed-
Nonoptimal lipids commonly present in 6. Daniels SR, Greer FR; American Academy of ucation Program (NCEP) Expert Panel on
young adults and coronary calcium later in Pediatrics, Committee on Nutrition. Lipid Detection, Evaluation, and Treatment of
life: the CARDIA (Coronary Artery Risk Devel- screening and cardiovascular health in High Blood Cholesterol in Adults (Adult
opment in Young Adults) study. Ann Intern childhood. Pediatrics. 2008;122(1):198 –208 Treatment Panel III) final report. Circula-
Med. 2010;153(3):137–146 7. Williams CL, Hayman LL, Daniels SR, et al. tion. 2002;106(25):3143–3421
3. Davis PH, Dawson JD, Riley WA, Lauer RM. Cardiovascular health in childhood: a state- 10. Rosenson RS. Lipoprotein classification; me-
Carotid intimal-medial thickness is related ment for health professionals from the tabolism; and role in atherosclerosis. In: Basow
to cardiovascular risk factors measured committee on atherosclerosis, hyperten- DS, ed. UpToDate. Watham, MA: UpToDate; 2010
from childhood through middle age: the sion, and obesity in the young (AHOY) of the 11. Friedewald WT, Levy RI, Fredrickson DS. Es-
Muscatine Study. Circulation. 2001;104(23): Council on Cardiovascular Disease in the timation of the concentration of low-density
2815–2819 Young, American Heart Association. Circu- lipoprotein cholesterol in plasma, without
4. Mimoun E, Aggoun Y, Pousset M, et al. Associa- lation. 2002;106(1):143–160 use of the preparative ultracentrifuge. Clin
tion of arterial stiffness and endothelial dysfunc- 8. Devaney BL, Gordon AR, Burghardt JA. Di- Chem. 1972;18(6):499 –502
tion with metabolic syndrome in obese children. etary intakes of students. Am J Clin Nutr. 12. Langsted A, Freiberg JJ, Nordestgaard BG.
J Pediatr. 2008;153(1):65–70 1995;61(1 suppl):205S–212S Fasting and nonfasting lipid levels: influ-
PEDIATRICS Volume 128, Number 3, September 2011 7
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015ence of normal food intake on lipids, lipo- 20. Frontini MG, Srinivasan SR, Xu J, Tang R, protein cholesterol among children. Pediat-
proteins, apolipoproteins, and cardiovascu- Bond MG, Berenson GS. Usefulness of child- rics. 2010;126(2):266 –273
lar risk prediction. Circulation. 2008; hood non-high density lipoprotein choles- 28. Takahashi O, Glasziou PP, Perera R, et al.
118(20):2047–2056 terol levels versus other lipoprotein mea- Lipid re-screening: what is the best mea-
13. Nordestgaard BG, Benn M. Fasting and non- sures in predicting adult subclinical sure and interval? Heart. 2010;96(6):
fasting LDL cholesterol: to measure or cal- atherosclerosis: the Bogalusa Heart Study. 448 – 452
culate? Clin Chem. 2009;55(5):845– 847 Pediatrics. 2008;121(5):924 –929
29. Glasziou PP, Irwig L, Heritier S, Simes RJ,
14. Langsted A, Nordestgaard BG. Nonfasting 21. Cui Y, Blumenthal RS, Flaws JA, et al. Non- Tonkin A; LIPID Study Investigators. Monitor-
lipids, lipoproteins, and apolipoproteins in high-density lipoprotein cholesterol level as
ing cholesterol levels: measurement error
individuals with and without diabetes: 58 a predictor of cardiovascular disease mor-
or true change? Ann Int Med. 2008;148(9):
434 individuals from the Copenhagen Gen- tality. Arch Intern Med. 2001;161(11):
656 – 661
eral Population Study. Clin Chem. 2011; 1413–1419
30. Newman WP, Freedman DS, Voors AW, et al.
57(3):482– 489 22. Craig SR, Amin RV, Russell DW, Paradise NF.
Relation of serum-lipoprotein levels and
15. Mora S, Rifai N, Buring JE, Ridker PM. Fast- Blood cholesterol screening influence of
systolic blood-pressure to early
ing compared with nonfasting lipids and fasting state on cholesterol results and
atherosclerosis: the Bogalusa Heart-Study.
apolipoproteins for predicting incident car- management decisions. J Gen Intern Med.
N Engl J Med. 1986;314(3):138 –144
diovascular events. Circulation. 2008; 2000;15(6):395–399
118(10):993–1001 23. Centers for Disease Control and Prevention. 31. Berenson GS, Srinivasan SR, Bao WH, New-
NHANES 2007–2008 public data general re- man WP, Tracy RE, Wattigney WA. Associa-
16. Nordestgaard BG, Benn M, Schnohr P,
lease file documentation. Available at: www. tion between multiple cardiovascular risk
Tybjaerg-Hansen A. Nonfasting triglycerides
cdc.gov/nchs/nhanes/nhanes2007-2008/ factors and atherosclerosis in children and
and risk of myocardial infarction, ischemic
generaldoc_e.htm. Accessed June 14, 2011 young adults. N Engl J Med. 1998;338(23):
heart disease, and death in men and
1650 –1656
women. JAMA. 2007;298(3):299 –308 24. Centers for Disease Control and Prevention.
A SAS program for the CDC growth charts. 32. Raitakari OT, Juonala M, Kahonen M, et al.
17. Bansal S, Buring JE, Rifai N, Mora S, Sacks
FM, Ridker PM. Fasting compared with non- Available at: www.cdc.gov/nccdphp/dnpao/ Cardiovascular risk factors in childhood
fasting triglycerides and risk of cardiovas- growthcharts/resources/sas.htm. Ac- and carotid artery intima-media thickness
cular events in women. JAMA. 2007;298(3): cessed June 27, 2011 in adulthood: the Cardiovascular Risk in
309 –316 25. Centers for Disease Control and Prevention. Young Finns Study. JAMA. 2003;290(17):
National Health and Nutrition Examination 2277–2283
18. Ridker PM, Rifai N, Cook NR, Bradwin G, Bur-
ing JE. Non-HDL cholesterol, apolipopro- Survey Laboratory Procedures Manual. 33. Pencina MJ, D’Agostino RB Sr, Larson MG,
teins A-I and B100, standard lipid measures, Available at: www.cdc.gov/nchs/data/ Massaro JM, Vasan RS. Predicting the 30-
lipid ratios, and CRP as risk factors for car- nhanes/lab7-11.pdf. Accessed February 7, year risk of cardiovascular disease: the Fra-
diovascular disease in women. JAMA. 2005; 2011 mingham Heart Study. Circulation. 2009;
294(3):326 –333 26. Cook S, Auinger P, Huang TT. Growth curves 119(24):3078 –3084
19. Srinivasan SR, Frontini MG, Xu J, Berenson for cardio-metabolic risk factors in chil- 34. Mora S, Rifai N, Buring JE, Ridker PM. Com-
GS. Utility of childhood non– high-density li- dren and adolescents. J Pediatr. 2009;155: parison of LDL cholesterol concentrations
poprotein cholesterol levels in predicting S6 –S26 by Friedewald calculation and direct mea-
adult dyslipidemia and other cardiovascu- 27. Freedman DS, Wang YC, Dietz WH, Xu JH, surement in relation to cardiovascular
lar risks: the Bogalusa Heart Study. Pediat- Srinivasan SR, Berenson GS. Changes and events in 27,331 women. Clin Chem. 2009;
rics. 2006;118(1):201–206 variability in high levels of low-density lipo- 55(5):888 – 894
8 STEINER et al
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015Fasting Might Not Be Necessary Before Lipid Screening: A Nationally
Representative Cross-sectional Study
Michael J. Steiner, Asheley Cockrell Skinner and Eliana M. Perrin
Pediatrics; originally published online August 1, 2011;
DOI: 10.1542/peds.2011-0844
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2011/07/28
/peds.2011-0844
Citations This article has been cited by 6 HighWire-hosted articles:
http://pediatrics.aappublications.org/content/early/2011/07/28
/peds.2011-0844#related-urls
Permissions & Licensing Information about reproducing this article in parts (figures,
tables) or in its entirety can be found online at:
http://pediatrics.aappublications.org/site/misc/Permissions.xht
ml
Reprints Information about ordering reprints can be found online:
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015Fasting Might Not Be Necessary Before Lipid Screening: A Nationally
Representative Cross-sectional Study
Michael J. Steiner, Asheley Cockrell Skinner and Eliana M. Perrin
Pediatrics; originally published online August 1, 2011;
DOI: 10.1542/peds.2011-0844
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2011/07/28/peds.2011-0844
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned,
published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point
Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on October 28, 2015You can also read