EVALUATION OF THE EFFECT OF DEADLY MUCORMYCOSIS IN POST COVID-19 PATIENTS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
EVALUATION OF THE EFFECT OF DEADLY MUCORMYCOSIS IN POST
COVID-19 PATIENTS
Tanmay Ghosh1, Sandipan Chatterjee2*
1
Assistant Professor, Department of Microbiology, Dinabandhu Andrews College, Baishnabghata,
South 24 Parganas, Kolkata – 700084, West Bengal, India.
2
Assistant Professor, Department of Botany, Suri Vidyasagar College, Suri, Birbhum - 731 101,
WestBengal, India
[1tanmay.tanmay.ghosh780@gmail.com, 2chatterjee.sandipan@rediffmail.com]
ABSTRACT
People of the entire world are fighting against the life-threatening disease COVID-19 during more than one
year. In this microbiological war a large number of people have already lost their life, some fighter have won
the war and many people have dedicated their life to take the human being to the door of victory in this war.
In such a time of disaster another life-threatening disease appears recently, known as Mucormycosis.
Mucormycosis, also known as “Black fungus” disease is playing the role of helping hand of COVID-19 to
make it winner in this war because it is infecting the recovered or recovering COVID-19 patients. It mainly
affects the people with suffering from some severe diseases as AIDS, cancer and mainly diabetes.
Mucormycosis is a rare disease but the trending pandemic COVID-19 continues to welcome it to be the
successor of next pandemic. It may fetal if it is untreated for long time and it also causes paralysis, seizure
like disease. This disease is caused by inhalation of black fungal spore from air or it may occur in the wound
skin. The aim of the discussion is to establish the interconnection between COVID-19 and Mucormycosis
and giving awareness about the infection.
Key-words: Mucormycosis, Microbiology, Pathology, Pharmaceutical, Biology.
I. INTRODUCTION
Coronavirus disease 2019 (COVID-19) pandemic was first flowed out in Wuhan, china in December 2019 and
since then the frequency of bacterial growth and fungal coinfections has been continuously ascending.
Flourishing record suggests that patients infected with severe acute respiratory syndrome coronavirus-2 (SARS
Cov-2) may develop also in bacterial and fungal secondary infections. In this time, the chance of causing
Invasive Pulmonary Aspergillosis (IPA) is high for post COVID-19 causes. It is caused by disclosure to
Mucormould which is generally found in soil, plants, manure and decaying fruits and vegetables. It is also found
in the nose, mucus of a healthy and normal people. Affects the sinuses, brain and lungs, life threatening in
diabetes and cancer patients or people with HIV/ AIDS. Effects to the COVID-19 patients recovering after three
weeks. Rhino- orbito- cerebral mucormycosis is considered as the most common manifestation. Here, we
described with a patient with his uncontrolled diabetes who treated for COVID-19 but he was read mitted after
three-week discharge with a diagnosis of rhinocerebralmucormycosis. COVID-19 patient has high risk of
development of mucormycosis as because intake of widespread glucocorticoid to cure COVID-19. This
glucocorticoid can lead to cause secondary fungal infection which is mucormycosis. This fungi mainly found in
sinuses.
www.turkjphysiotherrehabil.org 3737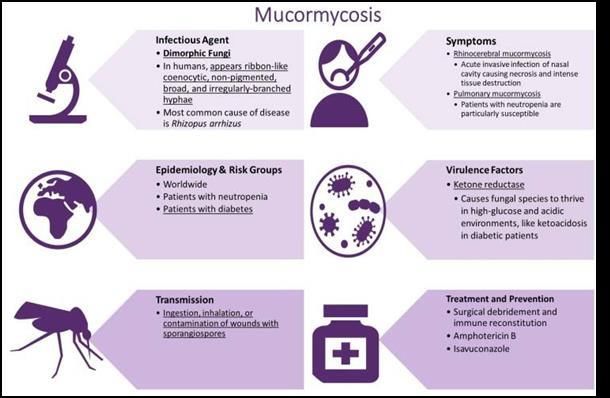
Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
Fig-1: Microscopic view of Mucormycosis fungi
Mucorales: causative agent of Mucormycosis:
Mucorales are the largest group of zygomycete fungi. These fungi also known as pin molds or Black Fungi. Black
fungi called because of its pigmentation. Mucorales are the order of fungi which are responsible for the disease
mucormycosis.
Scientific classification:
Kingdom: Fungi
Sub kingdom: Eumycota
Division: Zygomycota
Sub division: Mucomycotina
Order: Mucorales
Family: Mucoraceae
Species: Mucor sp.
II. MORPHOLOGY AND LIFE CYCLE OF MUCORALES
Mucorales are the group of saprophytic aerobic fungi characterized by huge and rapidly growing mycelia. These
are form in large quantity in anamorphic structure. The anamorphic sporangiospore are usually produced multiple
spore, which are abundantly found in air. The spores are released, when it matured by disintegration of
sporangium wall. The mature sporangiospore germinate to form haploid hyphae of a new mycelium. In case of
hecterothalic species of mucorales they reproduce by sexual mode of reproduction by formation of zygote.
Haploid zygotes fuse to form diploid zygospore and then after meiosis within zygospore, new mycelium or
sporangium are formed.
www.turkjphysiotherrehabil.org 3738Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
Fig-2: Mucorales
III. SYMPTOMS
Warning signs include pain and redness around the eyes or nose, with fever, headache, coughing, shortness of
breath, bloody vomits and altered mental status. According to the advisory, infection with mucormycosis should
be suspected when there are:
❖ Sinusitis, nasal blockade or congestion, nasal discharge (blackish/bloody).
❖ Local pain in the cheek bone, one sided facial pain, numbness or swelling.
❖ Blackish discoloration over bridge of nose/palate.
❖ Loosening of teeth, jaw involvement.
❖ Blurred or double vision with pain.
❖ Thrombosis, necrosis, skin lesion.
❖ Chest pain, pleural effusion, worsening of respiratory symptoms.
Fig 3: Sinus infection by mucormycosis
www.turkjphysiotherrehabil.org 3739Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
IV. CAUSE
Mucormycosis is caused by a group of moulds or saprophyte fungi, named mucormycota that normally grows in
soil and decaying organic material such as rotten leaves, wood, fruits etc. It can be also found in mucus and nose
of healthy people. To reduce the rate of mortality in the COVID-19 patients and to modulate their immune related
lung injury, corticosteroids are using randomly to fulfill the need of respiratory supports and supplementary
oxygen. This random use to mucormycosis that increase the rate of mortality. Its random use to the COVID-19
patients can increase the rate of mortality due to mucormycosis.
V. RELATION WITH COVID-19
There are no genetic relationship between coronavirus and mucormycosis but they are interconnected
immunologically. When a patient become too much infected by COVID-19 and got hospitalized, his immunity
power trying heart and soul to fight against coronavirus and in this case this patient is provided a huge amount of
corticosteroid that act as a strong support of immune system in this war by reducing inflammation in lungs and
repairing some damages that can happen for overdriving of immune system of body. But on the other hand,
steroids reduce immunity power and increase blood sugar levels in both diabetic and non-diabetic patients.
Patients suffering for COVID-19 disease are continuously use glucocorticoid. These types of steroid supported
our own immune system, suppressed the activity of White Blood Cell (WBC). As WBC become inactive several
fungal which are found in air, soil like mucor attack to the patient. Patient who is admitted in hospital for long
time has high chance to cause this disease because of it low immune response. Generally, this black fungus
naturally occurs in our environment. It may invade in our body lodge in the nasal passage and silently stay in our
body, a symptomatically. When a patients fell sick, increase blood sugar levels, patients who unable to form
neutrophils may victim to mucormycetes. Diabetic is very effective in lowering the immunity power. So in this
situation if mucormycetes can able to enter into the body they can easily cause severe infection without any
prevention and the patient have to accept death.
VI. TRANSMISSION
The causative agent of mucormycosis, Mucorales is a member of spore forming fungal group that have saclike
fruiting structure (sporangia) and produced yellow or brown spores that is 3-11 micrometers in diameter and they
are easily aerosolized. So they can enter into host by air flow. Staying in contact with rotten materials and dirty
environment are the suitable way for their transmission. Mucormycosis also can be transmitted from the
contaminated bandages, tongue depressors and other medical solutions or devices.
❖ It can spread by inhalation of fungal spore and it gets lodged into sinus and lungs.
❖ Low oxygen concentrations in blood help the fungi to replicate fast.
Fig 4: Overview of Mucormycosis
www.turkjphysiotherrehabil.org 3740Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
VII. TREATMENT
A rare but serious fungal infection known as mucormycosis and colloquially as black fungus is being detected
relatively frequently among COVID-19 patients in some states. The disease often manifests in the skin and
affects the lungs and brain. While it is treated with antifungals, mucormycosis may eventually require surgery.
Doctors have said that it is of at most importance to control diabetes, reduce steroids, and discontinue immune
modulatory drugs. It is important to diagnose the disease as early as possible. The Mucormycetes medicine is
costly enough. A six weeks dose of liposomal Amphotericin B is only a drug that can cure it. It is directly used on
infection site. Experts in the task force have stressed the need to control hypercemia and monitor blood glucose
levels after discharge following COVID-19 treatment and also diabetes. One should use steroids judiciously;
correct timing, correct dose and duration are important.
In some cases, it can require surgery. It can lead to eventual loss of upper jaw and sometimes even an eye.
VIII. PREVENTION
It is not possible to breath sincerely that no fungal spore enters in our body because the fungi of mucormycosis is
very common in environment and the person with low immunity power has the great chance to get this infection.
So people can protect themselves by protecting them from the environment and making yourself
immunologically strong:
Protection from Environment:
❖ Try to avoid the dusty and garbage area. If these areas can’t be avoided then use face mask.
❖ Avoid direct contact with flood water, water damaged buildings, rotten things.
❖ In the outside of home try to wear long part, full sleeves shirts, shoes and wear gloves specially at the
time of doing some outdoor or dusty activities.
❖ Always try to clean skin with soap.
Antifungal Medication:
If someone feels to have lower immunity power and have the chance to get infected mucormycosis for his/her
daily work, then he/she should consult with his/her medical practitioner and take some antifungal and immune
booster medicines for advance protection.
IX. CONCLUSION
During almost one and half year COVID-19 has made the world its kingdom of death and now it has been
welcome mucormycosis to be its successor. This fungal infection is carrying the similar risk factor even its
diagnosis become more challenging because of clinical suspicion and difficulty of isolating the causative fungi.
Diabetes mellitus has been associated with SARS Cov-2 infection for the use of a large amount of steroid to the
severe patients. Histopathology, direct examination and culture remain essential tools, although the molecular
methods are improving and for this account molecular based methods and new fungal genetic are being explored.
REFERENCES
1 Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. Epidemiology and outcome of zygomycosis: a review of
929 reported casesexternal icon. Clin Infect Dis. 2005 Sep 1;41(5):634-53.
2 Petrikkos G, Skiada A, Lortholary O, Roilides E, Walsh TJ, Kontoyiannis DP. Epidemiology and clinical manifestations of mucormycosisexternal
icon. Clin Infect Dis. 2012 Feb;54Suppl 1:S23-34.
3 Walsh TJ, Gamaletsou MN, McGinnis MR, Hayden RT, Kontoyiannis DP. Early clinical and laboratory diagnosis of invasive pulmonary,
extrapulmonary, and disseminated mucormycosis (zygomycosis)external icon. Clin Infect Dis. 2012 Feb;54Suppl 1:S55-60.
4 Avery RK, Michaels MG. Strategies for safe living after solid organ transplantationexternal icon. Am J Transplant. 2013 Mar;13Suppl 4:304-10..
5 CDC. Guidelines for preventing opportunistic infections among hematopoietic stem cell transplant recipients. MMWR Recomm Rep. 2000
Oct;49(RR-10):1-125, CE1-7.
6 Davies BW, Smith JM, Hink EM, Durairaj VD. Increased incidence of rhino-orbital-cerebral mucormycosis after Colorado floodingexternal icon.
Ophthalmic PlastReconstr Surg. 2017 May;33(3S Suppl 1):S148-S151.
7 Brizendine KD, Vishin S, Baddley JW. Antifungal prophylaxis in solid organ transplant recipientsexternal icon. Expert Rev Anti Infect Ther. 2011
May;9(5):571-81.
8 Rogers TR, Slavin MA, Donnelly JP. Antifungal prophylaxis during treatment for haematological malignancies: are we there yet? externaliconBr J
Haemato. 2011 Jun;153(6):681-97.
9 Prenissl J, Jaacks LM, Mohan V,et al. Variation in health system performance for managing diabetes among states in India: a cross-sectional study of
individuals aged 15 to 49 years. BMC Med 2019; 17:92.
10 Lim S, Bae JH, Kwon HS,et al. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol 2021; 17:11–30.
www.turkjphysiotherrehabil.org 3741Turkish Journal of Physiotherapy and Rehabilitation; 32(2)
ISSN 2651-4451 | e-ISSN 2651-446X
11 Prakash H, Chakrabarti A. Global Epidemiology of Mucormycosis. J Fungi (Basel) 2019; 5:26.
12 Chakrabarti A, Kaur H, Savio J, et al. Epidemiology and clinical outcomes of invasive mould infections in Indian intensive care units (FISF study). J
Crit Care 2019; 51:64-70.
13 Rudramurthy SM, Singh G, Hallur V et al. High fungal spore burden with predominance of Aspergillus in hospital air of a tertiary care hospital in
Chandigarh. Indian J Med Microbiol2016; 34:529-532.
14 Ibrahim AS, Spellberg B, Walsh TJ, et al. Pathogenesis of mucormycosis. Clin Infect Dis 2012; 54 (Suppl 1):S16-22.
15 Kathy H, Tony A, Matthew J, et al. A case of invasive pulmonary mucormycosis resulting from short courses of corticosteroids in a well-controlled
diabetic patient. Medical Mycology Case Reports 2020; 29:22-24.
www.turkjphysiotherrehabil.org 3742You can also read

















































