ESMO SUMMIT LATIN AMERICA 2019 - Palliative Care - Clinical Cases Presentation Joao Luiz Chicchi Thomé Oncologist and Palliative doctor - OncologyPRO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ESMO SUMMIT LATIN AMERICA 2019 Palliative Care - Clinical Cases Presentation Joao Luiz Chicchi Thomé Oncologist and Palliative doctor

CONFLICT OF INTEREST DISCLOSURE No conflict of Interest disclosure
ESMO SUMMIT LATIN AMERICA 2019 Case 1
CASE 1
• V.L.A.R., male, 77 years old, married, 2 sons and 2 grandsons, natural from São
Paulo, Brazil. Entrepreneur.
• Smoker from 17 yo to 32 yo, more than 80 cigarettes per day
• Without comorbidity
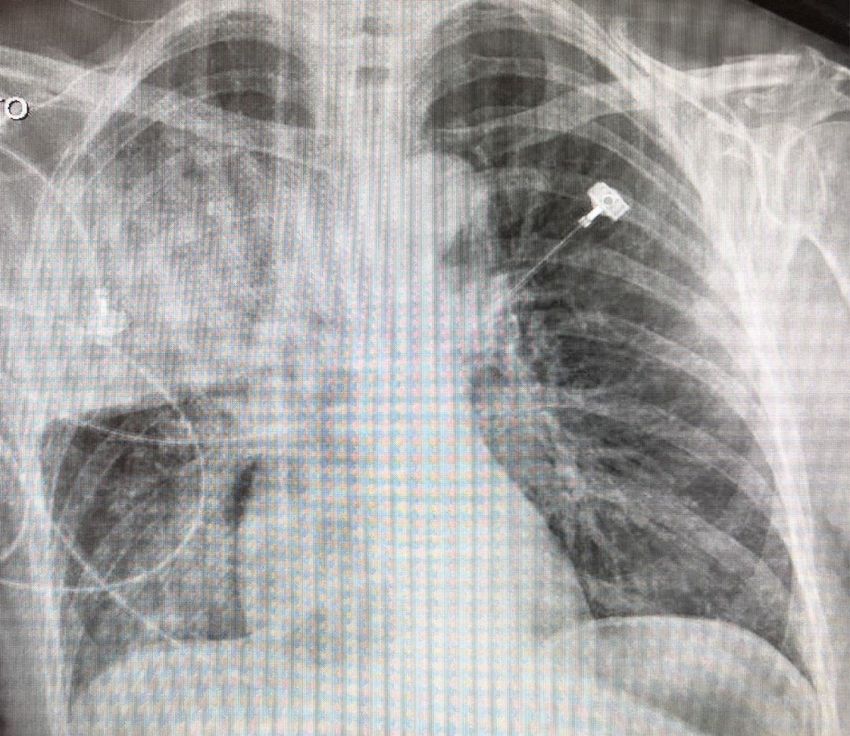
• 2011: X-Ray with suspected pulmonary nodule
◆ Without follow-up or more investigation
• 2017:
◆ August: Started with thoracic pain
◆ Oct: X-Ray with heterogeneous nodule and parenchymal densification adjacent
to the left pulmonary hilum at lingular topography.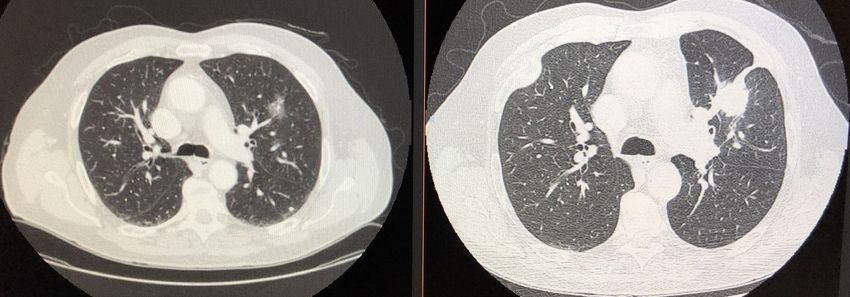
CASE 1
• Nov:
• Thoracic CT and PET CT:
◆ Enlargement lymph node at left pulmonary hilum (1.7 x 1.6cm) with
SUV max 3.9.
◆ Expansive pulmonary lesion in the left upper lobe (7.8cm),
affecting the anterior segment of lingular, associated with adjacent
atelectasic opacities, with SUV max 12.4.
◆ Osteolytic lesion in the 3rd right costal arch (4.7cm), with large
soft parts component bulging the pleural region, infiltrating the
intercostal muscle, with SUV max 7.1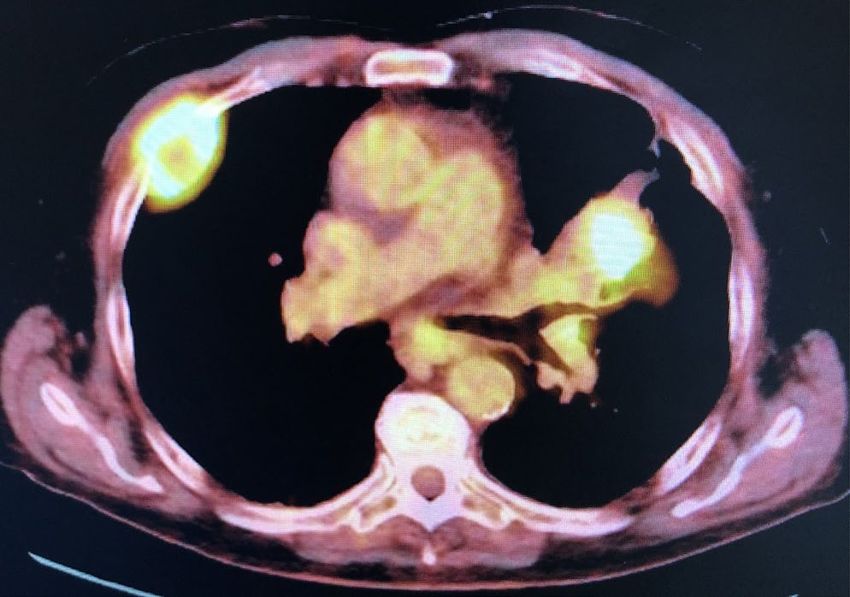
CASE 1
Treatment proposed:
First line:
Carboplatin +
Pemetrexede
(Nov.2017)
2011 2017
Pulmonary
Adenocarcinoma
T3N1M1
with bone metastasisCASE 1
Question 1
After first line therapy with carboplatin and pemetrexed, patient had myelotoxicity
◆
and progression disease with decreased Karnofsky scale from 90 to 60.
What should we do?
Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: Reliability, validity, and guidelines. J Clin Oncology. 1984; 2:187-CASE 1
Treatment proposed:
First line:
Carboplatin +
Pemetrexede
(Nov.2017)
2011 2017 Progression Disease
Adverse Effects
Pulmonary
Adenocarcinoma Second Line:
T3N1M1 Nivolumab
(Jan-Mar.2018)
with bone metastasis
Progression Disease
KPSCASE 1
Question 2
◆ After second line with
nivolumab, patient had
another progression
disease with more
decreased Karnofsky
Scale from 60 to 40.
When should we stop the
oncology therapeutic?
Question 3
◆ This kind of thinking
shrink the expectative of
life?ESMO SUMMIT LATIN AMERICA 2019 Case 2
CASE 2
Same patient of case 1:
◆ After stopped the specific treatment he had an improvement of performance,
getting back to his quite normal activities like walking through his neighborhood,
travel with his family.
◆ After 2 months, started with strong pain at his 3rd costal arch. And became
more anxious.
◆ At this time, he was using patch of buprenorphine, totalizing 15mg/week,
dipyrone 1g every 6h
◆ But without a correct useCASE 2
Tried to improved the analgesic medications
◆ Gabapentin 400mg every 8h and maintenance other medications.
◆ Pain got worse
Question 1
• What to do?
◆ Add more medications?
◆ Try other options like radiotherapy, psychotherapy, acupuncture?CASE 2
Was decided for a combined treatment
◆ Psychotherapy
◆ Radiotherapy: 5 fx of 400cGy at 3rd costal arch and left shoulder (new
progression of disease) on May 2018
Pain was controlled by for 4 months. Started getting worse and really difficult to control
on September 2018
◆ Patient resistance of high doses of opioids
Question 2:
• What to do to control his pain?CASE 2
Indicated intrathecal catheterization by epidural catheter of morphine
◆ Pain better controlled
◆ 2 episodes of intoxication by opioids
◆ Dose reduced and demystified about opioids and adverse effects
◆ Pain controlled till his death on Dec.2018ESMO SUMMIT LATIN AMERICA 2019 Case 3
CASE 3
• D.T.C, female, 85 years old, widow, 3 sons. Housekeeper, natural from São Paulo,
Brazil. Lived alone, with caregiver. Without religion
• Diagnoses:
◆ Neurological degenerative disease
◆ Advanced dementia - totally dependent, without neurological interaction
◆ Rheumatoid arthritis
◆ Non-investigated lung cancer because of her impossibility of treatment if
confirmed
• Hospitalized at December 15, 2018 with pulmonary sepsis from a bronchoaspiration
◆ At the emergency room:
◆ Received Ceftriaxone and Clindamicin
◆ Orotracheal intubation and sent to Intensive Care UnitCASE 3 At a previous conversation, patient said that didn’t want to be machine’s dependent. Her family knew that too. Question 1 • What to do in this case?
CASE 3
• Patient admitted at the ICU at the same day
• Parameters of ventilations was adjusted for her need and medications to prevent
discomfort too
• Talked to the family to understand what they were expecting. And a decision was
made: avoid any kind of discomfort
Question 2: Is the palliative extubation an option? How to do that?CASE 3
• After 2 days, family was distressed with the orotracheal intubation. They were
against this measure, because it was totally different from her wishes. And agreed
with the extubation
◆ Ventilatory parameters at the day of extubation: Support pressure, PEEP 6, SP
12, FiO2 60%, RR 25, V 330
◆ Extubation at 12:15h of Dec 18.2018.
◆ After, was putted a catheter of O2 2L/min
• Patient was transferred to the ward and died on December 20.2018 at 8h,
surrounded by her family as they wanted tooESMO SUMMIT LATIN AMERICA 2019 Case 4
CASE 4
• W.A.S., 69 years old, female, married
• 2015:
◆ March: submitted to screening tests and found a mass at the left ovarian,
without sings or symptoms
◆ PET TC: Hypermetabolic activity at a large mass at the left ovarian and at
retroperitoneal and external iliac lymph nodes (probable secondary
processes)
◆ May: Cytoreduction surgery
• High grade left ovarian adenocarcinoma, with 22.5cm, lymph node positive
and infiltration at the anterior wall of the rectum.CASE 4
◆ 2015
◆ Jun: Chemotherapy 6C Carboplatin + Paclitaxel + Bevacizumab and bevacizumab
as maintenance for 1 year
◆ 2016
◆ November: PD lymph node > Doxorrubicin + Carboplatin 6C till May 2017
◆ 2017
◆ December > PD peritoneum
◆ 2018
◆ Jan - April: Carboplatin + Paclitaxel > PD
◆ April - June: Gencitabin > PD - First episode of Malignant Bowel Obstruction (MBO)
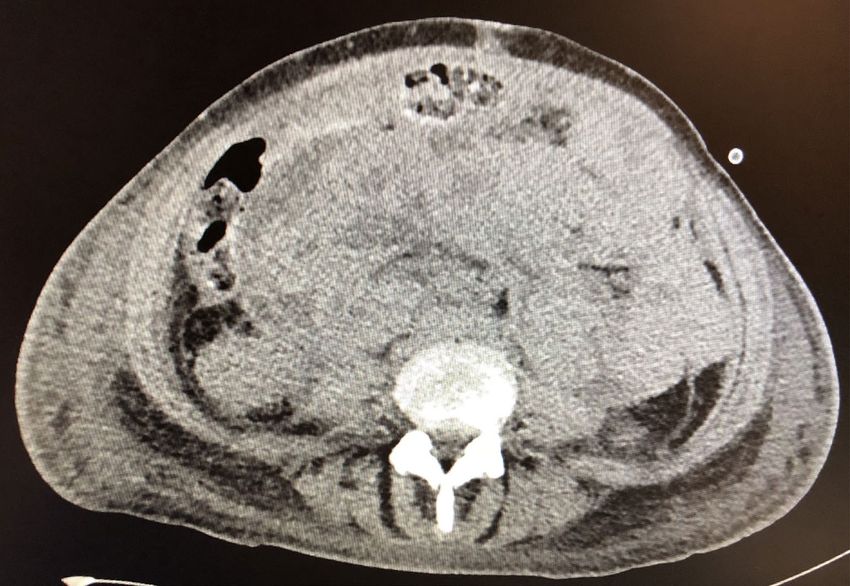
◆ June - July: Pemetrexed > PD and new MBO > HospitalizedCASE 4
Upper tract Obstructed
OBSTRUCTION POINTCASE 4
• July-Oct
◆ Hospitalized to treat the MBO
Question 1
• What are the measures to control the MBO?CASE 4
• July-Oct
◆ Hospitalized to treat the MBO
Question 1
• What are the measures to control the MBO?
◆ Tried clinical measures to revert the MBO, but without success
Question 2
• Invasive measures are adequate? Any other kind of clinical measures can be done?CASE 4
• July-Oct
◆ Hospitalized to treat the MBO
Question 1
• What are the measures to control the MBO?
◆ Tried clinical measures to revert the MBO, but without success
Question 2
• Invasive measures are adequate? Any other kind of clinical measures can be done?
◆ Made a decompressive gastrectomy on 10 Oct. 2018
Question 3
• Palliative sedation is an indication? When should be started?CASE 4
• July-Oct
◆ Hospitalized to treat the MBO
Question 1
• What are the measures to control the MBO?
◆ Tried clinical measures to revert the MBO, but without success
Question 2
• Invasive measures are adequate? Any other kind of clinical measures can be done?
◆ Made a decompressive gastrectomy on 10 Oct. 2018
Question 3
• Palliative sedation is an indication? When should be started?
◆ Initiated sedation on Oct 26, 2018 and patient died 8h afterYou can also read

















































