Enhanced feedback sensitivity to prednisolone in chronic fatigue syndrome
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ARTICLE IN PRESS
Psychoneuroendocrinology (2007) 32, 192–198
Available at www.sciencedirect.com
journal homepage: www.elsevier.com/locate/psyneuen
Enhanced feedback sensitivity to prednisolone in
chronic fatigue syndrome
Walid K. Jerjesa,, Norman F. Taylora, Peter J. Woodb, Anthony J. Clearec,d
a
Department of Clinical Biochemistry, Guy’s, King’s and St Thomas’ School of Medicine, Bessemer Road, London SE5 9RS, UK
b
Regional Endocrine Unit, Southampton General Hospital, Southampton SO16 6YD, UK
c
King’s College London, Institute of Psychiatry, Section of Neurobiology of Mood Disorders, Division of Psychiatry and
Psychological Medicine, De Crespigny Park, London SE5 8AF, UK
d
National Affective Disorders Unit, Bethlem Royal and Maudsley Hospitals, Monk’s Orchard Road, Beckenham,
Kent BR3 3BS, UK
Received 6 September 2006; received in revised form 29 November 2006; accepted 9 December 2006
KEYWORDS Summary
Chronic fatigue syn- Objective: Enhancement of negative feedback control of the HPA axis in patients with
drome; chronic fatigue syndrome (CFS) has been reported using the low dose dexamethasone
Prednisolone; suppression test. We have developed the use of prednisolone (5 mg) as a more
Urinary cortisol; physiologically appropriate alternative to dexamethasone in the investigation of mild
Cortisol metabolites; degrees of glucocorticoid resistance or supersensitivity. The objective of the study was to
Salivary cortisol; use this test to look for alterations in negative feedback control of the HPA axis in CFS
Negative feedback; patients.
Hypothalamo-pitui- Methods: Fifteen patients with CFS were recruited after fulfilling strict criteria including
tary-adrenal axis the absence of comorbid psychiatric diagnosis. They collected urine between 0900 and
1800 h and saliva at 0900 h pre-prednisolone. At midnight, they took prednisolone (5 mg)
orally and then collected urine and saliva at the same intervals the following day.
Results: Salivary cortisol was lower in CFS subjects pre-prednisolone than controls. Urinary
cortisol metabolites were lower in CFS subjects pre-prednisolone, but did not reach
significance. Both measures were significantly lower in CFS subjects post-dose. Mean
percentage suppression of both salivary cortisol and urinary cortisol metabolites was
significantly higher in CFS compared to controls.
Conclusion: There is enhanced sensitivity of the HPA axis to negative feedback in CFS as
demonstrated using the prednisolone suppression test. This provides further evidence of
alterations in the control of the HPA axis in patients with established CFS.
& 2007 Elsevier Ltd. All rights reserved.
Corresponding author. Tel.: +44 20 7346 4131; fax: +44 207 737 7434.
E-mail address: w_jerjes@yahoo.co.uk (W.K. Jerjes).
0306-4530/$ - see front matter & 2007 Elsevier Ltd. All rights reserved.
doi:10.1016/j.psyneuen.2006.12.005ARTICLE IN PRESS
Prednisolone suppression in chronic fatigue syndrome 193
1. Introduction urine approaches. We hypothesised that there would be
enhanced negative feedback sensitivity in patients with CFS
Chronic fatigue syndrome (CFS) is characterised by persis- in comparison to healthy subjects.
tent debilitating fatigue and exhaustion, together with a
number of other characteristic symptoms, unexplained by
identifiable organic disease (Fukuda et al., 1994). Since
many of the symptoms of CFS can also be associated with 2. Materials and methods
glucocorticoid deficiency states, evaluation of HPA axis
activity in CFS has been undertaken in numerous studies. As 2.1. Subjects
a result of this, it has been hypothesised that some features
of CFS are a result of moderate hypocortisolism. The Fifteen patients with CFS (7 males and 8 females) were
majority of the well designed studies in this area have recruited via the CFS clinic at King’s College Hospital (KCH),
demonstrated low levels of cortisol in blood, urine or saliva which sees secondary and tertiary care referrals from the
(reviewed by Cleare, 2003). More recently, we have also south of the United Kingdom. Subjects were interviewed by
found low levels of urinary and salivary free cortisol in a well experienced psychiatrists who used the semi-structured
characterised group of 15 CFS patients free from medication interview for CFS of Sharpe et al. (1997) and DSM-IV to
or comorbid psychiatric disorders (Jerjes et al., 2005, determine the presence of any psychiatric diagnoses.
2006a). However, the research in this area is not entirely Subjects were eligible for inclusion if they fulfilled the
consistent, and some other studies have shown no differ- 1994 Centers for Disease Control (CDC) criteria for CFS
ences in serum cortisol levels (Racciatti et al., 1998; (Fukuda et al., 1994) without any exclusionary psychiatric
Altemus et al., 2001), and we have found no difference in disorder as per these criteria. Further inclusion criteria
24 h urinary cortisol metabolite excretion between CFS and stipulated an age range of 25–60 years and the absence of
control subjects (Jerjes et al., 2006c). any history of neurological, endocrine or cardiovascular
A second hypothesis is that CFS symptoms result from disorder. In order to obtain as pure a measure of the HPA axis
alterations in central neuroendocrine pathways underlying as possible, we tested only patients who had never taken
the control of the HPA axis. Specifically, it has been any psychotropic medication or had been abstinent from
suggested that there is deficient suprahypothalamic drive, such medication for at least 2 months. Furthermore,
reflected in reduced hypothalamic output of corticotropin- although the modification in 1994 of the original CDC
releasing hormone (CRH, Demitrack et al., 1991). Being the diagnostic criteria permitted inclusion of patients with
principal modulator of the stress response, CRH not only comorbid major depression or anxiety disorders, patients
modulates endocrine and autonomic responses but also with a current major depressive episode or anxiety disorder
influences nociception and behaviour (Clauw and Chrousos, as defined by DSM-IV criteria were excluded from this study
1997). Several symptoms such as lethargy, pain and fatigue because of their potential impact on the HPA axis. Patients
have been associated with a deficiency of hypothalamic CRH were recruited consecutively over about 6 months. We have
secretion (Gold and Chrousos, 1999). reported previously on these CFS patients in terms of the
Third, enhancement of negative feedback control of the diurnal rhythm of salivary, urinary cortisol and cortisol
HPA axis has also been proposed as a cause of a hypofunc- metabolites, and found that they had lower salivary and
tional HPA axis in CFS (DeKloet et al., 1998). Preliminary urinary cortisol across the day without any differences in
reports suggested a heightened negative feedback in CFS cortisol metabolites (Jerjes et al., 2005, 2006a).
subjects using dexamethasone (Poland et al., 1996) or Twenty healthy volunteers (10 males and 10 females) as
hydrocortisone infusion (Lavelle and Dinan, 1996), while described in Jerjes et al. (2006b) were recruited from
Gaab et al. (2002) examined salivary cortisol levels before among the staff and student body at KCH and were matched
and after low dose dexamethasone (0.5 mg), finding greater for age and BMI with CFS patients. They were all assessed to
suppression in CFS, although levels of salivary cortisol in CFS be in good health without any serious medical illness or
were not different from controls pre-medication. However, history of psychiatric disorder. Subjects were all studied
dexamethasone may not be physiologically appropriate, during wintertime hours, between October 2002 and March
since it has much higher relative affinity for the glucocorti- 2003. All subjects had normal dietary habits, taking break-
coid receptor over the mineralocorticoid receptor (DeKloet fast, lunch and dinner at about the same time. All subjects
et al., 1998), does not bind to corticosteroid binding were asked to limit their intake of caffeine and alcohol
globulin (Pugeat et al., 1981), and has a much longer half during the collection period. All subjects were instructed to
life compared with cortisol (Cassidy et al., 2000). carry out sample collections at weekends to avoid possible
We have recently reported the use of prednisolone (5 mg) increase of cortisol levels, which might result from stress on
for investigation of mild degrees of glucocorticoid resistance working days. No female subjects were on the oral contra-
or hypersensitivity, based on cortisol assay in a convenient ceptive or pregnant. All subjects habitually went to bed
pre and post dose saliva sample at 0900 h or on a urine between 2300 and 0100 h and got up between 0700 and
sample collected 0900–1800 h (Jerjes et al., 2006b). 0800 h. All subjects gave written, informed consent and
Suppression was found to be approximately 50% for both ethical approval for the study was obtained from our local
saliva and urine in healthy subjects, but correlation committee.
between these measures was not established. Thus, the Patients and healthy controls collected urine between
objective of the study was to explore alterations in negative 0900 and 1800 h and provided saliva at 0900 h only (Day 1).
feedback control of the HPA axis in CFS patients, using the At midnight, all subjects took prednisolone (5 mg) and
prednisolone suppression test and assessing both saliva and collected urine and provided saliva at the same times theARTICLE IN PRESS
194 W.K. Jerjes et al.
following day. Percentage suppression of these measures 2.6. Cortisol metabolite measurements
was calculated as described below.
Urinary steroid profile analysis was carried out by high-
resolution gas chromatography of methyloxime-trimethylsi-
2.2. Questionnaires lyl ether (MO-TMS) derivatives as previously described
(Taylor, 2006). The intra- and interassay CVs were between
All subjects completed the Hospital Anxiety and Depression 7.1–21.1%, and 11.2–21.9%, respectively for different
scale (HADS) (Snaith and Zigmond, 1986) for symptoms of metabolites. Cortisol metabolites were calculated as mg/
anxiety and depression; and the Pittsburgh Sleep Quality 9 h period. Derived sums of total urinary cortisol metabolites
Index (PSQI) (Buysse et al., 1989) for sleep disturbance. were as previously reported (Trainer et al., 2001). Total
Patients completed further questionnaires to characterise cortisol metabolites were determined from the sum
their illness: the Chalder Fatigue Scale (Chalder et al., 1993) of tetrahydrocortisone (THE), tetrahydrocortisol (THF),
for fatigue severity; and the Work and Social Adjustment allo-tetrahydrocortisol (5aTHF), a-cortolone, b-cortolone,
Scale (Marks, 1986) for disability. a-cortol, and b-cortol.
2.3. Urinary collections 2.7. Statistical analysis
Subjects were provided with standard containers for urine Analysis was undertaken in two ways, as per the prior
and given clear instructions on how to complete the literature. First, we performed a repeated measures
collection. They were asked to empty their bladder normally analysis of variance for both total urinary cortisol metabo-
at 0900 h and to collect in the container all urine passed lites and salivary cortisol using before and after predniso-
between 0900 and 1800 h on Day 1. Prednisolone (5 mg) was lone administration as the within group factor and subject
taken orally at midnight at the end of Day 1. On Day 2, group (CFS or control) as the between group factor. Since
subjects were again asked to empty their bladder at 0900 h not all of the raw data were normally distributed, the data
and to collect all urine between 0900 and 1800 h. Upon were log transformed prior to this analysis. Second, we
receipt of the specimen at the laboratory, the volume was calculated a summary measure for the percentage suppres-
noted, and after vigorous shaking, two 20 ml aliquots were sion by prednisolone using the following formula:
taken for freezing at 40 1C prior to subsequent analysis.
ððpre-prednisolone value post-prednisolone valueÞ
=ðpre-prednisolone valueÞÞ 100.
2.4. Saliva collections
Since the percentage suppression data were normally
Saliva was collected using plain Salivettes (Sarstedt, distributed, group comparisons were made by the indepen-
Leicester, UK). Subjects were asked not to take a sample dent t-test (using SPSS for windows V 11). Raw data and
after brushing their teeth in order to avoid falsely high demographic data were also analysed using t-tests, with log
cortisol values due to plasma exudates from minor bleeding transformation for data that was not normally distributed as
in the oral cavity. For the 10 min prior to each sample, indicated.
subjects were asked to remain sitting, not to drink anything, Data are expressed as mean7standard deviation.
smoke or chew gum. During saliva collections, subjects were
instructed not to touch the samples with their hands. In
3. Results
association with urine collections, subjects provided one
0900 h sample on the first morning and provided another
saliva sample at 0900 h the following morning after taking 3.1. Demographic and questionnaire data
prednisolone (5 mg) at midnight. Subjects then kept the
samples in their refrigerator overnight and returned them to There was no difference in mean age and BMI between the
the laboratory the next day. 15 patients with CFS and the 20 controls (mean age (yrs);
3577.9 and 32711.4, p ¼ 0.4; and BMI (kg/m2); 24.475.0
and 23.774.3, respectively, p ¼ 0.6). Patients with CFS had
2.5. Saliva cortisol measurements disrupted sleep compared to controls; total PSQI scores
were 9.873.3 and 3.172.1, respectively, po0.01). The CFS
Upon receipt at the laboratory, saliva samples were subjects had higher levels of self-rated symptoms of anxiety
centrifuged and the clear fluid stored at 20 1C until and depression, compared to controls. Scores for the HADS
analysis. After defrosting, salivary cortisol was analysed by scale were 7.375.6 and 3.573.0, po0.01 for anxiety and
direct immunofluorimetric assay using the ‘‘DELFIA’’ system. 8.073.9 and 2.372.6, po0.01, respectively for depression.
Microtitre strip format plates were coated with goat anti- The CFS subjects reported high mean scores of fatigue on
rabbit antiserum, and samples were incubated with rabbit the Chalder fatigue scale: all scored above the ‘‘caseness’’
anti-cortisol antiserum 2330-5105 (Biogenesis Ltd, Poole, cut off score of 4 using the categorical scoring method,
UK) or rabbit anti-cortisone antiserum N-137 and the while the mean using the Likert scoring method was
corresponding steroid-3-CMO-biotin tracers. Europium-la- 25.173.0. CFS patients also reported high levels of
belled neutralite avidin was used to detect bound tracer disability on the Work and Social Adjustment Scale
(Wood et al., 1997). Inter-assay imprecisions (CV%) were less (22.574.7). The mean duration of illness for CFS patients
than 12% for salivary cortisol results over 2 nmol/l. was 2.770.6 years.ARTICLE IN PRESS
Prednisolone suppression in chronic fatigue syndrome 195
3.2. Salivary cortisol 100
Mean levels of cortisol in saliva at 0900 h were lower in Controls
90
patients with CFS than controls at baseline (6.973.3 nmol/l CFS
and 11.575.2 nmol/l, respectively, t ¼ 3.0, p ¼ 0.005).
Percentage Suppression After Prednisolone
80
After prednisolone (5 mg) administration, mean levels of
salivary cortisol were again significantly lower in CFS
compared to controls (3.371.7 and 6.773.2 nmol/l, re- 70
spectively, t ¼ 4.4, po0.001 on log transformed data).
The repeated measures analysis of variance showed: a 60
significant overall effect of group, cortisol being lower in
CFS subjects (F 1,33 ¼ 15.2, po0.001); a significant effect 50
of prednisolone in lowering cortisol (F 1,33 ¼ 344,
po0.0001); and a significant group by prednisolone inter-
action, with a larger effect seen in the CFS group (F 40
1,33 ¼ 9.5, p ¼ 0.004).
30
3.3. Total urinary cortisol metabolites
20
The baseline levels of urinary cortisol metabolites
(0900–1800 h) did not differ significantly between CFS 10
patients and controls (18607432 and 22087908 mg/9 h,
respectively, t ¼ 1.0, p ¼ 0.32 on log transformed data).
0
After taking prednisolone (5 mg), urinary cortisol metabolite Urinary Cortisol Salivary
levels were significantly lower in patients with CFS Metabolites Cortisol
compared to controls (3017160 and 9597356 mg/9 h,
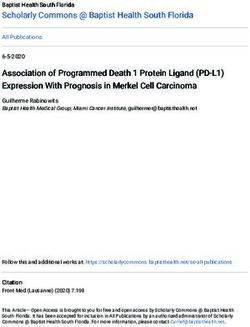
respectively, t ¼ 6.6, po0.0001). Figure 1 Scatter plot showing each individual’s percentage
The repeated measures analysis of variance showed: a suppression after the administration of prednisolone at 12
significant overall effect of group, total cortisol metabolites midnight, measured by urinary cortisol metabolites
being lower in CFS subjects (F 1,33 ¼ 29.7, po0.001); a (0900–1800 h) and salivary cortisol (0900 h) the following day.
significant effect of prednisolone in lowering total cortisol Healthy controls are shown with closed circles and Chronic
metabolites (F 1,33 ¼ 253, po0.0001); and a significant Fatigue Syndrome (CFS) patients with open diamonds. CFS
group by prednisolone interaction, with a larger effect seen patients showed a significantly higher mean suppression after
in the CFS group (F 1,33 ¼ 42.4, po0.001). prednisolone with both measures (see text).
3.4. Percentage suppression by prednisolone
percentage suppression of urinary cortisol metabolites was
Mean percentage suppression of salivary cortisol at 0900 h higher than for saliva in both groups, and the difference
and urinary cortisol metabolites (0900–1800 h) was signifi- between CFS and controls was larger, probably because
cantly higher in CFS compared to controls. For salivary urinary cortisol metabolites show a long period of suppres-
cortisol, suppression was 52710% in patients and 41712% in sion post dose (up to 18 h) (Jerjes et al., 2006b). This might
controls (t ¼ 3.0, p ¼ 0.005). For Urinary cortisol meta- be because salivary levels only provide a snapshot at 0900 h,
bolites, suppression was 82711% in patients and 5678% in which might not reflect the overall suppression as accu-
controls (t ¼ 8.5, po0.0001). These results are shown rately.
graphically in Fig. 1. This study has several advantages over previous work.
Thus, analysis by percentage suppression indicated the First, an increased negative feedback has been confirmed
same findings as the repeated measures analysis of variance: using two biological measures, salivary free cortisol and
for both salivary cortisol and total urinary cortisol metabo- urinary cortisol metabolites. Second, patients in whom
lites, there was a larger suppressive effect of prednisolone there was comorbid psychiatric disorder or had prescribed
in CFS subjects than controls. medication that may have affected the HPA axis have been
excluded. Third, prednisolone was used in place of
4. Discussion dexamethasone. This has a more physiological action, with,
for example, a relative potency at glucocorticoid and
This is the first study to examine response of the HPA axis to mineralocorticoid receptors similar to that of the main
prednisolone in CFS. The findings support suggestions that endogenous corticosteroid cortisol, and having privileged
there is enhanced negative feedback on the HPA axis in CFS. CNS penetration (DeKloet et al., 1998). Dexamethasone has
The timing of sample collection was optimised for normal poor CNS penetration and thus only activates glucocorticoid
subjects (Jerjes et al., 2006b) but it is appropriate for our receptors and may miss the important physiological inter-
study group of CFS patients since we have demonstrated actions between mineralocorticoid and glucocorticoid re-
that they have a normal circadian rhythm for both saliva ceptors. The poor CNS penetration is due to the effect of
(Jerjes et al., 2005) and urine (Jerjes et al., 2006a) The multiple drug resistance (mdr1a) P-glycoprotein (BourgeoisARTICLE IN PRESS 196 W.K. Jerjes et al. et al., 1993) at the level of the endothelial cells of the effective in some patients with CFS (Cleare et al., 1999) and blood-brain barrier (Cordon-Cardo et al., 1989). It is that those with higher GR sensitivity were most likely to possible, for example, that changes in the glucocorticoid respond to therapy (Cleare et al., 2001). receptor might be compensated by changes in the miner- The present study has some potential limitations. First, it alocorticoid receptor. Given this more physiological effect is possible that this is a cohort with low HPA axis function of prednisolone, our finding of enhanced suppression in and thus the findings require replication elsewhere in a response to prednisolone is strong evidence that the separate cohort. However, in the literature, half of well- response of the HPA axis to endogenous negative feedback designed studies measuring cortisol in CFS using well- is enhanced in CFS. validated methods do show hypocortisolism. Second, exact These findings extend those of Gaab et al. (2002) who awakening time was not recorded in the current study, found heightened HPA sensitivity in CFS, measuring salivary although all subjects got up between 0700 and 0800 h. Data cortisol before and after low dose dexamethasone (0.5 mg). presented by Gaab et al. (2002) indicate a post-awakening In vitro studies of feedback provide further support for rise in salivary cortisol up to 30 min in both CFS and control enhanced GR sensitivity in CFS. Visser et al. (1998) found in subjects. Since our subjects were sampled at least 60 min CD4T lymphocytes from a small group of patients with CFS, post awakening the interval between awakening and that inhibition of CD4 proliferation occurred with a lower sampling should not have influenced the results. Third, the concentration of dexamethasone than in controls. (Visser et menstrual cycle phase in female subjects was not con- al., 2001) and in a further study of 10 CFS and 14 controls trolled. Altemus et al. (1997) have demonstrated an showed that this was not due to increased GR affinity or effect of menstrual cycle phase on dexamethasone re- number. Two studies do not support the presence of sponse, with reduced expression in lymphocytes of GR mRNA enhanced GR function in CFS. One study reported only in in the luteal phase. Another study has suggested that women abstract (Majeed et al., 1995) reported a decreased GH in the luteal phase show a significantly higher salivary response to dexamethasone, but some patients in the cortisol in response to a psychosocial stressor compared to sample were also suffering with irritable bowel syndrome women in the follicular phase (Kirschbaum et al., 1999). and fibromyalgia. Also, this study did not measure feedback Several others have not found such an association between sensitivity directly, and the validity of the Dexamethasone- the HPA axis and menstrual cycle phase (Kudielka and GH response as an index of GR function is not well Kirschbaum, 2003; Cevik et al., 2004). It is thus possible that established, especially as GH function itself may be these results are confounded by influence of menstrual cycle disturbed in CFS (Moorkens et al., 1998). The second study phase on prednisolone-induced suppression of the HPA axis. (Kavelaars et al., 2000) found a reduced effect of Fourth, It has been noted that HPA axis changes in CFS are dexamethasone on white cells, using T cell proliferation apparent late in the course of the illness (Cleare, 2003) but as a marker, but this was in adolescent patients, not in do not accompany the early stages of chronic fatigue (Candy adults, and there is little understanding of how CFS or the et al., 2003). The patients in this study had been ill for a HPA axis compares between adolescents and older subjects relatively short duration (mean 2.770.6 years) in the with CFS. context of CFS. Thus they might not have developed HPA The suggestion that there is enhanced negative feedback axis changes to the extent that might be found in patients ill and upregulated GR function in CFS is consistent with the for longer periods. Nevertheless, they did exhibit lower observed reports of mild hypocortisolism in CFS (Cleare, salivary cortisol levels and numerically (but not statistically) 2003). Although the temporal link between the two findings lower urinary cortisol metabolite levels (Jerjes et al., 2005, cannot be tested, it is plausible that the enhanced negative 2006a). feedback is one of the aetiological factors in the develop- It has been reported that hypocortisolism in CFS is likely ment of hypocortisolism in CFS. It has previously been noted to be the result of a number of interacting influences, that enhanced negative feedback in CFS is similar to the including current or previous stressors, but also psychiatric findings in a number of other conditions that may be stress status and medication (where not controlled for), nutri- related, such as posttraumatic stress disorder (Yehuda et tional status, sleep disturbance, physical activity levels and al., 1995), women with histories of childhood sexual abuse deconditioning (reviewed by Cleare, 2003). It is therefore (Stein et al., 1997), adolescents exposed to earth quake- likely that any observed alteration to negative feedback in related trauma (Goenjian et al., 1996), burnout syndrome CFS would have a multifactorial origin. (Pruessner et al., 1999), and chronic pelvic pain (Heim et In conclusion, these findings of enhanced HPA axis al., 1998). Gaab et al. (2002) hypothesised that precipitat- suppression in CFS by prednisolone suggests that there is ing or chronic stress may be the common factor underlining enhanced physiological negative feedback in CFS and the similar findings in each of these conditions. Supporting upregulated GR and/or MR receptors. This provides further this, a recent experimental study by Zarkovic et al. (2003) evidence of alterations to the control of the HPA axis in examined the effect of prolonged psychological stress on patients with established CFS. This state of enhanced cortisol secretion induced by continuous air raids, after physiological negative feedback could be a factor underlying elimination of the stress-inducing factor, in five healthy the observed hypocortisolism in some patients (including the adults. They found a transient suppression of the HPA axis, group studied here), or could be a response to stress or other manifested by low morning cortisol and reduced cortisol effects of the illness such as sleep and activity levels. response to ACTH. Further work assessing the status of both GR and MR It also appears that enhanced GR receptor function may receptors at various stages of the genesis of CFS may be be of clinical relevance. We have found that low doses of helpful in understanding the role of the HPA axis in this hydrocortisone to replace the hypothesised deficiency are condition.
ARTICLE IN PRESS
Prednisolone suppression in chronic fatigue syndrome 197
Acknowledgement to its definition and study. International Chronic Fatigue
Syndrome Study Group. Ann. Intern. Med. 121, 953–959.
We thank Dorothy Blair for her excellent help in patient Gaab, J., Huster, D., Peisen, R., Engert, V., Schad, T., Schurmeyer,
recruitment and sample collection. T.H., Ehlert, U., 2002. Low-dose dexamethasone suppression
test in chronic fatigue syndrome and health. Psychosom. Med.
64, 311–318.
Goenjian, A.K., Yehuda, R., Pynoos, R.S., Steinberg, A.M., Tashjian,
References M., Yang, R.K., Najarian, L.M., Fairbanks, L.A., 1996. Basal
cortisol, dexamethasone suppression of cortisol, and MHPG in
Altemus, M., Redwine, L., Leong, Y.M., Yoshikawa, T., Yehuda, R., adolescents after the 1988 earthquake in Armenia. Am. J.
Detera-Wadleigh, S., Murphy, D.L., 1997. Reduced sensitivity to Psychiatry 153, 929–934.
glucocorticoid feedback and reduced glucocorticoid receptor Gold, P.W., Chrousos, G.P., 1999. The endocrinology of melancholic
mRNA expression in the luteal phase of the menstrual cycle. and atypical depression: relation to neurocircuitry and somatic
Neuropsychopharmacology 17, 100–109. consequences. Proc. Assoc. Am. Physicians 111, 22–34.
Altemus, M., Dale, J.K., Michelson, D., Demitrack, M.A., Gold, P.W., Heim, C., Ehlert, U., Hanker, J.P., Hellhammer, D.H., 1998. Abuse-
Straus, S.E., 2001. Abnormalities in response to vasopressin related posttraumatic stress disorder and alterations of the
infusion in chronic fatigue syndrome. Psychoneuroendocrinology hypothalamic-pituitary-adrenal axis in women with chronic
26, 175–188. pelvic pain. Psychosom. Med. 60, 309–318.
Bourgeois, S., Gruol, D.J., Newby, R.F., Rajah, F.M., 1993. Jerjes, W.K., Cleare, A.J., Wessely, S., Wood, P.J., Taylor, N.F.,
Expression of an mdr gene is associated with a new form of 2005. Diurnal patterns of salivary cortisol and cortisone output in
resistance to dexamethasone-induced apoptosis. Mol. Endocri- chronic fatigue syndrome. J. Affect. Disord. 87, 299–304.
nol. 7, 840–851. Jerjes, W.K., Peters, T.J., Taylor, N.F., Wood, P.J., Wessely, S.,
Buysse, D.J., Reynolds, C.F., Monk, T.H., Berman, S.R., Kupfer, D.J., Cleare, A.J., 2006a. Diurnal excretion of urinary cortisol,
1989. The Pittsburgh Sleep Quality Index: a new instrument for cortisone, and cortisol metabolites in chronic fatigue syndrome.
psychiatric practice and research. Psychiatry Res. 28, 193–213. J. Psychosom. Res. 60, 145–153.
Candy, B., Chalder, T., Cleare, A.J., Peakman, A., Skowera, A., Jerjes, W.K., Cleare, A.J., Wood, P.J., Taylor, N.F., 2006b.
Wessely, S., Weinman, J., Zuckerman, M., Hotopf, M., 2003. Assessment of subtle changes in glucocorticoid negative feed-
Predictors of fatigue following the onset of infectious mono- back using prednisolone: comparison of salivary free cortisol and
nucleosis. Psychol. Med. 33, 847–855. urinary cortisol metabolites as endpoints. Clin. Chim. Acta. 364,
Cassidy, F., Ritchie, J.C., Verghese, K., Carroll, B.J., 2000. 279–286.
Dexamethasone metabolism in dexamethasone suppression test Jerjes, W.K., Taylor, N.F., Peters, T.J., Wessely, S., Cleare, A.J.,
suppressors and nonsuppressors. Biol. Psychiatry 47, 677–680. 2006c. Urinary cortisol and cortisol metabolite excretion in
Cevik, R., Gur, A., Acar, S., Nas, K., Sarac, A.J., 2004. Hypotha- Chronic Fatigue Syndrome Psychosom. Med 68, 578–582.
lamic-pituitary-gonadal axis hormones and cortisol in both Kavelaars, A., Kuis, W., Knook, L., Sinnema, G., Heijnen, C.J., 2000.
menstrual phases of women with chronic fatigue syndrome and Disturbed neuroendocrine-immune interactions in chronic fati-
effect of depressive mood on these hormones. BMC Musculoske- gue syndrome. J. Clin. Endocrinol. Metab. 85, 692–696.
let. Disord. 5, 47–52. Kirschbaum, C., Kudielka, B.M., Gaab, J., Schommer, N.C.,
Chalder, T., Berelowitz, G., Pawlikowska, T., Watts, L., Wessely, S., Hellhammer, D.H., 1999. Impact of gender, menstrual cycle
Wright, D., Wallace, E.P., 1993. Development of a fatigue scale. phase, and oral contraceptives on the activity of the hypotha-
J. Psychosom. Res. 37, 147–153. lamus-pituitary-adrenal axis. Psychosom. Med. 61, 154–162.
Clauw, D.J., Chrousos, G.P., 1997. Chronic pain and fatigue Kudielka, B.M., Kirschbaum, C.A., 2003. Wakening cortisol re-
syndromes: overlapping clinical and neuroendocrine features sponses are influenced by health status and awakening time but
and potential pathogenic mechanisms. Neuroimmunomodulation not by menstrual cycle phase. Psychoneuroendocrinology 28,
4, 134–153 Review. 35–47.
Cleare, A.J., 2003. The neuroendocrinology of chronic fatigue Lavelle, E., Dinan, T.G., 1996. Hypothalamo-pituitary-adrenal
syndrome. Endocr. Rev. 24, 236–252 Review. function in chronic fatigue syndrome: a study of fast feedback
Cleare, A.J., Heap, E., Malhi, G.S., Wessely, S., O’Keane, V., Miell, mechanisms. Royal College of Surgeons of Ireland Research
J., 1999. Low-dose hydrocortisone in chronic fatigue syndrome: Meeting, Dublin, Ireland.
a randomised crossover trial. Lancet 353, 455–458. Majeed, T., Dinan, T.G., Thakore, J., Gray, C., Behan, P., 1995.
Cleare, A.J., Sookdeo, S., Jones, J., O’Keane, V., Miell, J., 2001. Defective dexamethasone included growth release in chronic
Plasma leptin in chronic fatigue syndrome, and a placebo- fatigue syndrome; evidence for glucocorticoid receptor resis-
controlled study of the effects of low-dose hydrocortisone on tance and lack of plasticity? J. Ir. Coll. Physicians Surg. 24,
leptin secretion. Clin. Endocrinol. 55, 113–119. 20–24.
Cordon-Cardo, C., O’Brien, J.P., Casals, D., Rittman-Grauer, L., Marks, I., 1986. Behavioural Psychotherapy: Maudsley Pocket Book
Biedler, J.L., Melamed, M.R., Bertino, J.R., 1989. Multidrug- of Clinical Management. Bristol, Wright.
resistance gene (P-glycoprotein) is expressed by endothelial Moorkens, G., Wynants, H., Abs, R., 1998. Effect of growth hormone
cells at blood brain barrier sites. Proc. Natl. Acad. Sci. USA 86, treatment in patients with chronic fatigue syndrome: a
695–698. preliminary study. Growth. Horm. IGF. Res. 8, 131–133.
DeKloet, E.R., Vreugdenhil, E., Oitzl, M.S., Joels, M., 1998. Brain Poland, R.E., Lin, K-M., Lutchmansingh, P., McCracken, J.P., 1996.
corticosteroid receptor balance in health and disease. Endocr. Biological markers in CFS and neurasthenia. X World Congress of
Rev. 19, 269–301. Psychiatry, vol. 1, Madrid, Spain, p. 184.
Demitrack, M.A., Dale, J.K., Straus, S., Laue, L., Listwak, S.J., Pruessner, J.C., Hellhammer, D.H., Kirschbaum, C., 1999. Burnout,
Kruesi, M.J., Chrousos, G.P., Gold, P.W., 1991. Evidence for perceived stress, and cortisol responses to awakening. Psycho-
impaired activation of hypothalamic-pituitary-adrenal axis in som. Med. 61, 197–204.
patients with chronic fatigue syndrome. J. Clin. Endocrinol. Pugeat, M.M., Dunn, J.F., Nisula, B.C., 1981. Transport of steroid
Metab. 73, 1224–1234. hormones: interaction of 70 drugs with testosterone-binding
Fukuda, K., Straus, S.E., Hickie, I., Sharpe, M.C., Dobbins, J.G., globulin and corticosteroid-binding globulin in human plasma. J.
1994. The chronic fatigue syndrome: a comprehensive approach Clin. Endocrinol. Metab. 53, 69–75.ARTICLE IN PRESS
198 W.K. Jerjes et al.
Racciatti, D., Sensi, S., DeRemigis, P., Barberio, A., DiSciascio, T., feron-gamma production and increased sensitivity to dexa-
Pizzigallo, E., 1998. Neuroendocrine aspects of chronic fatigue methasone. J. Infect. Dis. 177, 451–454.
syndrome. Am. J. Med. 104, 1S–3S. Visser, J., Lentjes, E., Haspels, I., Graffelman, W., Blauw, B.,
Sharpe, M., Chalder, T., Palmer, I., Wessely, S., 1997. Chronic DeKloet, R., Nagelkerken, L., 2001. Increased sensitivity to
fatigue syndrome. A practical guide to assessment and manage- glucocorticoids in peripheral blood mononuclear cells of chronic
ment. Gen. Hosp. Psychiatry 19, 185–199. fatigue syndrome patients, without evidence for altered density
Snaith, R.P., Zigmond, A.S., 1986. The hospital anxiety and or affinity of glucocorticoid receptors. J. Invest. Med. 49,
depression scale. Br. Med. J. (Clin. Res. Ed). 292, 344. 195–204.
Stein, M.B., Yehuda, R., Koverola, C., Hanna, C., 1997. Enhanced Wood, P.J., Kilpatrick, K., Barnard, G., 1997. New direct salivary
dexamethasone suppression of plasma cortisol in adult women cortisol and cortisone assays using the ‘‘Delfia’’ system. J.
traumatized by childhood sexual abuse. Biol. Psychiatry 42, 680–686. Endocrinol. 155, 71.
Taylor, N.F., 2006. Urinary steroid profiling. Methods Mol. Biol. 324, Yehuda, R., Boisoneau, D., Lowy, M.T., Giller, E.L., 1995. Dose-
159–175 Review. response changes in plasma cortisol and lymphocyte glucocorti-
Trainer, P.J., Drake, W.M., Perry, L.A., Taylor, N.F., Besser, G.M., coid receptors following dexamethasone administration in
Monson, J.P., 2001. Modulation of cortisol metabolism by the combat veterans with and without posttraumatic stress disorder.
growth hormone receptor antagonist pegvisomant in patients Arch. Gen. Psychiatry 52, 583–593.
with acromegaly. J. Clin. Endocrinol. Metab. 86, 2989–2992. Zarkovic, M., Stefanova, E., Ciric, J., Penezic, Z., Kostic, V.,
Visser, J., Blauw, B., Hinloopen, B., Brommer, E., DeKloet, E.R., Sumarac-Dumanovic, M., Macut, D., Ivovic, M.S., Gligorovic,
Kluft, C., Nagelkerken, L., 1998. CD4T lymphocytes from P.V., 2003. Prolonged psychological stress suppresses cortisol
patients with chronic fatigue syndrome have decreased inter- secretion. Clin. Endocrinol. (Oxf). 59, 811–816.You can also read