Treatment Options in Alopecia Areata - Avid Science
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hair Disorders Chapter 09 Treatment Options in Alopecia Areata Nilgun Senturk* Department of Dermatology, Ondokuz Mayis University School of Medicine, Turkey * Corresponding Author: Nilgun Senturk, Department of Dermatology, On- dokuz Mayis University School of Medicine, Samsun, Turkey, Tel: +90 533 725 68 30; Fax. +90 362 457 60 41; Email: senturk.nilgun@gmail.com First Published April 23, 2018 Copyright: © 2018 Nilgun Senturk. This article is distributed under the terms of the Creative Commons Attribu- tion 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give ap- propriate credit to the original author(s) and the source. 2 www.avidscience.com

Hair Disorders
Abstract
Different treatment options including topical, intralesional, and
systemic agents, as well as devices, are available for the treatment of
alopecia areata, but evidence based data is sparse for most of them.
Remission rates may be partly attributed to spontaneous remission,
which is expected to occur during the course of the disease. Treat-
ment choice in alopecia areata depends on several factors such as se-
verity, extent of the disease, age of the patient, associated diseases,
and involvement of life quality. In this chapter, treatment options and
practical considerations will be presented.
Topical Agents
Topical and Intralesional Steroids
Topical and intralesional steroids are the treatment of choice
for patients with limited alopecia areata located on the eyebrows and
scalp and using corticosteroids needs attention for maximizing effi-
cacy while minimizing side effects [1].
Topical Corticosteroids
Topical corticosteroids are preferred in the first step for children
and adults in which intralesional steroids are not suitable. Although
they are less effective than steroid injections they might be effective
approximately 50 % of patients [2-4].
A variety of formulations are available including lotions, creams,
ointments, foams and sprays. The choice depends on the features of
the area to be treated. Usually use of high potency topical corticoster-
oids are preferred due to higher efficacy. Application under occlusion
increases the potency of topical corticosteroids but also side effects.
For long term use, topical steroids should be applied as on-and-off
use with intervals. Initial signs of improvement can take six to twelwe
weeks with high rates of relapse after discontinuation [2,3].
www.avidscience.com 3
Hair Disorders
Intralesional Corticosteroids
Intralesional corticosteroid injections should be performed on
both existing and newly forming patches of alopecia. For this pur-
pose, triamcinolone acetonide is commonly used and it is more effec-
tive than topical treatment, such as steroids and calcineurin inhibitors
[5,6]. The dose per visit is determined by the extent of disease and
tolerance of the patient (Table 1). Clinical improvement takes two to
six weeks and at the end of six months, if there is no response alterna-
tive treatments may be attempted [4,6].
Table 1: Principals of intralesional corticosteroid injection.
▶▶ Before injection dilute Triamcinolone acetonide as follows
▶▶ 2.5 to 5.0 mg/mL is on the face, eyebrow, beard
▶▶ 5 to 10 mg/mL on the scalp
▶▶ Injection depth should be deep dermis or upper subcutis
▶▶ In order to reduce pain;
▶▶ Inject with 30-gauge needle
▶▶ In small volumes
▶▶ Into multiple sites
▶▶ With 1 cm apart
▶▶ Do not exceed 40 mg per session
▶▶ Repeat treatment every 4-6 weeks if necessary
▶▶ Stop treatment if complete regrowing occurs or no response at the end of 6 months
It should be kept in mind that, with multiple injections and high-
er concentrations, side effects may occur. Topical and intralesional
corticosteroids have similar side effects such as, local skin atrophy,
folliculitis, telangiectasias, hypopigmentation, and hypothalamic–
pituitary–adrenal axis suppression [5,6]. Although intralesional tri-
amcinolone injection has some risks, it is a good first-line option for
patients both adults and adolescenst with limited hair loss. It is not
appropriate for those with more severe disease and children younger
than 10 years of age because of potential fear of pain [7].
4 www.avidscience.com
Hair Disorders
Topical Immunotherapy
Topical immunotherapy with contact sensitizers has been used
since 1970’s to treat dermatological conditions in which altered im-
munological state assumed to play role. For alopecia areata, topical
immunotherapy is suitable option for patients with severe or chronic
recurrent disease [8]. Several mechanisms of action have been pro-
posed such as inhibition of the pathologic immune response by an-
tigenic competition, the induction of lymphocyte apoptosis, or the
modulation of cytokine profiles leading to an increase in T-regulatory
lymphocytes in the inflammatory infiltrate [9-13].
Its efficacy has been shown in some uncontrolled studies and
found variable response rates. Some conditions may be associated
with poor response to topical immunotherapy (Table 2). Generally
patients achieving significant hair regrowth range between 40 to 60
percent with 60 percent relapse rates [14-16].
Table 2: Indicators of poor response to topical immunotherapy.
▶▶ Extensive hair loss
▶▶ Alopecia totalis / alopecia universalis
▶▶ History of thyroid disease
▶▶ Younger onset
▶▶ Nail involvement
▶▶ Long-standing disease
Combination with antralin may increase the efficacy of topical
sensitization [17]. It is expected that 1–2 % of patients could not be
sensitized, and for sensitized patients further development of toler-
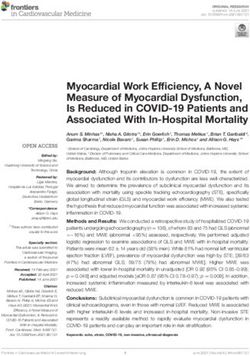
ance is also possible. If sensitization occurs, application should be
performed at least three to six months to obtain acceptable hair re-
growth (Figures 1a and 1b).
www.avidscience.com 5
Hair Disorders
1: A
1: B
Figure 1a and 1b: Improvement of scalp alopecia before and 12 months after treatment
with SADBE.
6 www.avidscience.com
Hair Disorders
Due to mutagenity in Ames test, dinitrochlorobenzene (DNCB)
which is previously used for contact sensitization, is no longer pre-
ferred. Currently diphenylcyclopropenone (DPCP) and squaric acid
dibutyl ester (SADBE), are used for topical immunotherapy. DPCP
is often favored over SADBE because it is less expensive and more
stable in solution. Efficacy investigations have shown similar results
with both contact sensitizer [17]. None of them is recommended as
a first-line treatment for patchy alopecia, and for eyelashes [18,19].
Principals of topical immunotherapy are summarized in Table 3.
Table 3: Principals of topical immunotherapy.
▶▶ Avoid self contact with the solution that results in sensitization
▶▶ Always wear protective gloves and mask
▶▶ Refrigeration and protection from light is necessary for DPCP and SADBE
▶▶ For sensitization begin with the application of a 2% solution to 4x4 cm area, on the
scalp
▶▶ After 1-2 weeks of sensitization, begin treatment with the application of a 0.001%
concentration of the allergen to the affected areas
▶▶ Do not wash for 48 hours
▶▶ Protect treated areas from direct sunlight
▶▶ If severe eczema occurs a week may be passed or concentration may be decreased
▶▶ Repeat treatment weekly with slowly increasing concentrations to a maximum con-
centration of 2%
▶▶ Mild erythema and eczematous reaction is desired
▶▶ Hair regrowth may occur after 3 months
▶▶ Once maximal hair regrowth is achieved decrease treatment frequency
▶▶ Discontinue treatment if there is no response after six months
Eczematous reaction with blistering is a potential side effect of
topical immunotherapy. If reaction is severe, contact allergen should
be washed off, cold compress and corticosteroid creams should be
initiated. Other potential side effects include cervical and occipital
lymphadenopathy, pruritus, urticaria, vitiligo, the development of
multiple lentigines and dyschromia. Use in pregnancy is not recom-
www.avidscience.com 7Hair Disorders
mended because of possible mutagenic properties [18]. Concomitant
use of oral non-sedative antihistamin, fexofenadine, may prevent the
itch induced by DPCP in patients with alopecia areata [20,21]. Patient
compliance, accessibility and the cost are major issues of topical im-
munotherapy.
Anthralin
Although evidence of its effectiveness is limited, topical anthra-
lin is used in the treatment of alopecia areata as short contact therapy
(Table 4) [1]. It is thought to have an immunomodulatory effect re-
sulting in the inhibition of tumor necrosis factor (TNF)-α/β and in-
terferon (IFN)-γ [22,23].
Table 4: Short-contact therapy with anthralin.
▶▶ Apply anthralin 0.5 or 1% cream to the affected areas for 20 to 30 minutes daily
▶▶ Then rinse off with cool to lukewarm water
▶▶ Increase contact time by 10 minutes every two weeks up to one hour or to the time
required to induce mild dermatitis
▶▶ Then continue at that exposure time
In small studies, improvement between 25–75 percent of the pa-
tients has been reported with side effects such as pruritus, local ery-
thema, and scaling [24,25]. Mild irritation with erythema and scaling
is desired but should not be allowed to become severe vesicular reac-
tion. Treatment should be applied for three months before reevaluat-
ing for its effectiveness. Due to low risk potential, it is predominantly
used in children as an alternative to corticosteroids.
Anthralin will stain hair, skin, and clothing, linens, towels, and
showers brown. Patients should wash their hands with lukewarm wa-
ter immediately after application.
8 www.avidscience.comHair Disorders
Minoxidil
Minoxidil is an antihypertensive vasodilator agent and has stim-
ulating effect on hair growth.
Randomized trials of minoxidil have been small, but some [26-
28] of them have found evidence of benefit, at least for patients with
limited alopecia areata. Minoxidil 5% solution is more effective than
the 2% and few patients achieve cosmetically significant regrowth
[29]. In contrast to agents which act on inflammation such as corti-
costeroids and immunomodulatory agents, minoxidil promote hair
growth, and is suitable to use in combination with other modalities
[30]. Use of topical minoxidil is also suggested to reduce hair loss after
tapering corticosteroids [31].
For evaluation of its effectiveness, minoxidil should be tried at
least three to six months and if it works, continued application is re-
quired for maintenance. Minoxidil is not effective in patients with
alopecia totalis and universalis [32]. Topical minoxidil is generally
well tolerated but as an adverse event growth of facial hair in women,
pruritus or dermatitis may occur [33,34].
Topical Prostaglandin Analogs
Bimatoprost is a prostaglandin F2-α (PGF2 α) analog, which in-
duce hypertrichosis, initially used to treat alopecia areata of eyelash-
es[35]. In case reports and some studies, effectiveness has been shown
and patients with 50 % loss get more benefit [36-38]. Mild eye irrita-
tion, hyperemia and conjunctivitis are reported side effects [39,40].
Bimatoprost has been used for the scalp alopecia and showed a
higher efficacy to topical corticosteroid therapy (50 % versus 22 %).
Although side effects were not reported with bimatoprost, relapse and
resistance were observed [39]. Similar results were also obtained in a
pediatric case study [40].
www.avidscience.com 9Hair Disorders
Photochemotherapy
Photochemotherapy is a treatment option for alopecia areata.
Psoralen plus ultraviolet A (PUVA) can be administered with the
topical or oral 8-methoxypsoralen. Several uncontrolled series have
suggested efficacy rates of PUVA of 60 to 65 percent, with a high re-
lapse rate [41-44]. After initial hair regrowth, decreasing in efficacy
may be expected due to regrown hair inhibiting the UVA light to
reach the skin. Photochemotherapy may be suitable in patients with
extensive alopecia areata (more than 75 percent of scalp involved),
alopecia totalis, or alopecia universalis when topical immunotherapy
is contraindicated or unavailable for the patient. Treatment usually
takes four to six months. It should be kept in mind that, long-term
treatment with PUVA has been associated with an increased risk for
cutaneous malignancy.
308 nm Excimer Laser
308 nm excimer laser has been shown to be effective in patchy
alopecia areata. Treatment was performed for 3 months about 24-27
sessions. But it is not suitable for alopecia totalis or universalis. [45-
47].
Systemic Therapies
Systemic therapies are suitable for severe and recalcitrant alope-
cia areata. A high relapse rate, limited efficacy data, and the potential
adverse effects of these drugs limit their use to refractory cases.
Systemic Steroids
Systemic glucocorticoid therapy may induce hair growth in alo-
pecia areata [1]. The efficacy of prednisone (40 mg tapered over six
weeks) was investigated in a prospective study of children and adults
with alopecia areata, in which 13 patients achieved at least 50 percent
hair regrowth, after six weeks of treatment [48].
10 www.avidscience.comHair Disorders
For acute and widespread alopecia areata (more than 30% surface
area) systemic corticosteroid therapy, either orally or intravenously,
is suitable. For the prevention of side effects, pulsed administration
has been proposed as prednisolone 300 mg per oral at 4-week inter-
vals, for a minimum of four doses or until cosmetically acceptable
hair growth is obtained [49]. Clinical response may become evident
approximately 2 to 3 months of therapy. Additionally, short courses
of systemic glucocorticoids (40 to 60 mg per day in adults or 1 mg/
kg per day in children tapered over four to six weeks) may be used
to stop rapid disease progression in patients with widespread active
disease.
Although systemic glucocorticoids stimulate hair growth, the
adverse effects associated with these agents limit the duration of
therapy and recurrence frequently occurs after the discontinuation
of treatment. Minoxidil may be used for preventing recurrences after
prednisone discontinuation [48].
Other Immunsupressive Agents
Sulfasalazine
Sulfasalazine is a drug with immunosuppressive and immu-
nomodulatory properties. In uncontrolled studies, successful therapy
in approximately 25 percent of patients with alopecia areata have been
reported [50-52]. However, relapse rates of up to 45 percent have been
reported [51].
Methotrexate
As in other lymphocyte-mediated autoimmune diseases, the use
of methotrexate (MTX) alone or in combination with low-dose oral
corticosteroids for the treatment of extensive alopecia areata has been
proposed with an overall success rate of 64% [53].
Best results are achieved with 30 mg weekly subcutaneous MTX
in combination with oral prednisone 20 mg daily: re-growth of hair
begins within 2 to 4 months of this regimen [54].
www.avidscience.com 11Hair Disorders
Cyclosporine
Cyclosporine may induce hair regrowth in alopecia areata via
inhibition of helper T cell activation [55]. Although hair growth oc-
curs between the second and the fourth week of therapy with the dose
of 6 mg/kg/d, significant hair loss, occurred in all patients within 3
months of discontinuation of cyclosporine treatment [55].
For treatment of severe alopecia areata, combination regimens
of oral cyclosporine with low-dose corticosteroids have been found to
be effective [56]. Nevertheless, long-term toxicities and risks related
to immunosuppression limit its use.
Azathioprine
Effectiveness of azathioprine has been shown in uncontrolled
studies in which hair regrowth encountered in some patients with
moderate to severe alopecia areata [57,58]. Responses occurred four
to six months after the initiation of treatment, and four of the six re-
sponders had persistent improvement after the discontinuation. Ad-
verse effects (diarrhea, liver enzyme elevation, pancreatitis, or bone
marrow suppression) occurred in 5 of the 14 treated patients, result-
ing in treatment cessation in four patients.
Statins
There is increasing evidence that statins (3-hydroxy-3-methyl-
glutaryl co-enzyme A reductase inhibitors) have immunomodulatory
activities. [59]. After original report of hair regrowth in a patient with
alopecia universalis following initiation of simvastatin and ezetimibe
therapy, effectiveness has been shown in several case reports and case
series but findings could not be reproduced subsequently [60-64].
For that reason, limited data obtained from case series of a condition
where spontaneous remissions may occur, and these results need to
be clarified by large placebo-controlled trials.
12 www.avidscience.comHair Disorders
Targeted Therapies
Biological agents
Neither tumor necrosis factor alpha (TNF alpha) inhibitors such
as etanercept and infliximab, nor LFA-1 inhibitor efalizumab were ef-
fective for the treatment of alopecia areata. [65-67]. TNF-alpha in-
hibitors rather worsen the course of the disease [68].
Janus Kinase Inhibitors
Hair regrowth during tofacitinib treatment (selective Janus ki-
nase 1/3 inhibitor) has been shown in alopecia areata (Figures 2-4)
[69-75]. Effect of tofacitinib may result from inhibition of T lympho-
cyte activation. In a retrospective study with 90 adults with severe
alopecia treatment with tofacitinib (5 to 10 mg twice daily) for at least
four months suggests benefit [69]. In this study, patients with longer
duration of disease (more than 10 years) had lower response rate and
no serious adverse effects noted. Tofacitinib therapy is associated with
increased risk for infection, including serious infections [74]. The de-
velopment of malignancy and laboratory abnormalities has also been
reported in patients receiving tofacitinib therapy for other diseases
[75].
Similar results were also reported for potential role of Janus ki-
nase 1/2 inhibitor ruxolutinib in the treatment of alopecia areata [76].
In a patient with refractory alopecia universalis, treatment with rux-
olitinib 0.6% cream (twice daily for 12 weeks) appeared to stimulate
almost full eyebrow regrowth and approximately 10 percent regrowth
of scalp hair [77]. Further studies are necessary to conclude the ef-
ficacy and safety of topical Janus kinase inhibitors for the treatment
of alopecia areata.
www.avidscience.com 13Hair Disorders
2: A
2: B
Figure 2a and 2b: Succesful treatment of alopecia totalis with tofacitinib, before and
12 months after therapy.
14 www.avidscience.comHair Disorders
3: A
3: B
Figure 3a and 3b: Succesful treatment of alopecia totalis with tofacitinib, before and
12 months after therapy.
www.avidscience.com 15Hair Disorders
Platelet-Rich Plasma (PRP)
PRP has gained popularity in several dermatologic conditions
and includes several growth factors such as platelet derived growth
factor, TGF-beta, fibroblast growth factor, insulin-like growth factors
1 and 2, vascular endothelial growth factor, epidermal growth factor
(EGF), IL-8 and keratinocyte growth factor.
In a double-blind, placebo controlled study with 45 patients in-
tralesional injections of PRP, intralesional triamcinolone or placebo
were applied on one half of the scalp of the patients with randomized
design while other half was not treated. Three treatments were given
for each patient, with monthly intervals. PRP was found to increase
hair regrowth and decrease hair dystrophy, burning or itching sensa-
tion compared to intralesional triamcinolone or placebo [78].
Since detailed immunologic pathogenesis of alopecia areata is
almost explored, and targeted therapies gained more attention; treat-
ment with PRP with unknown mechanism may only be used as an
adjuctive therapy[79].
Special Conditions
Eyebrow Alopecia Areata
Topical steroids or steroid injections are the mainstay of treat-
ment of eyebrow AA. Generally in this area use of lower concentra-
tions (2.5 mg/mL) is suggested in order to limit the chance of tran-
sient atrophy[7]. Eyebrow tattooing is a popular option for those with
treatment-resistant eyebrow AA.
Eyelash Alopecia Areata
There are no established treatments for the local treatment of
eyelash disease. Topical prostaglandin analogues have been studied
for this purpose [35,37]. False eyelashes are a cosmetic option for
these patients.
16 www.avidscience.comHair Disorders
Beard Alopecia Areata
Alopecia areata of the beard is challenging and topical treatment
with steroids can elicit folliculitis. Usually injections of triamcinolone
acetonide (5 mg/mL) is suggested for resistant areas[7]. Atrophy re-
mains a main side effect and must be discussed with all patients.
Scalp Camouflage Options
Individuals with advanced forms of AA may be benefited from
a wig or hairpiece. These products can be worn while using all forms
of treatment. Scalp camouflaging options with coloured sprays and
fibres can be used to camouflage small areas of hair loss. Wigs are gen-
erally less usefull in men where shaving the scalp, are often preferred
approach [80].
Children with Alopecia Areata
Therapeutic options for children are more limited than for adults
due to concerns about tolerability and side-effects [80]. Topical thera-
pies are the primary therapeutic modality in this age group, with po-
tent topical glucocorticoids as the first-line treatment [81,82]. Topical
minoxidil and topical immunotherapy are additional options for the
treatment of children. Anthralin may also be used, but the significant
irritation reaction can limit its use in children.
Use of oral glucocorticoids for extensive and progressive alope-
cia areata may induce hair regrowth, but patients often relapse upon
the cessation of therapy. The use of long-term systemic glucocorti-
coids is generally not recommended due to concern for systemic side
effects [81].
Studies of PUVA therapy in children with alopecia areata have
variable results and is not favored for the use in children due to its
association with cutaneous malignancies [82].
The psychological effects of hair loss are often of concern in chil-
dren, and particularly adolescents, with alopecia areata. Counseling
and support services may be indicated.
www.avidscience.com 17Hair Disorders
Conclusion
Since up to 50 percent of patients with limited alopecia areata
will experience spontaneous regrowth of hair less than one year’s du-
ration, treatment is not necesarry for all patients.
For cosmetic reasons, alopecia areata can cause severe emotional
distress; and counseling in such patients is needed. For patients who
desire treatment, aproach should be tailored according to the age of
the patient, extend of disease, associated conditions and the involve-
ment of life quality (Table 5).
Table 5: Practical points for the treatment of alopecia areata.
• Alopecia areata localized to scalp intralesional injections of corticosteroids is the first
choice of treatment.
• In children or adults with limited disease who cannot tolerate intralesional therapy,
topical corticosteroids are suggested.
• If intradermal or topical corticosteroid therapy is not enough, topical 5% minoxidil eit-
her alone or in combination with continued corticosteroid therapy is suggested.
• Patients with extensive disease, or limited disease who do not respond to topical
agents can be treated with topical immunotherapy.
• If topical immunotherapy does not work or contraindicated, photochemotherapy may
be tried but long-term photochemotherapy should be avoided.
• In patients with widespread active disease systemic short courses of glucocorticoid
therapy may be utilized to stop disease progression. For potential adverse effects they
are not suitable for long-term use.
• For resistant cases other immunsupressives or targeted therapies may be tried.
• Patients who do not desire treatment may benefit from cosmetic interventions such as
wigs for female and shaving the scalp for male patients.
• Eyebrow tattooing or false eyelashes can be helpful.
18 www.avidscience.comHair Disorders
References
1. Messenger AG, McKillop J, Farrant P, McDonagh AJ, Slad-
den M. British Association of Dermatologists’ guidelines for
the management of alopecia areata. Br J Dermatol. 2012;
166: 916-926.
2. Keipert JA, Kelly R. Temporary Cushing’s syndrome from
percutaneous absorption of betamethasone 17-valerate.
Med J Aust. 1971; 1: 542-544.
3. Ro BI. Alopecia areata in Korea (1982-1994). J Dermatol
1995; 22: 858-864.
4. Chang KH, Rojhirunsakool S, Goldberg LJ. Treatment of
severe alopecia areata with intralesional steroid injections.
J Drugs Dermato. 2009; 8: 909-912.
5. Trüeb RM, Dias MFRG. Alopecia Areata: a Comprehensive
Review of Pathogenesis and Management. Clinic Rev Allerg
Immunol. 2018; 54: 68-87.
6. Kuldeep C, Singhal H, Khare AK, Mittal A, Gupta LK, et al.
Randomized comparison of topical betamethasone valerate
foam, intralesional triamcinolone acetonide and tacrolimus
ointment in management of localized alopecia areata. Int J
Trichol. 2011; 3: 20–24.
7. Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J.
Alopecia areata update: part II. Treatment. J Am Acad Der-
matol. 2010; 62: 191-202.
8. Wiseman MC, Shapiro J, MacDonald N, Lui H. Predictive
model for immunotherapy of alopecia areata with diphen-
cyprone. Arch Dermatol. 2001; 137: 1063-1068.
9. Happle R. Antigenic competition as a therapeutic concept
for alopecia areata. Arch Dermatol Res. 1980; 267: 109-114.
www.avidscience.com 19Hair Disorders
10. Herbst V, Zöller M, Kissling S, Wenzel E, Stutz N, et al. Di-
phenylcyclopropenone treatment of alopecia areata induces
apoptosis of perifollicular lymphocytes. Eur J Dermatol.
2006; 16: 537-542.
11. Happle R, Klein HM, Macher E. Topical immunotherapy
changes the composition of the peribulbar infiltrate in alo-
pecia areata. Arch Dermatol Res. 1986; 278: 214-218.
12. Wasyłyszyn T, Kozłowski W, Zabielski SL. Changes in distri-
bution pattern of CD8 lymphocytes in the scalp in alopecia
areata during treatment with diphencyprone. Arch Derma-
tol Res. 2007; 299: 231-237.
13. Hoffmann R, Wenzel E, Huth A, van der Steen P, Schäufele
M, et al. Cytokine mRNA levels in Alopecia areata before
and after treatment with the contact allergen diphenylcyclo-
propenone. J Invest Dermatol 1994; 103: 530-533.
14. Cotellessa C, Peris K, Caracciolo E, Mordenti C, Chimenti
S. The use of topical diphenylcyclopropenone for the treat-
ment of extensive alopecia areata. J Am Acad Dermatol.
2001; 44: 73-76.
15. Aghaei S. Topical immunotherapy of severe alopecia areata
with diphenylcyclopropenone (DPCP): experience in an
Iranian population. BMC Dermatol. 2005; 5: 6.
16. Dall’oglio F, Nasca MR, Musumeci ML, La Torre G, Ricciar-
di G, et al. Topical immunomodulator therapy with squaric
acid dibutylester (SADBE) is effective treatment for severe
alopecia areata (AA): results of an open-label, paired-com-
parison, clinical trial. J Dermatolog Treat. 2005; 16: 10-14.
17. Durdu M, Özcan D, Baba M, Seçkin D. Efficacy and safety of
diphenylcyclopropenone alone or in combination with an-
thralin in the treatment of chronic extensive alopecia areata:
a retrospective case series. J Am Acad Dermatol. 2015; 72:
640-650.
20 www.avidscience.comHair Disorders
18. Ajith C, Gupta S, Kanwar AJ. Efficacy and safety of the topi-
cal sensitizer squaric acid dibutyl ester in Alopecia areata
and factors influencing the outcome. J Drugs Dermatol.
2006; 5: 262-266.
19. Vedak P, Kroshinsky D. Squaric acid sensitization is not re-
quired for response in the treatment of alopecia areata. J Am
Acad Dermatol. 2015; 73: 471-476.
20. Katagiri K, Arakawa S, Hatano Y, Fujiwara S. Fexofenadine,
an H1-receptor antagonist, partially but rapidly inhibits the
itch of contact dermatitis induced by diphenylcyclopro-
penone in patients with alopecia areata. J Dermatol. 2006;
33: 75–79.
21. Inui S, Nakajima T, Toda N, Itami S. Fexofenadine hydro-
chloride enhances the efficacy of contact immunotherapy
for extensive alopecia areata: retrospective analysis of 121
cases. J Dermatol. 2009; 36: 323–327.
22. Tang L, Cao L, Sundberg JP, Lui H, Shapiro J. Restoration of
hair growth in mice with an alopecia areata-like disease us-
ing topical anthralin. Exp Dermatol. 2004; 13: 5–10.
23. Tang L, Cao L, Pelech S, Lui H, Shapiro J. Cytokines and
signal transduction pathways mediated by anthralin in alo-
pecia areataaffected Dundee experimental balding rats. J In-
vestig Dermatol Symp Proc. 2003; 8: 87–90.
24. Schmoeckel C, Weissmann I, Plewig G, Braun-Falco O.
Treatment of alopecia areata by anthralin-induced derma-
titis. Arch Dermatol. 1979; 115: 1254–1255.
25. Fiedler-Weiss VC, Buys CM. Evaluation of anthralin in
the treatment of alopecia areata. Arch Dermatol. 1987; 123:
1491–1493.
26. Price VH. Double-blind, placebo-controlled evaluation of
topical minoxidil in extensive alopecia areata. J Am Acad
Dermatol. 1987; 16: 730-736.
www.avidscience.com 21Hair Disorders
27. Fenton DA, Wilkinson JD. Topical minoxidil in the treat-
ment of alopecia areata. Br Med J (Clin Res Ed). 1983; 287:
1015-1017.
28. Vestey JP, Savin JA. A trial of 1% minoxidil used topically
for severe alopecia areata. Acta Derm Venereol. 1986; 66:
179-180.
29. Fiedler-Weiss VC. Topical minoxidil solution (1% and 5%)
in the treatment of alopecia areata. J Am Acad Dermatol.
1987; 16: 745-748.
30. Fiedler VC, Wendrow A, Szpunar GJ, Metzler C, DeVillez
RL. Treatment-resistant alopecia areata. Response to combi-
nationtherapy with minoxidil plus anthralin. Arch Derma-
tol. 1990; 126: 756–759
31. Olsen EA, Carson SC, Turney EA. Systemic steroids with
or without 2% topical minoxidil in the treatment of alopecia
areata. Arch Dermatol. 1992; 128: 1467–1467.
32. Vestey JP, Savin JA. A trial of 1% minoxidil used topically
for severe alopecia areata. Acta Derm Venereol. 1986; 66:
179-180.
33. Lucky AW, Piacquadio DJ, Ditre CM, Dunlap F, Kantor I,
et al. A randomized, placebo-controlled trial of 5% and 2%
topical minoxidil solutions in the treatment of female pat-
tern hair loss. J Am Acad Dermatol. 2004; 50: 541-553.
34. Olsen EA, Dunlap FE, Funicella T, Koperski JA, Swinehart
JM, et al. A randomized clinical trial of 5% topical minoxidil
versus 2% topical minoxidil and placebo in the treatment of
androgenetic alopecia in men. J Am Acad Dermatol. 2002;
47: 377-385.
35. Zaheri S, Hughes B. Successful use of bimatoprost in the
treatment of alopecia of the eyelashes. Clin Exp Dermatol.
2010; 35: 161–162.
22 www.avidscience.comHair Disorders
36. Roseborough I, Lee H, Chwalek J, Stamper RL, Price VH.
Lack of efficacy of topical latanoprost and bimatoprost oph-
thalmic solutions in promoting eyelash growth in patients
with alopecia areata. J Am Acad Dermatol. 2009; 60: 705–
706.
37. Ochoa BE, Sah D, Wang G, Stamper R, Price VH. Instilled
bimatoprost ophthalmic solution in patients with eyelash
alopecia areata. J Am Acad Dermatol. 2009; 61: 530–532.
38. Vila TO, Camacho Martinez FM. Bimatoprost in the treat-
ment of eyelash universalis alopecia areata. Int J Trichol.
2010; 2: 86–88.
39. Zaher H, Gawdat HI, Hegazy RA, Hassan M. Bimatoprost
versus mometasone furoate in the treatment of scalp alo-
pecia areata: a pilot study. Dermatol Basel Switz. 2015; 230:
308–313.
40. Li AW, Antaya RJ. Successful treatment of pediatric alopecia
areata of the scalp using topical bimatoprost. Pediatr Der-
matol. 2016; 33: 282–283.
41. Claudy AL, Gagnaire D. PUVA treatment of alopecia areata.
Arch Dermatol. 1983; 119: 975-978.
42. Lassus A, Eskelinen A, Johansson E. Treatment of alopecia
areata with three different PUVA modalities. Photoderma-
tol. 1984; 1: 141-145.
43. Mitchell AJ, Douglass MC. Topical photochemotherapy for
alopecia areata. J Am Acad Dermatol. 1985; 12: 644-649.
44. van der Schaar WW, Sillevis Smith JH. An evaluation of PU-
VA-therapy for alopecia areata. Dermatologica. 1984; 168:
250-252.
45. Zakaria W, Passeron T, Ostovari N, Lacour JP, Ortonne JP.
308-nm excimer laser therapy in alopecia areata. J Am Acad
Dermatol. 2004; 51: 837-838.
www.avidscience.com 23Hair Disorders
46. Al-Mutairi N. 308-nm excimer laser for the treatment of
alopecia areata. Dermatol Surg. 2007; 33: 1483.
47. Al-Mutairi N. 308-nm excimer laser for the treatment of
alopecia areata in children. Pediatr Dermatol. 2009; 26: 547-
550.
48. Olsen EA, Carson SC, Turney EA. Systemic steroids with or
without 2% topical minoxidil in the treatment of alopecia
areata. Arch Dermatol. 1992; 128: 1467-1470.
49. Sharma VK. Pulsed administration of corticosteroids in
the treatment of alopecia areata. Int J Dermatol. 1996; 35:
133–136.
50. Ellis CN, Brown MF, Voorhees JJ. Sulfasalazine for alopecia
areata. J Am Acad Dermatol. 2002; 46: 541-544.
51. Aghaei S. An uncontrolled, open label study of sulfasalazine
in severe alopecia areata. Indian J Dermatol Venereol Lep-
rol. 2008; 74: 611-613.
52. Rashidi T, Mahd AA. Treatment of persistent alopecia areata
with sulfasalazine. Int J Dermatol. 2008; 47: 850-852.
53. Joly P The use of methotrexate alone or in combination
with low doses of oral corticosteroids in the treatment of
alopecia totalis or universalis. J Am Acad Dermatol. 2006;
55: 632–636 .
54. Chartaux E, Joly P. Long-term follow-up of the efficacy of
methotrexate alone or in combination with low doses of oral
corticosteroids in the treatment of alopecia areata totalis or
universalis. Ann Dermatol Venereol. 2010; 137: 507–513.
55. Gupta AK, Ellis CN, Cooper KD, Nickoloff BJ, Ho VC, et
al. Oral cyclosporine for the treatment of alopecia areata.
A clinical and immunohistochemical analysis. J Am Acad
Dermatol. 1990; 22: 242-250.
24 www.avidscience.comHair Disorders
56. Lee D, Oh DJ, Kim JW, Park SW, Oh MK, et al. Treatment of
severe alopecia areata: combination therapy using systemic
cyclosporine a with low dose corticosteroids. Ann Derma-
tol. 2008; 20: 172–178
57. Vañó-Galván S, Hermosa-Gelbard Á, Sánchez-Neila N,
Miguel-Gómez L, Saceda-Corralo D, et al. Treatment of re-
calcitrant adult alopecia areata universalis with oral azathio-
prine. J Am Acad Dermatol. 2016; 74: 1007-1008.
58. Farshi S, Mansouri P, Safar F, Khiabanloo SR. Could aza-
thioprine be considered as a therapeutic alternative in the
treatment of alopecia areata? A pilot study. Int J Dermatol.
2010; 49: 1188-1193.
59. Namazi MR Statins: novel additions to the dermatologic ar-
senal? Exp Dermatol. 2004; 13: 337–339.
60. Robins DN. Case reports: alopecia universalis: hair growth
following initiation of simvastatin and ezetimibe therapy. J
Drugs Dermatol. 2007; 6: 946–947.
61. Ali A, Martin JM IV. Hair growth in patients alopecia ar-
eata totalis after treatment with simvastatin and ezetimibe. J
Drugs Dermatol. 2010; 9: 62–64.
62. Lattouf C, Jimenez JJ, Tosti A, Miteva M, Wikramanayake
TC, et al. Treatment of alopecia areata with simvastatin/
ezetimibe. J Am Acad Dermatol. 2015; 2: 359–361.
63. Loi C, Starace M, Piraccini BM. Alopecia areata (AA) and
treatment with simvastatin/ezetimibe: experience of 20 pa-
tients. J Am Acad Dermatol. 2016; 74: 99-100.
64. Freitas-Gouveia M, Trüeb RM. Unsuccessful treatment of
alopecia areata with simvastatin/ezetimibe: experience in 12
patients. Skin Appendage Disord. 2017; 3: 156–160.
www.avidscience.com 25Hair Disorders
65. Strober BE, Siu K, Alexis AF, Kim G, Washenik K, et al.
Etanercept does not effectively treat moderate to severe
alopecia areata: an open-label study. J Am Acad Dermatol.
2005; 52: 1082-1084.
66. Fabre C, Dereure O. Worsening alopecia areata and de novo
occurrence of multiple halo nevi in a patient receiving inf-
liximab. Dermatology. 2008; 216: 185-186.
67. Price VH, Hordinsky MK, Olsen EA, Roberts JL, Siegfried
EC, et al. Subcutaneous efalizumab is not effective in the
treatment of alopecia areata. J Am Acad Dermatol. 2008; 58:
395-402.
68. Tosti A, Pazzaglia M, Starace M, Bellavista S, Vincenzi C, et
al. Alopecia areata during treatment with biologic agents.
Arch Dermatol. 2006; 142: 1653-1654.
69. Liu LY, Craiglow BG, Dai F, King BA. Tofacitinib for the
treatment of severe alopecia areata and variants: A study of
90 patients. J Am Acad Dermatol. 2017; 76: 22-28.
70. Craiglow BG, King BA. Killing two birds with one stone:
oral tofacitinib reverses alopecia universalis in a patient with
plaque psoriasis. J Invest Dermatol. 2014; 134: 2988-2990.
71. Dhayalan A, King BA. Tofacitinib Citrate for the Treatment
of Nail Dystrophy Associated With Alopecia Universalis.
JAMA Dermatol. 2016; 152: 492-493.
72. Craiglow BG, Liu LY, King BA. Tofacitinib for the treatment
of alopecia areata and variants in adolescents. J Am Acad
Dermatol. 2017; 76: 29-32.
73. Ibrahim O, Bayart CB, Hogan S, Piliang M, Bergfeld WF.
Treatment of Alopecia Areata With Tofacitinib. JAMA Der-
matol. 2017; 153: 600-602.
26 www.avidscience.comHair Disorders
74. Papp KA, Menter A, Strober B, Langley RG, Buonanno M, et
al. Efficacy and safety of tofacitinib, an oral Janus kinase in-
hibitor, in the treatment of psoriasis: a Phase 2b randomized
placebo-controlled dose-ranging study. Br J Dermatol. 2012;
167: 668-677.
75. Wollenhaupt J, Silverfield J, Lee EB, Curtis JR, Wood SP, et
al. Safety and efficacy of tofacitinib, an oral janus kinase in-
hibitor, for the treatment of rheumatoid arthritis in open-
label, longterm extension studies. J Rheumatol. 2014; 41:
837-852.
76. Pieri L, Guglielmelli P, Vannucchi AM. Ruxolitinib-induced
reversal of alopecia universalis in a patient with essential
thrombocythemia. Am J Hematol. 2015; 90: 82-83.
77. Craiglow BG, Tavares D, King BA. Topical Ruxolitinib for
the Treatment of Alopecia Universalis. JAMA Dermatol.
2016; 152: 490-491.
78. Trink A, Sorbellini E, Bezzola P, Rodella L, Rezzani R, et al. A
randomized, double-blind, placebo- and active-controlled,
half-head study to evaluate the effects of plateletrich plasma
on alopecia areata. Br J Dermatol. 2013; 169: 690–694.
79. Strazzulla LC, Avila L, Lo Sicco K, Shapiro J. An Overview
of the Biology of Platelet-Rich Plasma and Microneedling as
Potential Treatments for Alopecia Areata. J Investig Derma-
tol Symp Proc. 2018; 19: S21-S24.
80. Draelos ZD. Camouflage technique for alopecia areata:
What is a patient to do? Dermatol Ther. 2011; 24: 305-310.
81. Harrison S, Sinclair R. Optimal management of hair loss (al-
opecia) in children. Am J Clin Dermatol. 2003; 4: 757-570.
82. Hawit F, Silverberg NB. Alopecia areata in children. Cutis.
2008; 82: 104-110.
www.avidscience.com 27You can also read