Endomicroscopic Diagnosis of Atypical Food Allergies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
New Method White Paper
Endomicroscopic Diagnosis of Atypical Food Allergies
Ralf Kiesslich, Head of the Department of Internal Medicine, Helios Dr. Horst Schmidt Kliniken Wiesbaden
Introduction
Approximately 10% to 20% of the world’s population is affected by Irritable Bowel Syndrome
(IBS) with chronic symptoms of abdominal pain, constipation, cramping, bloating, nausea,
and diarrhea. Diagnosis of IBS is based on symptoms and ruling out conditions that mimic the
disorder (e.g., Crohn’s disease). A standard part of the IBS patient’s workup is testing for food
sensitivities, intolerances, and allergies. Although evidence is inconclusive on the relationship
between specific foods and IBS, a recent study using endomicroscopy found that more than
50% of IBS patients could have atypical (i.e., nonImmunoglobin E [IgE] mediated) food allergies. 1, 2
Research suggests that the physiologic immune reaction brought on by food allergies or sensitivities may trigger
the onset and/or increased severity of IBS symptoms.3 Recent literature supports that inflammation and intestinal
permeability are similarly found with food allergies.1, 4 Acting as the controller of nutrient absorption, the intestine
could likely be susceptible to changing its motor and sensory function as a result of low-grade inflammation from
food allergens.5
Challenges
“I was suffering for years from bloating and abdominal discomfort associated with food intake. Nobody could find the
reason. Endomicroscopic testing changed my life. I am now without symptoms by using a wheat free diet.” J.M.
The journey to diagnose IBS-related gastrointestinal symptoms—including any food allergies—is often typified by
frequent outpatient visits, inpatient stays, prescriptions, and hospitalizations. 6 These patients may undergo a
variety of exams, tests, procedures, and diets (e.g., questionnaires, scans, endoscopy). Many different physicians
and specialists, such as nutritionists, allergologists, and gastroenterologists, perform these assessments, resulting
in multiple (often uncoordinated) visits, care delays, insurance burdens, and out-of-pocket costs to the patient.
Furthermore, the patients’ perception of their illness, its chronicity, and diagnosis uncertainty—based on
symptoms alone—often means physicians perform extensive investigations using iterative testing methods.
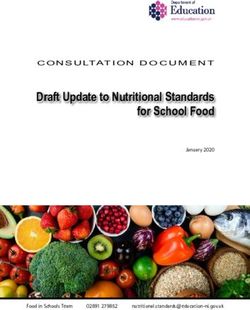
Food allergy-related symptoms can be treated by an exclusion diet, whereas non-food-related ailments of IBS
lead to symptomatic therapy. Thus, the food allergy diagnosis is an important step in managing IBS-related
symptoms. Figure 1 shows the typical algorithm used to diagnose food allergies. Standard diagnostic steps
include skin tests and serological markers (IgE antibodies). Only half of patients with IBS and IgE-related food
allergies receive a definitive diagnosis after standard testing.7
Figure 1: Food Allergy Diagnosis Algorithm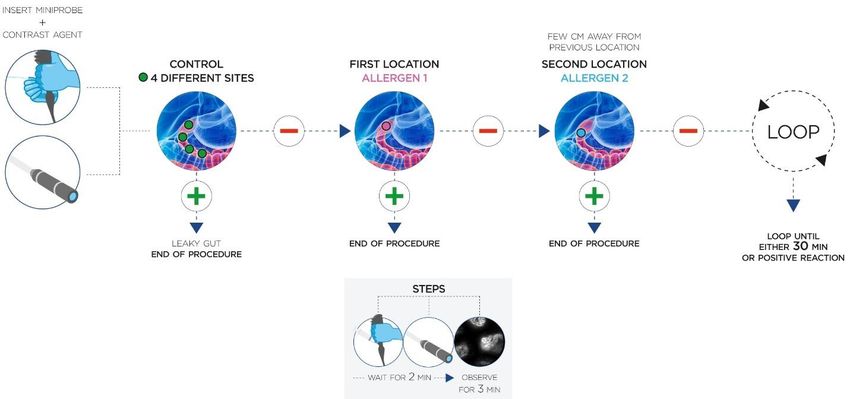
Opportunities Diagnosing Atypical Food Allergies
Current diagnostic methods for typical and atypical food allergies, especially non-IgE mediated ones, are limited
and highly variable (Table 1). Food challenges or exclusion diets are time-consuming—the clinical reaction to the
ingested food occurs several hours after ingestion, and a negative response is unknown for days.
The need exists for primary care physicians, gastroenterologists, nutritionists, and allergologists to have a diagnostic
method for differentiating and identifying food allergens in patients that have tested positive or negative with
current food allergies tests, especially those with negative IgE findings. An emerging new diagnostic tool is confocal
laser endomicroscopy with functional imaging.
Table 1. Common Diagnostic Methods for Typical and Atypical Food Allergies
Test Condition Population Duration Accuracy Results
Skin Prick Test IgE-related 1-4% Adults 2 Weeks 50-60% false Predictive for sensitivity but limited in
(SPT) Food 6 % of Children 2 positives 8 predicting allergy.9
Atopy Patch Allergy
Tests (APTs)
Blood Test IgE-related 1-4% Adults 2 Minutes 50-60% false Predictive for sensitivity but limited in
(measuring IgE) Food 6 % of Children 2 positives 8 predicting allergy.9 Not recommended
Allergy by the National Institutes of Health,
due to lack of scientific evidence and
standardization.2
Oral Food Food 3% to 28% Months to Self-Reported Not definitive. Clinical reaction several
Challenges Intolerance (depending on the Years hours after ingestion, negative
Elimination country studied) 10%- response unknown for days. Hard to
Diets (FODMAP, 15% in Western follow. Risks of nutritional deficiencies.
Paleolithic, countries 6 Intended for short-term management
gluten-free) only. Lasting effects (diets) to gut
microbiota are unknown. 2
Hydrogen Food European descent Minutes Unclear for Definitive for lactose or sucrose
Breath Test Intolerance 0.05% to 0.2%. With individuals with intolerance.
3-10% in circumpolar suspected IBS 11, 12 NOTE: Accuracy based on use of
populations 10 evidence-based protocol.13
Confocal Laser Atypical 3% to 28% depending 2-5 Over 84% effective Definitive, visualized changes in
Endomicroscopy and Typical on the country studied minutes in improving intestinal permeability to agent on
(CLE) Food and 10%-15% in of symptoms with diet contact. Current testing includes wheat,
Allergy Western countries 6 exposure intervention 13 yeast, milk, soy, and egg white.14
Confocal Laser Endomicroscopy (CLE)
Confocal Laser Endomicroscopy (CLE) is an
established diagnostic fiber optic system. Used
during endoscopic procedures, CLE’s advanced
imaging technology places the power of a
confocal microscope at the head of a sub-3mm
catheter probe. With a contrasting agent, the
endomicroscopy’s flexible microscope
magnifies—in real time—the patient’s internal
cellular architecture. This magnification enables
the identification of cells and vessels of the
mucous membrane lining in the gastrointestinal
tract (Figure 2). Figure 2: CLE Probe in Contact with Tissue
Additionally, CLE enables the imaging of dynamic processes, such as intestinal barrier dysfunction and intestinal
barrier cell shedding, which constitute positive markers for food allergies.15
Visualizing the Intestinal Response to Food
CLE’s examination capability is clinically valuable for better understanding of the intestinal immune
pathophysiology. In 2014, Fritscher-Ravens et al. first described the value of endomicroscopy for diagnosing food
allergies when the duodenal reaction to food allergens in IBS patients was observed and quantified. They
evaluated the structural/functional changes that occurred in the intestinal mucosa in vivo and noted the response
followed a defined sequence indicative of an atypical food allergy. 4
In a subsequent study using CLE on IBS
patients with non-IgE-mediated atypical
food allergies, Fristcher-Ravens et al.
found wheat was the predominant
allergen.1 These findings supported what
has been commonly accepted—food
allergens trigger an immune system
response in the gut resulting in intestinal
low-grade inflammation.4 Furthermore,
IBS patients exposed to specific foods
showed changes in intestinal
permeability. A change in cellular
structure can be seen as layer(s) of Figure 3: Cell Structural Changes with Food Challenge
epithelial cells break up and are shed,
forming gaps and inducing an immediate increase in duodenal mucosal fluid permeability. As a result, the
contrasting agent floods into the lumen, widening the space between the villi, and changing the appearance from
black to white.1 This response to food antigens is clearly visible with CLE and follows a defined pathophysiology
sequence within 2-5 minutes of exposure to the food allergen (Figure 3).14
CLE Criteria for Positive Food Reaction
The high-resolution visualization of the reaction to applied food on the mucosa is characterized and interpreted
using the CLE Criteria for Positive Food Reaction (Table 2). Any observed positive reaction (CLE+) indicates an
immune reaction to the applied food nutrient. Note that both criteria for contrasting agent leak and cell shedding
must be visible to validate a CLE positive reaction.
Table 2: CLE Criteria for Positive Food Reaction
Criteria Positive Reaction (CLE+)
Control Image Contrasting Agent Leak Cell Shedding
Before food exposure, the physician records a Gaps formed from exposure to food The intestinal epithelial, representing
baseline endomicroscopy video for post-food allergens let the contrasting agent a thin layer of the villi, breaks up
challenge comparison and checks for barrier leak into the lumen, changing from with pronounced and continued
dysfunction without exposure. This image bright/white lumen in contrast to shedding of cells.
shows an absence of any leak, cell shedding, dark villus.
breaks, or gaps with a mostly dark lumen
compared to bright villi. Both criteria must be met for CLE+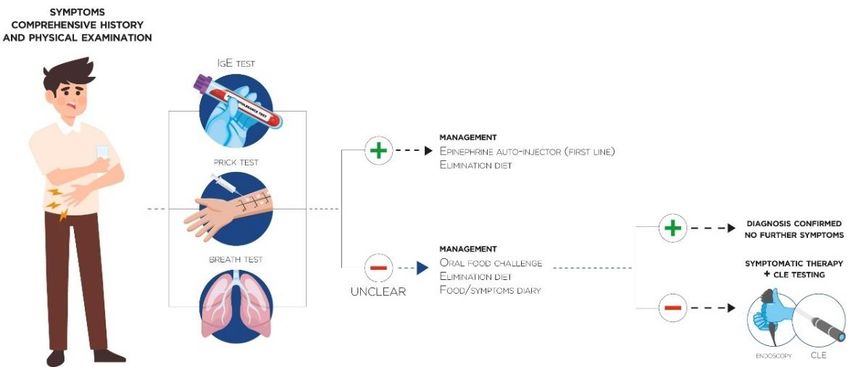
Solution
CLE Food Allergy Sensitivities Test (FAST)
Using the high-resolution, real-time imaging capabilities of CLE, physicians can perform a new endomicroscopic
diagnostic method to detect—and definitively differentiate—food allergens, including safe nutrients, in patients
experiencing symptoms of IBS. This standardized procedure, CLE Food Allergy Sensitivities Test (FAST), consists
of observing microscopic immune reactions in the duodenal mucosa after the application of food allergens known
to be contributors of IBS symptoms (Figure 4).
Figure 4: CLE FAST Procedure
Standardized List of the Most Common Food Allergens
The CLE FAST includes a standardized list of the most common Table 3: Suggested Food
allergens (Table 3). Other foods such as walnut, sesame, crustacean Concentrations for CLE FAST of the
shellfish, fish, and celery are added when indicated by the patient as a Most Common Food Allergens
possible allergen. In the United States, serious food allergy reactions Nutrient Amount Saline
are attributed to eight foods: eggs, milk, peanut, tree nuts, soy, wheat, Wheat Flour 3g 30 ml
fish, and crustacean shellfish. (foodallergy.org) Dry Yeast 1.5 g 30 ml
The food concentration amount for the CLE FAST imitates the natural Soy Flour 3g 30 ml
amount a healthy person can consume without showing negative Milk Powder 1.5 g 30 ml
effects/symptoms. Using CLE, the defined amount of allergen is Dry Egg White 1.5 g 30 ml
applied directly on the duodenum using the working channel of the Peanut Flour 3g 30 ml
endoscope to achieve uniform application compared to swallowing.
Screening for CLE Eligibility
The following screening tests are recommended for candidates of the atypical food allergy CLE procedure:
• IBS identified using Rome III Criteria
• Moderate/severe refractory daily symptoms >1 year4
• IgE serological testing, celiac serology, and skin tests for food allergies as well as breath tests for lactose and
fructose intolerance
• No structural cause of symptoms identified with gastroscopy or colonoscopy
• Symptoms potentially related to food allergy.
To further test the patient's eligibility for the CLE FAST, patients are asked to eat a hypoallergenic diet for 3 days
to exclude any accidental ingestion of potential food allergies prior to the examination.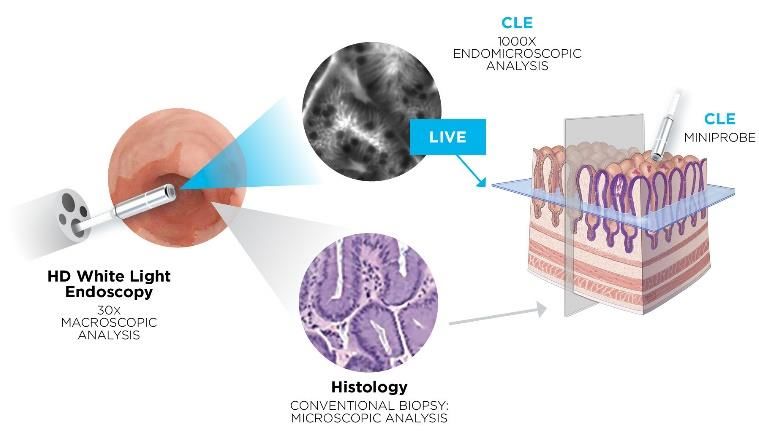
Standardized Procedure
Preparation
Supplies: The following items are necessary to perform the CLE FAST procedure:
1 Regular gastroscope or double lumen gastroscope with working channel of an inner diameter of
2.8 mm or larger
1 Cellvizio probe - GastroFlex or ColoFlex
2.5 mL contrasting agent (Fluorescein concentration 10%)
5 Food samples prepared for application (Table 3)
1 Transparent suction cap (optional)
20 mg Butylscopolamin infusion (optional)
Pre-Test Consultation:
• Up to 7 days before the procedure, provide the patient with the Irritable Bowel Syndrome Severity Scoring
System (IBS-SSS) (Appendix A). The pre-test responses will be evaluated after the procedure.
• Two to three days before the CLE FAST, have the patient follow an exclusion diet and eat only
hypoallergenic nutritional foods (exclusively rice, potatoes, olive oil, salt).
• Approximately 24 hours before the procedure (or as appropriate with current practice), provide the
patient information and preparation instructions for standard gastroscopy of the duodenum.
Test Instructions (Day of Procedure)
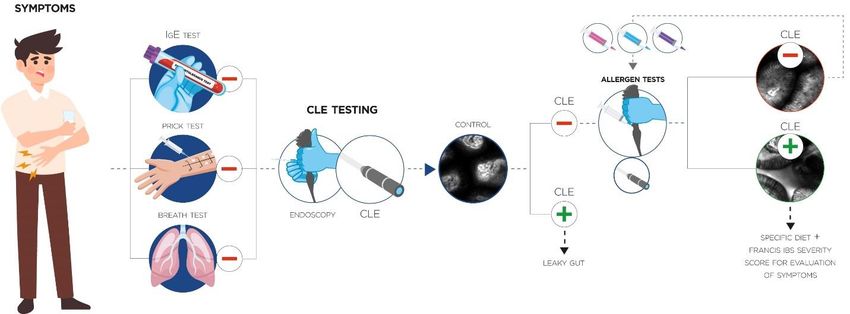
The steps to conduct the CLE FAST are described below and shown in Figure 5.
Figure 5: Atypical Food Allergy CLE FAST Procedure
1. Perform a standard gastroscopy to observe any sign(s) of abnormal mucosal structural defect that would
suggest a known gastrointestinal disease. In the case of any mucosal abnormality observed on endoscopy,
the CLE FAST procedure may not be applicable. In the case of mild reflux disease, the test can proceed.
2. Inject 2.5 ml fluorescein 10% contrasting agent intravenously.
3. To establish a baseline, perform endomicroscopy of the duodenum at a minimum of 4 sites (about 20 seconds
each) to verify mucosal integrity (i.e., no contrasting agent leakage into the lumen) prior to any provocation.
Some contrast agent in the lumen at one of the 4 sites may be normal; however, the test can proceed. For
patients showing excessive leaks, testing should be suspended; the barrier dysfunction test would be
considered already positive and no further allergen testing should be added.
During the baseline and all following CLE measurements, mucosal areas that exhibit bleeding and other
visible indications of inflammation should be avoided to get a true baseline and no false positives.
4. Through the working channel of the endoscope, apply one food allergen onto the duodenal mucosa starting
from the most distal part.
• Leave space between each provocation site.
• Start with the food allergen that will less likely trigger a reaction.
5. Wait for 2 minutes after application of food before starting imaging and observation.
Caution:
During these 2 minutes, avoid touching the probe tip on the mucosa to prevent injuries and fluorescent
leakage.
Switch off the laser during the 2 minutes of waiting to avoid bleaching artifacts; afterwards switch the
laser on again.
Limit exploration to a few locations (pinpoint and move to next site).
Avoid imaging at “6 o’clock position” as fluid with contrast agent may impair the reading.
Observe endomicroscopically the mucosal reaction to the food application (up to 3 minutes per site should be
sufficient).
• If the observed reaction is positive (CLE+), conclude the test.
• If the observed reaction is negative (CLE-), extract the probe, flush with saline in the channel, and move
to the next site with the next allergen.
6. Repeat steps 4 and 5. Before applying a new allergen, move the endoscope to the new site towards the
proximal end of the duodenum.
7. The test should be concluded within 30 minutes after injection of the contrast agent due to the increasing risk
of false positives. Eventually, the contrast agent will be visible in the lumen (but with no cell shedding).
Post-Test Observation
• Within 24 hours of the test, evaluate the general health condition of the patient and rule out any late allergic
reaction resulting from the test. Added medical exams could be necessary (e.g., gastroscopy, colonoscopy,
abdominal ultrasound).
• Provide the patient with the IBS-SSS questionnaire to be evaluated at the follow-up visit.
Patient’s Follow-up Visits
For patients with a positive reaction (CLE+) after provocation:
• Prescribe an elimination diet of the reacted food allergen for 6 months.
• Assess symptoms documented by the patient in the IBS-SSS at baseline and after the exclusion diet.
For patients without any reaction (CLE-), repeat test with a new set of 5 different foods.
For patients with fluorescence leakage before provocation, suggest the patient undergo a wheat-free diet.
Physicians might also provide symptomatic therapy while discussing further procedures to get final diagnosis.
For continued patient management, follow current guidelines.Discussion It is generally recognized that IBS symptoms are an immune system response. Now, with CLE, physicians can clinically observe this response after the sequential application of food as part of a standardized diagnostic procedure, CLE FAST. This visualization allows physicians to identify atypical food allergens and prescribe an endomicroscopically tailored exclusion diet. Results Recent studies using this standardized CLE food testing procedure found IBS patients report improved symptoms—and in some cases cessation—after their personalized exclusion diet. Of all CLE+ patients tested, 68.4% had symptom scores improved by 80% or more.1 The average improvement of symptom scores for all CLE+ patients was 70% after 3 months and 73% after 6 months. A recent abstract suggests the response could go as high as >80% following the diet based on IBS-SSS scores.14 One of the most constant and prominent findings of another recent food challenge using CLE was the immediate and positive reaction showing disruption of the small intestinal barrier and epithelial leaks after a food challenge. 1 A current study of 56 patients using endomicroscopic observation identified improvements in food-associated functional changes of the enteric mucosa that followed an exclusion diet tailored to the study findings.14 Easy, Painless, and Immediate For patients, the CLE FAST is painless, requires no added preparation for a general endoscopy, and delivers a conclusive diagnosis on specific food allergens in less than 30 minutes. For physicians, testing can be done with minimal training on CLE image interpretation and during standard endoscopy. When integrated as a standard diagnostic tool into the food allergy workup/workflow and Rome III Criteria, physicians can optically diagnose diseased tissue and make treatment decisions instantaneously in a minimally invasive manner. Conclusive Diagnosis and Treatment CLE FAST gives general care providers, gastroenterologists, nutritionists, and allergologists the opportunity to improve the lives of IBS patients with a conclusive diagnosis to identify foods that sicken them. The increased level of confidence in treating atypical food allergies changes the IBS patient-physician dynamics to one that creates a healthy and positive partnership.
Appendix A: Irritable Bowel Syndrome Severity Scoring System (IBS-SSS) To obtain approval for use of the C.Y. Francis, J. Morris, and P.J. Whorwel Irritable Bowel Syndrome Severity Scoring System (IBS-SSS), go to: https://eprovide.mapi-trust.org/instruments/irritable-bowel-syndrome-severity-scoring-system.
References 1 Fritscher-Ravens A, Pflaum T, Mösinger M, Ruchay Z, Röcken C, Milla PJ, Das M, Böttner M, Wedel T, Schuppan D. Many Patients With Irritable Bowel Syndrome Have Atypical Food Allergies Not Associated With Immunoglobulin E. Gastroenterology. 2019 Jul;157(1):109-118.e5. doi: 10.1053/j.gastro.2019.03.046. Epub 2019 May 15. 2 Crowe SE. Food Allergy Vs Food Intolerance in Patients With Irritable Bowel Syndrome. Gastroenterol Hepatol (N Y). 2019;15(1):38–40. PMID: 30899207; PMCID: PMC6423694. 3 Hayes PA, Fraher MH, Quigley EM. Irritable bowel syndrome: the role of food in pathogenesis and management. Gastroenterol Hepatol (N Y). 2014;10(3):164–174. PMID: 24829543; PMCID: PMC4014048. 4 Fritscher-Ravens A, Schuppan D, Ellrichmann M, Schoch S, Röcken C, Brasch J, Bethge J, Böttner M, Klose J, Milla PJ. Confocal endomicroscopy shows food-associated changes in the intestinal mucosa of patients with irritable bowel syndrome. Gastroenterology. 2014 Nov;147(5):1012-20.e4. doi: 10.1053/j.gastro.2014.07.046. Epub 2014 Jul 30. 5 Ohman L, Simrén M. Pathogenesis of IBS: role of inflammation, immunity and neuroimmune interactions. Nat Rev Gastroenterol Hepatol. 2010;7:163–173. doi: 10.1038/nrgastro.2010.4 6 Olafsdottir LB, Gudjonsson H, Jonsdottir HH, Jonsson JS, Bjornsson E, Thjodleifsson B. Irritable bowel syndrome: physicians' awareness and patients' experience. World journal of gastroenterology. 2012; 18(28), 3715–3720. doi:10.3748/wjg.v18.i28.3715 7 Halpert A. Review Irritable Bowel Syndrome: Patient-Provider Interaction and Patient Education. J. Clin. Med. 2018, 7(1), 3. doi: 10.3390/jcm7010003 8 Food Allergy Research & Education (FARE). foodallergy.org. Accessed March 2, 2020. https://www.foodallergy.org/sites/default/files/migrated-files/file/Final-FARE-Food-Allergy-Facts-Statistics.pdf 9 Čelakovská J, Krcmova l, Bukac J, Vaneckova J. (2017) Sensitivity and specificity of specific IgE, skin prick test and atopy patch test in examination of food allergy. Food and Agricultural Immunology. 2017;28:2, 238-247. doi: 10.1080/09540105.2016.1258548 10 Food Intolerance Network. Sucrose Intolerance. 13 June 2014. Accessed 2 July 2020. www.food-intolerance-network.com 11 Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am J Gastroenterol. 2017;112(5):775-784. doi:10.1038/ajg.2017.46 12 Ford AC, Spiegel BM, Talley NJ, Moayyedi P. Small intestinal bacterial overgrowth in irritable bowel syndrome: systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2009;7 (12): 1279–86. doi:10.1016/j.cgh.2009.06.031. PMID 19602448. 13 Paterson W, Camilleri M, Simren M, Boeckxstaens G, Vanner SJ. Breath Testing Consensus Guidelines for SIBO: RES IPSA LOCQUITOR. Am J Gastroenterol. 2017;112(12):1888-1889. doi:10.1038/ajg 14 Kiesslich R, Adib-Tezer H, Teubner D, Frieling T, Mudter J, Bayerl C, Wenda NK, Gosepath J. Endomicroscopic detection of atypical food allergy in patients with irritable bowel syndrome – a new diagnostic era? Abstract presented at: Digestive Disease Week; May 3, 2020. 15 Goetz M, Malek N, Kiesslich R. Microscopic imaging in endoscopy: endomicroscopy and endocytoscopy. Nat Rev Gastroenterol Hepatol. 2014;11, 11–18. doi.org/10.1038/nrgastro.2013.134
You can also read