Eisenmetabolismus in der klinischen Praxis - Günter Weiss c G. Weiss - Innere Medizin Online
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Eisenmetabolismus in der klinischen Praxis
Günter Weiss
Universitätsklinik für Innere Medizin II
Infektiologie, Immunologie, Rheumatologie, Pneumologie
Medizinische Universität Innsbruck
guenter.weiss@i-med.ac.at
c G. Weiss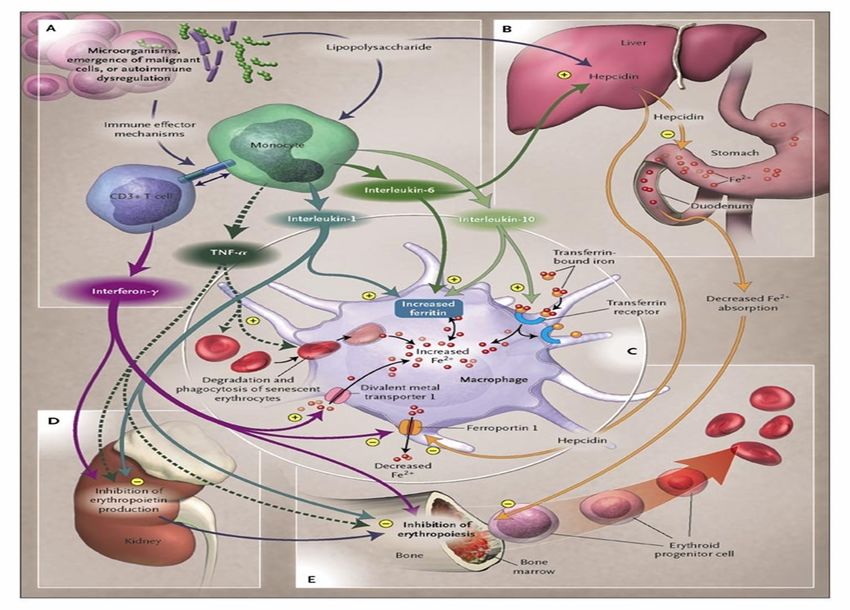
Eisen-Steckbrief
vierthäufigstes Element
meist oxidiert (Hematit, Magnetit, Limonit)
MG 55.847 ; Oxidationsstufen -2 bis +6
EISEN essentiell für Stoffwechsel und Wachstum aller eukaryoten Lebewesen
Zentraler Bestandteil von Enzymen der Atmungskette, im Zitratzyklus, der
DNA-Synthese
essentiell für Sauerstofftransport: Hämoglobin/Myoglobin
aber: katalysiert toxische Radikalbildung-Fenton (OH-)
Stringente Koordination des Fe- Metabolismus notwendig!
c G. Weiss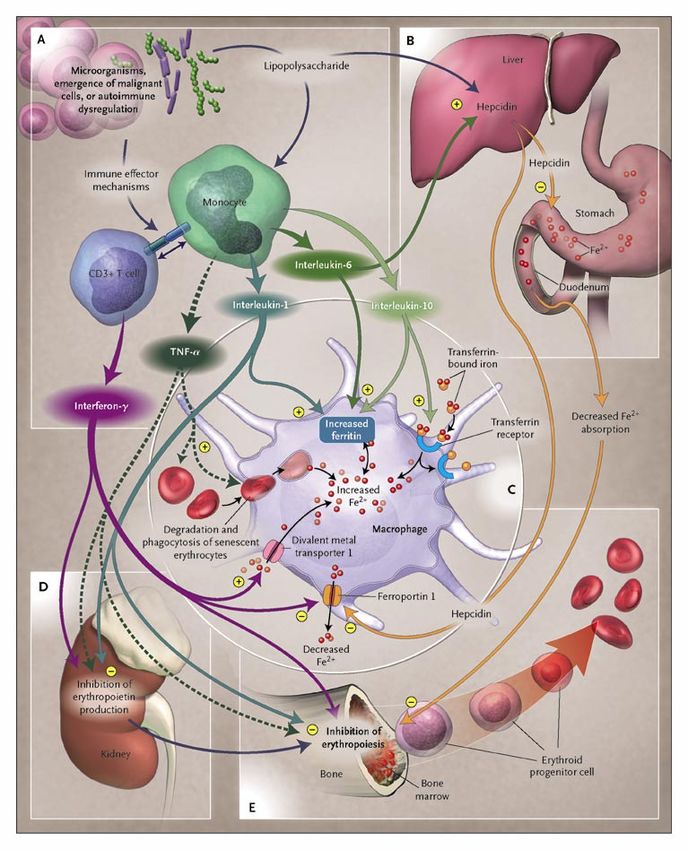
Stringent control of iron homeostasis is
essential for life!
90–95% of daily
iron needed for
erythropoiesis
(ca 25–30 mg/day)
c G. Weiss Anderson GJ, Powell LW. J Clin Invest 2000;105:1185–6.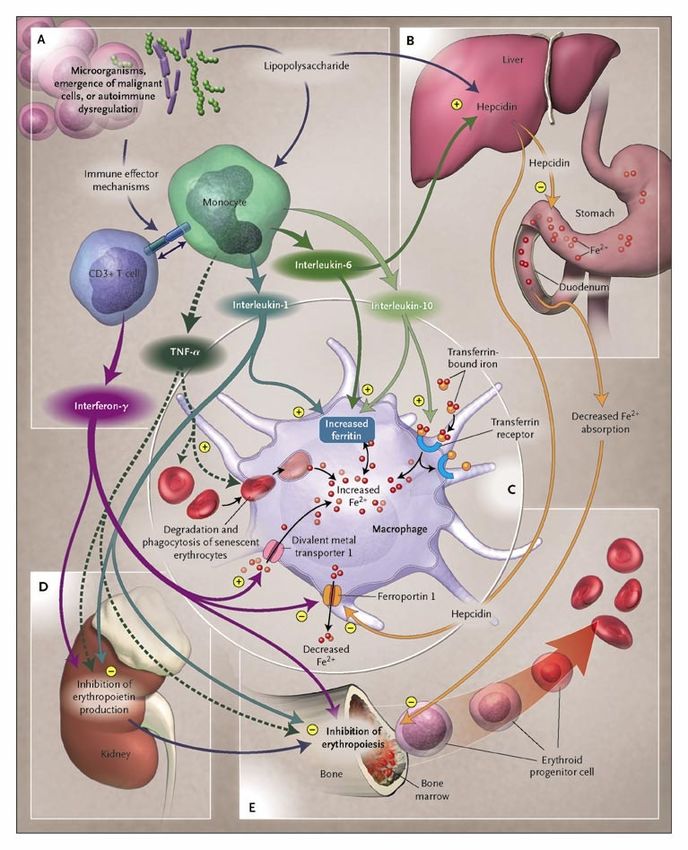
Hepcidin the master regulator of iron homeostasis
c G.Weiss Poli et al. Front Pharmacol 2014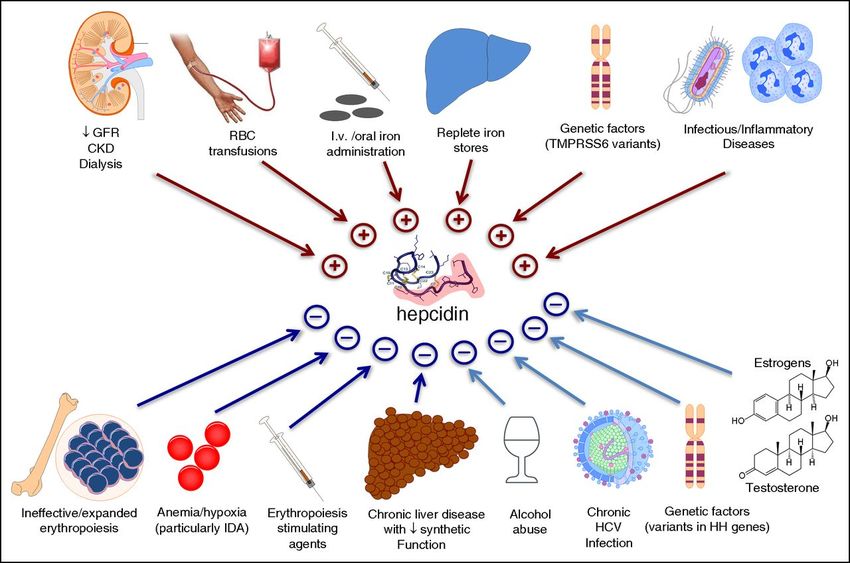
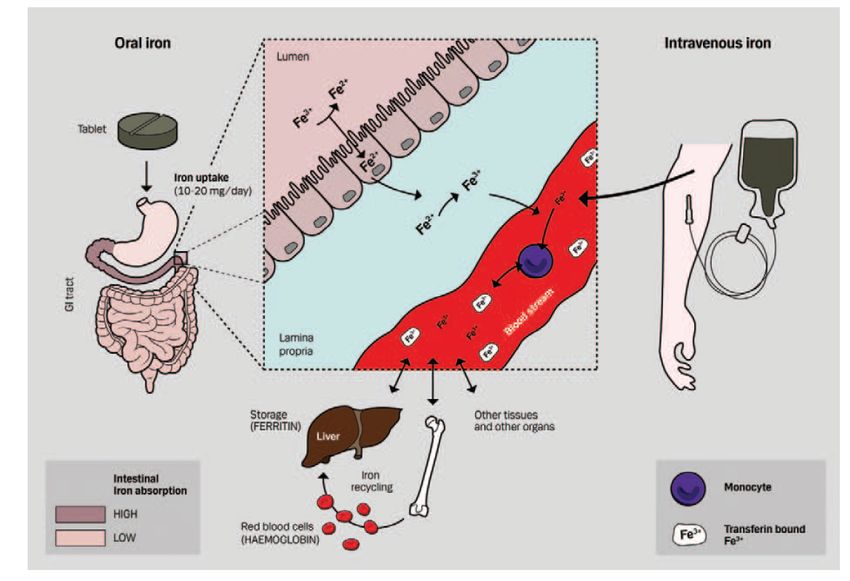
Regulation of systemic iron homeostasis
c G. Weiss Vaulont S, et al. J Clin Invest 2005;115:2079–82.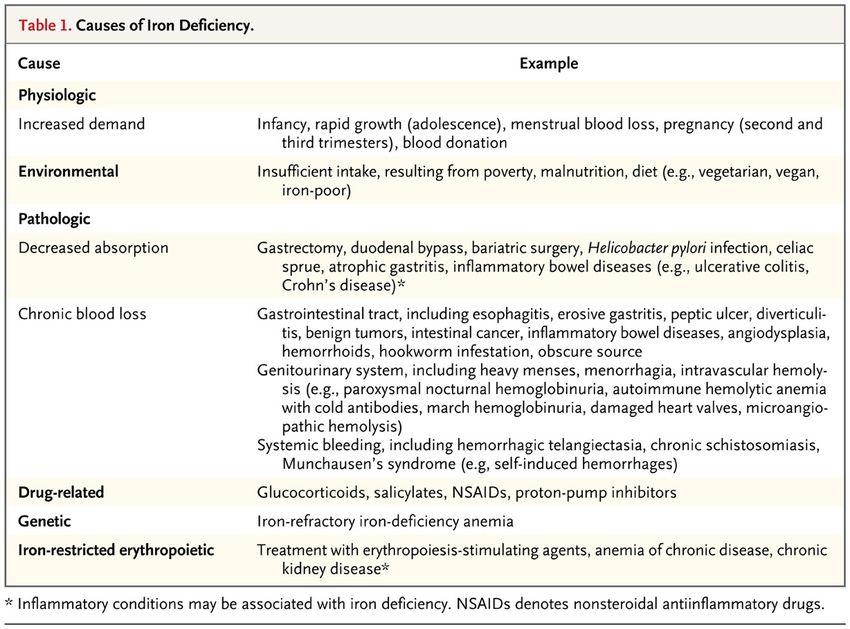
c G.Weiss Girelli et al. Blood 2016
Pathophysiologie des Eisenstoffwechsels
* „wahrer“Eisenmangel: verminderte Resorption, erhöhter Verlust (Blutung)
Folge: Eisenmangelanämie-IDA
*funktioneller Eisenmangel: bei Erkrankungen mit zellulärer Immunaktivierung Eisen im RES
gebunden; nicht ausreichend für Hämatopoese zur Verfügung;
Folge: Anämie chronischer Erkrankungen
* Eisenüberladung: primär: hereditäre Hämochromatose (5 Subtypen)
sekundär: transfusionsbedingt, Bantu-Siderose
Folge: toxische Gewebeschädigung über eisenvermittelte Radikalbildung
c G. Weiss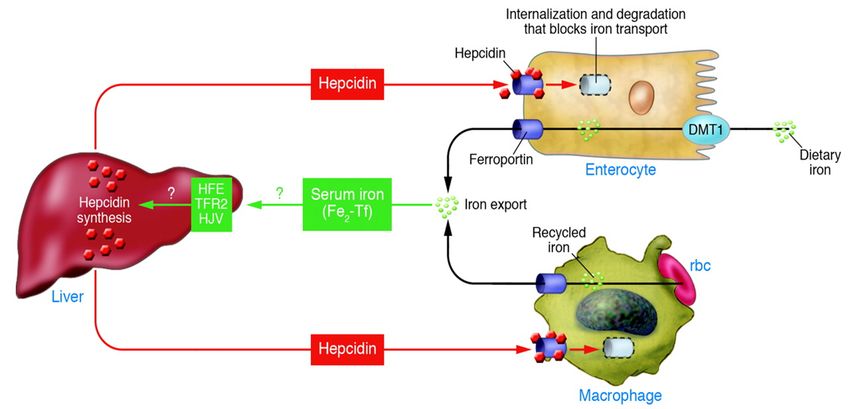
Genetische Hämochromatose
Brissot et al. Nat Rev Dis Prim 2018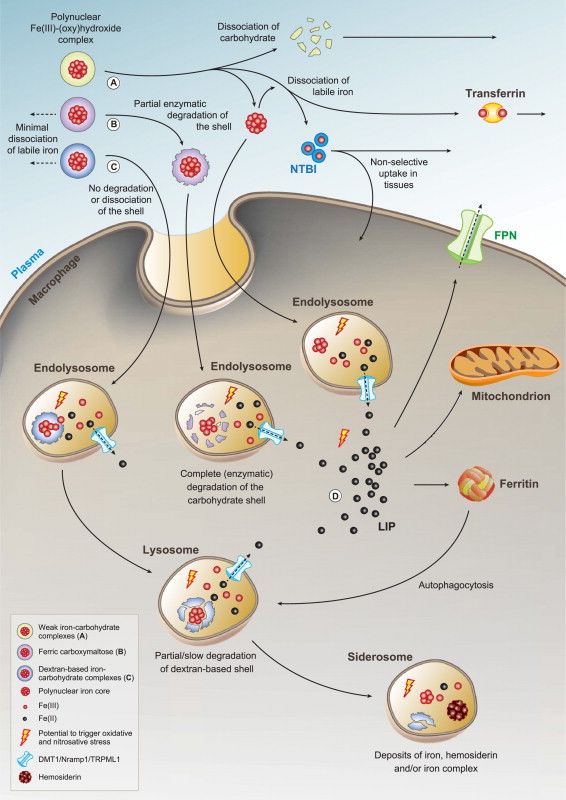
Pathophysiologie: Mangel an Hepcidin, dadurch vermehrte Eisenaufnahme im
Darm und Ablagerung in parenchymatösen Organen
c G.Weiss
de Domenico et al Clin Invest 2007
Hereditary Hemochromatosis (HH)-type1 (HFE)
*Most frequent inherited autosomal-recessive disorder in people of
Western/ Northern-European origin
•Allele frequency of C282Y is 9-12%,
• between 1:250 to 1:400 homozygous for the C282Y mutation
•Phenotypic expression of iron overload is highly variable (64-86%
develop increased ferritin levels during life)
• Genetic and environmental modifiers!
c G.WeissAbklärung eines V.a. Hämochromatose
Transferrin-Sättigung> 45% (häufig 60-100%)
Erhöhtes Ferritin > 300µg/l (Frauen > 200 µg/l)
Fehlende Evidenz für chron. hepatolog.-
oder hämatolog. EK
HFE-Mutation? (C282Y)
ja nein
Genetische Testung für seltene Mutationen
HFE-1 Hämochromatose positiv negativ
Therapie und nonHFE1-Hämochromatose Bei massiver Eisenüberladung
ggf. Leberbiopsie
Familienscreening c G.WeissTherapy of hemochromatosis
• phlebotomy—until patients are anemic!
• Symptomatic therapy of organ insufficiencies (heart, liver,
arthralgias)
• Iron chelation therapy not efficient
c G.WeissSecondary iron overload
Iron overload due to multiple blood transfusion for correction of anemia in patients
•with hemoglobinopathias (e.g. thalassemia,, sickle cell disease)
•malignancies (e.g. myelodysplastic syndromes)
•Cancer chemotherapy, bone marrow transplantation
Consequences: as with primary iron overload
— progressive organ failure due to iron deposition;
cardio-vascular disease (oxidative stress);
In addition: immune–dysfunction (iron mediated effects on cellular immunity)
c G.WeissNon-relapse mortality (incl. infections) increases with pre-
transplant serum ferritin level
Survival and non-relapse mortality in MDS patients undergoing
allogeneic stem cell transplantation
Non-relapse mortality, probability
Cumulative proportion surviving
1.0 HR = 1.40 1.0 HR = 1.42
p = 0.01 p = 0.03
0.8 Serum ferritin < 1,000 µg/L 0.8
Serum ferritin 1,000–1,999 µg/L
0.6 Serum ferritin 2,000–3,000 µg/L 0.6
Serum ferritin > 3,000 µg/L
0.4 0.4 Serum ferritin < 1,000 µg/L
Serum ferritin 1,000–1,999 µg/L
0.2 0.2 Serum ferritin 2,000–3,000 µg/L
Serum ferritin > 3,000 µg/L
0 0
0 20 40 60 80 100 120 140 160 0 20 40 60 80 100 120 140 160
Duration, months Duration, months
Overall survival by Non-relapse mortality by
serum ferritin level before SCT serum ferritin level before SCT
SCT, stem cell transplantation. Alessandrino EP, et al. Haematologica. 2010;95:476-84.Iron at the host–pathogen interface
• Essential for growth and proliferation of Exerts subtle effects on cell-mediated
several microbes immunity in vitro (macrophage effector
• Expression of iron acquisition and pathways, IFN-γ activity, iNOS expression)
siderophore systems is linked to
microbial pathogenicity
Control of iron homeostasis is important in the course of an infection
IFN-γ, interferon-gamma; iNOS, inducible nitric oxide synthase. c G.WeissSecondary iron overload
Iron overload due to multiple blood transfusion for correction of anemia in patients
•with hemoglobinopathias (e.g. thalassemia,, sickle cell disease)
•malignancies (e.g. myelodysplastic syndromes)
•Cancer chemotherapy, bone marrow transplantation
Consequences: as with primary iron overload
— progressive organ failure due to iron deposition;
cardio-vascular disease (oxidative stress);
In addition: immune–dysfunction (iron mediated effects on cellular immunity)
Therapy: iron chelators (daily application)
phlebotomy not applicable (anemic patients!)
c G.WeissNeurologische Erkrankungen und
Eisenhomöestase
Weitere Erkrankungen: Restless legs Syndrom
Multisystematrophie ?
Alzheimer Demenz
c G.WeissEisenmangelanämie
Häufigste Anämieform weltweit
ca. 2 Mrd. Menschen von Eisenmangel betroffen
Ursachen:
akute und chronische Blutungen (v.a. Menses und gastrointestinal)
Resorptionsstörungen (Coeliakie, spez. Fe- Resorptionsdefekte, Fe-Mangelernährung,
Achlorhydrie?, ...)
chron. Infekte im Darm (Hackenwürmer, Lamblien etc.)
c G. WeissCauses of Iron Deficiency.
Camaschella C. N Engl J Med 2015;372:1832-1843Prevalence of (IDA) in children and pregnant women The global prevalence of anaemia for the general population is 24.8% and it is estimated that 1,6 billion people are affected by anaemia (WHO;1993-2005).
Clinical signs of iron deficiency
c G. Weiss
c G.WeissIron deficiency is associated with reduced exercise
capacity in HF patients (1)
Peak oxygen consumption 58
Ventilatory response to exercise
17
Iron deficiency pIron deficiency negatively affects the activity of citric acid cycle
and mitochondrial respiration
+
IRON
+
c G. Weiss
Oexle & Weiss. BBA 1999Abschätzung der Eisenverfügbarkeit durch Ferritin im Serum
• Ferritin ist ein Parameter für das im Körper gespeicherte Eisen
• Ferritin i.S. normal: 15-400 µg/l (erw. Mann)
10-300 µg/l (erw. Frau)
• ein erniedrigtes Ferritin i.S. < 15 µg/l beweist einen absoluten Fe-Mangel !
allerdings weisen schon Pat. mit Ferritin unter 30 µg/l Zeichen des Eisenmangels auf
deshalb muß man bei FerritinEisenmangelanämie-Diagnostik
hypochrome, mikrozytäre Anämie (oft primäre klinische Manifestation bei GI-Tumoren!)
Serumeisen, Ferritin erniedrigt, Transferrin hoch
1. Identifizierung einer möglichen Blutungsquelle
ausführliche Anamnese--Ernährung, Blutungshinweise?, Gyn- FU, Gastro-intestinale DU;
invasive GI-Infektion,Tumoren!!
DD: resorptive Störung (Malabsorption/Coeliakie, Ernährung) hämatolog. GK
(Thalassämie..?)
2. Therapieversuch mit oralem Eisen
c G. WeissEndoscopic findings in 100 patients with iron-
deficiency anaemia
Hämoccult auch bei
(vermuteter) Hypermennorhoe
c G. Weiss Rockey D, Cello JN. Engl J Med 1993; 329:1691–5.Iron deficiency anaemia not responsive
to oral iron therapy
• Negative iron balance (menstruation +/- specific diet, vegan…)
• Compliance problem—side effects
• H. pylori infection
• Achlorhydria, autoimmune gastritis (APCA+)
c G. WeissIron deficiency anaemia not responsive
to oral iron therapy
• Negative iron balance (menstruation +/- specific diet, vegan…)
• H. pylori infection
• Achlorhydria, autoimmune gastritis (APCA+)
• Impaired iron absorption (e.g. celiac disease)
• Vitamin deficiency (B12, folic acid, D3)
• Obesity
• Erythropoietin therapy, iron consumption
(training, growth)
• Genetic defect
c G. WeissAssociation of vitamin D deficiency and anaemia subtypes in persons ≥ 60 years.
Perlstein T S et al. Blood 2011;117:2800-2806
c G.WeissKEIN ANSPRECHEN AUF ORALE EISENTHERAPIE!-
INFLAMMATION?
RELATIVER versus ABSOLTUER EISENMANGEL
c G. Weiss
Weiss G, Goodnough LT. N Engl J Med 2005;352:1011–23.INFLAMMATION ALTERS IRON HOMEOSTASIS
and vice versa
Anaemia of chronic disease
Anaemia of inflammation
n The most frequently diagnosed anaemia in hospitalized patients
n Mild to moderate in severity; normocytic and normochromic
n Develops in patients with cellular immune activation
n Degree of anaemia correlates with extent of immune activationc G. Weiss Weiss G et al. Blood 2019
Pathways for iron retention in ACD
a collaborative work of acute phase proteins (Hepcidin) and cytokines
Weiss G. et al. Nat Rev Rheumatol 2013ACD is an immune-driven disease c G.Weiss Weiss G, Goodnough LT. N Engl J Med 2005;352:1011–23.
Positive effects of ACD?
n Withholds iron from infectious pathogens, thus limiting their growth 1
– iron acquisition is important for the pathogenicity of bacteria and fungi
n Reduces supply of oxygen to rapidly proliferating tissues
n Strengthens the immune response
– via impaired expression of EPO
– via iron restriction
EPO, erythropoietin. 1. Weinberg ED. Biochim Biophys Acta. 2009;1790:600-5.Anaemia diagnosis
Parameter ACD IDA
Serum iron concentration Reduced to normal Reduced
Transferrin levels Reduced to normal Increased
Transferrin saturation Reduced to normal Reduced
Ferritin Normal to increased Reduced
Serum transferrin receptor Normal Increased
sTfR/log ferritin Low (2)
Zinc protoporphyrin IX High High
Percentage hypochromic RBC n.a. High
Cytokines (TNF, IL-1, IL-6) Increased Normal
Cytokine levels are inversely correlated with the degree of anaemia
Sole iron determination in serum is not clinically useful
c G.WeissWhy is the differential diagnosis between ACD and IDA
important?
Because these patients may need contrasting therapies!!!
no additional iron in ACD
(iron is poorly absorbed and retained in macrophages)
iron needed in IDA
(true iron deficiency)
Clarify the underlying cause of IDA or ACD
c G.WeissIRON THERAPY
Nielsen O.H. et al. Medicine 2015THERAPIE
URSACHE des EISENMANGELS/der
Anämie feststellen und therapieren!!!
c G. WeissORALE EISENTHERAPIE
INDIKATION:
Wahrer Eisenmangel (vorher: Klärung der Ursache!!)
Keine Entzündungszeichen (Blockade der Resorption)
Keine Resorptionsstörung (Coeliakie)
•1x tägliche GABE (mind. 50mg) !!!
•Verbesserung der Resorption durch Vitamin C
•Einnahme auf nüchternen Magen !?– reduziert Compliance wegen NW (Gastrointestinal)
•– deshalb ggf. besser mit Essen einnehmen– keine Milchprodukte
c G. WeissAbsolute amount of iron absorbed in relation to the dose administered for the first
administration (continuous line°) and the second administration (broken line+).
Diego Moretti et al. Blood 2015;126:1981-1989Old and new preparations
Ferrous sulfate (FeSO4) Ferric maltol (Ferracru)
c G. WeissDie Resorption von Eisen aus dem Darm ist
bei Entzündung reduziert
c G. Weiss
Theurl I, et al. Blood 2009;113:5277–86.Intravenous iron therapy
• Indication:
– True and functional iron deficiency
– Defect of absorption
– Intolerance to oral iron therapy
– Lack of efficacy of oral iron therapy
– Convenience
– (Mild) chronic inflammation (autoimmune diseases [RA,
IBD], dialysis, chronic heart failure…)
c G.WeissNielsen O.H. et al. Medicine 2015
Model depicting the metabolism of various iv iron preparations and possible points of
iron-induced oxidative/nitrosative stress.
hepcidin
Koskenkorva-Frank et al. , Free Radical Biology and Medicine, Volume 65, 2013, 1174 - 1194Intravenous iron therapy
• Indication:
– True and functional iron deficiency
– Defect of absorption
– Rapid replenishment of empty iron stores and anemia
– Intolerance of oral iron therapy
– Lack of efficacy with oral iron therapy
– Chronic inflammation (autoimmune diseases (RA, IBD), dialysis, chronic heart failure…)
EMA-warning of very rare but life threatening anaphylactic reactions (mainly linked to
older iron dextran drugs which are no longer in clinical use)
Risk of Hypophosphatemia
Efficacy in advanced inflammation unknown
c G.Weissc G. Weiss Rampton et al. Haematologica 2014
IRON THERAPY CAVE: UNCERTAINTIES regarding the effects of iron therapy in patients with CANCER (palliative setting?), acute and chronic infections Nielsen O.H. et al. Medicine 2015
THERAPIEKONTOLLE
Hämoglobin-Anstieg– Beginn nach 3-4 Wochen (Ziel mind. 1g/dL– cave
repetitive Blutabnahmen)
Falls vorhanden: Retikulozyten oder Reti- Hb-Gehalt (2-3 Wochen)
Ferritin bzw. TfS– gute Indikatoren bei fehlender Inflammation
c G. WeissIron therapy balance
• Avoid over- and under-treatment
• Identify patients who will benefit from iron repletion/therapy
(e.g. true iron deficiency, perioperative blood management, avoidance of
transfusions, CHF...)
• Identify patients who may not benefit from iron therapy
c G.WeissDANKE
You can also read