The MEDIRAD multi-national 131I dosimetry study for thyroid ablation and adjuvant therapy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The MEDIRAD multi-national 131I
dosimetry study for thyroid ablation
and adjuvant therapy
Francesca Leek1, Jan Taprogge1, Rebecca Gregory8, Kate
Newbold1, Frederik Verburg2, Markus Luster2, Tino Schurrat2,
Johannes Trans-Gia3, Uta Eberlein3, Constantin Lapa3,
Andreas K Buck3, Michael Lassmann3, Erick Mora-Ramirez456,
Manuel Bardies45, Delphine Vallot7, Frederic Courbon7,
Lavinia Vija7, Glenn Flux1
1. The Royal Marsden NHSFT and Institute of Cancer Research, UK; 2.
University Hospital Marburg, Germany; 3. University Hospital Wuerzburg,
Germany; 4. Centre de Recherches en Cancerologie de Toulouse, France; 5.
INSERM, Universite Toulouse III Paul Sabatier, France; 6. University of
Costa Rica, Costa Rica; 7. IUCT-Oncopole, Toulouse Oncology Institute,
France; 8. Barts Health NHSFT, UK
This project has received funding from the Euratom research and
training programme 2014-2018 under grant agreement No 755523.
Implications of Medical Low Dose Radiation Exposure
4 year EC Horizon 2020 funded project (2017 – 2021); 33 partners in 14 countries.
Aims
• increase knowledge of health effects of diagnostic and therapeutic medical radiation
procedures.
• improve recording and estimation of doses.
• develop evidence based policies.
WP3 Impact of low dose radiation exposure from 131I radioiodine ablation of thyroid
cancer
Objectives
• Establish range of absorbed doses delivered to healthy organs.
• Determine threshold absorbed dose required for successful thyroid ablation.
• Assess the relation between patient biokinetics, success of thyroid ablation and acute to
mid-term toxicity.
• Assess optimal methods for internal dosimetry that can be applied practically in a large
scale European multicentre setting.
EC Horizon 2020 NFRP-9
Background
Differentiated thyroid cancer (DTC) is the most common endocrine malignancy, with a
UK incidence of ~2,500 per year.
Standard approach to treatment is radioiodine therapy (RAIT) following
thyroidectomy.
Current practice based on activity administered rather than dose to thyroid.
Activity administered for ablation is variable throughout Europe.
Hypothesis
Response is more dependent on the absorbed dose delivered to thyroid remnant or
residual disease than the level of activity administered. This would introduce the
possibility of tailoring administered activities to individual patients.
EC Horizon 2020 NFRP-9
Work package design
Patient recruitment &
standardised data acquisition
Dose data
repository &
biobank
Centralised Biomarkers of
Biokinetic
dosimetry absorbed dose
modelling
calculations and sensitivity
Large scale
epidemiological
study
EC Horizon 2020 NFRP-9
Clinical protocol
Multicentre, international, prospective observational study.
100 adults with DTC post-total thyroidectomy will be recruited across four centres:
• Philipps-Universität Marburg & Universitätsklinikum Würzburg, Germany
• Institut Universitaire du Cancer de Toulouse Oncopole, France
• The Royal Marsden NHSFT, UK
Inclusion criteria
• Adults with histological evidence for DTC (papillary, follicular variants)
• Pathology stratification (AJCC/TNM 2017): pT1b - pT3, Nx-N0-N1, M0
• Total thyroidectomy performed within 8 weeks of radioiodine treatment
Exclusion criteria
• Aggressive histology variants
• EBRT / systemic chemotherapy in the last 6 weeks
• Previous radioiodine treatment
• Pregnancy/breast-feeding
Patient admission
• 1.1 - 3.7 GBq 131I; mode of TSH stimulation at clinician discretion
EC Horizon 2020 NFRP-9
Imaging and data acquisition standardisation
Acquisition protocol development
Flexible image acquisition protocol for dosimetry allows for inter-centre variabilities
with respect to access to hybrid imaging and local radiation protection regulations.
Time post-131I admin. Mandatory Additional*
6±2h WB planar and/or SPECT(/CT)**
24 ± 4 h WB planar SPECT(/CT)**
48 ± 4 h WB planar and SPECT(/CT)**
72 ± 12 h WB planar SPECT(/CT)**
96 ± 12 h WB planar SPECT(/CT)**
168 ± 24 h WB planar and/or SPECT(/CT)**
* To be conducted at the discretion of each site; ** SPECT(/CT) range: base of skull to top of thigh
EC Horizon 2020 NFRP-9
Imaging and data acquisition standardisation
Validation of centres within imaging network
First European network able to perform
standardised quantitative 131I imaging for
dosimetry has been established.
Each centre performed routine gamma camera
quality assurance tests relevant to 131I imaging
prior to calibration.
Each system characterised in terms of sensitivity,
recovery coefficients and dead time.
Centre Country Gamma camera
RMH UK 2 x Siemens Intevo Excel SPECT/CT
UKW Germany Siemens Intevo Bold SPECT/CT
UMR Germany Siemens Symbia S SPECT
IUCT-O France GE Discovery 670 SPECT/CT
EC Horizon 2020 NFRP-9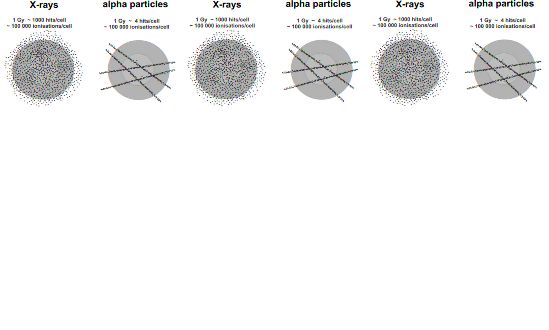
Imaging and data acquisition standardisation
System volume sensitivity
Manufacturer Model SVS
[cps/MBq]
Intevo Excel 79.1
Intevo Excel 81.6
Siemens
Intevo Bold 91.9
Symbia S 44.9
GE Discovery 670 57.8
EC Horizon 2020 NFRP-9
Imaging and data acquisition standardisation
Recovery coefficient determination
Six 3D printed spheres of varying volumes, 0.524 - 144 ml, positioned in a head
shaped phantom SPECT scanned.
Data was centrally reconstructed and partial volume corrections determined.
EC Horizon 2020 NFRP-9
Imaging and data acquisition standardisation
Dead-time characterisation
UK protocol developed for high activity 131I
imaging was modified to comply with local
radiation protection rules in France and
Germany:
• high activities of liquid 131I deemed to be a
contamination risk.
• phantom designed and built to allow the
use of a high activity sealed source of 131I.
EC Horizon 2020 NFRP-9Imaging and data acquisition standardisation
Dead-time characterisation
Manufacturer Model DT [μs]
Intevo Excel1 1.42 ± 0.08
Intevo Excel2 1.69 ± 0.06
Siemens
Intevo Bold 3.47 ± 0.16
Symbia S 4.59 ± 0.07
EC Horizon 2020 NFRP-9Current status
Data acquisition and dosimetry protocols suitable for implementation in a multicentre
setting have been developed.
All four imaging centres have been set-up for quantitative imaging.
Ethics applications are under review with local IRBs.
A population biokinetic model has been developed incorporating covariates to explain
inter-patient variation.
Methodologies have been developed for planar and 3D dosimetry.
Preparatory work is being undertaken to conduct biomarker studies with γ-H2AX as a
marker of both radiation damage to the DNA and of sensitivity.
EC Horizon 2020 NFRP-9Conclusions
First European multicentre dosimetry study with SPECT/CT will be performed.
Results are expected to identify the threshold absorbed dose required for a
successful response.
Introduce the possibility of patient specific treatment planning that will minimise risk to
the patient while ensuring a successful outcome.
This will:
• facilitate the development of a large scale epidemiological study of the effect of low
absorbed doses from irradiation of normal organs and internal sources of
radionuclides.
• lead to recommendations and protocols for the calculation of absorbed doses to
normal organs from internal sources of 131I that will facilitate accurate risk analysis
in a large population.
EC Horizon 2020 NFRP-9This project has received funding from the Euratom research and training programme 2014-2018 under grant agreement No 755523.
Imaging and data acquisition standardisation
Standardisation SPECT/CT with low dose CT
Scanning parameters SPECT/CT parameters for I-131 imaging
(at IUCT-O), HEGP, high-energy general purpose; SPECT, single-
EC Horizon
photon 2020CT
emission NFRP-9Biokinetic modelling and treatment planning
Pharmacokinetic models of the International Commission on Radiation Protection
developed for healthy humans or animals.
Not appropriate to estimate radiation doses for individual patients or potentially a specific
patient cohort:
• Disease may affect bio-kinetic properties
• Radioiodine kinetics after partial or full thyroidectomy in thyroid cancer patients
Aim
Develop model for 131I-NaI in thyroid cancer patients
• Is personalised treatment planning based on individual biokinetics feasible?
• Assess relationship between patient biokinetics and outcome.
EC Horizon 2020 NFRP-9Pilot data-set & Methods
• 21 thyroid cancer patients after near-total or complete
thyroidectomy treated with 3000 MBq of 131I-NaI
• SPECT scans at 24, 48, 72 and (96) hours
• Blood activity from samples at 24, 48, 72 and 144 h
• Whole body activity retention measurements
• Two classical approaches for population modelling:
• Two-stage approach (= fit each subject individually)
• Naïve-pooled approach (= fit all at the same time)
• Use Non-Linear Mixed Effects (NLME) modelling instead:
• Fixed effects: Population parameters (rate constants)
• Random effects: Inter-patient variability +
residual errors (i.e. measurement uncertainties)
EC Horizon 2020 NFRP-9Blood sampling and immunofluorescence analysis
• Blood sampling • Incubation with specific antibodies for
• Centrifugation Separation of γ-H2AX and 53BP1
leucocytes • Immunofluorescence analysis: manual
enumeration of co-localizing γ-H2AX
and 53BP1 foci in 100 cells
• Washing in PBS
• Fixation with ethanol
Würzburg München
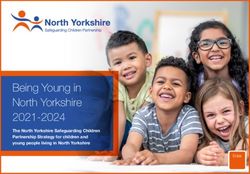
EC Horizon 2020 NFRP-9Ex-vivo calibration curves for α- and β/γ-emitting
radionuclides
• small γ-H2AX + 53BP1 foci for β/γ-emitters
• γ-H2AX + 53BP1 tracks for α- emitters
Lu-177+I-131
ܴܨܫ ܴܨܫ ܴܨܫ
( = )ܦ0.0147 ȉ ȉ ݉ ିݕܩଵ ȉ ܦ+ 0.0363 ȉ
݈݈ܿ݁ ݈݈ܿ݁ ݈݈ܿ݁
γ
Schumann et al., Sci Rep. 2018.
Schumann et al., EJNMMI Res. 2018.
EC Horizon 2020 NFRP-9
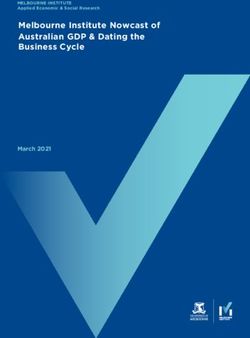
Eberlein et al. PLoS ONE, 2015In-vivo study with Lu-177-PSMA (16 patients)
• γ-H2AX + 53BP1 radiation induced foci (RIF) as a function of the absorbed dose to the
blood
Schumann et al. accepted 03/2019, EJNMMI
first three sampling time points:
EC Horizon 2020 NFRP-9
up to 2.6 h after administrationNext steps: Blood sampling protocol for radioiodine
therapy
• 20 patients from Würzburg (full protocoll)
• Blood sampling time points:
• before administration for background value and ex-vivo irradiation
• 1 h after administration
• 2 h after administration
• 3 h after administration
• 4 h after administration approx. 50 mGy
• 24 h after administration after 1 h incubation
• 48 h after administration +
• 96 h after administration 10 patients from
• 168 h after administration (optional) Marburg
EC Horizon 2020 NFRP-9You can also read