DICHIARAZIONE Relatore: DANIELA PIETRA - siesonline
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DICHIARAZIONE
Relatore: DANIELA PIETRA
Come da nuova regolamentazione della Commissione Nazionale per la Formazione Continua del Ministero della Salute, è richiesta la
trasparenza delle fonti di finanziamento e dei rapporti con soggetti portatori di interessi commerciali in campo sanitario.
• Posizione di dipendente in aziende con interessi commerciali in campo sanitario (NIENTE DA DICHIARARE)
• Consulenza ad aziende con interessi commerciali in campo sanitario (NIENTE DA DICHIARARE)
• Fondi per la ricerca da aziende con interessi commerciali in campo sanitario (NIENTE DA DICHIARARE)
• Partecipazione ad Advisory Board (NIENTE DA DICHIARARE)
• Titolarietà di brevetti in compartecipazione ad aziende con interessi commerciali in campo sanitario (NIENTE DA
DICHIARARE)
• Partecipazioni azionarie in aziende con interessi commerciali in campo sanitario (NIENTE DA DICHIARARE)
• Altro
Somatic mutations of CALR
in myeloproliferative neoplasms
Daniela Pietra
Division of Hematology
Department of Oncology and Hematology
Fondazione IRCCS Policlinico San Matteo Pavia
University of Pavia Medical School
The genetic basis of MPN
PV ET PMF
wild
type
5%
wild
2005 wild
type type JAK2
JAK2 V617F
JAK2 V617F JAK2
41% V617F
47%
53%
V617F 59%
95%
JAK2
ex12
wild
2006-2007 5%
type
wild
type
37% JAK2
JAK2 ex12 JAK2
V617F
40%
V617F
JAK2 53%
MPL V617F MPL
59%
MPL
95% 4%
7%
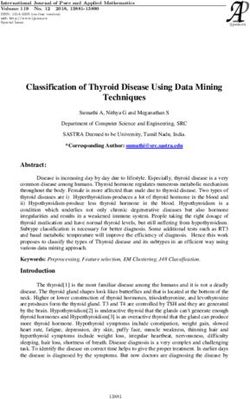
CALR ex9 somatic mutations in MPN
• WES on genomic DNA from granulocytes and
CD3+ T-cells from 6 PMF identified recurrently
somatic mutations in CALR
• The screening of a cohort of 896 MPN patients
identified 150 cases (17%) with indels in CALR
– 0/382 PV
– 78/311 ET (25%)
– 72/203 PMF (35%)
• All CALR-pos patients were negative for JAK2
and MPL
Klampfl et al. NEJM 2013;369:2379-90
The genetic basis of MPN
PV ET PMF
wild
type
5%
wild
2005 wild
type type JAK2
JAK2 V617F
JAK2 V617F JAK2
41% V617F
47%
53%
V617F 59%
95%
JAK2
ex12
wild
2006-2007 5%
type
wild
type
37% JAK2
JAK2 ex12 JAK2
V617F
40%
V617F
JAK2 53%
MPL V617F MPL
59%
MPL
95% 4%
7%
JAK2 wild wild
ex12 type type
5% 12% 5%
2013 CALR
CALR
35%
JAK2
25% JAK2 V617F
CALR JAK2 V617F 53%
V617F MPL 59%
4% MPL
95% 7%
A novel C-term peptide in mutant CALR
N-‐domain
P-‐domain
C-‐domain
KDEL
5’
UTR
Ex.
1
E
x.
2
E
x.
3
Ex.
4
E
x.
5
E
x.
6
E
x.
7
Ex.
8
Ex.
9
3’
UTR
Both impaired Ca-binding activity
and cellular dislocation may play a
role in the abnormal proliferation of
cells expressing a mutant CALR
Klampfl et al. NEJM 2013;369:2379-90
Unpublished dataGenetic and functional analysis
of CALR mutations
e128 RAMPAL et al BLOOD, 29 MAY 2014 x VOLUME 123, NUMBER 22
e128 RAMPAL et al BLOOD, 29 MAY 2014 x VOLUME 123, NUMBER 22
Klampfl et al. NEJM 2013;369:2379-90
Rampal et al. Blood 2014;123:e123-e133
Figure 3. CALR-mutant MPN patients are characterized by a gene signature associated with activated JAK2 signaling. (A) Mutational status of JAK2, CALR, and MPL
mutational status as well as clinical MPN diagnosis in 290 MPN patients. An individual column represents each patient. (B) GSEA showing enrichment of JAK2 shRNA
signature in MPN patients with CALR mutations relative to normal subjects. (C) Heatmap representation of the 433 significantly differentially expressed genes (413 genes
upregulated and 20 downregulated; FDR ,0.01 and FC .2) in granulocytes from CALR-mutant MPN patients relative to normal subjects (21 MPN patients and 11 normal
subjects). A red-blue color scale depicts normalized gene expression levels (red: high; blue: low). (D) GSEA showing significant enrichment of CALR-mutant MPN signature in
MPN patients with homozygous JAK2V617F mutations relative to normal subjects.
Figure 3. CALR-mutant MPN patients are characterized by a gene signature associated with activated JAK2 signaling. (A) Mutational status of JAK2, CALR, and MPL
mutational status as well as clinical MPN diagnosis in 290 MPN patients. An individual column represents each patient. (B) GSEA showing enrichment of JAK2 shRNA(solid cancers, used as controls), JAK2V617F-mutated polycythemia fainter in myeloid and erythroid cells, compared with m
vera, ET and PMF patients; MPL-mutated ET or PMF (n ¼ 8); yocytes (Figures 3e and f).
JAK2/MPL/CALR triple-negative patients; CALR-mutated ET or PMF
CALR mutations primarly affect
patients, including the CALRdel52, CALRins5 and CALRindel Preferential expression of calreticulin in cells of megakar
(ins50 -TCCTTCAG-delGCAGAGAAACAAATGAAGGACAAACAGGACG-30 ) lineage
(n ¼ 2) mutations. Results are presented in Figure 2. Subjects We then asked whether the much more pronounced
with non-hematologic disorders (not shown), MPN patients observed in megakaryocytes compared with cells of the
harboring the JAK2V617F and MPLW515 mutation and and erythroid cell lineages was a consequence of the ac
the biology of megakaryocytes triple-negative ET and PMF patients, all resulted negative with
the antibody raised against anti-mutated calreticulin (panel 2a).
Conversely, the three variants of CALR mutations showed strong
immunostaining (panel 2b), thus establishing the specificity of the
of the CALR mutation itself or rather it reflected a ph
megakaryocytic lineage-associated overexpression of ca
To this end, we used a commercially available antibody
against the N terminus of calreticulin, therefore expected
Klampfl et al. NEJM 2013;369:2379-90
Vannucchi et al. Leukemia 2014;28:1811-1818
Figure 3. Immunostaining of bone marrow biopsies with the anti-mutated CALR antibody. Panel a shows two megakaryocytes labele
anti-mutated calreticulin antibody together with a negative one. In panel b, abnormal, small megakaryocytes in the bone mar
CALRins5 PMF patient are shown. Panel c shows a low-resolution picture of an advanced fibrosis in a CALRdel52 patient and d is a hig
field from panel c (square) to show the abnormally shaped large megakaryocytes within buddles of fibers. In panels e and f, the fainFrom bloodjournal.hematologylibrary.org at POLICLINICO S. MATTEO AMMINISTRAZIONE on March 17, 2014. For
personal use only.
1546 RUMI et al BLOOD, 6 MARCH 2014 x VOLUME 123, NUMBER 10
The impact of CALR mutations on ET
Table 2. Demographic, hematologic, and clinical features at diagnosis of patients with ET, subdivided according to JAK2 or CALR mutation
status, and of patients with PV
ET
CALR mutated (A) JAK2 mutated (B) PV (C) P
No. 176 466 468 (A) vs (B) (B) vs (C) (A) vs (C)
Sex (male/female) 90/86 (51%/49%) 167/299 (36%/64%) 233/235 (50%/50%) .001 ,.001 .791
Age at onset, years, median (range) 45 (15-83) 50 (15-92) 57 (13-86) .001 ,.001 ,.001
Hemoglobin, g/dL, median (range) 13.8 (11.3-17.6) 14.4 (10-17.7) 18.2 (15.0-24.0) ,.001 ,.001 ,.001
WBC count, 3109/L, median (range) 8.0 (4.0-17.9) 9.0 (4.0-28.0) 10.0 (3.4-55.3) ,.001 ,.001 ,.001
PLT count, 3109/L, median (range) 883 (500-3000) 700 (456-2148) 464 (109-1472) ,.001 ,.001 ,.001
Serum erythropoietin, mU/mL, median (range) 9.4 (1.2-27) 4.7 (0-47) 2.7 (0-66) ,.001 ,.001 ,.001
Splenomegaly, no. (%) 4 (2.3%) 30 (6.4%) 105 (22.4%) .046 ,.001 ,.001
Lactate dehydrogenase, mU/mL, median (range) 199 (78-472) 200 (77-540) 217 (104-758) .83 ,.001 .003
Circulating CD341 cells, 3106/L, median (range) 4.1 (0.6-18) 4 (0-15.3) 3.4 (0-261.3) .50 .037 .039
Thrombosis at diagnosis, no. (%) 5 (2.8%) 33 (7.1%) 49 (10.5%) .059 .082 .001
Table 2 reports the demographic and clinical characteristics at (P , .001 in all comparisons). Patients with PV had higher values for
diagnosis of the patients studied according to their genotype, whereas Hb level and WBC count, lower values for PLT count and serum
the main hematologic parameters are summarized in Figure 1. Patients Epo, and higher frequency of splenomegaly compared with both
with CALR-mutated ET were significantly younger than those with CALR- and JAK2-mutated ET patients (P values shown in Table 2).
JAK2-mutated ET (P 5. 001) or PV (P , .001). Compared with The incidence of thrombosis at diagnosis was significantly higher in
patients with CALR-mutated ET, those with JAK2-mutated ET had
higher hemoglobin (Hb) level and white blood cell (WBC) count,
23 CALR variants
patients with PV than in those with CALR-mutated ET (P 5 .001), but
not different between patients with PV and those with JAK2-mutated
and lower platelet (PLT) count and serum erythropoietin (Epo) level ET (P 5 .08).
Type 1: 46%
Type 2: 38%
Rumi et al. Blood 2014;123:1544-1551CALR-mutant ET is a distinct
nosolgical entity
25.1% 34.7%
28.6%
10.5%
93%
77%
50%
42%
32%
18%
Rumi et al. Blood 2014;123:1544-1551From www.bloodjournal.org by guest on October 3, 2014. For personal use only.
The impact of CALR mutations on PMF
BLOOD, 14 AUGUST 2014 x VOLUME 124, NUMBER 7 MUTATIONS AND PROGNOSIS OF PRIMARY MYELOFIBROSIS 1063
Table 1. Demographic and clinical features at diagnosis of 617 patients with PMF subdivided according to their genotype (JAK2, CALR, and
MPL mutation status)
JAK2 (V617F)-mutant CALR-mutant MPL-mutant Patients with nonmutated JAK2, CALR,
No. = 617 patients patients patients and MPL (triple-negative subjects) P
No. (%) 399 (64.7%) 140 (22.7%) 25 (4.0%) 53 (8.6%)
Sex (male/female) 266/133 77/63 17/8 34/19 .101
Age at onset, median (range), y 63 (18-91) 50 (26-83) 64 (31-84) 67 (31-88) ,.001
Hemoglobin, median (range), g/dL 12 (3-19.6) 11.7 (7.1-15.9) 11 (6.5-15) 9.9 (5-19) ,.001
WBC count, median (range), 3109/L 10 (1.6-106.2) 8.2 (2.2-45) 8.4 (2.1-20.3) 8.4 (2.4-90.8) .002
PLT count, median (range), 3109/L 310 (25-1963) 509 (46-1563) 307 (53-958) 175 (19-3279) ,.001
Circulating blasts, median (range), % 0 (0-20) 0 (0-10) 0 (0-4) 0 (0-16) ,.001
Lactate dehydrogenase, median (range), 553 (149-3440) 692 (203-3610) 580 (183-2291) 531 (160-3173) .208
mU/mL
Circulating CD341 cells, median (range), 16.2 (0.8-1190) 34.2 (1.7-1902) 100 (6.3-506.3) 45.3 (1.6-485.5) .022
3106/L
IPSS risk group, %
Low 31 51 28 10 ,.001
Intermediate 1 31 23 36 26
Intermediate 2 22 18 24 17
High 16 8 12 47
Type1 CALR mutation is significantly more frequent
mutation.6 In the current work, we studied a large population of
patients with PMF followed at 4 different centers and analyzed the
Statistical analysis
Numerical variables have been summarized by their median and range, and
in PMF than in ET (72% vs 46%, PThe impact of CALR mutations on PMF
Thrombosis
Lower IPSS
Leukemic transformation
Higher IPSS
Rumi et al. Blood 2014;124:1062-1069JAK2, CALR, and MPL mutation status is
essential in PMF diagnosis and prognosis
CALR and ASXL1 mutations-based prognosis in myelofibrosis
A Tefferi et al
Rumi et al. Blood 2014;124:1062-1069
1497
CALR+ASXL1-
1
N=46
Median 10.4 years
0.8
0.6 PConclusions • Accounting for JAK2, MPL, and CALR mutation status is of fundamental diagnostic and prognostic relevance in MPN, especially when bone marrow fibrosis is present • It also provides a new powerful tool for understanding the molecular basis of MPN, indicating a role of megakaryocytes in the pathogenesis of MPNs
Role of megakaryocytes
in the pathofisiology of MPN
• Under normal conditions, MK
contribute to the bone marrow matrix
environment by expressing fibronectin,
type IV collagen, and laminin
• A unifying model of the pathofisiology
of MPN implies that the founding driver
mutation activates the JAK-STAT
pathway in MK, resulting in
thrombocytosis initially and in bone
marrow fibrosis in the long term
Cazzola & Kralovics Blood 2014;123:3714-9Patterns of clonal evolution and
phenotypic switch in MPN
• JAK2-pos ET may transform into PV
and then progress to sMF: % V617F
alleles is a major factor in causing the
different phenotypes and 9pUPD is
associated with fibrotic evolution
• MPL mutations are found in ET and
PMF; 1pUPD is associated with
myelofibrotic transformation
• CALR ex9 mutations are found in ET
and PMF, but 19pUPD seems to be a
rare event. Disease evolution is mainly
characterised by the progressive
expansion of a heterozygous clone
that becomes fully dominant in the BM
and specifically activates MK
Cazzola & Kralovics Blood 2014;123:3714-9You can also read